
Comparison of Tooth Color and Enamel and Dentinal Thickness between Orthodontically Treated and Untreated Individuals

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Teeth
2.2. Color Measurements
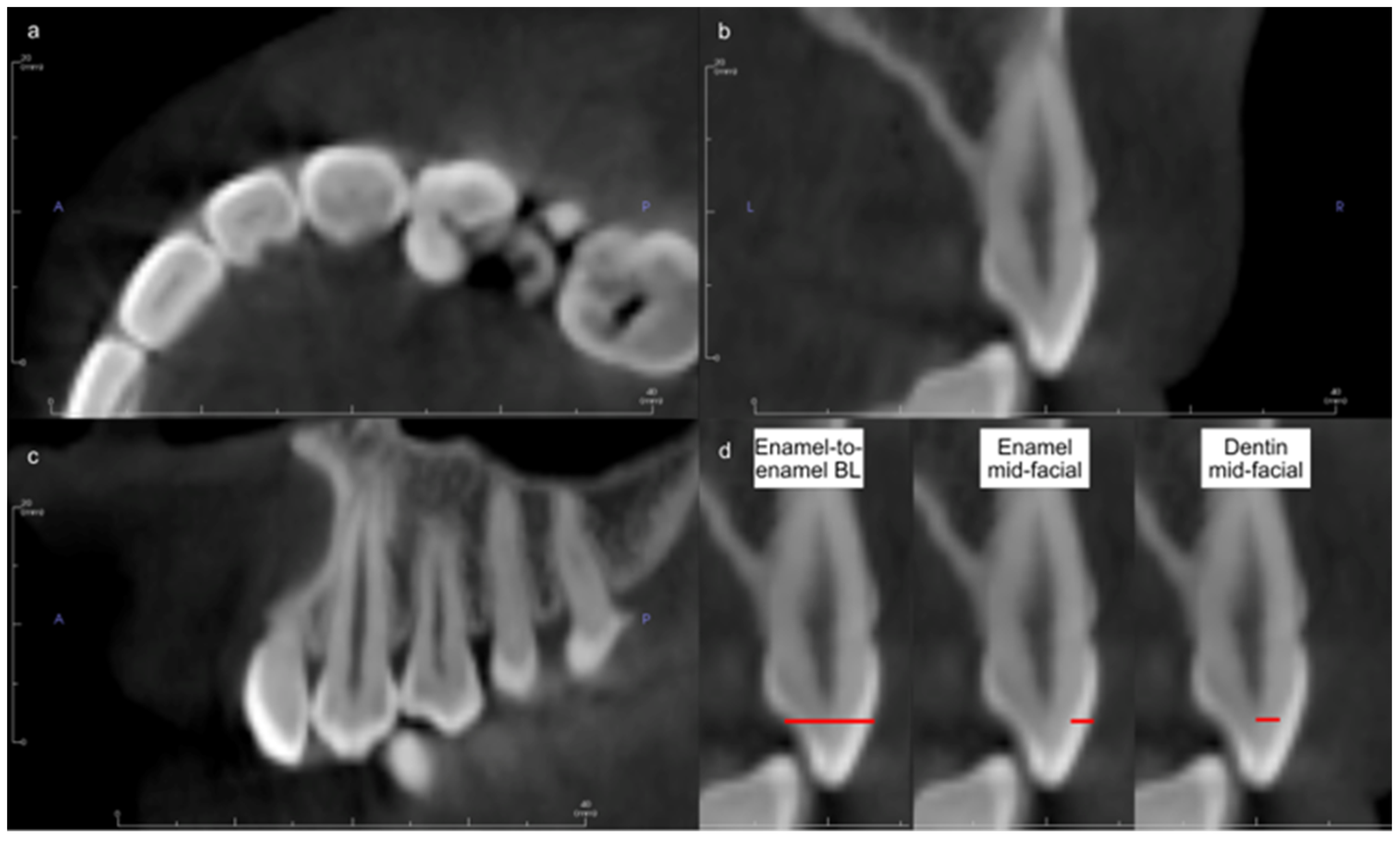
2.3. CBCT Measurements
2.4. Data Management and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Isiksal, E.; Hazar, S.; Akyalcin, S. Smile esthetics: Perception and comparison of treated and untreated smiles. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 8–16. [Google Scholar] [CrossRef]
- Baik, U.B.; Kim, H.; Chae, H.S.; Myung, J.Y.; Chun, Y.S. Teeth discoloration during orthodontic treatment. Korean J. Orthod. 2017, 47, 334–339. [Google Scholar] [CrossRef] [Green Version]
- Zachrisson, B.U.; Skogan, O.; Hoymyhr, S. Enamel cracks in debonded, debanded, and orthodontically untreated teeth. Am. J. Orthod. 1980, 77, 307–319. [Google Scholar] [CrossRef]
- Gorucu-Coskuner, H.; Atik, E.; Taner, T. Tooth color change due to different etching and debonding procedures. Angle Orthod. 2018, 88, 779–784. [Google Scholar] [CrossRef] [Green Version]
- Pinzan-Vercelino, C.R.M.; Lima, S.N.L.; Pereira, F.; Gurgel, J.A.; Silva, G.R.D.; Freitas, K.M.S. Efficacy of products for bleaching and whitening under orthodontic brackets. Dent. Press J. Orthod. 2022, 27, e2220325. [Google Scholar] [CrossRef]
- Tunca, M.; Kaya, Y. Effect of various orthodontic adhesives on enamel colour changes after fixed treatment. J. Orofac. Orthop. 2023, 84, 125–133. [Google Scholar] [CrossRef]
- Tabatabaian, F.; Beyabanaki, E.; Alirezaei, P.; Epakchi, S. Visual and digital tooth shade selection methods, related effective factors and conditions, and their accuracy and precision: A literature review. J. Esthet. Restor. Dent. 2021, 33, 1084–1104. [Google Scholar] [CrossRef]
- Hardan, L.; Bourgi, R.; Cuevas-Suarez, C.E.; Lukomska-Szymanska, M.; Monjaras-Avila, A.J.; Zarow, M.; Jakubowicz, N.; Jorquera, G.; Ashi, T.; Mancino, D.; et al. Novel Trends in Dental Color Match Using Different Shade Selection Methods: A Systematic Review and Meta-Analysis. Materials 2022, 15, 468. [Google Scholar] [CrossRef]
- Joiner, A. Tooth colour: A review of the literature. J. Dent. 2004, 32 (Suppl. 1), 3–12. [Google Scholar] [CrossRef]
- Paul, S.; Peter, A.; Pietrobon, N.; Hammerle, C.H. Visual and spectrophotometric shade analysis of human teeth. J. Dent. Res. 2002, 81, 578–582. [Google Scholar] [CrossRef]
- Da Silva, J.D.; Park, S.E.; Weber, H.P.; Ishikawa-Nagai, S. Clinical performance of a newly developed spectrophotometric system on tooth color reproduction. J. Prosthet. Dent. 2008, 99, 361–368. [Google Scholar] [CrossRef]
- Judeh, A.; Al-Wahadni, A. A comparison between conventional visual and spectrophotometric methods for shade selection. Quintessence Int. 2009, 40, e69–e79. [Google Scholar]
- Karamouzos, A.; Papadopoulos, M.A.; Kolokithas, G.; Athanasiou, A.E. Precision of in vivo spectrophotometric colour evaluation of natural teeth. J. Oral Rehabil. 2007, 34, 613–621. [Google Scholar] [CrossRef]
- Tung, F.F.; Goldstein, G.R.; Jang, S.; Hittelman, E. The repeatability of an intraoral dental colorimeter. J. Prosthet. Dent. 2002, 88, 585–590. [Google Scholar] [CrossRef]
- Eliades, T.; Kakaboura, A.; Eliades, G.; Bradley, T.G. Comparison of enamel colour changes associated with orthodontic bonding using two different adhesives. Eur. J. Orthod. 2001, 23, 85–90. [Google Scholar]
- Hwang, S.-P.K.I.-N.; Cho, J.-H.; Hwang, H.-S. Tooth color changes associated with the bracket bonding and debonding. Korean J. Orthod. 2006, 36, 114–124. [Google Scholar]
- Trakyalı, G.; Özdemir, F.I.; Arun, T. Enamel colour changes at debonding and after finishing procedures using five different adhesives. Eur. J. Orthod. 2009, 31, 397–401. [Google Scholar]
- Zaher, A.R.; Abdalla, E.M.; Abdel Motie, M.A.; Rehman, N.A.; Kassem, H.; Athanasiou, A.E. Enamel colour changes after debonding using various bonding systems. J. Orthod. 2012, 39, 82–88. [Google Scholar]
- Boncuk, Y.; Cehreli, Z.C.; Polat-Ozsoy, O. Effects of different orthodontic adhesives and resin removal techniques on enamel color alteration. Angle Orthod. 2014, 84, 634–641. [Google Scholar] [CrossRef]
- Kaya, Y.; Alkan, Ö.; Değirmenci, A.; Keskin, S. Long-term follow-up of enamel color changes after treatment with fixed orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 213–220. [Google Scholar]
- Chen, Q.; Zheng, X.; Chen, W.; Ni, Z.; Zhou, Y. Influence of orthodontic treatment with fixed appliances on enamel color: A systematic review. BMC Oral Health 2015, 15, 31. [Google Scholar]
- Hall, N.E.; Lindauer, S.J.; Tufekci, E.; Shroff, B. Predictors of variation in mandibular incisor enamel thickness. J. Am. Dent. Assoc. 2007, 138, 809–815. [Google Scholar] [CrossRef]
- Sindi, K.H.; Bubb, N.L.; Gutteridge, D.L.; Evans, J.A. In vitro enamel thickness measurements with ultrasound. Ultrasound Med. Biol. 2015, 41, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Mangal, S.; Mathew, S.; Sreenivasa Murthy, B.V.; Nagaraja, S.; Dinesh, K.; Ramesh, P. Cone-beam computed tomographic evaluation of remaining dentin thickness in bifurcated roots of maxillary first premolars after rotary instrumentation and post space preparation: An in vitro study. J. Conserv. Dent. 2018, 21, 63–67. [Google Scholar] [CrossRef]
- Algarni, A.; Kang, H.; Fried, D.; Eckert, G.J.; Hara, A.T. Enamel Thickness Determination by Optical Coherence Tomography: In vitro Validation. Caries Res. 2016, 50, 400–406. [Google Scholar] [CrossRef]
- Seeliger, J.; Machoy, M.; Koprowski, R.; Safranow, K.; Gedrange, T.; Woźniak, K. Enamel thickness before and after orthodontic treatment analysed in optical coherence tomography. BioMed Res. Int. 2017, 2017, 8390575. [Google Scholar]
- Kim, S.K.; Lee, H.S.; Park, S.W.; Lee, E.S.; de Josselin de Jong, E.; Jung, H.I.; Kim, B.I. Quantitative light-induced fluorescence technology for quantitative evaluation of tooth wear. J. Biomed. Opt. 2017, 22, 121701. [Google Scholar] [CrossRef]
- Bauss, O.; Rohling, J.; Meyer, K.; Kiliaridis, S. Pulp vitality in teeth suffering trauma during orthodontic therapy. Angle Orthod. 2009, 79, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, S.; Ajmera, S.; Ganeshkar, S.V. Volumetric pulp changes after orthodontic treatment determined by cone-beam computed tomography. J. Endod. 2014, 40, 1758–1763. [Google Scholar] [CrossRef]
- Sulieman, M. An overview of tooth discoloration: Extrinsic, intrinsic and internalized stains. Dent. Update 2005, 32, 463–464, 466–468, 471. [Google Scholar] [CrossRef]
- Watts, A.; Addy, M. Tooth discolouration and staining: A review of the literature. Br. Dent. J. 2001, 190, 309–316. [Google Scholar] [CrossRef]
- Shaikh, S.Y.; Shaikh, S.S. Direct Linear Measurement of Root Dentin Thickness and Dentin Volume Changes with Post Space Preparation: A Cone-Beam Computed Tomography Study. Contemp. Clin. Dent. 2018, 9, 77–82. [Google Scholar] [CrossRef]
- Karamouzos, A.; Athanasiou, A.E.; Papadopoulos, M.A.; Kolokithas, G. Tooth-color assessment after orthodontic treatment: A prospective clinical trial. Am. J. Orthod. Dentofacial Orthop. 2010, 138, 537.e1–537.e8; discussion 537–539. [Google Scholar] [CrossRef]
- Paravina, R.D. Performance assessment of dental shade guides. J. Dent. 2009, 37 (Suppl. 1), e15–e20. [Google Scholar] [CrossRef]
- Pintado-Palomino, K.; de Almeida, C.; Oliveira-Santos, C.; Pires-de-Souza, F.P.; Tirapelli, C. The effect of electronic cigarettes on dental enamel color. J. Esthet. Restor. Dent. 2019, 31, 160–165. [Google Scholar] [CrossRef]
- Perez Mdel, M.; Ghinea, R.; Rivas, M.J.; Yebra, A.; Ionescu, A.M.; Paravina, R.D.; Herrera, L.J. Development of a customized whiteness index for dentistry based on CIELAB color space. Dent. Mater. 2016, 32, 461–467. [Google Scholar] [CrossRef]
- Ahn, J.S.; Lee, Y.K. Color distribution of a shade guide in the value, chroma, and hue scale. J. Prosthet. Dent. 2008, 100, 18–28. [Google Scholar] [CrossRef]
- Paravina, R.D.; Perez, M.M.; Ghinea, R. Acceptability and perceptibility thresholds in dentistry: A comprehensive review of clinical and research applications. J. Esthet. Restor. Dent. 2019, 31, 103–112. [Google Scholar] [CrossRef]
- Wishney, M. Potential risks of orthodontic therapy: A critical review and conceptual framework. Aust. Dent. J. 2017, 62 (Suppl. 1), 86–96. [Google Scholar] [CrossRef] [Green Version]
- Al Maaitah, E.F.; Abu Omar, A.A.; Al-Khateeb, S.N. Effect of fixed orthodontic appliances bonded with different etching techniques on tooth color: A prospective clinical study. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 43–49. [Google Scholar] [CrossRef]
- Corekci, B.; Toy, E.; Ozturk, F.; Malkoc, S.; Ozturk, B. Effects of contemporary orthodontic composites on tooth color following short-term fixed orthodontic treatment: A controlled clinical study. Turk. J. Med. Sci. 2015, 45, 1421–1428. [Google Scholar]
- Jahanbin, A.; Ameri, H.; Khaleghimoghaddam, R. Effect of adhesive types on enamel discolouration around orthodontic brackets. Aust. Orthod. J. 2009, 25, 19–23. [Google Scholar]
- Joo, H.J.; Lee, Y.K.; Lee, D.Y.; Kim, Y.J.; Lim, Y.K. Influence of orthodontic adhesives and clean-up procedures on the stain susceptibility of enamel after debonding. Angle Orthod. 2011, 81, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Ye, C.; Zhao, Z.; Zhao, Q.; Du, X.; Ye, J.; Wei, X. Comparison of enamel discoloration associated with bonding with three different orthodontic adhesives and cleaning-up with four different procedures. J. Dent. 2013, 41 (Suppl. 5), e35–e40. [Google Scholar] [CrossRef]
- Wriedt, S.; Keller, S.; Wehrbein, H. The effect of debonding and/or bleaching on enamel color—An in-vitro study. J. Orofac. Orthop. 2008, 69, 169–176. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Montasser, M.A.; Abd El Latief, M.H.; Modica, G.G.; Scribante, A. Home Oral Care with Biomimetic Hydroxyapatite vs. Conventional Fluoridated Toothpaste for the Remineralization and Desensitizing of White Spot Lesions: Randomized Clinical Trial. Int. J. Environ. Res. Public. Health 2022, 19, 8676. [Google Scholar] [CrossRef]
- Scribante, A.; Dermenaki Farahani, M.R.; Marino, G.; Matera, C.; Rodriguez, Y.B.R.; Lanteri, V.; Butera, A. Biomimetic Effect of Nano-Hydroxyapatite in Demineralized Enamel before Orthodontic Bonding of Brackets and Attachments: Visual, Adhesion Strength, and Hardness in In Vitro Tests. Biomed. Res. Int. 2020, 2020, 6747498. [Google Scholar] [CrossRef] [Green Version]
- Falcone, M.E.; Kelly, J.R.; Rungruanganut, P. In Vivo Color Relationships Between the Maxillary Central Incisors and Canines as a Function of Age. Int. J. Prosthodont. 2016, 29, 496–502. [Google Scholar] [CrossRef] [Green Version]
- He, W.H.; Park, C.J.; Byun, S.; Tan, D.; Lin, C.Y.; Chee, W. Evaluating the relationship between tooth color and enamel thickness, using twin flash photography, cross-polarization photography, and spectrophotometer. J. Esthet. Restor. Dent. 2020, 32, 91–101. [Google Scholar]
- Ten Bosch, J.; Coops, J. Tooth color and reflectance as related to light scattering and enamel hardness. J. Dent. Res. 1995, 74, 374–380. [Google Scholar]
- Perez, M.M.; Herrera, L.J.; Carrillo, F.; Pecho, O.E.; Dudea, D.; Gasparik, C.; Ghinea, R.; Bona, A.D. Whiteness difference thresholds in dentistry. Dent. Mater. 2019, 35, 292–297. [Google Scholar] [CrossRef]
- Esan, T.A.; Olusile, A.O.; Akeredolu, P.A. Factors influencing tooth shade selection for completely edentulous patients. J. Contemp. Dent. Pract. 2006, 7, 80–87. [Google Scholar]
- Kailasam, V.; Rangarajan, H.; Easwaran, H.N.; Muthu, M.S. Proximal enamel thickness of the permanent teeth: A systematic review and meta-analysis. Am. J. Orthod. Dentofacial Orthop. 2021, 160, 793–804 e793. [Google Scholar] [CrossRef]
- Ragain, J.C., Jr.; Johnston, W.M. Color acceptance of direct dental restorative materials by human observers. Color Res. Appl. 2000, 25, 278–285. [Google Scholar] [CrossRef]

{kind=link}
| Thickness | Overall | Control | Case |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |
| Enamel-to-enamel buccolingual | 5.97 ± 1.91 | 5.89 ± 1.89 | 6.08 ± 1.94 |
| Enamel mid-facial | 1.24 ± 0.19 | 1.24 ± 0.19 | 1.24 ± 0.22 |
| Dentin mid-facial | 1.87 ± 0.84 | 1.85 ± 0.84 | 1.89 ± 0.84 |
| Measurement Method | Color Value | Overall (n = 228) Mean ± SD | Control (n = 124) Mean ± SD | Case (n = 104) Mean ± SD |
|---|---|---|---|---|
| Age | 23.91 | 24.29 | 23.46 | |
| Vita 3D-Master | L* | 56.86 ± 1.99 | 57.13 ± 2.03 | 56.54 ± 1.91 |
| Chroma | 11.35 ± 2.69 | 10.83 ± 2.58 | 11.97 ± 2.69 | |
| H degree | 80.94 ± 2.22 | 81.31 ± 2.38 | 80.5 ± 1.93 | |
| a* | 1.84 ± 0.69 | 1.69 ± 0.70 | 2.01 ± 0.65 | |
| b* | 11.2 ± 2.63 | 10.71 ± 2.53 | 11.8 ± 2.64 | |
| WID | 14.74 ± 4.74 | 15.77 ± 4.73 | 13.51 ± 4.47 | |
| Vita Easy Shade | L* | 59.6 ± 2.85 | 59.36 ± 2.98 | 59.89 ± 2.66 |
| Chroma | 11.25 ± 2.67 | 10.99 ± 2.69 | 11.55 ± 2.62 | |
| H degree | 83.6 ± 2.86 | 83.45 ± 3.03 | 83.79 ± 2.66 | |
| a* | 1.29 ± 0.69 | 1.31 ± 0.73 | 1.29 ± 0.66 | |
| b* | 11.15 ± 2.62 | 10.89 ± 2.64 | 11.45 ± 2.58 | |
| WID | 17.56 ± 4.90 | 17.69 ± 5.04 | 17.41 ± 4.75 |
| Color Value | Control Median (IQR) | Case Median (IQR) | p Value * | |
|---|---|---|---|---|
| Vita 3D-Master | L* | 56.6 (1.8) | 56.6 (3.4) | 0.066 |
| Chroma | 11.0 (2.9) | 11.6 (3.5) | 0.001 * | |
| H degree | 81.9 (3.6) | 80.2 (2.5) | 0.002 * | |
| a* | 1.6 (0.8) | 2.0 (0.9) | 0.001 * | |
| b* | 10.9 (2.7) | 11.4 (3.4) | 0.001 * | |
| WID | 16.3 (5.5) | 12.5 (6.6) | 0.001 * | |
| Vita Easy Shade | L* | 60.6 (5.1) | 61.3 (3.6) | 0.179 |
| Chroma | 10.5 (3.4) | 11.0 (3.4) | 0.131 | |
| H degree | 83.5 (3.6) | 83.6 (3.6) | 0.511 | |
| a* | 1.1 (0.8) | 1.1 (0.8) | 0.989 | |
| b* | 10.5 (3.4) | 10.9 (3.5) | 0.115 | |
| WID | 16.5 (5.4) | 16.5 (5.4) | 0.635 |
| Color Value | Male (n = 120) Median (IQR) | Female (n = 108) Median (IQR) | p Value * | |
|---|---|---|---|---|
| Vita 3D-Master | L* | 57.1 (2.7) | 56.4 (3.4) | 0.012 * |
| Chroma | 11.0 (4.2) | 11.0 (3) | 0.001 * | |
| H degree | 81.9 (2.5) | 81.1 (2.5) | 0.257 | |
| a* | 1.6 (0.9) | 1.6 (0.8) | 0.030 * | |
| b* | 10.9 (3.9) | 10.9 (2.9) | 0.001 * | |
| WID | 16.30 (6.78) | 16.30 (5.45) | 0.001 * | |
| Vita Easy Shade | L* | 61.3 (3.6) | 60.6 (5.1) | 0.399 |
| Chroma | 11.0 (4.2) | 10.5 (1.8) | 0.008 * | |
| H degree | 83.6 (3.6) | 83.5 (3.6) | 0.859 | |
| a* | 1.1 (0.8) | 1.1 (0.8) | 0.481 | |
| b* | 10.9 (4.2) | 10.5 (2) | 0.009 * | |
| WID | 16.30 (5.37) | 17.07 (5.37) | 0.128 |
| Control Median (IQR) | Treatment Median (IQR) | p Value * | |
|---|---|---|---|
| Enamel-to-enamel buccolingual | 5.37 (2.79) | 5.50 (3.52) | 0.507 |
| Enamel mid-facial | 1.22 (0.25) | 1.21 (0.27) | 0.803 |
| Dentin mid-facial | 1.53 (1.02) | 1.55 (1.48) | 0.656 |
| Male Median (IQR) | Female Median (IQR) | p Value * | |
|---|---|---|---|
| Enamel-to-enamel buccolingual | 5.46 (3.58) | 5.37 (2.91) | 0.685 |
| Enamel mid-facial | 1.22 (0.25) | 1.22 (0.36) | 0.603 |
| Dentin mid-facial | 1.57 (1.40) | 1.50 (1.12) | 0.538 |
| Thickness | Overall | ||||||
|---|---|---|---|---|---|---|---|
| L | Chroma | H Degree | a | b | WID | ||
| Enamel-to-enamel buccolingual | VM | −0.216 * | 0.315 * | −0.267 * | 0.367 * | 0.308 * | −0.385 * |
| VE | −0.414 * | 0.418 * | −0.512 * | 0.521 * | 0.417 * | −0.486 * | |
| Enamel mid-facial | VM | −0.024 | 0.211 * | 0.000 | 0.157 | 0.211 * | −0.228 * |
| VE | −0.270 * | 0.292 * | −0.335 * | 0.339 * | 0.292 * | −0.308 * | |
| Dentin mid-facial | VM | −0.255 * | 0.258 * | −0.298 * | 0.351 * | 0.252 * | −0.340 * |
| VE | −3.90 * | 0.374 * | −0.485 * | 0.486 * | 0.372 * | −0.453 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hakami, Z.; Marghalani, H.Y.; Hedad, I.; Khawaji, M.; Abutaleb, G.; Hakami, A.; Almoammar, S.; Alshehri, A. Comparison of Tooth Color and Enamel and Dentinal Thickness between Orthodontically Treated and Untreated Individuals. Diagnostics 2023, 13, 2066. https://doi.org/10.3390/diagnostics13122066
Hakami Z, Marghalani HY, Hedad I, Khawaji M, Abutaleb G, Hakami A, Almoammar S, Alshehri A. Comparison of Tooth Color and Enamel and Dentinal Thickness between Orthodontically Treated and Untreated Individuals. Diagnostics. 2023; 13(12):2066. https://doi.org/10.3390/diagnostics13122066
Chicago/Turabian StyleHakami, Zaki, Hussain YA Marghalani, Ismaeel Hedad, Mazen Khawaji, Ghadah Abutaleb, Amjad Hakami, Salem Almoammar, and Abdulrahman Alshehri. 2023. "Comparison of Tooth Color and Enamel and Dentinal Thickness between Orthodontically Treated and Untreated Individuals" Diagnostics 13, no. 12: 2066. https://doi.org/10.3390/diagnostics13122066