
Basic Principles of Rotational Thromboelastometry (ROTEM®) and the Role of ROTEM—Guided Fibrinogen Replacement Therapy in the Management of Coagulopathies
 and
and 
Abstract
:1. Introduction
2. The Measuring Principle of ROTEM
2.1. INTEM Assay
2.2. EXTEM Assay
2.3. FIBTEM Assay
2.4. APTEM Assay
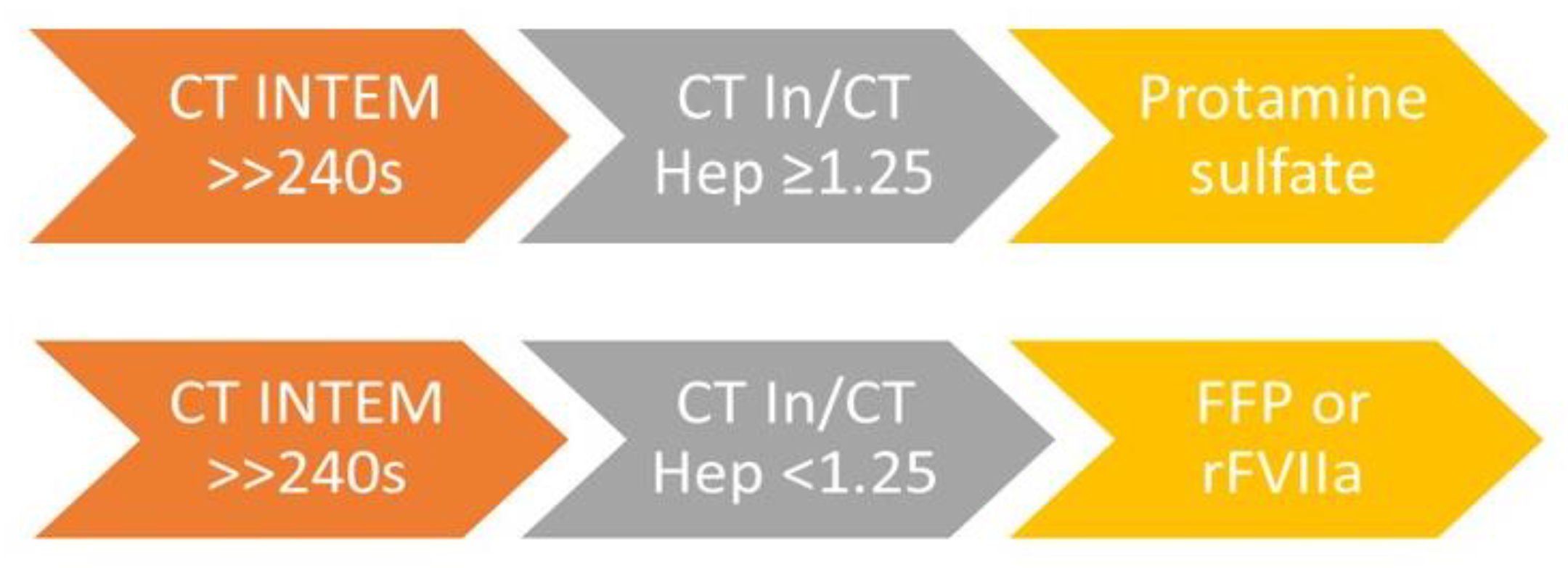
2.5. HEPTEM Assay
3. Interpretation of Results
4. The Importance of ROTEM Examination in the Management of Acquired Coagulopathies



5. The Application of ROTEM in the Management of Bleeding in Patients with Congenital Fibrinogen Disorders
6. Limitations of ROTEM
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nichols, J.H. Point-of-Care Testing. In Contemporary Practice in Clinical Chemistry, 4th ed.; AACC Press: Washington, DC, USA, 2020; pp. 323–336. ISBN 9780128154991. [Google Scholar]
- Görlinger, K.; Dirkmann, D.; Hanke, A. Rotational Thromboelastometry (ROTEM®). In Trauma Induced Coagulopathy; Gonzalez, E., Moore, H., Moore, E., Eds.; Springer: Cham, Switzerland, 2016; pp. 267–298. [Google Scholar]
- Carll, T.; Wool, G.D. Basic principles of viscoelastic testing. Transfusion 2020, 60, S1–S9. [Google Scholar] [CrossRef]
- Volod, O.; Bunch, C.M.; Zackariya, N.; Moore, E.E.; Moore, H.B.; Kwaan, H.C.; Neal, M.D.; Al-Fadhl, M.D.; Patel, S.S.; Wiarda, G.; et al. Viscoelastic Hemostatic Assays: A Primer on Legacy and New Generation Devices. J. Clin. Med. 2022, 11, 860. [Google Scholar] [CrossRef]
- Whiting, D.; DiNardo, J.A. TEG and ROTEM: Technology and clinical applications. Am. J. Hematol. 2014, 89, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Theusinger, O.M.; Schröder, C.M.; Eismon, J.; Emmert, M.Y.; Seifert, B.; Spahn, D.R.; Baulig, W. The influence of laboratory coagulation tests and clotting factor levels on Rotation Thromboelastometry (ROTEM(R)) during major surgery with hemorrhage. Anesth. Analg. 2013, 117, 314–321. [Google Scholar] [CrossRef] [PubMed]
- De Vries, J.J.; Veen, C.S.B.; Snoek, C.J.M.; Kruip, M.J.H.A.; de Maat, M.P.M. FIBTEM clot firmness parameters correlate well with the fibrinogen concentration measured by the Clauss assay in patients and healthy subjects. Scand. J. Clin. Lab. Investig. 2020, 80, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Harr, J.N.; Moore, E.E.; Chin, T.L.; Chapman, M.P.; Ghasabyan, A.; Stringham, J.R.; Banerjee, A.; Silliman, C.C. Viscoelastic hemostatic fibrinogen assays detect fibrinolysis early. Eur. J. Trauma. Emerg. Surg. 2015, 41, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Skornova, I.; Slavik, L.; Stasko, J.; Kubisz, P.; Krcova, V.; Bartova, L.; Bradacova, P.; Macichova, M.; Ulehlova, J.; Vazanova, A.; et al. Hemostáza-Laboratórne Metódy, ich Využitie a Interpretácia vo Vybraných Klinických Situáciách. [Haemostasis—Laboratory Methods, Their Use and Interpretation in Selected Clinical Situations]; Martin Slovakia: Bratislava, Slovakia, 2020; pp. 148–154. ISBN 978-80-89694-78-5. [Google Scholar]
- Kinoshita, H.; Saito, J.; Nakai, K.; Noguchi, S.; Takekawa, D.; Tamai, Y.; Kitayama, M.; Hirota, K. Clotting functional stability of withdrawing blood in storage for acute normovolemic hemodilution: A pilot study. J. Anesth. 2021, 35, 35–42. [Google Scholar] [CrossRef]
- Maegele, M.; Lefering, R.; Yucel, N.; Tjardes, T.; Rixen, D.; Paffrath, T.; Simanski, C.; Neugebauer, E.; Bouillon, B.; AG Polytrauma of the German Trauma Society (DGU). Early coagulopathy in multiple injury: An analysis from the German Trauma Registry on 8724 patients. Injury 2007, 38, 298–304. [Google Scholar] [CrossRef]
- Soonam, J.; Nitty, S.M.; Sukesh, C.N. Early prediction of coagulopathy in acquired bleeding disorders—Revisited using rotational thromboelastometry. Int. J. Contemp. Med. Res. 2019, 6, 1–5. [Google Scholar]
- Fries, D.; Innerhofer, P.; Reif, C.; Streif, W.; Klingler, A.; Schobersberger, W.; Velik-Salchner, C.; Friesenecker, B. The Effect of Fibrinogen Substitution on Reversal of Dilutional Coagulopathy: An In Vitro Model. Anesth. Analg. 2006, 102, 347–351. [Google Scholar] [CrossRef]
- De Lorenzo, C.; Calatzis, A.; Welsch, U.; Heindl, B. Fibrinogen concentrate reverses dilutional coagulopathy induced in vitro by saline but not by hydroxyethyl starch 6%. Anesth. Analg. 2006, 102, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Lier, H.; Vorweg, M.; Hanke, A.; Görlinger, K. Thromboelastometry guided therapy of severe bleeding. Essener Runde algorithm. Hamostaseologie 2013, 33, 51–61. [Google Scholar]
- Walsh, M.; Fritz, S.; Hake, D.; Son, M.; Greve, S.; Jbara, M.; Chitta, S.; Fritz, B.; Miller, A.; Bader, M.K.; et al. Targeted thromboelastographic (TEG) blood component and pharmacologic hemostatic therapy in traumatic and acquired coagulopathy. Curr. Drug Targets 2016, 17, 954–970. [Google Scholar] [CrossRef] [PubMed]
- Blayney, A.; McCullough, J.; Wake, E.; Walters, K.; Campbell, D.; Ho, D.; Chan, E.; Chalasani, A.; Winearls, J. Substitution of ROTEM FIBTEM A5 for A10 in trauma: An observational study building a case for more rapid analysis of coagulopathy. Eur. J. Trauma. Emerg. Surg. 2022, 48, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Tsantes, A.G.; Papadopoulos, D.V.; Trikoupis, I.G.; Tsante, K.A.; Mavrogenis, A.F.; Koulouvaris, P.; Vaiopoulos, A.G.; Piovani, D.; Nikolopoulos, G.K.; Kokoris, S.I.; et al. The Prognostic Performance of Rotational Thromboelastometry for Excessive Bleeding and Increased Transfusion Requirements in Hip Fracture Surgeries. Thromb. Haemost. 2022, 122, 895–904. [Google Scholar] [CrossRef]
- Tsantes, A.G.; Papadopoulos, D.V.; Roustemis, A.G.; Trikoupis, I.G.; Piovani, D.; Tsante, K.A.; Mantzios, P.G.; Mavrogenis, A.F.; Sokou, R.; Kokoris, S.I.; et al. Rotational Thromboelastometry Predicts Transfusion Requirements in Total Joint Arthroplasties. Semin. Thromb. Hemost. 2023, 49, 134–144. [Google Scholar] [CrossRef]
- Ichikawa, J.; Kodaka, M.; Nishiyama, K.; Hirasaki, Y.; Ozaki, M.; Komori, M. Reappearance of circulating heparin in whole blood heparin concentration-based management does not correlate with postoperative bleeding after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2014, 28, 1003–1007. [Google Scholar] [CrossRef]
- Boer, C.; Meesters, M.I.; Milojevic, M.; Benedetto, U.; Bolliger, D.; von Heymann, C.; Jeppsson, A.; Koster, A.; Osnabrugge, R.L.; Ranucci, M.; et al. EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2018, 32, 88–120. [Google Scholar] [CrossRef]
- Karkouti, K.; Callum, J.; Crowther, M.A.; McCluskey, S.A.; Pendergrast, J.; Tait, G.; Yau, T.M.; Beattie, W.S. The relationship between fibrinogen levels after cardiopulmonary bypass and large volume red cell transfusion in cardiac surgery: An observational study. Anesth. Analg. 2013, 117, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Mace, H.; Lightfoot, N.; McCluskey, S.; Selby, R.; Roy, D.; Timoumi, T.; Karkouti, K. Validity of Thromboelastometry for Rapid Assessment of Fibrinogen Levels in Heparinized Samples During Cardiac Surgery: A Retrospective, Single-center, Observational Study. J. Cardiothorac. Vasc. Anesth. 2016, 30, 90–95. [Google Scholar] [CrossRef]
- Reinhöfer, M.; Brauer, M.; Franke, U.; Barz, D.; Marx, G.; Lösche, W. The value of rotation thromboelastometry to monitor disturbed perioperative haemostasis and bleeding risk in patients with cardiopulmonary bypass. Blood Coagul. Fibrinolysis 2008, 19, 212–219. [Google Scholar] [CrossRef]
- Görlinger, K.; Shore-Lesserson, L.; Dirkmann, D.; Hanke, A.A.; Rahe-Meyer, N.; Tanaka, K.A. Management of hemorrhage in cardiothoracic surgery. J. Cardiothorac. Vasc. Anesth. 2013, 27 (Suppl. 4), S20–S34. [Google Scholar] [CrossRef]
- Ranucci, M.; Pistuddi, V.; Baryshnikova, E.; Colella, D.; Bianchi, P. Fibrinogen Levels After Cardiac Surgical Procedures: Association with Postoperative Bleeding, Trigger Values, and Target Values. Ann. Thorac. Surg. 2016, 102, 78–85. [Google Scholar] [CrossRef]
- Giani, M.; Russotto, V.; Pozzi, M.; Forlini, C.; Fornasari, C.; Villa, S.; Avalli, L.; Rona, R.; Foti, G. Thromboelastometry, Thromboelastography, and Conventional Tests to Assess Anticoagulation During Extracorporeal Support: A Prospective Observational Study. ASAIO J. 2021, 67, 196–200. [Google Scholar] [CrossRef]
- Holcomb, J.B.; Wade, C.E.; Michalek, J.E.; Chisholm, G.B.; Zarzabal, L.A.; Schreiber, M.A.; Gonzalez, E.A.; Pomper, G.J.; Perkins, J.G.; Spinella, P.C.; et al. Increased plasma and platelet to red blood cell ratios improves outcome in 466 massively transfused civilian trauma patients. Ann. Surg. 2008, 248, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, J.B.; Tilley, B.C.; Baraniuk, S.; Fox, E.E.; Wade, C.E.; Podbielski, J.M.; del Junco, D.J.; Brasel, K.J.; Bulger, E.M.; Callcut, R.A.; et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs. a 1:1:2 ratio and mortality in patients with severe trauma: The PROPPR randomized clinical trial. JAMA 2015, 313, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Morse, B.C.; Dente, C.J.; Hodgman, E.I.; Shaz, B.H.; Winkler, A.; Nicholas, J.M.; Wyrzykowski, A.D.; Rozycki, G.S.; Feliciano, D.V. Outcomes after massive transfusion in nondrama patients in the era of damage control resuscitation. Am. Surg. 2012, 78, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Matzek, L.J.; Kurian, E.B.; Frank, R.D.; Weister, T.J.; Gajic, O.; Kor, D.J.; Warner, M.A. Plasma, platelet and red blood cell transfusion ratios for life-threatening non-traumatic haemorrhage in medical and post-surgical patients: An observational study. Vox Sang. 2022, 117, 361–370. [Google Scholar] [CrossRef]
- Görlinger, K.; Pérez-Ferrer, A.; Dirkmann, D.; Saner, F.; Maegele, M.; Calatayud, Á.A.P.; Kim, T.Y. The role of evidence-based algorithms for rotational thromboelastometry-guided bleeding management. Korean J. Anesthesiol. 2019, 72, 297–322. [Google Scholar] [CrossRef]
- Maegele, M. Modern coagulation management in bleeding trauma patients: Point-of-care guided administration of coagulation factor concentrates and hemostatic agents. Med. Klin. Intensiv. Notfmed. 2019, 114, 400–409. [Google Scholar] [CrossRef]
- Requena, T.; Koller, T.; Paniagua, P.; Gil, J.M.; Fernandez, J.A.; Moral, V. Recommended thresholds for fibrinogen substitution (FS) in rotational thrombelastometry (ROTEM) subtest FIBTEM and conventional Clauss method (CM) do not correspond: 6AP6-6. Eur. J. Anaesthesiol. 2011, 28, 95. [Google Scholar] [CrossRef]
- Levy, J.H.; Welsby, I.; Goodnough, L.T. Fibrinogen as a therapeutic target for bleeding: A review of critical levels and replacement therapy. Transfusion 2014, 54, 1389–1405. [Google Scholar] [CrossRef]
- Franchini, M.; Lippi, G. Fibrinogen replacement therapy: A critical review of the literature. Blood Transfus. 2012, 10, 23–27. [Google Scholar]
- Simurda, T.; Brunclikova, M.; Asselta, R.; Caccia, S.; Zolkova, J.; Kolkova, Z.; Loderer, D.; Skornova, I.; Hudecek, J.; Lasabova, Z. Genetic Variants in the FGB and FGG Genes Mapping in the Beta and Gamma Nodules of the Fibrinogen Molecule in Congenital Quantitative Fibrinogen Disorders Associated with a Thrombotic Phenotype. Int. J. Mol. Sci. 2020, 21, 4616. [Google Scholar] [CrossRef]
- Görlinger, K.; Sakai, T.; Dirkmann, D.; Planinsic, R.; Saner, F. Bleeding Related to Liver Transplant. In Management of Bleeding Patients; Teruya, J., Ed.; Springer: Cham, Switzerland, 2016. [Google Scholar] [CrossRef]
- Simurda, T.; Zolkova, J.; Snahnicanova, Z.; Loderer, D.; Skornova, I.; Sokol, J.; Hudecek, J.; Stasko, J.; Lasabova, Z.; Kubisz, P. Identification of Two Novel Fibrinogen Bβ Chain Mutations in Two Slovak Families with Quantitative Fibrinogen Disorders. Int. J. Mol. Sci. 2017, 19, 100. [Google Scholar] [CrossRef] [PubMed]
- Koller, T.; Parera Ruiz, A.; Diaz-Ricart, M.; Gómez Caro, A.M. Role of fibrinogen concentrates for treatment of critical perioperative hemorrhage. Drugs Today 2021, 57, 219–239. [Google Scholar] [CrossRef] [PubMed]
- Manco-Johnson, M.J.; Dimichele, D.; Castaman, G.; Fremann, S.; Knaub, S.; Kalina, U.; Peyvandi, F.; Piseddu, G.; Mannucci, P.; FIBRINOGEN CONCENTRATE STUDY GROUP. Pharmacokinetics and safety of fibrinogen concentrate. J. Thromb. Haemost. 2009, 7, 2064–2069. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.T.; Nascimento, B.; Beckett, A. Thromboelastography and Thromboelastometry in Assessment of Fibrinogen Deficiency and Prediction for Transfusion Requirement: A Descriptive Review. BioMed Res. Int. 2018, 2018, 7020539. [Google Scholar] [CrossRef]
- Simurda, T.; Asselta, R.; Zolkova, J.; Brunclikova, M.; Dobrotova, M.; Kolkova, Z.; Loderer, D.; Skornova, I.; Hudecek, J.; Lasabova, Z.; et al. Congenital Afibrinogenemia and Hypofibrinogenemia: Laboratory and Genetic Testing in Rare Bleeding Disorders with Life-Threatening Clinical Manifestations and Challenging Management. Diagnostics 2021, 11, 2140. [Google Scholar] [CrossRef]
- Szanto, T.; Lassila, R.; Lemponen, M.; Lehtinen, E.; Neerman-Arbez, M.; Casini, A. Whole Blood Thromboelastometry by ROTEM and Thrombin Generation by Genesia According to the Genotype and Clinical Phenotype in Congenital Fibrinogen Disorders. Int. J. Mol. Sci. 2021, 22, 2286. [Google Scholar] [CrossRef]
- Zhou, J.; Xin, Y.; Ding, Q.; Chen, Y.; Dai, J.; Lu, Y.; Wu, X.; Liang, Q.; Wang, H.; Wang, X. Thromboelastography predicts risks of obstetric complication occurrence in (hypo)dysfibrinogenemia patients under non-pregnant state. Clin. Exp. Pharmacol. Physiol. 2016, 43, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Khunakanan, S.; Akaraborworn, O.; Sangthong, B.; Thongkhao, K. Correlation between Maximum Clot Firmness in FIBTEM and Fibrinogen Level in Critical Trauma Patients. Crit. Care Res. Pr. 2019, 2019, 2756461. [Google Scholar] [CrossRef] [PubMed]
- Treliński, J.; Pachniewska, K.; Matczak, J.; Robak, M.; Chojnowski, K. Assessment of Selected ROTEM Parameters, Kinetics of Fibrinogen Polymerization and Plasmin Amidolytic Activity in Patients with Congenital Fibrinogen Defects. Adv. Clin. Exp. Med. 2016, 25, 1255–1263. [Google Scholar] [CrossRef] [PubMed]
- Wikkelsø, A.; Wetterslev, J.; Møller, A.M.; Afshari, A. Thromboelastography (TEG) or thromboelastometry (ROTEM) to monitor haemostatic treatment versus usual care in adults or children with bleeding. Cochrane Database Syst. Rev. 2016, 2016, CD007871. [Google Scholar] [CrossRef]
- Kuiper, G.J.A.J.M.; Kleinegris, M.C.F.; van Oerle, R.; Spronk, H.M.; Lancé, M.D.; Ten Cate, H.; Henskens, Y.M. Validation of a modified thromboelastometry approach to detect changes in fibrinolytic activity. Thromb. J. 2016, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Schöchl, H.; Nienaber, U.; Hofer, G.; Voelckel, W.; Jambor, C.; Scharbert, G.; Kozek-Langenecker, S.; Solomon, C. Goal-directed coagulation management of major trauma patients using thromboelastometry (ROTEM)-guided administration of fibrinogen concentrate and prothrombin complex concentrate. Crit. Care 2010, 14, 55. [Google Scholar] [CrossRef]
- Weber, C.F.; Klaus Görlinger, K.; Meininger, D.; Herrmann, E.; Bingold, T.; Moritz, A.; Cohn, L.H.; Zacharowski, K. Point-of-Care Testing: A Prospective, Randomized Clinical Trial of Efficacy in Coagulopathic Cardiac Surgery Patients. Anesthesiology 2012, 117, 531–547. [Google Scholar] [CrossRef]
- Topf, H.G.; Strasser, E.R.; Breuer, G.; Rascher, W.; Rauh, M.; Fahlbusch, F.B. Closing the gap—Detection of clinically relevant von Willebrand disease in emergency settings through an improved algorithm based on rotational Thromboelastometry. BMC Anesth. 2019, 19, 10. [Google Scholar] [CrossRef]
- Simurda, T.; Drotarova, M.; Skornova, I.; Dobrotova, M.; Brunclikova, M.; Necas, L.; Cibula, Z.; Kubisz, P.; Stasko, J. Perioperative Monitoring with Rotational Thromboelastometry in a Severe Hemophilia A Patient Undergoing Elective Ankle Surgery. In Seminars in Thrombosis and Hemostasis; Thieme Medical Publishers, Inc.: New York, NY, USA, 2023. [Google Scholar]
- Simurda, T.; Casini, A.; Stasko, J.; Hudecek, J.; Skornova, I.; Vilar, R.; Neerman-Arbez, M.; Kubisz, P. Perioperative management of a severe congenital hypofibrinogenemia with thrombotic phenotype. Thromb. Res. 2020, 188, 1–4. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assay | Investigated Area | Used Reagent |
|---|---|---|
| INTEM | Intrinsic coagulation pathway FXII, FXI, FIX, FVIII, FX, FV, FII, FI, fibrin, platelets, fibrinolysis | partial thromboplastin, ellagic acid |
| EXTEM | Extrinsic coagulation pathway FVII, FX, FV, FII, FI, fibrin, platelets, fibrinolysis | recombinant tissue factor, phospholipids |
| FIBTEM | Contribution of fibrinogen to the clot formation after platelet inactivation | recalcification and platelet inhibitor cytochalasin D |
| APTEM | Inhibition of fibrinolysis, comparison to EXTEM can indicate/detect hyperfibrinolysis | recalcification and fibrinolysis inhibitor aprotinin/tranexamic acid |
| HEPTEM | Heparin inactivation in heparinized patients | recalcification, heparinase I * |
| Assay | CT (s) | CFT (s) | Angle α (°) | A10 (mm) | A20 (mm) | MCF (mm) | LI30 (%) | ML (%) in 1 h |
|---|---|---|---|---|---|---|---|---|
| EXTEM | 38–79 | 34–159 | 63–83 | 43–65 | 50–71 | 50–72 | 94–100 | <15 |
| INTEM | 100–240 | 30–110 | 70–83 | 44–66 | 50–71 | 50–72 | 94–100 | <15 |
| FIBTEM | - | - | - | 7–23 | 8–24 | 9–25 | - | - |
| APTEM | A better clot formation in APTEM compared to EXTEM indicates an in vitro effect of antifibrinolytics (aprotinin and tranexamic acid) | |||||||
| HEPTEM | A better clot formation in HEPTEM compared to INTEM indicates the presence of heparin or heparin-like anticoagulants | |||||||
| Targeted Increase in FIBTEM A10 (A5) (mm) | Dose of Fibrinogen (mg/kg) | Fibrinogen Concentrate (mL/kg) |
|---|---|---|
| 2 | 12.5 | 0.6 (1 g per 80 kg) |
| 4 | 25.0 | 1.2 (2 g per 80 kg) |
| 6 | 37.5 | 1.9 (3 g per 80 kg) |
| 8 | 50.0 | 2.5 (4 g per 80 kg) |
| 10 | 62.5 | 3.1 (5 g per 80 kg) |
| 12 | 75.0 | 3.8 (6 g per 80 kg) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drotarova, M.; Zolkova, J.; Belakova, K.M.; Brunclikova, M.; Skornova, I.; Stasko, J.; Simurda, T. Basic Principles of Rotational Thromboelastometry (ROTEM®) and the Role of ROTEM—Guided Fibrinogen Replacement Therapy in the Management of Coagulopathies. Diagnostics 2023, 13, 3219. https://doi.org/10.3390/diagnostics13203219
Drotarova M, Zolkova J, Belakova KM, Brunclikova M, Skornova I, Stasko J, Simurda T. Basic Principles of Rotational Thromboelastometry (ROTEM®) and the Role of ROTEM—Guided Fibrinogen Replacement Therapy in the Management of Coagulopathies. Diagnostics. 2023; 13(20):3219. https://doi.org/10.3390/diagnostics13203219
Chicago/Turabian StyleDrotarova, Miroslava, Jana Zolkova, Kristina Maria Belakova, Monika Brunclikova, Ingrid Skornova, Jan Stasko, and Tomas Simurda. 2023. "Basic Principles of Rotational Thromboelastometry (ROTEM®) and the Role of ROTEM—Guided Fibrinogen Replacement Therapy in the Management of Coagulopathies" Diagnostics 13, no. 20: 3219. https://doi.org/10.3390/diagnostics13203219