
Cell-Free DNA as a New Biomarker of IVF Success, Independent of Any Infertility Factor, Including Endometriosis

 ,
,  , and
, and
Abstract
1. Introduction
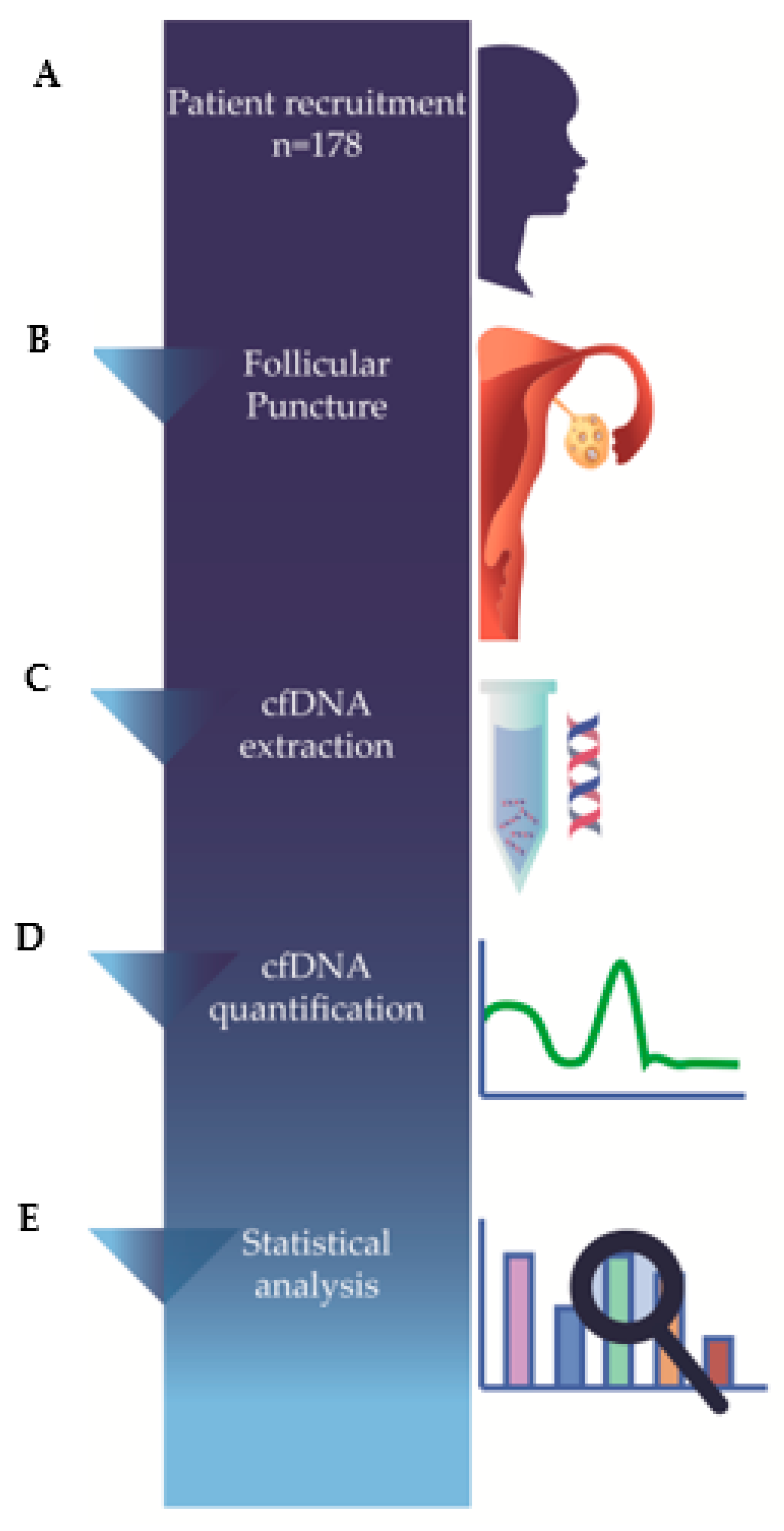
2. Materials and Methods
2.1. Study Population
2.2. Ethical Approval
2.3. Follicular Fluid Sample Collection
2.4. Follicular Fluid Preparation
2.5. Cell-Free DNA Extraction
2.6. Cell-Free DNA Quantification
2.7. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zegers-Hochschild, F.; Adamson, G.D.; Dyer, S.; Racowsky, C.; de Mouzon, J.; Sokol, R.; Rienzi, L.; Sunde, A.; Schmidt, L.; Cooke, I.D.; et al. The International Glossary on Infertility and Fertility Care. Hum. Reprod. 2017, 32, 1786–1801. [Google Scholar] [CrossRef] [PubMed]
- Xiong, D.K.; Chen, H.H.; Ding, X.P.; Zhang, S.H.; Zhang, J.H. Association of polymorphisms in glutathione S-transferase genes (GSTM1, GSTT1, GSTP1) with idiopathic azoospermia or oligospermia in Sichuan, China. Asian J. Androl. 2015, 17, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Goudakou, M.; Kalogeraki, A.; Matalliotakis, I.; Panagiotidis, Y.; Gullo, G.; Prapas, Y. Cryptic sperm defects may be the cause for total fertilization failure in oocyte donor cycles. Reprod. Biomed. Online 2012, 24, 148–152. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gullo, G.; Cucinella, G.; Perino, A.; Gullo, D.; Segreto, D.; Laganà, A.S.; Buzzaccarini, G.; Donarelli, Z.; Marino, A.; Allegra, A.; et al. The Gender Gap in the Diagnostic-Therapeutic Journey of the Infertile Couple. Int. J. Environ. Res. Public Health. 2021, 18, 6184. [Google Scholar] [CrossRef]
- Balaban, B.; Gardner, D.K. Morphological assessment of blastocyst stage embryos: Types of grading systems and their reported outcomes. In Human Gametes and Preimplantation Embryos: Assessment and Diagnosis; Gardner, D., Sakkas, D., Seli, E., Wells, D., Eds.; Springer Science and Media: New York, NY, USA, 2013; pp. 31–43. [Google Scholar] [CrossRef]
- Rule, K.; Chosed, R.J.; Arthur Chang, T.; David Wininger, J.; Roudebush, W.E. Relationship between blastocoel cell-free DNA and day-5 blastocyst morphology. J. Assist. Reprod. Genet. 2018, 35, 1497–1501. [Google Scholar] [CrossRef]
- Yanaihara, A.; Mitsukawa, K.; Iwasaki, S.; Otsuki, K.; Kawamura, T.; Okai, T. High concentrations of lactoferrin in the follicular fluid correlate with embryo quality during in vitro fertilization cycles. Fertil. Steril. 2007, 87, 279–282. [Google Scholar] [CrossRef]
- Estes, S.J.; Ye, B.; Qiu, W.; Cramer, D.; Hornstein, M.D.; Missmer, S.A. A proteomic analysis of IVF follicular fluid in women ≤32 years old. Fertil. Steril. 2009, 92, 1569–1578. [Google Scholar] [CrossRef]
- Revelli, A.; Delle Piane, L.; Casano, S.; Molinari, E.; Massobrio, M.; Rinaudo, P. Follicular fluid content and oocyte quality: From single biochemical markers to metabolomics. Reprod Biol. Endocrinol. 2009, 7, 40. [Google Scholar] [CrossRef]
- Baka, S.; Malamitsi-Puchner, A. Novel follicular fluid factors influencing oocyte developmental potential in IVF: A review. Reprod. Biomed. Online. 2006, 12, 500–506. [Google Scholar] [CrossRef]
- Wallace, M.; Cottell, E.; Gibney, M.J.; McAuliffe, F.M.; Wingfield, M.; Brennan, L. An investigation into the relationship between the metabolic profile of follicular fluid, oocyte developmental potential, and implantation outcome. Fertil. Steril. 2012, 97, 1078–1084.e8. [Google Scholar] [CrossRef]
- Angelucci, S.; Ciavardelli, D.; Di Giuseppe, F.; Eleuterio, E.; Sulpizio, M.; Tiboni, G.M.; Giampietro, F.; Palumbo, P.; Di Ilio, C. Proteome analysis of human follicular fluid. Biochim. Et Biophys. Acta (BBA)-Proteins Proteom. 2006, 1764, 1775–1785. [Google Scholar] [CrossRef]
- Stroun, M.; Anker, P.; Lyautey, J.; Lederrey, C.; Maurice, P.A. Isolation and characterization of DNA from the plasma of cancer patients. Eur. J. Cancer Clin. Oncol. 1987, 23, 707–712. [Google Scholar] [CrossRef]
- Volik, S.; Alcaide, M.; Morin, R.D.; Collins, C. Cell-free DNA (cfDNA): Clinical Significance and Utility in Cancer Shaped by Emerging Technologies. Mol. Cancer Res. 2016, 14, 898–908. [Google Scholar] [CrossRef]
- Scalici, E.; Traver, S.; Molinari, N.; Mullet, T.; Monforte, M.; Vintejoux, E.; Hamamah, S. Cell-free DNA in human follicular fluid as a biomarker of embryo quality. Hum Reprod. 2014, 29, 2661–2669. [Google Scholar] [CrossRef]
- Diaz, L.A., Jr.; Bardelli, A. Liquid biopsies: Genotyping circulating tumor DNA. J. Clin. Oncol. 2014, 32, 579–586. [Google Scholar] [CrossRef]
- Schwarzenbach, H.; Hoon, D.S.; Pantel, K. Cell-free nucleic acids as biomarkers in cancer patients. Nat. Rev. Cancer. 2011, 11, 426–437. [Google Scholar] [CrossRef]
- Pisetsky, D.S.; Fairhurst, A.M. The origin of extracellular DNA during the clearance of dead and dying cells. Autoimmunity. 2007, 40, 281–284. [Google Scholar] [CrossRef]
- Gahan, P.B. Biology of circulating nucleic acids and possible roles in diagnosis and treatment in diabetes and cancer. Infect. Disord. Drug Targets. 2012, 12, 360–370. [Google Scholar] [CrossRef]
- Marzese, D.M.; Hirose, H.; Hoon, D.S. Diagnostic and prognostic value of circulating tumor-related DNA in cancer patients. Expert Rev. Mol. Diagn. 2013, 13, 827–844. [Google Scholar] [CrossRef]
- Lo, Y.M.; Corbetta, N.; Chamberlain, P.F.; Rai, V.; Sargent, I.L.; Redman, C.W.; Wainscoat, J.S. Presence of fetal DNA in maternal plasma and serum. Lancet. 1997, 350, 485–487. [Google Scholar] [CrossRef]
- Traver, S.; Assou, S.; Scalici, E.; Haouzi, D.; Al-Edani, T.; Belloc, S.; Hamamah, S. Cell-free nucleic acids as non-invasive biomarkers of gynecological cancers, ovarian, endometrial and obstetric disorders and fetal aneuploidy. Hum. Reprod. Updat. 2014, 20, 905–923. [Google Scholar] [CrossRef] [PubMed]
- Scalici, E.; Mullet, T.; Hoa, A.F.; Gala, A.; Loup, V.; Anahory, T.; Belloc, S.; Hamamah, S. Les acides nucléiques circulants et infertilité [Circulating nucleic acids and infertility]. Gynécologie Obs. Fertil. 2015, 43, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Zachariah, R.; Schmid, S.; Radpour, R.; Buerki, N.; Fan, A.X.; Hahn, S.; Holzgreve, W.; Zhong, X.Y. Circulating cell-free DNA as a potential biomarker for minimal and mild endometriosis. Reprod. Biomed. Online. 2009, 18, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Czamanski-Cohen, J.; Sarid, O.; Cwikel, J.; Levitas, E.; Lunenfeld, E.; Douvdevani, A.; Har-Vardi, I. Decrease in cell free DNA levels following participation in stress reduction techniques among women undergoing infertility treatment. Arch. Women's Ment. Health. 2014, 17, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Traver, S.; Scalici, E.; Mullet, T.; Molinari, N.; Vincens, C.; Anahory, T.; Hamamah, S. Cell-free DNA in Human Follicular Microenvironment: New Prognostic Biomarker to Predict in vitro Fertilization Outcomes. PLoS ONE. 2015, 10, e0136172. [Google Scholar] [CrossRef][Green Version]
- Prapas, Y.; Petousis, S.; Panagiotidis, Y.; Gullo, G.; Kasapi, L.; Papadeothodorou, A.; Prapas, N. Injection of embryo culture supernatant to the endometrial cavity does not affect outcomes in IVF/ICSI or oocyte donation cycles: A randomized clinical trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 162, 169–173. [Google Scholar] [CrossRef]
- Umetani, N.; Kim, J.; Hiramatsu, S.; Reber, H.A.; Hines, O.J.; Bilchik, A.J.; Hoon, D.S. Increased integrity of free circulating DNA in sera of patients with colorectal or periampullary cancer: Direct quantitative PCR for ALU repeats. Clin. Chem. 2006, 52, 1062–1069. [Google Scholar] [CrossRef]
- Mandel, P.; Metais, P. Les acides nucléiques du plasma sanguin chez l’homme [Nuclear Acids in Human Blood Plasma]. CR Seances Soc. Biol. Fil. 1948, 142, 241–243. [Google Scholar]
- Ralla, B.; Stephan, C.; Meller, S.; Dietrich, D.; Kristiansen, G.; Jung, K. Nucleic acid-based biomarkers in body fluids of patients with urologic malignancies. Crit. Rev. Clin. Lab. Sci. 2014, 51, 200–231. [Google Scholar] [CrossRef]
- Swarup, V.; Rajeswari, M.R. Circulating (cell-free) nucleic acids--a promising, non-invasive tool for early detection of several human diseases. FEBS Lett. 2007, 581, 795–799. [Google Scholar] [CrossRef]
- Jahr, S.; Hentze, H.; Englisch, S.; Hardt, D.; Fackelmayer, F.O.; Hesch, R.D.; Knippers, R. DNA fragments in the blood plasma of cancer patients: Quantitations and evidence for their origin from apoptotic and necrotic cells. Cancer Res. 2001, 61, 1659–1665. [Google Scholar]
- Burgio, S.; Polizzi, C.; Buzzaccarini, G.; Laganà, A.S.; Gullo, G.; Perricone, G.; Perino, A.; Cucinella, G.; Alesi, M. Psychological variables in medically assisted reproduction: A systematic review. Menopausal Rev. 2022, 21, 47–63. [Google Scholar] [CrossRef]
- Habib, N.; Buzzaccarini, G.; Centini, G.; Moawad, G.N.; Ceccaldi, P.F.; Gitas, G.; Alkatout, I.; Gullo, G.; Terzic, S.; Sleiman, Z. Impact of lifestyle and diet on endometriosis: A fresh look to a busy corner. Menopausal Rev. 2022, 21, 124–132. [Google Scholar] [CrossRef]
- Scutiero, G.; Iannone, P.; Bernardi, G.; Bonaccorsi, G.; Spadaro, S.; Volta, C.A.; Greco, P.; Nappi, L. Oxidative Stress and Endometriosis: A Systematic Review of the Literature. Oxidative Med. Cell. Longev. 2017, 2017, 7265238. [Google Scholar] [CrossRef]
- Agarwal, A.; Aponte-Mellado, A.; Premkumar, B.J.; Shaman, A.; Gupta, S. The effects of oxidative stress on female reproduction: A review. Reprod. Biol. Endocrinol. 2012, 10, 49. [Google Scholar] [CrossRef]
- Sedensky, M.M.; Morgan, P.G. Mitochondrial respiration and reactive oxygen species in mitochondrial aging mutants. Exp. Gerontol. 2006, 41, 237–245. [Google Scholar] [CrossRef]
- Pisoschi, A.M.; Pop, A. The role of antioxidants in the chemistry of oxidative stress: A review. Eur. J. Med. Chem. 2015, 97, 55–74. [Google Scholar] [CrossRef]
- Franks, S.; Stark, J.; Hardy, K. Follicle dynamics and anovulation in polycystic ovary syndrome. Hum. Reprod. Updat. 2008, 14, 367–378. [Google Scholar] [CrossRef]
- Dewailly, D.; Andersen, C.Y.; Balen, A.; Broekmans, F.; Dilaver, N.; Fanchin, R.; Griesinger, G.; Kelsey, T.W.; La Marca, A.; Lambalk, C.; et al. The physiology and clinical utility of anti-Mullerian hormone in women. Hum. Reprod. Updat. 2014, 20, 370–385. [Google Scholar] [CrossRef]
- Stigliani, S.; Anserini, P.; Venturini, P.L.; Scaruffi, P. Mitochondrial DNA content in embryo culture medium is significantly associated with human embryo fragmentation. Hum. Reprod. 2013, 28, 2652–2660. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Mean | n | Min-Max | SD | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q115) | p-Value (q115) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247) | p-Value (q247) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247/q115) | p-Value (q247/q115) |
|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 34 | - | 19–39 | 3.69 | - | - | - | - | - | - |
| <35 years | - | 92 | - | - | 1.3 ± 1.7 [1.0–1.7] | 0.259 | 1.7 ± 2.9 [1.1–2.3] | 0.670 | 9.7 ± 1.1 [9.5–9.9] | 0.017 |
| ≥35 years | - | 86 | - | - | 1.5 ± 1.8 [1.1–1.9] | 1.3 ± 1.8 [0.9–1.7] | 10.1 ± 1.2 [9.9–10.4] | |||
| BMI (kg/m2) | 24 | - | 17–33 | 3.70 | - | - | - | - | - | - |
| ≤25 kg/m2 | - | 123 | - | - | 1.5 ± 1.7 [1.2–1.8] | 0.612 | 1.6 ± 2.7 [1.1–2.1] | 0.427 | 9.9 ± 1.2 [9.7–10.2] | 0.582 |
| >25 kg/m2 | - | 55 | - | - | 1.4 ± 1.6 [0.9–1.8] | 1.3 ± 1.7 [0.8–1.7] | 9.8 ± 1.2 [9.5–10.2] | |||
| Ethnicity | - | - | - | - | - | - | - | - | - | - |
| Caucasian | - | 174 | - | - | 1.4 ± 1.7 [1.1–1.8] | 0.922 | 1.5 ± 2.4 [1.1–1.8] | 0.743 | 9.9 ± 1.1 [9.7–10.1] | 0.065 |
| Gypsy | - | 2 | - | - | 0.9 ± 1.2 [1.0–1.2] | 2.2 ± 2.5 [2.0–2.5] | 9.1 ± 0.7 [2.7–15.6] | |||
| Afro-Europeans | - | 2 | - | - | 1.3 ± 0.9 [0.7–9.9] | 0.4 ± 0.4 [0.3–4.3] | 11.7 ± 2.4 [10.2–33.8] | |||
| Age at menarche (years) | 12 | - | 8–18 | 1.82 | - | - | - | - | - | - |
| ≤12 years | - | 102 | - | - | 1.4 ± 1.6 [1.0–1.7] | 0.675 | 1.7 ± 2.8 [1.1–2.2] | 0.403 | 9.8 ± 1.2 [9.6–10.1] | 0.348 |
| 13–14 years | - | 52 | - | - | 1.4 ± 1.7 [0.9–1.9] | 1.1 ± 1.3 [0.7–1.5] | 10.0 ± 1.2 [9.7–10.4] | |||
| ≥15 years | - | 21 | - | - | 1.7 ± 2.2 [0.7–2.7] | 1.4 ± 2.3 [0.4–2.5] | 10.2 ± 1.1 [9.7–10.7] | |||
| Smoking Habits | - | - | - | - | - | - | - | - | - | - |
| Never | - | 130 | - | - | 1.4 ± 1.7 [1.1–1.7] | 0.998 | 1.5 ± 2.5 [1.0–1.9] | 0.741 | 10.0 ± 1.2 [9.7–10.2] | 0.572 |
| Previous | - | 21 | - | - | 1.4 ± 1.5 [0.7–2.1] | 1.7 ± 2.6 [0.5–2.9] | 9.9 ± 1.2 [9.4–10.4] | |||
| Present | - | 27 | - | - | 1.4 ± 1.7 [1.1–1.7] | 1.2 ± 1.5 [0.6–1.8] | 9.7 ± 1.7 [9.2–10.2] | |||
| Infertility length (months) | 53 | - | 14–192 | 32.8 | - | - | - | - | - | - |
| <24 months | - | 9 | - | - | 0.6 ± 0.8 [0.3–1.2] | 0.277 | 0.5 ± 0.3 [0.3–0.8] | 0.476 | 9.7 ± 1.02 [8.9–10.5] | 0.435 |
| 24–48 months | - | 91 | - | - | 1.5 ± 1.8 [1.1–1.9] | 1.6 ± 2.3 [1.1–2.1] | 9.8 ± 1.2 [9.6–10.1] | |||
| >48 months | - | 78 | - | - | 1.3 ± 1.6 [1.0–1.7] | 1.5 ± 2.4 [0.9–2.1] | 10.0 ± 1.1 [9.8–10.3] |
| Variable | n | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q115) | p-Value (q115) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247) | p-Value (q247) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247/q115) | p-Value (q247/q115) |
|---|---|---|---|---|---|---|---|
| Endometriosis | 45 | 1.2 ± 1.4 [0.8–1.6] | 0.528 | 1.3 ± 1.5 [0.8–1.7] | 0.376 | 9.9 ± 1.3 [9.5–10.3] | 0.822 |
| PCOS | 60 | 1.2 ± 1.5 [0.8–1.6] | 0.359 | 1.6 ± 3.5 [0.7–2.5] | 0.566 | 10.0 ± 1.2 [9.6–10.3] | 0.599 |
| POF | 40 | 1.6 ± 1.9 [1.0–2.2] | 0.494 | 1.5 ± 2.1 [0.8–2.2] | 0.999 | 10.0 ± 1.01 [9.7–10.4] | 0.326 |
| Idiopathic | 44 | 1.8 ± 2.1 [1.1–2.4] | 0.187 | 1.6 ± 1.5 [1.1–2.0] | 0.033 | 9.8 ± 1.1 [9.4–10.1] | 0.375 |
| Variable | Mean | n | Min-Max | SD | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q115) | p-Value (q115) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247) | p-Value (q247) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247/q115) | p-Value (q247/q115) |
|---|---|---|---|---|---|---|---|---|---|---|
| AMH (ng/mL) | 3.40 | - | 0.02–27 | 3.64 | - | - | - | - | - | - |
| ≤1 ng/mL | - | 35 | - | - | 1.6 ± 1.9 [0.9–2.3] | 0.479 | 1.7 ± 2.2 [0.9–2.5] | 0.534 | 9.9 ± 1.2 [9.5–10.3] | 0.940 |
| >1 ng/mL | - | 139 | - | - | 1.4 ± 1.7 [1.1–1.7] | 1.4 ± 2.5 [1.0–1.9] | 9.9 ± 1.2 [9.7–10.1] | |||
| AFC | 9.98 | - | 3–27 | 4.51 | - | - | - | - | - | - |
| ≤10 | - | 110 | - | - | 1.4 ± 1.7 [1.0–1.7] | 0.533 | 1.6 ± 2.3 [1.2–2.1] | 0.466 | 9.8 ± 1.1 [9.6–10.1] | 0.300 |
| >10 | - | 62 | - | - | 1.5 ± 1.8 [1.1–2.0] | 1.3 ± 2.7 [0.6–2.0] | 10.0 ± 1.2 [9.7–10.4] | |||
| Days of stimulation | 10.7 | - | 8–14 | 1.18 | - | - | - | - | - | - |
| ≤10 | - | 99 | - | - | 1.3 ± 1.8 [0.9–1.6] | 0.251 | 1.2 ± 2.0 [0.8–1.6] | 0.070 | 9.9 ± 1.1 [9.7–10.2] | 0.483 |
| >10 | - | 78 | - | - | 1.6 ± 1.7 [1.2–2.0] | 1.9 ± 2.8 [1.2–2.5] | 9.9 ± 1.3 [9.6–10.2] | |||
| Total dose of gonadotropins (IU/I) | 2383 | - | 150–3900 | 783.7 | - | - | - | - | - | - |
| <3000 IU/I | - | 113 | - | - | 1.5 ± 1.8 [1.2–1.9] | 0.317 | 1.5 ± 1.8 [1.2–1.9] | 0.625 | 9.9 ± 1.2 [9.7–10.1] | 0.838 |
| ≥3000 IU/I | - | 64 | - | - | 1.4 ± 1.8 [0.9–1.8] | 1.2 ± 1.6 [0.8–1.6] | 9.9 ± 1.1 [9.7–10.2] |
| Variable | Mean | n | Min-Max | SD | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q115) | p-Value (q115) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247) | p-Value (q247) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247/q115) | p-Value (q247/q115) |
|---|---|---|---|---|---|---|---|---|---|---|
| Retrieved oocytes | 9 | - | 0–32 | 5.85 | - | - | - | - | - | - |
| ≤6 | - | 37 | - | - | 1.7 ± 2.0 [1.0–2.4] | 0.268 | 1.7 ± 2.3 [0.9–2.5] | 0.614 | 10.0 ± 1.3 [9.5–10.4] | 0.661 |
| >6 | - | 140 | - | - | 1.3 ± 1.6 [1.1–1.7] | 1.4 ± 2.4 [1.0–1.8] | 9.9 ± 1.2 [9.7–10.1] | |||
| Mature oocytes | 8 | - | 0–27 | 5.41 | - | - | - | - | - | - |
| <8 | - | 101 | - | - | 1.5 ± 1.7 [1.1–1.8] | 0.315 | 1.4 ± 1.8 [1.1–1.8] | 0.848 | 9.9 ± 1.1 [9.7–10.1] | 0.378 |
| 8–12 | - | 35 | - | - | 1.7 ± 2.1 [1.0–2.5] | 1.1 ± 0.9 [0.7–1.4] | 10.1 ± 1.1 [9.7–10.5] | |||
| ≥13 | - | 40 | - | - | 0.9 ± 1.1 [0.6–1.3] | 2.0 ± 4.1 [0.7–3.3] | 9.7 ± 1.3 [9.3–10.2] | |||
| Total embryo number | 5 | - | 0–20 | 4.03 | - | - | - | - | - | - |
| ≤2 | - | 47 | - | - | 1.7 ± 1.8 [1.1–1.9] | 0.257 | 1.5 ± 2.1 [0.9–2.2] | 0.832 | 10.1 ± 1.2 [9.7–10.5] | 0.210 |
| >2 | - | 131 | - | - | 1.3 ± 1.7 [1.0–1.6] | 1.5 ± 2.5 [1.0–1.9] | 9.8 ± 1.1 [9.6–10.1] |
| Variable | n | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q115) | p-Value (q115) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247) | p-Value (q247) | FF cfDNA (ng/uL) Mean ± SD [95%CI] (q247/q115) | p-Value (q247/q115) |
|---|---|---|---|---|---|---|---|
| % embryo fragmentation | - | - | - | - | - | - | - |
| % fragmentation < 20 | 37 | 1.1 ± 1.3 [0.6–1.5] | 0.107 | 1.4 ± 1.3 [0.9–1.9] | 0.937 | 9.5 ± 1.0 [9.2–9.9] | 0.007 |
| % fragmentation ≥ 20 | 81 | 1.6 ± 1.8 [1.2–2.0] | 1.5 ± 2.6 [0.9–2.0] | 10.2 ± 1.2 [9.9–10.4] | |||
| βhCG analysis result | - | - | - | - | - | - | - |
| Positive | 44 | 1.6 ± 1.7 [1.1–2.1] | 0.146 | 1.3 ± 1.4 [0.9–1.8] | 0.043 | 9.9 ± 1.0 [9.5–10.2] | 0.377 |
| Negative | 84 | 1.3 ± 1.7 [1.0–1.7] | 1.4 ± 2.6 [0.8–2.0] | 10.1 ± 1.2 [9.8–10.4] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casteleiro Alves, M.M.; Oliani, L.; Almeida, M.; Cardoso, H.J.; Oliani, A.H.; Breitenfeld, L.; Ramalhinho, A.C. Cell-Free DNA as a New Biomarker of IVF Success, Independent of Any Infertility Factor, Including Endometriosis. Diagnostics 2023, 13, 208. https://doi.org/10.3390/diagnostics13020208
Casteleiro Alves MM, Oliani L, Almeida M, Cardoso HJ, Oliani AH, Breitenfeld L, Ramalhinho AC. Cell-Free DNA as a New Biomarker of IVF Success, Independent of Any Infertility Factor, Including Endometriosis. Diagnostics. 2023; 13(2):208. https://doi.org/10.3390/diagnostics13020208
Chicago/Turabian StyleCasteleiro Alves, Maria Manuel, Luísa Oliani, Micaela Almeida, Henrique José Cardoso, António Hélio Oliani, Luiza Breitenfeld, and Ana Cristina Ramalhinho. 2023. "Cell-Free DNA as a New Biomarker of IVF Success, Independent of Any Infertility Factor, Including Endometriosis" Diagnostics 13, no. 2: 208. https://doi.org/10.3390/diagnostics13020208
APA StyleCasteleiro Alves, M. M., Oliani, L., Almeida, M., Cardoso, H. J., Oliani, A. H., Breitenfeld, L., & Ramalhinho, A. C. (2023). Cell-Free DNA as a New Biomarker of IVF Success, Independent of Any Infertility Factor, Including Endometriosis. Diagnostics, 13(2), 208. https://doi.org/10.3390/diagnostics13020208