
Clinical Impact of the BIOFIRE Blood Culture Identification 2 Panel in Adult Patients with Bloodstream Infection: A Multicentre Observational Study in the United Arab Emirates

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Sample Collection and Processing
2.3. Laboratory Methods
2.3.1. Automated Blood Culture and Conventional Microbiological Testing
2.3.2. BIOFIRE Blood Culture Identification 2 (BCID2) Panel
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Detected Pathogens’ Characteristics
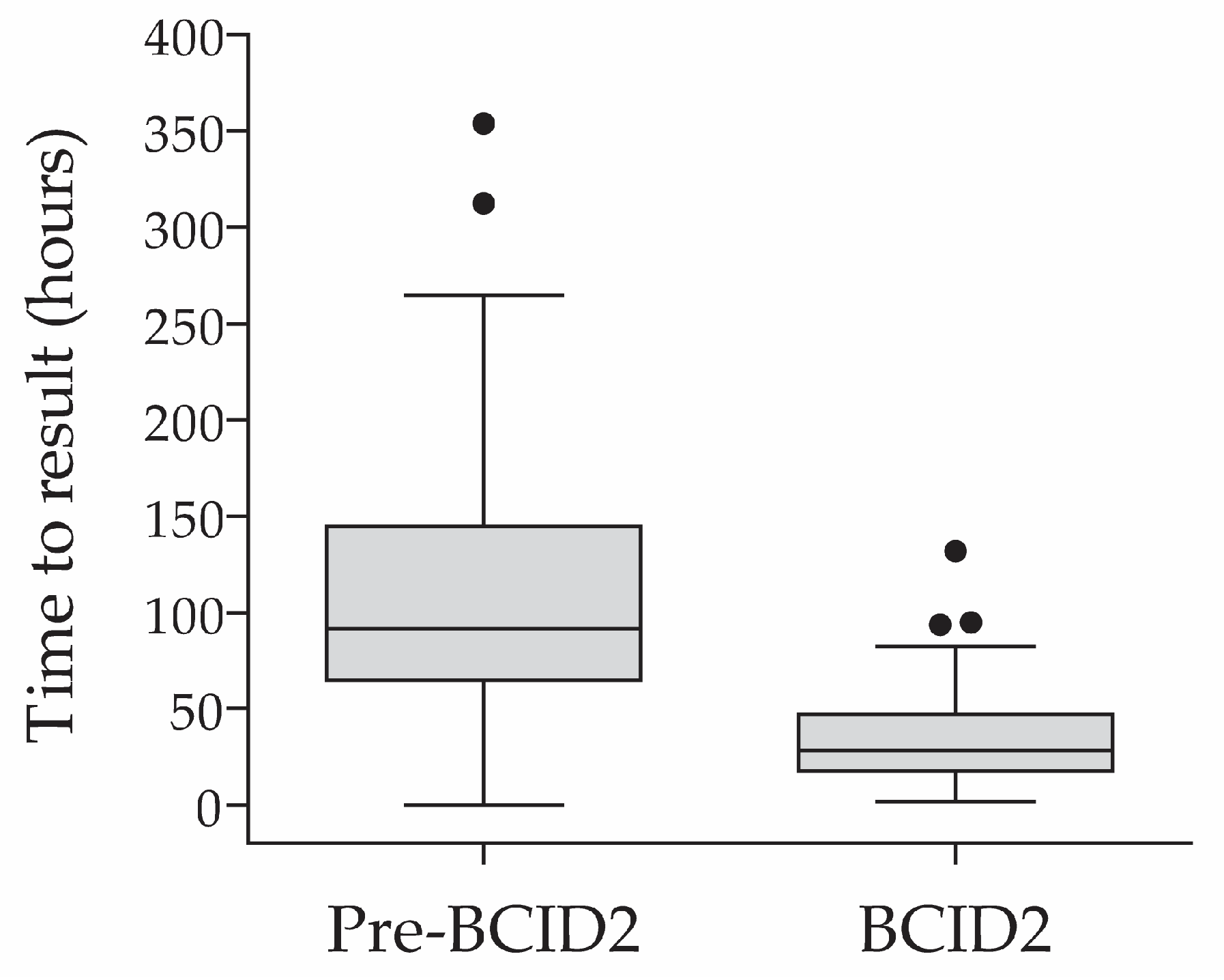
3.3. Time to Result Informing Targeted Therapy in the Pre-BCID2 vs. BCID2 Cohorts
3.4. Secondary Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goto, M.; Al-Hasan, M.N. Overall Burden of Bloodstream Infection and Nosocomial Bloodstream Infection in North America and Europe. Clin. Microbiol. Infect. 2013, 19, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Jaschinski, U.; Wittebole, X.; Szakmany, T.; Lipman, J.; Ñamendys-Silva, S.A.; Martin-Loeches, I.; Leone, M.; Lupu, M.-N.; Vincent, J.-L.; et al. Sepsis in Intensive Care Unit Patients: Worldwide Data From the Intensive Care over Nations Audit. Open Forum Infect. Dis. 2018, 5, ofy313. [Google Scholar] [CrossRef]
- Martinez, R.M.; Wolk, D.M. Bloodstream Infections. Microbiol. Spectr. 2016, 4, 653–689. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K.; International Forum of Acute Care Trialists. Assessment of Global Incidence and Mortality of Hospital-Treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef]
- McNamara, J.F.; Righi, E.; Wright, H.; Hartel, G.F.; Harris, P.N.A.; Paterson, D.L. Long-Term Morbidity and Mortality Following Bloodstream Infection: A Systematic Literature Review. J. Infect. 2018, 77, 1–8. [Google Scholar] [CrossRef]
- Tabah, A.; Buetti, N.; Staiquly, Q.; Ruckly, S.; Akova, M.; Aslan, A.T.; Leone, M.; Conway Morris, A.; Bassetti, M.; Arvaniti, K.; et al. Epidemiology and Outcomes of Hospital-Acquired Bloodstream Infections in Intensive Care Unit Patients: The EUROBACT-2 International Cohort Study. Intensive Care Med. 2023, 49, 178–190. [Google Scholar] [CrossRef]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control Antimicrobial Stewardship. Available online: https://www.ecdc.europa.eu/en/publications-data/directory-guidance-prevention-and-control/prudent-use-antibiotics/antimicrobial (accessed on 22 November 2022).
- Timsit, J.-F.; Ruppé, E.; Barbier, F.; Tabah, A.; Bassetti, M. Bloodstream Infections in Critically Ill Patients: An Expert Statement. Intensive Care Med. 2020, 46, 266–284. [Google Scholar] [CrossRef] [PubMed]
- Lamy, B.; Sundqvist, M.; Idelevich, E.A.; ESCMID Study Group for Bloodstream Infections, Endocarditis and Sepsis (ESGBIES). Bloodstream Infections—Standard and Progress in Pathogen Diagnostics. Clin. Microbiol. Infect. 2020, 26, 142–150. [Google Scholar] [CrossRef]
- Seymour, C.W.; Gesten, F.; Prescott, H.C.; Friedrich, M.E.; Iwashyna, T.J.; Phillips, G.S.; Lemeshow, S.; Osborn, T.; Terry, K.M.; Levy, M.M. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. N. Engl. J. Med. 2017, 376, 2235–2244. [Google Scholar] [CrossRef]
- Kadri, S.S.; Lai, Y.L.; Warner, S.; Strich, J.R.; Babiker, A.; Ricotta, E.E.; Demirkale, C.Y.; Dekker, J.P.; Palmore, T.N.; Rhee, C.; et al. Inappropriate Empirical Antibiotic Therapy for Bloodstream Infections Based on Discordant In-Vitro Susceptibilities: A Retrospective Cohort Analysis of Prevalence, Predictors, and Mortality Risk in US Hospitals. Lancet Infect. Dis. 2021, 21, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Peri, A.M.; Ling, W.; Furuya-Kanamori, L.; Harris, P.N.A.; Paterson, D.L. Performance of BioFire Blood Culture Identification 2 Panel (BCID2) for the Detection of Bloodstream Pathogens and Their Associated Resistance Markers: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy Studies. BMC Infect. Dis. 2022, 22, 794. [Google Scholar] [CrossRef] [PubMed]
- Peri, A.M.; Bauer, M.J.; Bergh, H.; Butkiewicz, D.; Paterson, D.L.; Harris, P.N. Performance of the BioFire Blood Culture Identification 2 Panel for the Diagnosis of Bloodstream Infections. Heliyon 2022, 8, e09983. [Google Scholar] [CrossRef]
- Berinson, B.; Both, A.; Berneking, L.; Christner, M.; Lütgehetmann, M.; Aepfelbacher, M.; Rohde, H. Usefulness of BioFire FilmArray BCID2 for Blood Culture Processing in Clinical Practice. J. Clin. Microbiol. 2021, 59, e0054321. [Google Scholar] [CrossRef]
- Caméléna, F.; Péan de Ponfilly, G.; Pailhoriès, H.; Bonzon, L.; Alanio, A.; Poncin, T.; Lafaurie, M.; Dépret, F.; Cambau, E.; Godreuil, S.; et al. Multicenter Evaluation of the FilmArray Blood Culture Identification 2 Panel for Pathogen Detection in Bloodstream Infections. Microbiol. Spectr. 2023, 11, e0254722. [Google Scholar] [CrossRef] [PubMed]
- El Sherif, H.M.; Elsayed, M.; El-Ansary, M.R.; Aboshanab, K.M.; El Borhamy, M.I.; Elsayed, K.M. BioFire FilmArray BCID2 versus VITEK-2 System in Determining Microbial Etiology and Antibiotic-Resistant Genes of Pathogens Recovered from Central Line-Associated Bloodstream Infections. Biology 2022, 11, 1573. [Google Scholar] [CrossRef]
- Holma, T.; Torvikoski, J.; Friberg, N.; Nevalainen, A.; Tarkka, E.; Antikainen, J.; Martelin, J.J. Rapid Molecular Detection of Pathogenic Microorganisms and Antimicrobial Resistance Markers in Blood Cultures: Evaluation and Utility of the next-Generation FilmArray Blood Culture Identification 2 Panel. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 363–371. [Google Scholar] [CrossRef]
- Sparks, R.; Balgahom, R.; Janto, C.; Polkinghorne, A.; Branley, J. Evaluation of the BioFire Blood Culture Identification 2 Panel and Impact on Patient Management and Antimicrobial Stewardship. Pathology 2021, 53, 889–895. [Google Scholar] [CrossRef]
- Claeys, K.C.; Schlaffer, K.; Smith, R.; Hitchcock, S.; Jiang, Y.; Evans, S.; Johnson, J.K.; Leekha, S. Day at the Races: Comparing BioFire FilmArray Blood Culture ID Panels with Verigene Blood Culture Panel in Gram-Negative Bloodstream Infections Using DOOR-MAT Analysis. Clin. Infect. Dis. 2021, 73, 1103–1106. [Google Scholar] [CrossRef]
- Altun, O.; Almuhayawi, M.; Ullberg, M.; Özenci, V. Clinical Evaluation of the FilmArray Blood Culture Identification Panel in Identification of Bacteria and Yeasts from Positive Blood Culture Bottles. J. Clin. Microbiol. 2013, 51, 4130–4136. [Google Scholar] [CrossRef]
- Verroken, A.; Despas, N.; Rodriguez-Villalobos, H.; Laterre, P.-F. The Impact of a Rapid Molecular Identification Test on Positive Blood Cultures from Critically Ill with Bacteremia: A Pre-Post Intervention Study. PLoS ONE 2019, 14, e0223122. [Google Scholar] [CrossRef] [PubMed]
- Muzzi, M.; Viaggi, B.; Fabbri, S.; Bechi, L.; Scirè-Calabrisotto, C.; Villa, G.; Romagnoli, S. The Impact of Fast Microbiology in Intensive Care Units in the Era of Antibiotic Resistance: An Observational Retrospective Study. Curr. Microbiol. 2022, 79, 79. [Google Scholar] [CrossRef] [PubMed]
- Rule, R.; Paruk, F.; Becker, P.; Neuhoff, M.; Chausse, J.; Said, M. Diagnostic Accuracy of the BioFire FilmArray Blood Culture Identification Panel When Used in Critically Ill Patients with Sepsis. J. Microbiol. Methods 2021, 189, 106303. [Google Scholar] [CrossRef] [PubMed]
- Schumann, J.; Johanns, U.; Ahmad-Nejad, P.; Ghebremedhin, B.; Woebker, G. The Impact of the FilmArray-Based Detection of Microbial Pathogens from Positive Blood Culture Vials on the Time to Optimal Antimicrobial Regimen in Intensive Care Units of the Helios University Clinic Wuppertal, Germany. J. Clin. Med. 2021, 10, 5880. [Google Scholar] [CrossRef]
- Donnars, A.; Mahieu, R.; Declerck, C.; Chenouard, R.; Lemarié, C.; Pailhoriès, H.; Requin, J.; Kempf, M.; Eveillard, M. BIOFIRE® Blood Culture IDentification 2 (BCID2) Panel for Early Adaptation of Antimicrobial Therapy in Adult Patients with Bloodstream Infections: A Real-Life Experience. Diagn. Microbiol. Infect. Dis. 2023, 105, 115858. [Google Scholar] [CrossRef]
- Banerjee, R.; Teng, C.B.; Cunningham, S.A.; Ihde, S.M.; Steckelberg, J.M.; Moriarty, J.P.; Shah, N.D.; Mandrekar, J.N.; Patel, R. Randomized Trial of Rapid Multiplex Polymerase Chain Reaction–Based Blood Culture Identification and Susceptibility Testing. Clin. Infect. Dis. 2015, 61, 1071–1080. [Google Scholar] [CrossRef]
- Rule, R.; Paruk, F.; Becker, P.; Neuhoff, M.; Chausse, J.; Said, M. Clinical Utility of the BioFire FilmArray Blood Culture Identification Panel in the Adjustment of Empiric Antimicrobial Therapy in the Critically Ill Septic Patient. PLoS ONE 2021, 16, e0254389. [Google Scholar] [CrossRef]
- Bork, J.T.; Leekha, S.; Heil, E.L.; Zhao, L.; Badamas, R.; Johnson, J.K. Rapid Testing Using the Verigene Gram-Negative Blood Culture Nucleic Acid Test in Combination with Antimicrobial Stewardship Intervention against Gram-Negative Bacteremia. Antimicrob. Agents Chemother. 2015, 59, 1588–1595. [Google Scholar] [CrossRef]
- Huang, A.M.; Newton, D.; Kunapuli, A.; Gandhi, T.N.; Washer, L.L.; Isip, J.; Collins, C.D.; Nagel, J.L. Impact of Rapid Organism Identification via Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Combined with Antimicrobial Stewardship Team Intervention in Adult Patients with Bacteremia and Candidemia. Clin. Infect. Dis. 2013, 57, 1237–1245. [Google Scholar] [CrossRef]
- Beganovic, M.; Timbrook, T.T.; Wieczorkiewicz, S.M. Predictors of Time to Effective and Optimal Antimicrobial Therapy in Patients With Positive Blood Cultures Identified via Molecular Rapid Diagnostic Testing. Open Forum Infect. Dis. 2019, 6, ofy350. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Moreno, R. Clinical review: Scoring systems in the critically ill. Crit. Care 2010, 14, 207. [Google Scholar] [CrossRef]
- Doern, G.V.; Carroll, K.C.; Diekema, D.J.; Garey, K.W.; Rupp, M.E.; Weinstein, M.P.; Sexton, D.J. Practical Guidance for Clinical Microbiology Laboratories: A Comprehensive Update on the Problem of Blood Culture Contamination and a Discussion of Methods for Addressing the Problem. Clin. Microbiol. Rev. 2019, 33, e00009-19. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.M.; Binnicker, M.J.; Campbell, S.; Carroll, K.C.; Chapin, K.C.; Gilligan, P.H.; Gonzalez, M.D.; Jerris, R.C.; Kehl, S.C.; Patel, R.; et al. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiology. Clin. Infect. Dis. 2018, 67, 813–816. [Google Scholar] [CrossRef] [PubMed]
- Clinical Laboratory and Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; CLSI Supplement M100, Clinical Laboratory and Standards Institute: Wayne, PA, USA, 2020; ISBN 978-1-68440-067-6. [Google Scholar]
- Zadka, H.; Raykhshtat, E.; Uralev, B.; Bishouty, N.; Weiss-Meilik, A.; Adler, A. The Implementation of Rapid Microbial Identification via MALDI-ToF Reduces Mortality in Gram-Negative but Not Gram-Positive Bacteremia. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2053–2059. [Google Scholar] [CrossRef] [PubMed]
- Timbrook, T.T.; Morton, J.B.; McConeghy, K.W.; Caffrey, A.R.; Mylonakis, E.; LaPlante, K.L. The Effect of Molecular Rapid Diagnostic Testing on Clinical Outcomes in Bloodstream Infections: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2017, 64, 15–23. [Google Scholar] [CrossRef]
- Adam, K.M.; Abomughaid, M.M. Prevalence of Methicillin-Resistant in Saudi Arabia Revisited: A Meta-Analysis. Open Public Health J. 2018, 11. [Google Scholar] [CrossRef]
- Aljeldah, M.M. Prevalence of Methicillin-Resistant Staphylococcus Aureus (MRSA) in Saudi Arabia: A Systematic Review. J. Pure Appl. Microbiol. 2020, 14, 37–46. [Google Scholar] [CrossRef]
- García-Rivera, C.; Parra-Grande, M.; Merino, E.; Boix, V.; Rodríguez, J.C. Concordance of the Filmarray Blood Culture Identification Panel 2 and Classical Microbiological Methods in a Bacteriemia Diagnostic Unit. Diagn. Microbiol. Infect. Dis. 2022, 104, 115787. [Google Scholar] [CrossRef]
- Blaschke, A.J.; Heyrend, C.; Byington, C.L.; Fisher, M.A.; Barker, E.; Garrone, N.F.; Thatcher, S.A.; Pavia, A.T.; Barney, T.; Alger, G.D.; et al. Rapid Identification of Pathogens from Positive Blood Cultures by Multiplex Polymerase Chain Reaction Using the FilmArray System. Diagn. Microbiol. Infect. Dis. 2012, 74, 349–355. [Google Scholar] [CrossRef]
- Southern, T.R.; VanSchooneveld, T.C.; Bannister, D.L.; Brown, T.L.; Crismon, A.S.; Buss, S.N.; Iwen, P.C.; Fey, P.D. Implementation and Performance of the BioFire FilmArray® Blood Culture Identification Panel with Antimicrobial Treatment Recommendations for Bloodstream Infections at a Midwestern Academic Tertiary Hospital. Diagn. Microbiol. Infect. Dis. 2015, 81, 96–101. [Google Scholar] [CrossRef]
- Fiori, B.; D’Inzeo, T.; Giaquinto, A.; Menchinelli, G.; Liotti, F.M.; de Maio, F.; De Angelis, G.; Quaranta, G.; Nagel, D.; Tumbarello, M.; et al. Optimized Use of the MALDI BioTyper System and the FilmArray BCID Panel for Direct Identification of Microbial Pathogens from Positive Blood Cultures. J. Clin. Microbiol. 2016, 54, 576–584. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pre-BCID2 Cohort (n = 99) | BCID2 Cohort (n = 86) | p-Value | |
|---|---|---|---|
| Study population per centre, N (%) | <0.0001 | ||
| Rashid Hospital | 77 (77.8%) | 37 (43.0%) | |
| Sheikh Khalifa General Hospital | 13 (13.1%) | 43 (50.0%) | |
| Mediclinic City Hospital | 9 (9.1%) | 6 (7.0%) | |
| Age in years, median (IQR) | 56 (40–65) | 65 (45–79) | 0.001 |
| Age class, N (%) | 0.002 | ||
| 18–30 years old | 8 (8.1%) | 7 (8.1%) | |
| 31–40 years old | 17 (17.2%) | 4 (4.7%) | |
| 41–50 years old | 13 (13.1%) | 14 (16.3%) | |
| 51–60 years old | 26 (26.3%) | 13 (15.1%) | |
| 61–70 years old | 19 (19.2%) | 14 (16.3%) | |
| 71–85 years old | 16 (16.2%) | 34 (39.5%) | |
| Sex, N (%) | 0.433 | ||
| Male | 70 (70.7%) | 56 (65.1%) | |
| Female | 29 (29.3%) | 30 (34.9%) | |
| Vital signs on ICU admission, median (IQR) | |||
| Oxygen saturation (%) | 98 (95.0–100.0) 1 | 97 (96.0–99.0) 2 | 0.194 |
| Pulse rate (bpm) | 93 (86.0–111.0) 3 | 101 (89.0–114.0) | 0.177 |
| Systolic blood pressure (mmHg) | 107.5 (90.0–126.5) 3 | 108 (95.0–122.0) | 0.695 |
| Diastolic blood pressure (mmHg) | 64 (52.0–74.25) 3 | 58.5 (49.0–68.0) | 0.073 |
| Comorbidities, N (%) | |||
| Hypertension | 46 (46.5%) | 44 (51.2%) | 0.557 |
| Diabetes | 45 (45.5%) | 35 (40.7%) | 0.554 |
| Cardiac disease | 29 (29.3%) | 29 (33.7%) | 0.530 |
| Chronic lung disease | 9 (9.1%) | 28 (32.6%) | 0.0001 |
| Malignancy | 15 (15.2%) | 8 (9.3%) | 0.269 |
| Immunosuppressive treatment | 6 (6.1%) | 4 (4.7%) | 0.753 |
| SOT | 3 (3.0%) | 2 (2.3%) | 1.000 |
| HSCT | 2 (2.0%) | 0 (0.0%) | 0.500 |
| Number of comorbidities, N (%) | 0.221 | ||
| 0 | 33 (33.3%) | 20 (23.3%) | |
| 1 | 17 (17.2%) | 14 (16.3%) | |
| 2 | 21 (21.2%) | 29 (33.7%) | |
| 3 | 20 (20.2%) | 15 (17.4%) | |
| 4 to 5 | 8 (8.1%) | 8 (9.3%) |
| Study Population | Patients According to the Number of Detected Pathogens, N (%) | ||
|---|---|---|---|
| No Detections | One Detection | Two Detections | |
| Pre-BCID2 phase (n = 99) | 12 (12.1%) | 83 (83.8%) | 4 (4.0%) |
| BCID2 phase (n = 86) | 1 (1.2%) | 72 (83.7%) | 13 (15.1%) |
| Study Population | Patients According to the Number of Ordered Empirical Antibiotics, N (%) | ||||
|---|---|---|---|---|---|
| No Empirical Antibiotics | One Empirical Antibiotics | Two Empirical Antibiotics | Three Empirical Antibiotics | Unknown Number | |
| Pre-BCID2 phase (n = 99) | 1 (1.0%) | 32 (32.3%) | 42 (42.4%) | 24 (24.7%) | 0 (0.0%) |
| BCID2 phase (n = 86) | 1 (1.2%) | 37 (43.0%) | 30 (34.9%) | 17 (19.8%) | 1 (1.2%) 1 |
| Study Population | Patients According to Antibiotics Change, N (%) | ||
|---|---|---|---|
| No Record of Antibiotics Change 1 | Change to Targeted Antibiotics 2 | Unknown 3 | |
| Pre-BCID2 phase (n = 99) | 4 (4.0%) | 94 (94.9%) | 1 (1.0%) |
| BCID2 phase (n = 86) | 3 (3.5%) | 82 (95.3%) | 1 (1.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senok, A.; Dabal, L.A.; Alfaresi, M.; Habous, M.; Celiloglu, H.; Bashiri, S.; Almaazmi, N.; Ahmed, H.; Mohmed, A.A.; Bahaaldin, O.; et al. Clinical Impact of the BIOFIRE Blood Culture Identification 2 Panel in Adult Patients with Bloodstream Infection: A Multicentre Observational Study in the United Arab Emirates. Diagnostics 2023, 13, 2433. https://doi.org/10.3390/diagnostics13142433
Senok A, Dabal LA, Alfaresi M, Habous M, Celiloglu H, Bashiri S, Almaazmi N, Ahmed H, Mohmed AA, Bahaaldin O, et al. Clinical Impact of the BIOFIRE Blood Culture Identification 2 Panel in Adult Patients with Bloodstream Infection: A Multicentre Observational Study in the United Arab Emirates. Diagnostics. 2023; 13(14):2433. https://doi.org/10.3390/diagnostics13142433
Chicago/Turabian StyleSenok, Abiola, Laila Al Dabal, Mubarak Alfaresi, Maya Habous, Handan Celiloglu, Safia Bashiri, Naama Almaazmi, Hassan Ahmed, Ayman A. Mohmed, Omar Bahaaldin, and et al. 2023. "Clinical Impact of the BIOFIRE Blood Culture Identification 2 Panel in Adult Patients with Bloodstream Infection: A Multicentre Observational Study in the United Arab Emirates" Diagnostics 13, no. 14: 2433. https://doi.org/10.3390/diagnostics13142433
APA StyleSenok, A., Dabal, L. A., Alfaresi, M., Habous, M., Celiloglu, H., Bashiri, S., Almaazmi, N., Ahmed, H., Mohmed, A. A., Bahaaldin, O., Elimam, M. A. E., Rizvi, I. H., Olowoyeye, V., Powell, M., & Salama, B. (2023). Clinical Impact of the BIOFIRE Blood Culture Identification 2 Panel in Adult Patients with Bloodstream Infection: A Multicentre Observational Study in the United Arab Emirates. Diagnostics, 13(14), 2433. https://doi.org/10.3390/diagnostics13142433