
Adenomyosis and Its Possible Malignancy: A Review of the Literature


 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
PubMed Search Strategy
- Adenomyosis;
- Cancer (including Neoplasms);
- Endometriosis.
- From 2012 to 2023.
- Anatomy and histology;
- Etiology or pathogenesis;
- Management or organisation and administration;
- Symptoms;
- Imaging;
- Biomarkers;
- Histopathologies or pathology
- Management.
3. Pathogenesis
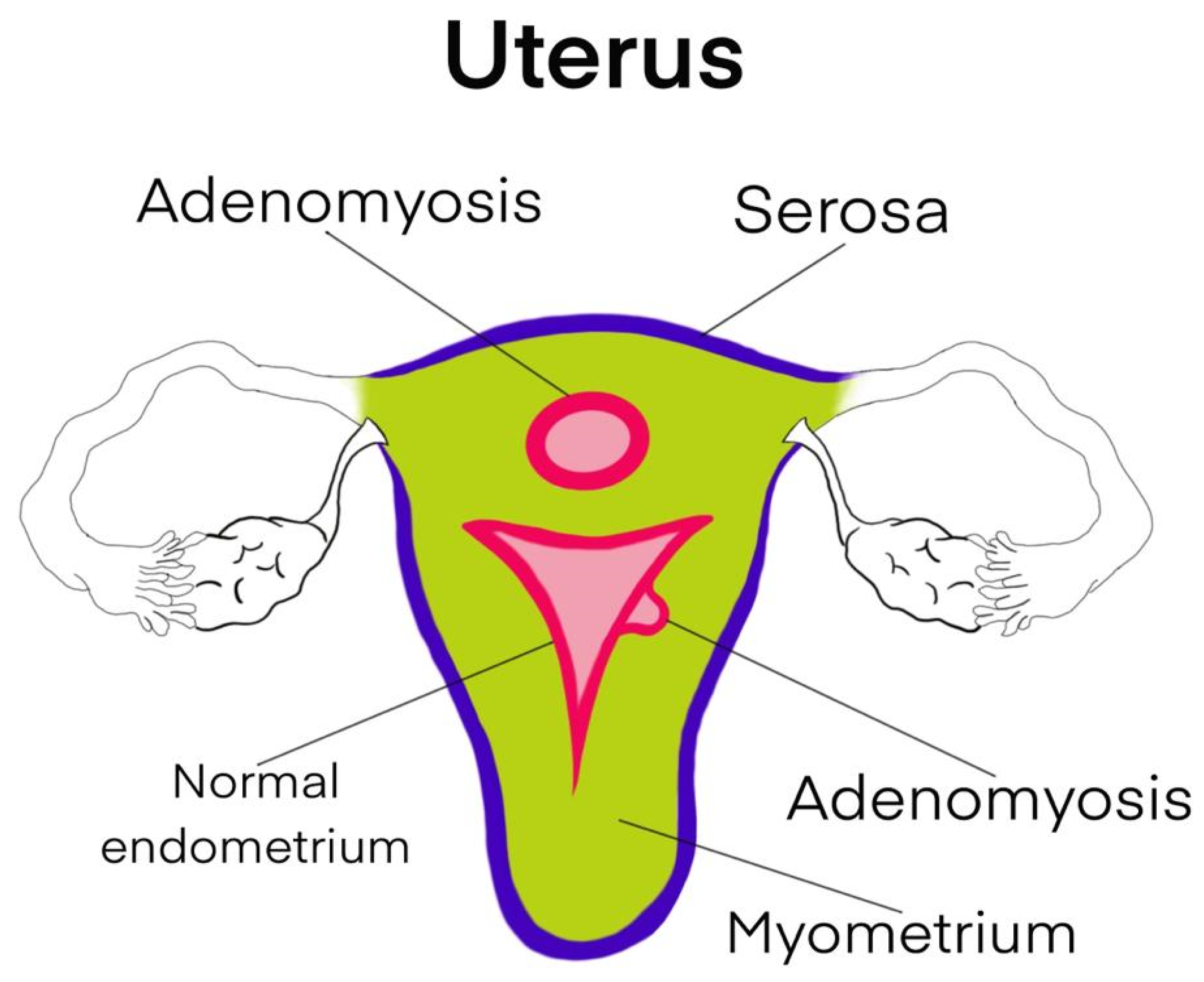
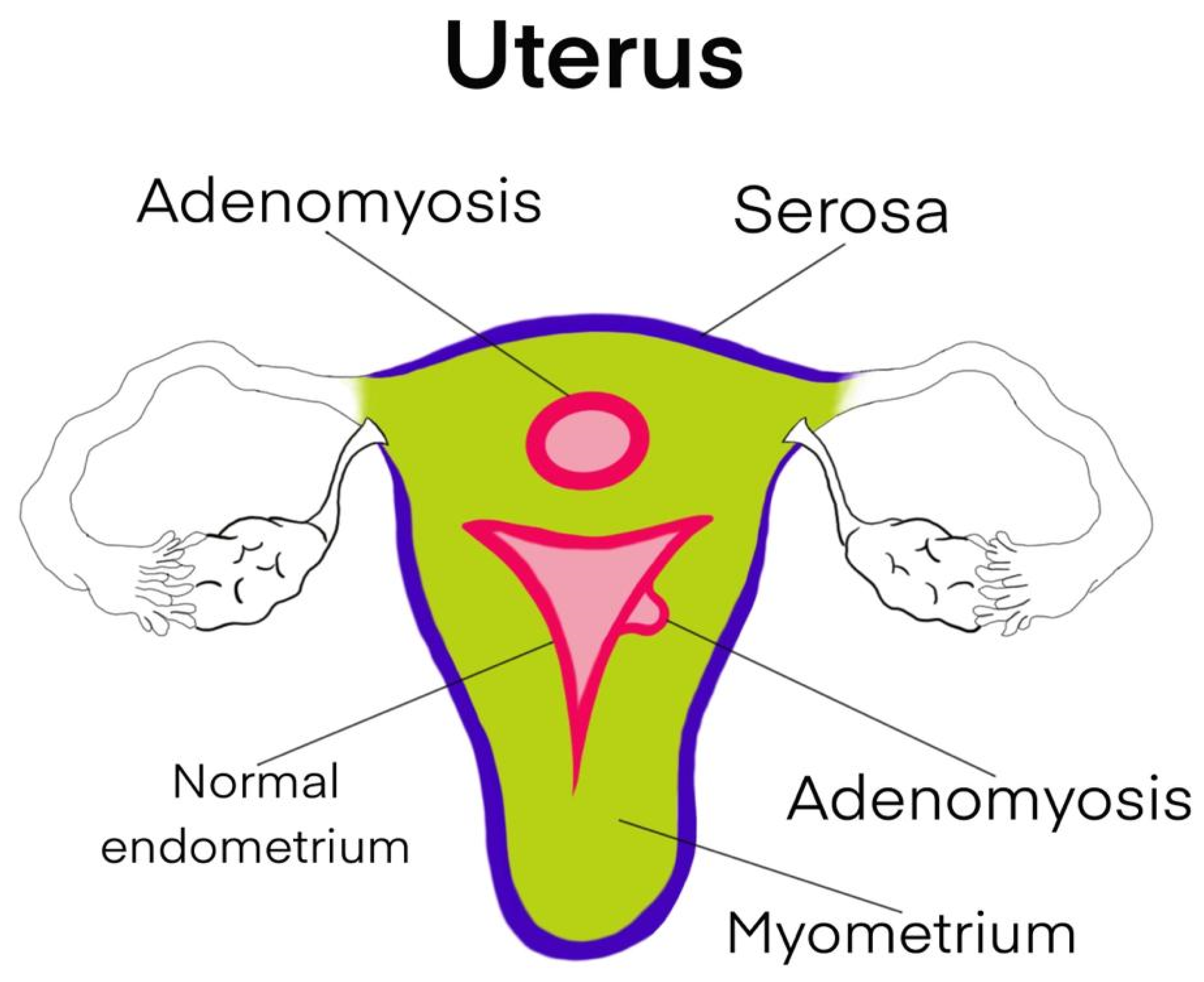
4. Anatomy
5. Diagnosis
5.1. Symptoms
5.2. Imaging and Biomarkers
5.3. Histopathological Examination
- Epithelial carcinomas;
- Other Mullerian type tumours, including Mullerian-type mucinous borderline tumours and serous borderline tumours;
- Sarcomas: adenosarcoma and endometrial stromal sarcoma [12].
6. Metastases
7. Associations with Other Types of Cancer
8. Differential Diagnosis
9. Management
10. Prognosis
11. Discussions
12. Future
13. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Y.; Li, N.; Zhang, R.; Bai, P. Primary low-grade extrauterine endometrial stromal sarcoma: Analysis of 10 cases with a review of the literature. World J. Surg. Oncol. 2022, 20, 17. [Google Scholar] [CrossRef]
- Chen, X.; Hamele-Bena, D.; Galic, V.L.; Liu-Jarin, X.; Ko, Y.C.; Herzog, T.; Wright, J.D.; Wright, T.C. Infiltrating adenomyosis of the cervix with features of a low-grade stromal sarcoma: A case report and a literature review. Int. J. Gynecol. Pathol. 2014, 33, 253–257. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Q.; Wang, W.; Yang, J.; Xia, J.; Wei, Y. Endometrioid adenocarcinoma arising in adenomyosis in a patient with pelvic organ prolapse-case report. BMC Womens Health 2023, 23, 150. [Google Scholar] [CrossRef]
- Baba, A.; Yamazoe, S.; Dogru, M.; Ogawa, M.; Takamatsu, K.; Miyauchi, J. Clear cell adenocarcinoma arising from adenomyotic cyst: A case report and literature review. J. Obstet. Gynaecol. Res. 2016, 42, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Provendier, A.; Angeles, M.A.; Meyrignac, O.; Illac, C.; Ducassou, A.; Martínez-Gómez, C.; Gladieff, L.; Martinez, A.; Ferron, G. Clear cell adenocarcinoma arising from the abdominal wall after cesarean section in a patient with uterine adenomyosis. J. Surg. Case Rep. 2020, 2020, rjaa070. [Google Scholar] [CrossRef] [PubMed]
- Giannella, L.; Marconi, C.; Di Giuseppe, J.; Delli Carpini, G.; Fichera, M.; Grelloni, C.; Giuliani, L.; Montanari, M.; Insinga, S.; Ciavattini, A. Malignant Transformation of Postmenopausal Endometriosis: A Systematic Review of the Literature. Cancers (Basel) 2021, 13, 4026. [Google Scholar] [CrossRef]
- Lee, S.J.; Park, J.Y. A Rare Case of Intramural Müllerian Adenosarcoma Arising from Adenomyosis of the Uterus. J. Pathol. Transl. Med. 2017, 51, 433–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, P.G.; Gulati, G.; Shintre, H.; Mannur, S.; Paul, G.; Mehta, S. Extrauterine adenomyoma: A review of the literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 228, 130–136. [Google Scholar] [CrossRef]
- Caramelo, O.; Marinho, C.; Rebelo, T.; Amaral, N.; Mota, F.; Xavier da Cunha, F.; Torgal, I. A case of endometrial stromal sarcoma with synchronous bilateral adenocarcinoma of ovary. Case Rep. Obstet. Gynecol. 2012, 2012, 687510. [Google Scholar] [CrossRef] [Green Version]
- Machida, H.; Maeda, M.; Cahoon, S.S.; Scannell, C.A.; Garcia-Sayre, J.; Roman, L.D.; Matsuo, K. Endometrial cancer arising in adenomyosis versus endometrial cancer coexisting with adenomyosis: Are these two different entities. Arch. Gynecol. Obstet. 2017, 295, 1459–1468. [Google Scholar] [CrossRef] [PubMed]
- Szubert, M.; Kozirog, E.; Wilczynski, J. Adenomyosis as a Risk Factor for Myometrial or Endometrial Neoplasms-Review. Int. J. Environ. Res. Public Health 2022, 19, 2294. [Google Scholar] [CrossRef]
- Higashiura, Y.; Kajihara, H.; Shigetomi, H.; Kobayashi, H. Identification of multiple pathways involved in the malignant transformation of endometriosis (Review). Oncol. Lett. 2012, 4, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, J.Y.; Jung, Y.Y.; Kim, H.S. Clinicopathological Characteristics and KRAS Mutation Status of Endometrial Mucinous Metaplasia and Carcinoma. Anticancer Res. 2018, 38, 2779–2786. [Google Scholar] [CrossRef]
- Santoro, A.; Angelico, G.; Inzani, F.; Spadola, S.; Arciuolo, D.; Valente, M.; Fiorentino, V.; Mulè, A.; Scambia, G.; Zannoni, G.F. The Many Faces of Endometriosis-Related Neoplasms in the Same Patient: A Brief Report. Gynecol. Obstet. Investig. 2020, 85, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Stefanko, D.P.; Eskander, R.; Aisagbonhi, O. Disseminated Endometriosis and Low-Grade Endometrioid Stromal Sarcoma in a Patient with a History of Uterine Morcellation for Adenomyosis. Case Rep. Obstet. Gynecol. 2020, 2020, 7201930. [Google Scholar] [CrossRef]
- Camboni, A.; Marbaix, E. Ectopic Endometrium: The Pathologist’s Perspective. Int. J. Mol. Sci. 2021, 22, 10974. [Google Scholar] [CrossRef] [PubMed]
- Cui, R.R.; Wright, J.D. Risk of Occult Uterine Sarcoma in Presumed Uterine Fibroids. Clin. Obstet. Gynecol. 2016, 59, 103–118. [Google Scholar] [CrossRef]
- Weigel, M.T.; Krämer, J.; Schem, C.; Wenners, A.; Alkatout, I.; Jonat, W.; Maass, N.; Mundhenke, C. Differential expression of MMP-2, MMP-9 and PCNA in endometriosis and endometrial carcinoma. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 160, 74–78. [Google Scholar] [CrossRef]
- Zhu, H.L.; Gao, S.Y.; Shen, D.H.; Cui, H. Clinicopathological Characteristics of Ten Patients with Atypical Glandular Hyperplasia Transformation of Adenomyosis. Chin. Med. J. (Engl.) 2016, 129, 364–366. [Google Scholar] [CrossRef]
- Nakai, Y.; Maeda, E.; Kanda, T.; Ikemura, M.; Ushiku, T.; Sasajima, Y.; Isshiki, S.; Abe, O. Uterine adenomyosis with extensive glandular proliferation: Case series of a rare imaging variant. Diagn Interv. Radiol. 2020, 26, 153–159. [Google Scholar] [CrossRef]
- Okimura, H.; Tatsumi, H.; Ito, F.; Yamashita, S.; Kokabu, T.; Kitawaki, J. Endometrioid carcinoma arising from diaphragmatic endometriosis treated with laparoscopy: A case report. J. Obstet. Gynaecol. Res. 2018, 44, 972–977. [Google Scholar] [CrossRef]
- Izumi, Y.; Yamamoto, T.; Matsunaga, N.; Ota, T.; Owaki, Y.; Shinohara, K.; Tsuzuki, T.; Suzuki, K. Endometrial cancer arising from adenomyosis: Case report and literature review of MRI findings. Radiol Case Rep 2020, 15, 427–430. [Google Scholar] [CrossRef]
- Tashima, L.; Hori, K.; Ono, H.; Nagano, T.; Nakatsuka, S.I.; Ito, K. Endometrioid adenocarcinoma originating simultaneously from endometrium, sites of adenomyosis and ovarian endometriosis: A case report and review of our cancer database. Int. J. Surg. Case Rep. 2017, 41, 226–229. [Google Scholar] [CrossRef]
- Tetikkurt, S.; Çelik, E.; Taş, H.; Cay, T.; Işik, S.; Usta, A.T. Coexistence of adenomyosis, adenocarcinoma, endometrial and myometrial lesions in resected uterine specimens. Mol. Clin. Oncol. 2018, 9, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Nama, N.; Cason, F.D.; Misra, S.; Hai, S.; Tucci, V.; Haq, F.; Love, J.; Ullah, A.; Peterson, P.; Grishko, F.F.; et al. Carcinosarcoma of the Uterus: A Study From the Surveillance Epidemiology and End Result (SEER) Database. Cureus 2020, 12, e10283. [Google Scholar] [CrossRef] [PubMed]
- Hermens, M.; van Altena, A.M.; Velthuis, I.; van de Laar, D.C.M.; Bulten, J.; van Vliet, H.A.A.M.; Siebers, A.G.; Bekkers, R.L.M. Endometrial Cancer Incidence in Endometriosis and Adenomyosis. Cancers (Basel) 2021, 13, 4592. [Google Scholar] [CrossRef] [PubMed]
- Strehl, J.D.; Wachter, D.L.; Fiedler, J.; Heimerl, E.; Beckmann, M.W.; Hartmann, A.; Agaimy, A. Pattern of SMARCB1 (INI1) and SMARCA4 (BRG1) in poorly differentiated endometrioid adenocarcinoma of the uterus: Analysis of a series with emphasis on a novel SMARCA4-deficient dedifferentiated rhabdoid variant. Ann. Diagn Pathol. 2015, 19, 198–202. [Google Scholar] [CrossRef]
- Taneichi, A.; Fujiwara, H.; Takahashi, Y.; Takei, Y.; Machida, S.; Saga, Y.; Takahashi, S.; Suzuki, M. Influences of uterine adenomyosis on muscle invasion and prognosis of endometrioid adenocarcinoma. Int. J. Gynecol. Cancer 2014, 24, 1429–1433. [Google Scholar] [CrossRef]
- Elbasateeny, S.S.; Salem, A.A.; Abdelsalam, W.A.; Salem, R.A. Immunohistochemical expression of cancer stem cell related markers CD44 and CD133 in endometrial cancer. Pathol. Res. Pract. 2016, 212, 10–16. [Google Scholar] [CrossRef]
- Angelico, G.; Santoro, A.; Straccia, P.; Inzani, F.; Cianfrini, F.; Spadola, S.; Arciuolo, D.; Valente, M.; D’Alessandris, N.; Mulè, A.; et al. Diagnostic and Prognostic Role of WT1 Immunohistochemical Expression in Uterine Carcinoma: A Systematic Review and Meta-Analysis across All Endometrial Carcinoma Histotypes. Diagnostics (Basel) 2020, 10, 637. [Google Scholar] [CrossRef] [PubMed]
- McCluggage, W.G. Pathologic Staging of Endometrial Carcinomas: Selected Areas of Difficulty. Adv. Anat. Pathol. 2018, 25, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, S.; Akaev, I.; Marani, C.; Chopra, M.; Yeoh, C.C. Immunohistochemical Expression of Different Subtypes of Cytokeratins by Endometrial Stromal Sarcoma. Appl. Immunohistochem. Mol. Morphol. 2019, 27, 466–470. [Google Scholar] [CrossRef] [Green Version]
- Vetvicka, V.; Fiala, L.; Garzon, S.; Buzzaccarini, G.; Terzic, M.; Laganà, A.S. Endometriosis and gynaecological cancers: Molecular insights behind a complex machinery. Prz. Menopauzalny 2021, 20, 201–206. [Google Scholar] [CrossRef]
- Saavalainen, L.; Lassus, H.; But, A.; Tiitinen, A.; Härkki, P.; Gissler, M.; Pukkala, E.; Heikinheimo, O. Risk of Gynecologic Cancer According to the Type of Endometriosis. Obstet. Gynecol. 2018, 131, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, T.I.; Krikunova, L.I.; Ryabchenko, N.I.; Mkrtchyan, L.S.; Khorokhorina, V.A.; Salnikova, L.E. Association of the apolipoprotein E 2 allele with concurrent occurrence of endometrial hyperplasia and endometrial carcinoma. Oxid. Med. Cell Longev. 2015, 2015, 593658. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, K.; Moeini, A.; Machida, H.; Scannell, C.A.; Casabar, J.K.; Kakuda, M.; Adachi, S.; Garcia-Sayre, J.; Ueda, Y.; Roman, L.D. Tumor Characteristics and Survival Outcome of Endometrial Cancer Arising in Adenomyosis: An Exploratory Analysis. Ann. Surg. Oncol. 2016, 23, 959–967. [Google Scholar] [CrossRef]
- Terzic, M.; Aimagambetova, G.; Kunz, J.; Bapayeva, G.; Aitbayeva, B.; Terzic, S.; Laganà, A.S. Molecular Basis of Endometriosis and Endometrial Cancer: Current Knowledge and Future Perspectives. Int. J. Mol. Sci. 2021, 22, 9274. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wei, Z.; Tang, Z.; Xue, C.; Yu, H.; Zhang, D.; Li, Y.; Liu, X.; Shi, Y.; Zhang, L.; et al. IL-37bΔ1-45 suppresses the migration and invasion of endometrial cancer cells by targeting the Rac1/NF-κB/MMP2 signal pathway. Lab. Investig. 2021, 101, 760–774. [Google Scholar] [CrossRef]

{kind=link}
| Pathogenesis | Genetics | Inflamation and Immunology | Hormones | Oxidative Stress |
|---|---|---|---|---|
| Adenomyosis with a similar role in malignancy | K-RAS mutation (V-Ki-RAS 2 Kirsten rat) CTNNB1 encoding B-cathenin ARID1A (A-rich interactive domain-containing protein 1A) p53 JAZF1-SuZ12 EPC1-PHF1 PTEN loss | COX2 TNF-α Toll-like receptors (TLR1) Nuclear factor Kappa (NF-KB) Macrophage IL-6 IL-10 | Oestrogen Poor response to progesteron | ROS Annexin ANXA2 EMT MMP2 and 9 (metalloproteinase) |
| Article | Number of Patients | Disease Free Survival (DSF) | Overall Survival | Prognosis | Mean Age (Range) | Muscle Invasion (≥½) | Influence of Adenomyosis on Cancer |
|---|---|---|---|---|---|---|---|
| Akiyo Taneichi [28] 2014 (A) | 362 ▪ 121 (33.4%)—with adenomyosis; ▪ 241 (66.6%)—no adenomyosis; | No difference | No difference | Similar | Adenomyosis 56 years (32–84) | Significant p < 0.05 ▪ 19.5%—adenomyosis; ▪ 10.1%— non-adenomyosis; | No significant influence on prognosis. |
| Hiroko Machida [10] 2017 (B) | 396 ▪ 46—EC-AIA (cancer arising from adenomyosis)—11.61%; ▪ 350—EC-A (cancer coexisting with adenomyosis)—88.39% | No difference | OS decreased in EC-AIA p = 0.031 | EC-AIA—poor prognosis | EC-AIA 58.9 years | Significant p < 0.001 ▪ EC-AIA—51.6%; ▪ EC-A—19.4% | Unclear |
| Marjolein Hermens [26] 2021 (C) | 129,872—enrolled ▪ 50,766 with endometriosis → 1827 developed endometrial cancer (3.59%); ▪ 85,051 with adenomyosis → 1408 developed endometrial cancer (1.65%) | No difference | No difference | Similar Adenomyosis has a poor response at hormonal treatment | Endometriosis 39 years (32–45) | Not investigated | The heterogeneity of the study is overdue, but endometriosis seems to have a greater influence than adenomyosis. |
| Koji Matsuo [36] 2015 (D) | 1340 enrolled—all with endometrial cancer ▪ EC-AIA = 46 patients (3.43%); ▪ nonEC-AIA = 1294 patients (96.57%) | Significant poorer in EC-AIA p = 0.014 | Significantly decreased in EC-AIA p = 0.001 | Poorer in EC-AIA | EC-AIA 58.9 years (58.9 ± 9.9) | ▪ EC-AIA—51.6%; ▪ nonEC-AIA—26.6%; Significant p = 0.002 | With a lack of hormonal receptors in the cancer developed from adenomyosis ther was therefore a reduced hormonal response. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moraru, L.; Mitranovici, M.-I.; Chiorean, D.M.; Moraru, R.; Caravia, L.; Tiron, A.T.; Cotoi, O.S. Adenomyosis and Its Possible Malignancy: A Review of the Literature. Diagnostics 2023, 13, 1883. https://doi.org/10.3390/diagnostics13111883
Moraru L, Mitranovici M-I, Chiorean DM, Moraru R, Caravia L, Tiron AT, Cotoi OS. Adenomyosis and Its Possible Malignancy: A Review of the Literature. Diagnostics. 2023; 13(11):1883. https://doi.org/10.3390/diagnostics13111883
Chicago/Turabian StyleMoraru, Liviu, Melinda-Ildiko Mitranovici, Diana Maria Chiorean, Raluca Moraru, Laura Caravia, Andreea Taisia Tiron, and Ovidiu Simion Cotoi. 2023. "Adenomyosis and Its Possible Malignancy: A Review of the Literature" Diagnostics 13, no. 11: 1883. https://doi.org/10.3390/diagnostics13111883
APA StyleMoraru, L., Mitranovici, M.-I., Chiorean, D. M., Moraru, R., Caravia, L., Tiron, A. T., & Cotoi, O. S. (2023). Adenomyosis and Its Possible Malignancy: A Review of the Literature. Diagnostics, 13(11), 1883. https://doi.org/10.3390/diagnostics13111883