Abstract
The soluble urokinase plasminogen activator receptor (suPAR), as a correlate of chronic low-grade inflammation, may be used to predict individual cardiovascular risk. Since chronic low-grade inflammation is thought to be associated with the development of cardiovascular disease, this study aimed to evaluate if suPAR plasma levels are correlated with cardiovascular risk factors in young and healthy adults (aged 25–41 years). Consequently, data from the GAPP (genetic and phenotypic determinants of blood pressure and other cardiovascular risk factors) study were used to investigate suPAR plasma levels in relation to the following cardiovascular risk factors and laboratory parameters: BMI, physical activity, alcohol consumption, smoking status, blood pressure parameters, glucose status, and lipid levels. Additionally, suPAR was compared to the healthy lifestyle score and the Framingham score representing the overall cardiovascular risk profile. These associations were assessed using two different statistical approaches. Firstly, all cardiovascular risk factors and scores were compared amongst sex-specific suPAR plasma levels with ANOVA analysis. Secondly, sex-specific multivariable linear regressions were performed. Female participants had higher plasma suPAR levels than male participants (1.73 ng/mL versus 1.50 ng/mL; p < 0.001). A significant inverse correlation between suPAR plasma levels and HDL cholesterol was found in men (p = 0.001) and women (p < 0.001). Furthermore, male (p < 0.001) and female participants (p < 0.001) who smoked showed significantly higher plasma levels of suPAR (p < 0.001). For male participants, an inverse correlation of the healthy lifestyle score with suPAR plasma levels (p = 0.001) and a positive correlation of the Framingham score with suPAR plasma levels (p < 0.001) were detected. In women, no such correlation was found. The cholesterol levels (p = 0.001) and HbA1c (p = 0.008) correlated significantly with plasma suPAR levels in female participants. suPAR plasma levels were found to be strongly associated with certain cardiovascular risk factors; however, sex-specific differences were found. These sex-specific differences might be explained by the higher prevalence of cardiovascular risk factors in men resulting in a stronger correlation of suPAR as a marker of low-grade inflammation, since the existence of the risk factors already led to subclinical damage in men. Further research on suPAR levels in an older study population is needed.
1. Introduction
As a result of the globally increasing prevalence of cardiovascular risk factors and cardiovascular diseases, research nowadays not only focuses on possible causes and appropriate treatments, but furthermore, on possible preventive measures as well [1,2]. Cardiac biomarkers are consequently being investigated as possible components of personalized risk stratification strategies to customize appropriate preventive measures individually [3].
Compared with the fluctuating plasma levels of hsCRP, the plasma levels of the soluble urokinase plasminogen activator receptor (suPAR) are regarded as being more stable [4]. Therefore, suPAR is being examined as a potential alternative biomarker and a more accurate estimate of the inflammation status [4]. The soluble urokinase plasminogen activator receptor is produced as a cleavage product of the membrane-bound uPAR [5]. This receptor is activated by uPA and its signaling pathway regulates the coagulation cascade and cell signaling, influencing the survival and proliferation as well as the motility of cells [6]. uPAR is located on a wide variety of cells including immune cells and structural cells (such as keratinocytes, fibroblasts, as well as endothelial cells), but also on megakaryocytes, smooth muscle cells, and certain tumor cells [7]. Inflammation is thought to upregulate uPAR expression [8].
The primary aim of the study was to evaluate the association of suPAR plasma levels with cardiovascular risk factors. Additionally, the association of suPAR plasma levels with the overall cardiovascular risk estimated by the healthy lifestyle score and the Framingham risk score was assessed [9,10]. For the verification of predicted correlations between plasma levels of suPAR and cardiovascular risk factors in younger populations, the current study analyzed data from young and healthy adults aged 25–41 years.
2. Methods
2.1. Study Population
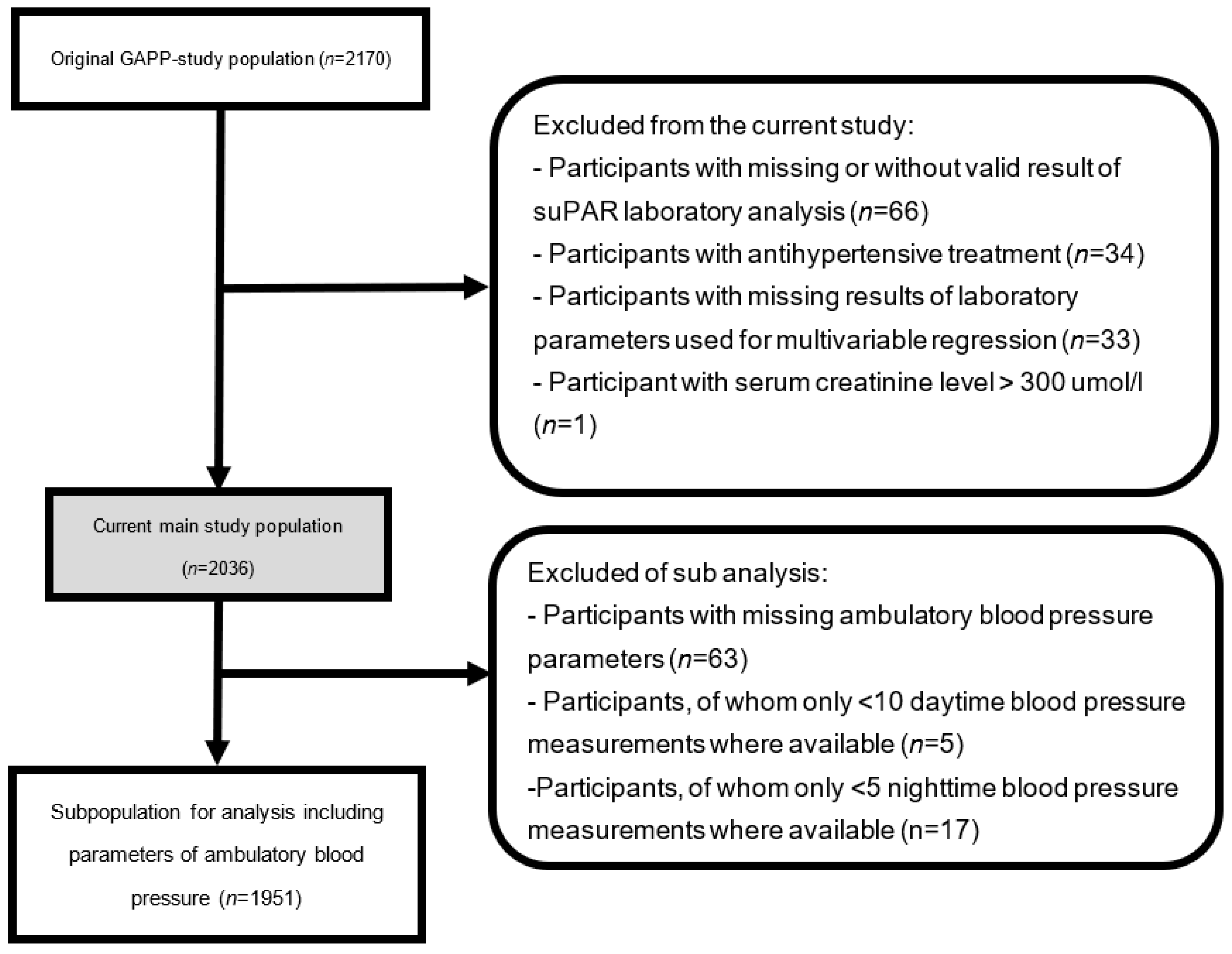
This substudy was based on the study population of the GAPP (genetic and phenotypic determinants of blood pressure and other cardiovascular risk factors) study. The GAPP project was constructed as a cohort study including the population of the Principality of Liechtenstein [11]. The overall aim of the GAPP study is to determine the possible causes and risk factors of arterial hypertension and cardiovascular disease. Exclusion criteria for participation were pre-existing cardiovascular disease or pre-existing documented obstructive sleep apnea syndrome and obesity class II, pregnancy or ongoing lactation, the daily intake of medication (such as antidiabetic drugs or insulin, as well as nonsteroidal anti-inflammatory drugs including aspirin or steroids (>1 day per week) and sympathomimetic drugs (>1 day per week)), the frequent consumption of liquorice (>1 day per week), or any known severe diseases [11]. Of the 2170 participants enrolled at baseline, 134 participants were excluded due to missing or invalid suPAR values (n = 66), the intake of antihypertensive treatment (n = 34), levels of creatinine >300 umol/L (n = 1), or missing parameters that are used as correction factors (n = 33), resulting in 2036 participants becoming eligible for the overall analyses (Figure 1). A subpopulation excluded participants with missing ambulatory blood pressure measurements (n = 63), or with fewer than 10 daytime or fewer than 5 nighttime blood pressure measurements (n = 22), resulting in 1951 participants (Figure 1). Written informed consent was obtained and the local ethics committee (KEK, Zürich, Switzerland) approved the study protocol.
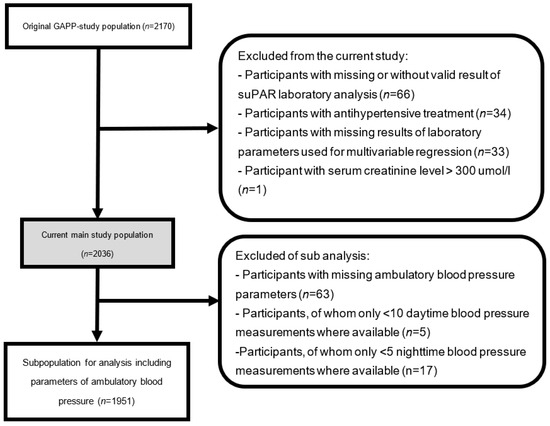
Figure 1.
Study population.
2.2. Assessment of Laboratory Parameters
Laboratory parameters were acquired through a fasting venous blood sample taken via a minimally invasive venipuncture and a morning urine sample. The blood samples were immediately analyzed in an accredited medical laboratory (ISO 17025) and parts of them were stored at −80 °C directly after centrifugation for possible future analyses [12]. EDTA plasma samples were used for the determination of plasma levels of suPAR using the enzyme immunoassay (suPARnostic, ViroGates, 3460 Birkerød, Denmark). The kidney function was estimated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [13]. Additionally, urinary sodium and creatinine levels were determined. A complete list of all laboratory parameters was previously described in the first paper published of the GAPP study project [11].
2.3. Cardiovascular Risk Profile Algorithms
We used 7 predefined health metrics as indicators for a healthy lifestyle summed up in a healthy lifestyle score [9,14]. If one of the health metrics was fulfilled, 1 point was added to the total score ranging from a minimum of 0 points to a maximum of 7 points. These seven health metrics included in the healthy lifestyle score were: physical activity exceeding or equaling 150 min of intense physical activity or 210 min of moderate physical activity per week, a BMI lower than 25 kg/m2, a nonsmoker status, an LDL plasma level of less than 160 mg/dL, an HbA1c of less than 5.7%, a systolic blood pressure < 120 mmHg, and healthy nutrition. The participants’ nutrition was qualified as healthy if at least two of the following criteria were met: the consumption of at least 4 portions of fruit or vegetables in a day, the consumption of fish at least 2 times a week, and a daily sodium intake lower than 1.5 g. Daily sodium intake was estimated using the Kawasaki formula, which calculates an estimate of 24 h sodium excretion based on natrium and creatinine in spot urine [15].
In addition, the Framingham score was used as an indicator of the individual cardiovascular risk profile. The score was based on each participants’ age, the HDL serum levels, the total cholesterol serum levels, the systolic blood pressure, the smoking status, and the glycemic status [10].
2.4. Blood Pressure Measurements
The conventional office blood pressure (BP) was measured three times on the nondominant arm using a validated oscillometric blood pressure monitor (Microlife BP3AG1, Microlife AG, Widnau, Switzerland). The mean of the conventional BP was calculated from the second and third blood pressure measurement. The mean arterial pressure (MAP) was calculated using an alternative equation, which contrasts the conventional formula by using the form factor 0.412 instead of 0.333 [16,17]. The MAP estimate calculated by this alternative equation seems to be in a closer relation with cardiovascular parameters (such as left ventricular mass, aortic stiffness, and carotid wall thickness) than the conventional one [16]. The MAP for the second and third office BP measurement was calculated and the mean of these two calculated MAPs was used for the statistical analyses. In this study, a systolic pressure of 140 mmHg or higher and a diastolic pressure of 90 mmHg were qualified for the diagnosis of arterial hypertension [18].
The 24 h blood pressure was recorded every 15 min from 07:30 to 22:00 and every 30 min from 22:00 to 07:30 with a validated ambulatory blood pressure monitoring system (BR-102 plus, Schiller AG, Baar, Switzerland). The participants were requested to keep their arm still during the time of recording, but were allowed to participate normally in their daily routine. The differentiation between day- and nighttime measurements was assigned individually according to the participants’ sleep diary kept during the measurement periods. The measurement of the 24 h BP was repeated if more than 20% of the BP measurements were invalid.
2.5. Statistical Analysis
Since this study confirmed sex-specific differences in mean suPAR plasma levels, the baseline characteristics, as listed in Table 1, describe the female and male study population separately and all of the following analyses were carried out sex-specifically [19]. All investigated cardiovascular risk factors, consisting of the BMI (kg/m2), an estimate for the physical activity, alcohol drinking and smoking habits, blood pressure indicators, and laboratory parameters (describing the glycemic profile, the blood lipids, renal function and hsCRP) that complemented the cardiovascular risk estimation scores or were used as correction factors, were represented in the sex-specific baseline characteristics. The distribution pattern of continuous variables was visually analyzed. Normally distributed variables are presented as means and were analyzed using the t-test. Atypically distributed variables are presented as medians and were analyzed using the Wilcoxon test. Categorical variables are presented in percentages and were analyzed using the chi-square test or Fisher’s exact test as appropriate.

Table 1.
Baseline characteristics.
In order to confirm the results, two different statistical approaches were used. Firstly, cardiovascular risk factors were compared between sex-specific quartiles of suPAR plasma levels using one-way ANOVA tests.
In a second step, we performed multivariable linear regression analyses of each cardiovascular risk factor continuously and also across sex-specific quartiles of suPAR plasma levels. The following variables were used as correction factors for the multivariable linear regression analyses: age, BMI, physical activity, HbA1c, renal function estimated by GFR, LDL, HDL, smoking status, and hsCRP. For the multivariable linear regressions analyzing the correlation of the healthy lifestyle score and the Framingham score with suPAR plasma levels, only age and eGFR were used as correction factors.
We considered correlations to be confirmed if they were proven in these two mentioned statistical approaches.
The statistical analyses were performed with RStudio (2021.09.1.372, Posit, Boston, MA, USA).
3. Results
Baseline characteristics stratified by sex are presented in Table 1. While there was no difference in age and hsCRP between the male and female study population, sex-specific differences were found for suPAR plasma levels (1.50 ng/mL vs. 1.73 ng/mL, p < 0.001) and all cardiovascular risk factors were investigated.
When comparing the means and medians of the cardiovascular risk factors between the quartiles of suPAR plasma levels in the male study population as listed in Table 2, positive correlations were found for BMI (p = 0.014), a comparison between current and past smoking statuses and those of nonsmokers (p < 0.001), cholesterol (p = 0.034), HDL cholesterol (p < 0.001), as well as an inverse correlation for HDL (p < 0.001). The healthy lifestyle score was inversely (p < 0.001) correlated with suPAR plasma levels and the Framingham score (p < 0.001) was positively correlated with suPAR plasma levels.
Table 2.
Baseline characteristics of the male study population according to suPAR quartiles.
These correlations were confirmed using the multivariable regression analyses, as presented in Table 3 for the variables HDL with a standardized β-regression coefficient of −0.155 (p < 0.001) and current smoking compared to past and completely absent smoking habits with a standardized β-regression coefficient of 0.267 (p < 0.001). An additional significant correlation was found for the variable irregular physical activity with a standardized β-regression coefficient of 0.780 (p = 0.014). Multivariable regression analyses also confirmed the correlation of suPAR plasma levels with cardiovascular risk profile algorithms, the healthy lifestyle score with a standardized β-regression coefficient of −0.129 (p = 0.001), and the Framingham score with a standardized β-regression coefficient of 0.161 (p < 0.001).
Table 3.
Multivariable linear regression analyses for the relationship between serum levels of suPAR and blood pressure parameters in men.
Table 4 shows positive correlations in the female population of suPAR plasma levels with the following risk factors: BMI (p < 0.001), a comparison between current and past smoking statuses and those of nonsmokers (p < 0.001), fasting glucose (p < 0.001), HbA1c (p < 0.001), cholesterol (p = 0.001), and an inverse correlation for HDL (p < 0.001). An inverse correlation was found between the suPAR plasma levels and the healthy lifestyle score (p = 0.005).
Table 4.
Baseline characteristics of the female study population according to suPAR quartiles.
When assessing correlations in the female study population using multivariable regression analyses as listed in Table 5, a confirmation of the earlier-mentioned correlations was found for HDL with a standardized β-regression coefficient of –0.114 (p < 0.001), HbA1c with a standardized β-regression coefficient of 0.081 (p = 0.008), cholesterol with a standardized β-regression coefficient of −0.094 (p < 0.001), and current smoking compared to past and completely absent smoking habits with a standardized β-regression coefficient of 0.076 (p = 0.017). The correlation of suPAR plasma levels and the healthy lifestyle score was not confirmed using multivariable regression analyses.
Table 5.
Multivariable linear regression analyses for the relationship between serum levels of suPAR and blood pressure parameters in women.
4. Discussion
This study showed significant higher suPAR plasma levels in the female population compared to the male population and sex-specific differences in the distribution of cardiovascular risk factors [20,21].
In accordance with recent studies, a statistically significant inverse correlation between suPAR plasma levels and the HDL serum levels was found in the male and female population, as well as higher suPAR plasma levels in smokers compared to nonsmokers and past smokers [21,22]. Furthermore, our study confirmed a positive correlation between cholesterol levels and suPAR plasma levels in the female population [21]. The biomarker suPAR is regarded as a marker of endothelial dysfunction and therefore also of atherosclerosis, which is why it seems plausible that smoking and higher cholesterol levels increase, whereas a higher HDL decreases plasma suPAR levels [23].
In contrast to other studies, our study could not confirm a correlation between BMI and suPAR plasma levels [21]. The highest BMIs observed in the current study population (BMI of 38 kg/m2) are not classified as obesity grade III (BMI 40 kg/m2), which was associated with higher suPAR plasma levels in the study published by Haupt, T.H. et al. [21]. The MONICA study resulted in the same conclusion as our study: that BMI is not independently associated with suPAR plasma levels [24]. This conclusion could imply that comorbidities associated with obesity are causing higher plasma levels of suPAR, rather than a higher BMI itself.
To the existing literature with an inconsistent evaluation of the association of suPAR and diabetes mellitus type 2, we now add that higher HbA1c in the female population seems to be correlated with higher suPAR plasma levels [21,24]. The sex-specific difference in this correlation cannot be explained by the already-existing literature, since a sex-independent correlation of suPAR and the endothelial dysfunction caused by permanently higher blood sugar levels reflected by the HbA1c levels would be expected [23,25].
Additionally, we used the healthy lifestyle score and the Framingham score as markers of the overall cardiovascular risk in our analyses, which correlated with suPAR plasma levels only in the male study population, but not in the female one. It was shown that in male participants, a higher lifestyle score, indicating a healthier way of living, resulted in statistically lower suPAR plasma levels, while a higher Framingham score, indicating a higher cardiovascular risk and mortality, was correlated with higher suPAR plasma levels [21].
Most research attempting to assess suPAR as an estimate for cardiovascular risk is based on study populations with a distinctly higher average age of around 50 years. While these studies predict correlations between plasma suPAR levels and the participants cardiovascular risk, our study results did not detect sex-independent consistency [21,22,24]. This is why we think that in elderly female participants with a higher prevalence of cardiovascular risk factors, such correlations might be found too. This suggests that suPAR might act as a predictor of the cardiovascular risk in elderly participants.
We did not find sex-independent correlations apart from the inverse correlation of plasma suPAR levels with HDL levels and the higher suPAR plasma levels found in smokers compared to nonsmokers and current smokers [26]. The consistency of these two correlations arguably displays the extent of the influence of smoking and lower HDL levels on cardiovascular health.
Nevertheless, there is an evident indication of a certain correlation of plasma suPAR levels with cardiovascular risk factors given statistically significant correlations of the healthy lifestyle score and the Framingham score with suPAR plasma levels in the male study population. Sex-specific differences in the correlation of suPAR plasma levels with these two validated scores might be a consequence of the higher prevalence of cardiovascular risk factors in men compared to women, as demonstrated in the sex-specific baseline characteristics [27]. An increase in cardiovascular risk factors in older women might explain age-specific correlations in women, which were demonstrated in other studies on this topic. This seems quite conceivable since this biomarker represents low-grade inflammation and only the persistent influence of cardiovascular risk factors results in accumulating damage, which is then detectable later on [28].
5. Strengths and Limitations
A major strength of our study is the young and healthy study population (aged 25–41 years) lacking any relevant comorbidities, thus minimizing possible interference by unknown confounders. Investigating the correlations of the biomarker suPAR with cardiovascular risk factors and the overall cardiovascular risk in a young and healthy population is important, since preventive measures to reduce the global burden of cardiovascular risk factors and diseases should take place before irreversible damage is set. Therefore, potential biomarkers should be well investigated in younger populations without manifestations of cardiovascular diseases to enable an early implementation of these biomarkers.
Furthermore, the great number of variables representing the cardiovascular risk factors results in a detailed description of the study population, which allows differentiated results.
Analyzing correlations in two different ways, firstly by comparing the quartiles and secondly using multivariable linear regression analyses, ensures reliable results.
A limitation of this study is the reduction in the size of the study population due to sex-specific analyses. These separations were necessary due to the statistically significant sex-specific differences in plasma levels of suPAR and in most of the investigated variables. Secondly, the generalizability of this study is limited, given the fact that the study only included people living in Liechtenstein.
Thirdly, this study was based on investigating possible correlations of the potential biomarker suPAR with cardiovascular risk factors. The insights gained by this study should be extended by integrating the hard clinical endpoints such as survival, mortality, and disease-free survival in future follow-up studies.
In conclusion, the evident indication that there is a certain correlation between suPAR plasma levels and cardiovascular risk factors, as well as the fact that there are suspected age-specific differences in these correlations, emphasizes the importance of further investigations in this topic and particularly of comparing the mentioned potential correlations in different age groups. In our opinion, a possible approach for further investigations would be a follow-up study of equal study design, hypothesis, and the same study population, with the only difference being an older study population, in order to evaluate if suPAR might be an age-specific biomarker reflecting cardiovascular risk solely in an elderly population. A second step would be to correlate individual changes in the plasma suPAR levels of each participant with the change in their individual cardiovascular risk profile.
Author Contributions
Conceptualization, N.F.W., K.G., O.C.W. and L.R.; Methodology, N.F.W. and L.R.; Formal analysis, N.F.W.; Writing—original draft, N.F.W.; Writing—review & editing, S.A., O.C.W., J.T., M.R., D.C. and L.R.; Supervision, L.R.; Project administration, K.G.; Funding acquisition, K.G. All authors have read and agreed to the published version of the manuscript.
Funding
The GAPP study is supported by the the Swiss National Science Foundation (PP00P3_133681, to David Conen), the Liechtenstein Government, the Swiss Heart Foundation, the Swiss Society of Hypertension, the University of Basel, University Hospital Basel, the Hanela Foundation, Schiller AG and Novartis.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the study protocol of the original GAPP study and all follow-up studies was approved by the local ethics committee (KEK, Zürich, Switzerland) on the 29 March 2012 (KEK-StV-Nr. 66/09).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Anonymized data that underlie the results reported in this article are available upon justified request to the corresponding author.
Acknowledgments
The authors thank the participants and staff of the GAPP study for their important contributions.
Conflicts of Interest
David Conen has received consulting fees from Roche Diagnostics and Trimedics, as well as speaker fees from Servier and BMS/Pfizer, all outside of the current work. Lorenz Risch and Martin Risch are key shareholders of the Dr Risch Medical Laboratory. The other authors have no financial or personal conflicts of interest to declare.
References
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Westermann, D.; Neumann, J.T.; Sörensen, N.A.; Blankenberg, S. High-sensitivity assays for troponin in patients with cardiac disease. Nat. Rev. Cardiol. 2017, 14, 472–483. [Google Scholar] [CrossRef] [PubMed]
- Andersen, O.; Eugen-Olsen, J.; Kofoed, K.; Iversen, J.; Haugaard, S.B. Soluble urokinase plasminogen activator receptor is a marker of dysmetabolism in HIV-infected patients receiving highly active antiretroviral therapy. J. Med. Virol. 2008, 80, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Montuori, N.; Visconte, V.; Rossi, G.; Ragno, P. Soluble and cleaved forms of the urokinase-receptor: Degradation products or active molecules? Thromb. Haemost. 2005, 93, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.W.; Marshall, C.J. Regulation of cell signalling by uPAR. Nat. Rev. Mol. Cell Biol. 2010, 11, 23–36. [Google Scholar] [CrossRef]
- Thunø, M.; Macho, B.; Eugen-Olsen, J. suPAR: The molecular crystal ball. Dis. Markers 2009, 27, 157–172. [Google Scholar] [CrossRef]
- Florquin, S.; van den Berg, J.G.; Olszyna, D.P.; Claessen, N.; Opal, S.M.; Weening, J.J.; Van Der Poll, T. Release of urokinase plasminogen activator receptor during urosepsis and endotoxemia. Kidney Int. 2001, 59, 2054–2061. [Google Scholar] [CrossRef]
- Yang, Q.; Cogswell, M.E.; Flanders, W.D.; Hong, Y.; Zhang, Z.; Loustalot, F.; Gillespie, C.; Merritt, R.; Hu, F.B. Trends in Cardiovascular Health Metrics and Associations with All-Cause and CVD Mortality among US Adults. JAMA 2012, 307, 1273–1283. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef]
- Conen, D.; Schön, T.; Aeschbacher, S.; Paré, G.; Frehner, W.; Risch, M.; Risch, L. Genetic and phenotypic determinants of blood pressure and other cardiovascular risk factors (GAPP). Swiss Med. Wkly. 2013, 143, w13728. [Google Scholar] [CrossRef] [PubMed]
- SN EN ISO/IEC 17025; Allgemeine Anforderung an die Kompetenz von Prüf- und Kalibrierlaboren. DIN: Berlin, Germany, 2017.
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Aeschbacher, S.; Bossard, M.; Ruperti Repilado, F.J.; Good, N.; Schoen, T.; Zimny, M.; Probst-Hensch, N.M.; Schmidt-Trucksäss, A.; Risch, M.; Risch, L.; et al. Healthy lifestyle and heart rate variability in young adults. Eur. J. Prev. Cardiol. 2016, 23, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, T.; Itoh, K.; Uezono, K.; Sasaki, H. A Simple Method for Estimating 24 h Urinary Sodium and Potassium Excretion from Second Morning Voiding Urine Specimen in Adults. Clin. Exp. Pharmacol. Physiol. 1993, 20, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, T.G.; Protogerou, A.D.; Vrachatis, D.; Konstantonis, G.; Aissopou, E.; Argyris, A.; Nasothimiou, E.; Gialafos, E.J.; Karamanou, M.; Tousoulis, D.; et al. Mean arterial pressure values calculated using seven different methods and their associations with target organ deterioration in a single-center study of 1878 individuals. Hypertens. Res. 2016, 39, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Meaney, E.; Alva, F.; Moguel, R.; Meaney, A.; Alva, J.; Webel, R. Formula and nomogram for the sphygmomanometric calculation of the mean arterial pressure. Heart 2000, 84, 64. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef]
- Frary, C.E.; Biering-Sørensen, T.; Nochioka, K.; Blicher, M.K.; Olesen, T.B.; Stidsen, J.V.; Greve, S.V.; Vishram-Nielsen, J.K.K.; Rasmussen, S.L.; Eugen-Olsen, J.; et al. Sex- and age-related differences in the predictive capability of circulating biomarkers: From the MONICA 10 cohort. Scand. Cardiovasc. J. 2021, 55, 65–72. [Google Scholar] [CrossRef]
- Mehta, A.; Desai, S.; Ko, Y.; Liu, C.; Dhindsa, D.S.; Nayak, A.; Hooda, A.; Martini, M.A.; Ejaz, K.; Sperling, L.S.; et al. Sex Differences in Circulating Soluble Urokinase-Type Plasminogen Activator Receptor (suPAR) Levels and Adverse Outcomes in Coronary Artery Disease. J. Am. Heart Assoc. 2020, 9, e015457. [Google Scholar] [CrossRef]
- Haupt, T.H.; Kallemose, T.; Ladelund, S.; Rasmussen, L.J.H.; Thorball, C.W.; Andersen, O.; Pisinger, C.; Eugen-Olsen, J. Risk Factors Associated with Serum Levels of the Inflammatory Biomarker Soluble Urokinase Plasminogen Activator Receptor in a General Population. Biomark. Insights 2014, 9, 91–100. [Google Scholar] [CrossRef]
- Lyngbæk, S.; Marott, J.L.; Sehestedt, T.; Hansen, T.W.; Olsen, M.H.; Andersen, O.; Linneberg, A.; Haugaard, S.B.; Eugen-Olsen, J.; Hansen, P.R.; et al. Cardiovascular risk prediction in the general population with use of suPAR, CRP, and Framingham Risk Score. Int. J. Cardiol. 2013, 167, 2904–2911. [Google Scholar] [CrossRef] [PubMed]
- Lyngbæk, S.; Sehestedt, T.; Marott, J.L.; Hansen, T.W.; Olsen, M.H.; Andersen, O.; Linneberg, A.; Madsbad, S.; Haugaard, S.B.; Eugen-Olsen, J.; et al. CRP and SuPAR Are Differently Related to Anthropometry and Subclinical Organ Damage. Int. J. Cardiol. 2013, 167, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Eugen-Olsen, J.; Andersen, O.; Linneberg, A.; Ladelund, S.; Hansen, T.; Langkilde, A.; Petersen, J.; Pielak, T.; Møller, L.N.; Jeppesen, J.; et al. Circulating soluble urokinase plasminogen activator receptor predicts cancer, cardiovascular disease, diabetes and mortality in the general population. J. Intern. Med. 2010, 268, 296–308. [Google Scholar] [CrossRef] [PubMed]
- Sherif, E.M.; El Maksood, A.A.A.; Youssef, O.I.; Salah El-Din, N.Y.; Khater, O.K.M. Soluble Urokinase Plasminogen Activator Receptor in Type 1 Diabetic Children, Relation to Vascular Complications. J. Diabetes Complicat. 2019, 33, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Diederichsen, M.Z.; Diederichsen, S.Z.; Mickley, H.; Steffensen, F.H.; Lambrechtsen, J.; Sand, N.P.R.; Christensen, K.L.; Olsen, M.H.; Diederichsen, A.; Grønhøj, M.H. Prognostic value of suPAR and hs-CRP on cardiovascular disease. Atherosclerosis 2018, 271, 245–251. [Google Scholar] [CrossRef]
- Pinho-Gomes, A.C.; Peters, S.A.E.; Thomson, B.; Woodward, M. Sex Differences in Prevalence, Treatment and Control of Cardiovascular Risk Factors in England. Heart 2020. [Google Scholar] [CrossRef]
- Sehestedt, T.; Lyngbæk, S.; Eugen-Olsen, J.; Jeppesen, J.; Andersen, O.; Hansen, T.; Linneberg, A.; Jørgensen, T.; Haugaard, S.; Olsen, M. Soluble urokinase plasminogen activator receptor is associated with subclinical organ damage and cardiovascular events. Atherosclerosis 2011, 216, 237–243. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).