
Towards Predicting Length of Stay and Identification of Cohort Risk Factors Using Self-Attention-Based Transformers and Association Mining: COVID-19 as a Phenotype

 , ,
, , 
Abstract
:1. Introduction
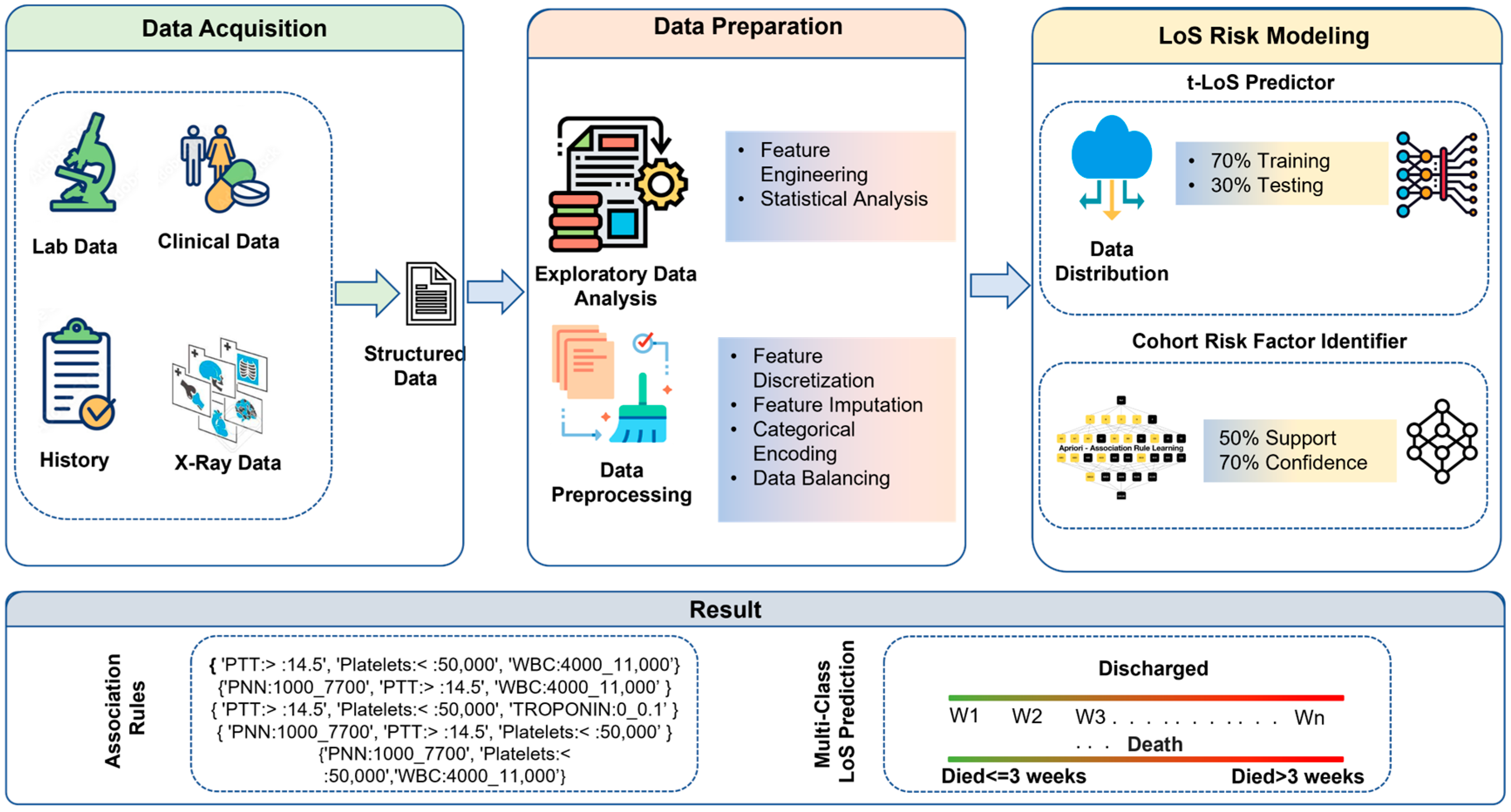
2. Materials and Methods
2.1. Data Acquisition
2.2. Data Preparation
2.2.1. Natural Binning
2.2.2. Encoding of Categorical Features
2.2.3. LoS Category Creation
2.2.4. Data Balancing with Respect to LoS
2.3. LoS Risk Modeling
2.3.1. t-LoS Predictor
2.3.2. Cohort Risk Factor Identifier (CRFI)
3. Results and Evaluation
3.1. COVID-19 Risk Model Results
3.2. CRFI Results
3.2.1. CRFI for Discharged Patient Category
3.2.2. CRFI for Deceased Patient Category
4. Discussion
- Age appears to be a strong risk factor for COVID-19 severity and its outcomes. Statsenko et al. [21] performed a detailed analysis and concluded that elderly patients with COVID-19 are more likely to progress to severe disease. The result of the CRFI for the deceased category identified rules for individuals aged ≥56 years and ≤73 years, while other age category rules were not frequently observed and found to be insignificant. In addition, the mining results for patients who stayed in the hospital for between three and four weeks followed 25% of the rules for patients aged ≥73. These observations validate the fact that age is correlated with COVD-19 severity and a significant factor in deciding LoS.
- A detailed analysis of CRFI rules for the patients who stayed in the hospital for between 3 and 4 weeks showed that 43% of the rules constituted either hypertension or diabetes; thus, these comorbidities not only increase the LoS in hospitals but also lead to severe COVID-19, leading to increased LoS in the hospital. This was also concluded by Adab et al., 2022 [22].
- An elevated level of D-dimers is an indicator and major risk factor for thrombosis (blood clotting) and increases the risk of medication and monitoring for a longer time [23]. We observed that for the people who were discharged between 3 and 4 weeks, the CRFI results for D-dimers show that 18% of the rules had a D-dimer value of more than 500 ng/mL FEU, thus increasing the LoS. In addition, in the mining results for patients who stayed more than 3 weeks in the hospital and died, elevated D-dimer values were present in 41% of the rules. This is also validated by the fact that for the people who were discharged within two weeks, the CRFI results show only 4.5% of the rules had a D-dimer value of more than 500 ng/mL FEU, and elevated D-dimer values were not found to be significant according to the CFRI results of patients who stayed less than one week.
- LDH is another factor that had an elevated level of more than 225 units/L in 23% of the rules, based on the CRFI results of patients discharged from the hospital between 3 and 4 weeks.
- Wagner et al. [24] concluded that lymphocyte count is one of the most important prognostic factors in determining COVID-19 severity, and our CRFI results for patients who died after spending more than 3 weeks in the hospital found that all the rules with lymphocytes consisted of values between 500 and 1000, while for patients who were discharged within two weeks, 86% of the time, these values were between 1000 and 4000. This again validates the fact that a lower lymphocyte count is critical in determining COVID-19 severity and LoS.
- During the initial stages of the COVID-19 pandemic, the medical community employed various treatments without substantial evidence to support their efficacy. This was due to the limited understanding of the novel coronavirus and its treatment options at the time. It is important to understand which medications, based on the lessons learned, could be useful to treat infections caused by new viral strains as viable epidemic response strategies. Our study shows that drugs such as Hydroxychloroquine and Favipiravir reduce the patient LoS. The CRFI results for patients who stayed less than a week in the hospital show 51% of the rules consisted of antibiotic medications, while in those discharged in less than 2 weeks, 52% of the rules consisted of antiviral medication. This analysis shows that the usage of antiviral and antibiotic medication effectively reduced patient LoS.
5. Limitation and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Patient Features | Optimized Binning Interval |
|---|---|
| Age | ≤37 years |
| ≥38 years and ≤55 years | |
| ≥56 years and ≤73 years | |
| ≥74 years | |
| pH | {≤7.35; 7.35–7.45; >7.45} |
| PaO2 | {≤80 mm Hg; >80 mm Hg} |
| PaCO2 | {≤35 mm Hg; 35–45mm Hg; >45 mm Hg} |
| HCO3 | {≤21 mEq/L; 21–27 mEq/L} |
| Temperature | {≤36 °C; 37.6–38.6 °C; >38.6 °C} |
| Respiratory Rate | {≤12 bpm; 12–20 bpm; 20–28 bpm} |
| Pulse | {≤79 bpm; 79–95 bpm; 95–111 bpm; 111–134 bpm; 134–185 bpm} |
| Systolic Blood Pressure | {≤90 mm Hg; 90–130 mm Hg} |
| Diastolic Blood Pressure | {≤60 mm Hg; 60–90 mm Hg} |
| Glasgow | {<4; 4–8; 8–12; 12–14; >14} |
| WBC | {≤4000/µL; 4000–11,000/µL; >4000/µL} |
| PNN | {≤500 mm3; 500–1000 mm3; 1000–7700 mm3; 7700–15,000 mm3} |
| Lymphocytes | {≤500 cells/µL; 500–1000 cells/µL; 1000–4000 cells/µL; >4000 cells/µL} |
| Hemoglobin | {≤8 g/dl; 8–10 g/dl; 10–12 g/dl} |
| Platelets | {≤50,000/µL; 50,000–150,000/µL; 150,000–450,000/µL} |
| Creatinine | {≤59 mg/dL; 59–104 mg/dL; 104–250 mg/dL; 250–500 mg/dL} |
| ALT | 1–41 U/L; >41 U/L |
| LDH | {≤135 IU/L; 135–225 IU/L} |
| FERRITIN | {≤792; 792–1976; 1976–4374; 4374–7627; 7627–159,000} |
| D_DIMER | {0–500 ng/mL; >500 ng/mL} |
| CRP | {≤6 mg/L; 6–100 mg/L; >100 mg/L} |
| PROCALCITONIN | {≤0.25 ng/mL; 0.25–0.5 ng/mL; >0.5 ng/mL} |
| TROPONIN | {≤0.1 ng/mL; >0.1 ng/mL} |
| ProBNP | {≤12 pg/mL; 12 pg/mL–5 pg/mL; 5–450 pg/mL} |
| PTT | {≤11.5; 11.5–14.5} |
| Vitamin D | {≤50 nmol/L; 50–250 nmol/L} |
| IL-6 | {≤37.5 pg/mL; >37.5 pg/mL} |
| Hyperparameters | Value |
|---|---|
| Learning rate | 0.001 |
| Weight decay | 0.0001 |
| Dropout rate | 0.2 |
| Batch size | 8 |
| Number of epochs | 15 |
| Number of transformer blocks | 3 |
| Number of attention heads | 4 |
| Embedding dimensions of the categorical features | 16 |
| MLP hidden layer units, as factors of the number of inputs | [2, 1] |
| Number of MLP blocks in the baseline model | 2 |
References
- World Health Organization. Second Round of the National Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic: January–March 2021: Interim Report, 22 April 2021; No. WHO/2019-nCoV/EHS_Continuity/Survey/2021.1; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Mathieu, E. Coronavirus (COVID-19) Hospitalizations. Our World in Data. Available online: https://ourworldindata.org/covid-hospitalizations (accessed on 28 December 2022).
- Bravata, D.M.; Perkins, A.J.; Myers, L.J.; Arling, G.; Zhang, Y.; Zillich, A.J.; Reese, L.; Dysangco, A.; Agarwal, R.; Myers, J.; et al. Association of intensive care unit patient load and demand with mortality rates in US Department of Veterans Affairs hospitals during the COVID-19 pandemic. JAMA Netw. Open 2021, 4, e2034266. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.M.; Wendlandt, B.; Zadravecz, F.J.; Adhikari, R.; Winslow, C.; Edelson, D.P. Association between intensive care unit transfer delay and hospital mortality: A multicenter investigation. J. Hosp. Med. 2016, 11, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Resar, R.; Nolan, K.; Kaczynski, D.; Jensen, K. Using real-time demand capacity management to improve hospitalwide patient flow. Jt. Comm. J. Qual. Patient Saf. 2011, 37, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.J.; Elixhauser, A. Overview of Hospital Stays in the United States, 2012. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Statistical Brief# 180; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2014. [Google Scholar]
- Luo, L.; Lian, S.; Feng, C.; Huang, D.; Zhang, W. Data mining-based detection of rapid growth in length of stay on COPD patients. In Proceedings of the 2017 IEEE 2nd International Conference on Big Data Analysis (ICBDA), Beijing, China, 10–12 March 2017; pp. 254–258. [Google Scholar]
- Dogu, E.; Albayrak, Y.E.; Tuncay, E. Length of hospital stay prediction with an integrated approach of statistical-based fuzzy cognitive maps and artificial neural networks. Med. Biol. Eng. Comput. 2021, 59, 483–496. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, H.; Thangam, M.; Amin, A.P. Artificial neural network-based prediction of prolonged length of stay and need for post-acute care in acute coronary syndrome patients undergoing percutaneous coronary intervention. Eur. J. Clin. Investig. 2021, 51, e13406. [Google Scholar] [CrossRef] [PubMed]
- Dan, T.; Li, Y.; Zhu, Z.; Chen, X.; Quan, W.; Hu, Y.; Tao, G.; Zhu, L.; Zhu, J.; Jin, Y.; et al. Machine learning to predict ICU admission, ICU mortality and survivors’ length of stay among COVID-19 patients: Toward optimal allocation of ICU resources. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Republic of Korea, 16–19 December 2020; pp. 555–561. [Google Scholar]
- Vekaria, B.; Overton, C.; Wiśniowski, A.; Ahmad, S.; Aparicio-Castro, A.; Curran-Sebastian, J.; Eddleston, J.; Hanley, N.A.; House, T.; Kim, J.; et al. Hospital length of stay for COVID-19 patients: Data-driven methods for forward planning. BMC Infect. Dis. 2021, 21, 700. [Google Scholar] [CrossRef] [PubMed]
- Zebin, T.; Chaussalet, T.J. Design and implementation of a deep recurrent model for prediction of readmission in urgent care using electronic health records. In Proceedings of the 2019 IEEE Conference on Computational Intelligence in Bioinformatics and Computational Biology (CIBCB), Siena, Italy, 9–11 July 2019; pp. 1–5. [Google Scholar]
- Johnson, A.E.W.; Pollard, T.J.; Shen, L.; Lehman, L.-W.H.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [PubMed]
- Harerimana, G.; Kim, J.W.; Jang, B. A deep attention model to forecast the Length of Stay and the in-hospital mortality right on admission from ICD codes and demographic data. J. Biomed. Inform. 2021, 118, 103778. [Google Scholar] [CrossRef] [PubMed]
- Rajkomar, A.; Oren, E.; Chen, K.; Dai, A.M.; Hajaj, N.; Hardt, M.; Liu, P.J.; Liu, X.; Marcus, J.; Sun, M.; et al. Scalable and accurate deep learning with electronic health records. Npj Digit. Med. 2018, 1, 1–10. [Google Scholar] [CrossRef]
- North, M.A. A method for implementing a statistically significant number of data classes in the Jenks algorithm. In Proceedings of the 2009 Sixth International Conference on Fuzzy Systems and Knowledge Discovery, Tianjin, China, 14–16 August 2009; Volume 1, pp. 35–38. [Google Scholar]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Huang, X.; Khetan, A.; Cvitkovic, M.; Karnin, Z. Tabtransformer: Tabular data modeling using contextual embeddings. arXiv 2020, arXiv:2012.06678. [Google Scholar]
- Borgelt, C.; Kruse, R. Induction of association rules: Apriori implementation. In Compstat; Physica: Heidelberg, Germany, 2002; pp. 395–400. [Google Scholar]
- GitHub—Covid19_Research. (n.d.). Available online: https://github.com/smileslab/Covid19_research/tree/main/Association_Mining (accessed on 28 December 2022).
- Statsenko, Y.; Al Zahmi, F.; Habuza, T.; Almansoori, T.M.; Smetanina, D.; Simiyu, G.L.; Gorkom, K.N.-V.; Ljubisavljevic, M.; Awawdeh, R.; Elshekhali, H.; et al. Impact of Age and Sex on COVID-19 Severity Assessed From Radiologic and Clinical Findings. Front. Cell. Infect. Microbiol. 2022, 11, 1395. [Google Scholar] [CrossRef] [PubMed]
- Adab, P.; Haroon, S.; O’Hara, M.E.; Jordan, R.E. Comorbidities and COVID-19. BMJ 2022, 377, o1431. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, A.; Prosch, H.; Zehetmayer, S.; Gysan, M.R.; Bernitzky, D.; Vonbank, K.; Idzko, M.; Gompelmann, D. Impact of persistent D-dimer elevation following recovery from COVID-19. PLoS ONE 2021, 16, e0258351. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.; DuPont, A.; Larson, S.; Cash, B.; Farooq, A. Absolute lymphocyte count is a prognostic marker in COVID-19: A retrospective cohort review. Int. J. Lab. Hematol. 2020, 42, 761–765. [Google Scholar] [CrossRef] [PubMed]

| Dataset Source | Description | Feature Frequency |
|---|---|---|
| General | Contains general information such as demographic data (gender, age, and ethnicity), epidemiological data (date of admission, date of death), and comorbidities such as hypertension, diabetes, COPD, interstitial lung disease, bronchial asthma, liver disease, HIV, cirrhosis, and cardiomyopathies | 68 |
| Lab Data | Contains elements related to blood tests such as WBC count, PNN, lymphocyte count, hemoglobin, platelets, creatinine, ALT LDH, FERRITIN, D-DIMER, CRP, PROCALCITONIN, TROPONIN, Pro-BNP, PTT, Vitamin D, and IL6 | 17 |
| X-ray Data | Contains elements related to X-rays, such as the presence of consolidation and bilateral or unilateral ground-glass opacities | 4 |
| Patient Characteristics | Details: % of Patients That Qualify | ||
|---|---|---|---|
| General | Demographic | Gender | Female: 49.7%; Male: 50.3% |
| Age | |||
| Mean | 58.8 years | ||
| Median | 60 years | ||
| IQR | 26.7 years | ||
| Nationality | Egypt: 2% | ||
| Philippines: 1.3% | |||
| Iraq: 0.32% | |||
| Saudi Arabia: 95.7% | |||
| Sudan: 0.36% | |||
| United Kingdom: 0.32% | |||
| Comorbidities | Diabetes | 69.2% | |
| Hypertension | 64.3% | ||
| Heart Ischemic | 17.2% | ||
| Heart Failure | 5.0% | ||
| Cardiomyopathies | 1.3% | ||
| COPD | 2.0% | ||
| Heart Failure | 4.9% | ||
| Interstitial Lung Disease | 0.3% | ||
| Bronchial Asthma | 15.0% | ||
| Cerebrovascular | 4.2% | ||
| Neurologic (Dementia) | 4.2% | ||
| Cirrhosis | 1.3% | ||
| HIV | 0.0% | ||
| Liver Disease | 2.0% | ||
| Obesity | 5.5% | ||
| Others | Psychiatric History | 1.3% | |
| End Stage Renal | 11.0% | ||
| Hemodialysis | 4.5% | ||
| Cancer | 6.0% | ||
| Solid Organ Transplant | 5.5% | ||
| Hematopoietic Cell Transplant | 0.0% | ||
| Smoker | 0.3% | ||
| Pregnancy | 5.0% | ||
| Sick Cell | 0.3% | ||
| Shortness of Breath (SOB) | 85.7% | ||
| Fever | 55.0% | ||
| Hemoptysis | 1.0% | ||
| Diarrhea | 11.0% | ||
| Cough | 72.0% | ||
| Headache | 7.5% | ||
| Abdominal Pain | 8.0% | ||
| Myalgia | 11.0% | ||
| Loss of Smell or Taste | 8.0% | ||
| Temperature | 100.0% | ||
| Respiratory Rate | 13.6% | ||
| Pulse | 100.0% | ||
| Nausea or Vomiting | 8.0% | ||
| Diastolic BP | 100.0% | ||
| Systolic BP | 100.0% | ||
| Glasgow | 100% | ||
| Lab Parameters | LDH | 100.0% | |
| PaCO2 | 100.0% | ||
| HCO3 | |||
| PaO2 | |||
| pH | |||
| Lymphocytes | |||
| PaO2 | |||
| WBC | |||
| ALT | |||
| PTT | |||
| D-Dimer | |||
| Platelets | |||
| WBC | |||
| Hemoglobin | |||
| CRP | |||
| Ferritin | |||
| AST | |||
| NT-proBNP | |||
| PROCALCITONI | |||
| TROPONIN | |||
| Vitamin D | |||
| IL-6 | |||
| Blood Group | |||
| INR | |||
| Fibrinogen | |||
| PNN | |||
| Medications | Immunomodulators (Tocilizumab) | 80.0% | |
| Antiviral (Favipiravir, Kaletra–Ribavirin–Interferon) | 98.0% | ||
| Antibiotic | 92.0% | ||
| Anticoagulant (Clexan, Heparine) | 87.0% | ||
| X-ray | Presence of Consolidation | 72.0% | |
| Presence of Ground-Glass Opacities | |||
| Bilateral or Unilateral | |||
| Classes | LoS in Hospital | Patient Frequency Original | Patient Frequency After SMOTE-N |
|---|---|---|---|
| Deceased | Less than or equal to 3 weeks | 36 | 36 |
| Greater than 3 weeks | 24 | 36 | |
| Discharged | Less than or equal to 1 week | 84 | 84 |
| 1–2 weeks | 79 | 84 | |
| 2–3 weeks | 37 | 84 | |
| 3–4 weeks | 12 | 84 | |
| Greater than 4 weeks | 36 | 84 |
| Classifiers | Discharged Dataset | Deceased Dataset | ||||||
|---|---|---|---|---|---|---|---|---|
| F1 | Accuracy | Precision | Recall | F1 | Accuracy | Precision | Recall | |
| LR | 0.74 | 0.73 | 0.77 | 0.74 | 0.68 | 0.68 | 0.7 | 0.73 |
| RF | 0.73 | 0.71 | 0.76 | 0.72 | 0.68 | 0.68 | 0.7 | 0.73 |
| DT | 0.65 | 0.65 | 0.68 | 0.65 | 0.62 | 0.64 | 0.64 | 0.66 |
| AB | 0.62 | 0.61 | 0.63 | 0.62 | 0.61 | 0.64 | 0.61 | 0.62 |
| GB | 0.54 | 0.52 | 0.61 | 0.53 | 0.50 | 0.5 | 0.6 | 0.6 |
| TabT * | 0.92 | 0.73 | 0.83 | 0.93 | 0.84 | 0.77 | 0.75 | 0.98 |
| Dataset Type | LoS Category | Association Rules |
|---|---|---|
| Discharged dataset | LoS ≤ 1 Week | {Anticoagulant, Cough, Antibiotics, Antiviral} |
| {Cough, LDH > 225, Antibiotics, Antiviral} | ||
| {Anticoagulant, SOB, Immunomodulators, LDH > 225, Antibiotics, Platelets < 50,000} | ||
| {PaO2 (0 to 80), Anticoagulant, SOB, LDH > 225, Antibiotics} | ||
| LoS 1–2 Weeks | {Fever, DIMER (0 to 500), Immunomodulators, Antibiotics, Temperature (36 to 37.6)} | |
| {PaO2(0 to 80), Fever, Immunomodulators, LDH > 225, Antibiotics, Antiviral} | ||
| {Anticoagulant, Fever, FERRITIN < 792, Immunomodulators, Glasgow > 14, Platelets < 50,000} | ||
| {Anticoagulant, Fever, SOB, HTN, Glasgow > 14, Antiviral} | ||
| LoS 2–3 Weeks | {Fever, DIMER > 500, LDH > 225, Antiviral} | |
| {Anticoagulant, Fever, HTN, Diastolic BP (60 to 90), Antiviral} | ||
| {Anticoagulant, Fever, HTN, Immunomodulators, Diastolic BP (60 to 90)} | ||
| {CRP (6 to 100), Fever, LDH > 225, Antiviral} | ||
| LoS 3–4 Weeks | {Anticoagulant, Lymphocytes (1000 to 4000), Antibiotics, Respiratory Rate (20 to 28), PNN (1000 to 7700)} | |
| {Anticoagulant, HTN, Immunomodulators, Lymphocytes (1000 to 4000), Antibiotics, Respiratory Rate (20 to 28), Antiviral} | ||
| {HTN, Immunomodulators, Lymphocytes (1000 to 4000), Antibiotics, Respiratory Rate (20 to 28), Antiviral} | ||
| {Anticoagulant, Immunomodulators, Lymphocytes (1000 to 4000), PNN (1000 to 7700)} | ||
| LoS ≥ 4 Weeks | {Immunomodulators, Platelets < 50,000, Antiviral, abnormal X-ray} | |
| {Antibiotics, PTT > 14.5, Platelets < 50,000} | ||
| {Anticoagulant, Immunomodulators, Antiviral} | ||
| {PNN (1000 to 7700), PTT > 14.5, Platelets < 50,000, Antiviral} | ||
| Deceased dataset | LoS ≤ 3 Weeks | {SOB, Antibiotics, PTT > 14.5, Platelets < 50,000, TROPONIN (0 to 0.1)} |
| {SOB, Antibiotics, Glasgow > 14, PNN: 1000_7700, Antiviral} | ||
| {LDH > 225, Diastolic BP (60 to 90), Glasgow > 14, Antiviral} | ||
| {PaO2 (0 to 80), Cough, Antibiotics, Glasgow > 14, Platelets < 50,000} | ||
| LoS > 3 Weeks | {ALT (0 to 41), Diabetes, HTN, Immunomodulators, Antibiotics} | |
| {Ph (7.35 to 7.45), ALT (0 to 41), HTN, Immunomodulators, Antibiotics, Platelets < 50,000} | ||
| {ALT (0 to 41), SOB, HTN, Immunomodulators, Antibiotics, PTT > 14.5} | ||
| {ALT (0 to 41), SOB, HTN, Immunomodulators, Glasgow > 14, Antiviral} |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, F.; Ananbeh, O.; Malik, K.M.; Odayani, A.A.; Hussain, I.B.; Kaabia, N.; Aidaroos, A.A.; Saudagar, A.K.J. Towards Predicting Length of Stay and Identification of Cohort Risk Factors Using Self-Attention-Based Transformers and Association Mining: COVID-19 as a Phenotype. Diagnostics 2023, 13, 1760. https://doi.org/10.3390/diagnostics13101760
Alam F, Ananbeh O, Malik KM, Odayani AA, Hussain IB, Kaabia N, Aidaroos AA, Saudagar AKJ. Towards Predicting Length of Stay and Identification of Cohort Risk Factors Using Self-Attention-Based Transformers and Association Mining: COVID-19 as a Phenotype. Diagnostics. 2023; 13(10):1760. https://doi.org/10.3390/diagnostics13101760
Chicago/Turabian StyleAlam, Fakhare, Obieda Ananbeh, Khalid Mahmood Malik, Abdulrahman Al Odayani, Ibrahim Bin Hussain, Naoufel Kaabia, Amal Al Aidaroos, and Abdul Khader Jilani Saudagar. 2023. "Towards Predicting Length of Stay and Identification of Cohort Risk Factors Using Self-Attention-Based Transformers and Association Mining: COVID-19 as a Phenotype" Diagnostics 13, no. 10: 1760. https://doi.org/10.3390/diagnostics13101760
APA StyleAlam, F., Ananbeh, O., Malik, K. M., Odayani, A. A., Hussain, I. B., Kaabia, N., Aidaroos, A. A., & Saudagar, A. K. J. (2023). Towards Predicting Length of Stay and Identification of Cohort Risk Factors Using Self-Attention-Based Transformers and Association Mining: COVID-19 as a Phenotype. Diagnostics, 13(10), 1760. https://doi.org/10.3390/diagnostics13101760