
The Visual Patient Avatar ICU Facilitates Information Transfer of Written Information by Visualization: A Multicenter Comparative Eye-Tracking Study

 , ,
, ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
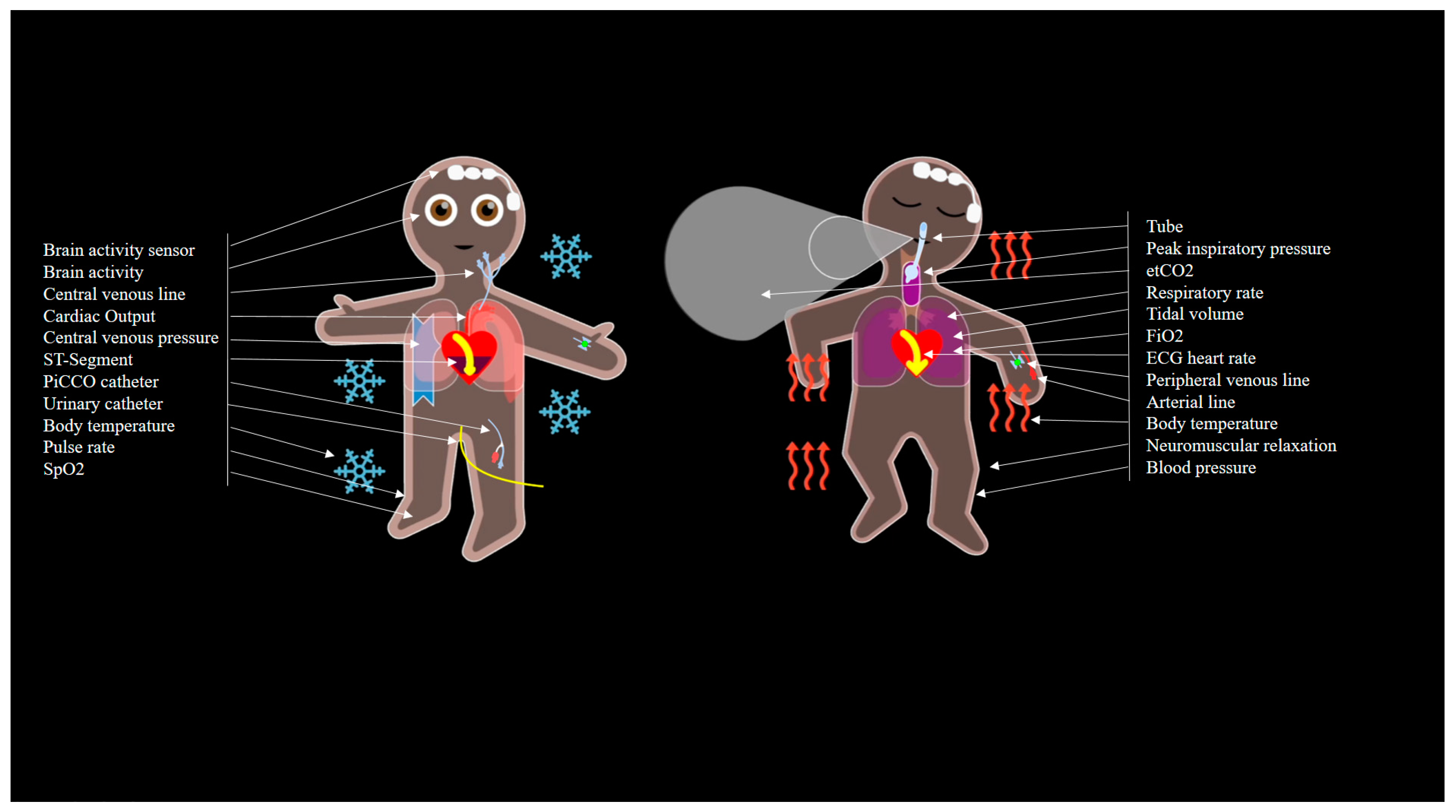
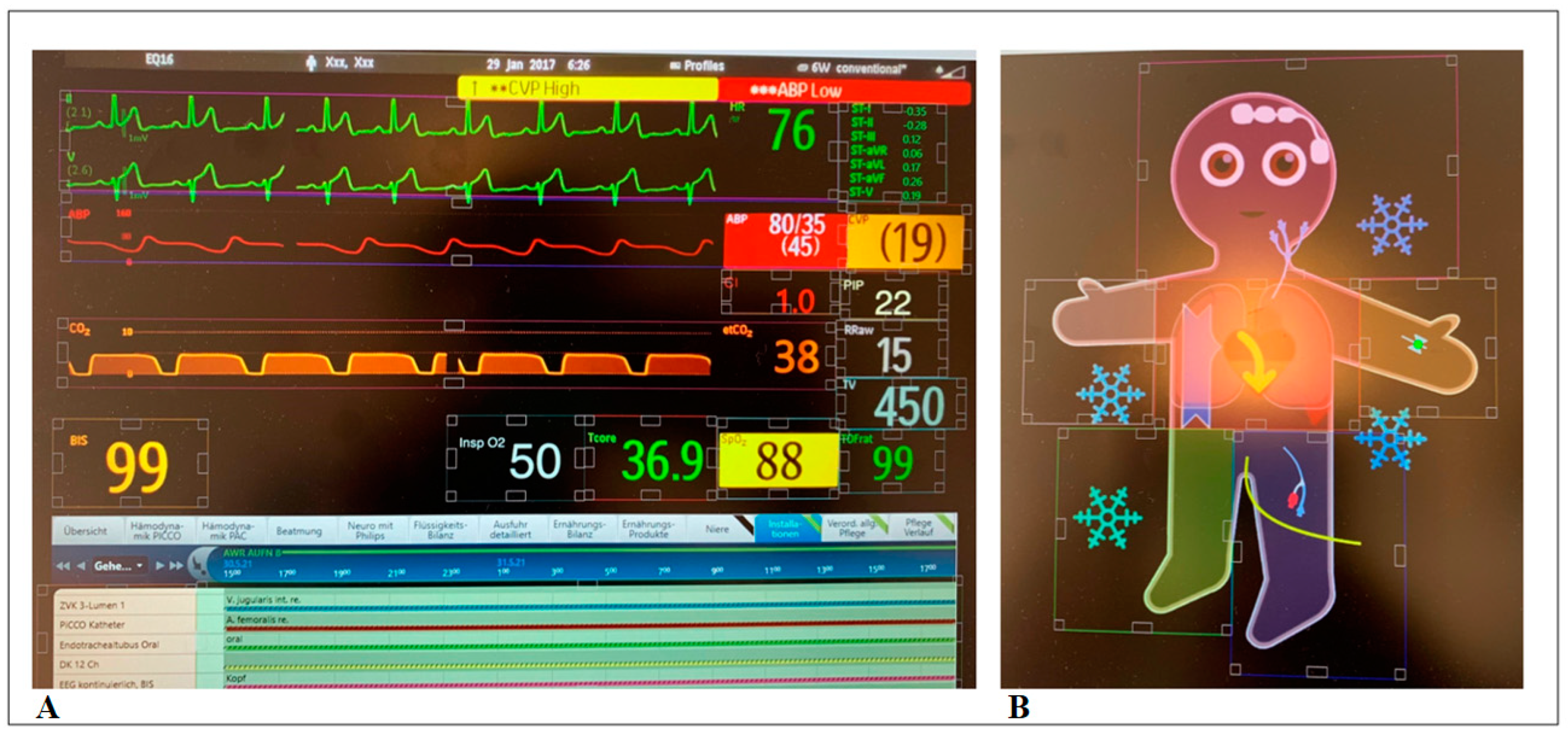
2.1. Description of the Visual-Patient-Avatar Technology
2.2. Study Design
2.3. Data Collection and Analysis
2.4. Outcomes and Statistical Analysis
2.4.1. Outcomes
2.4.2. Statistical Analysis
3. Results
3.1. Study and Participant Characteristics
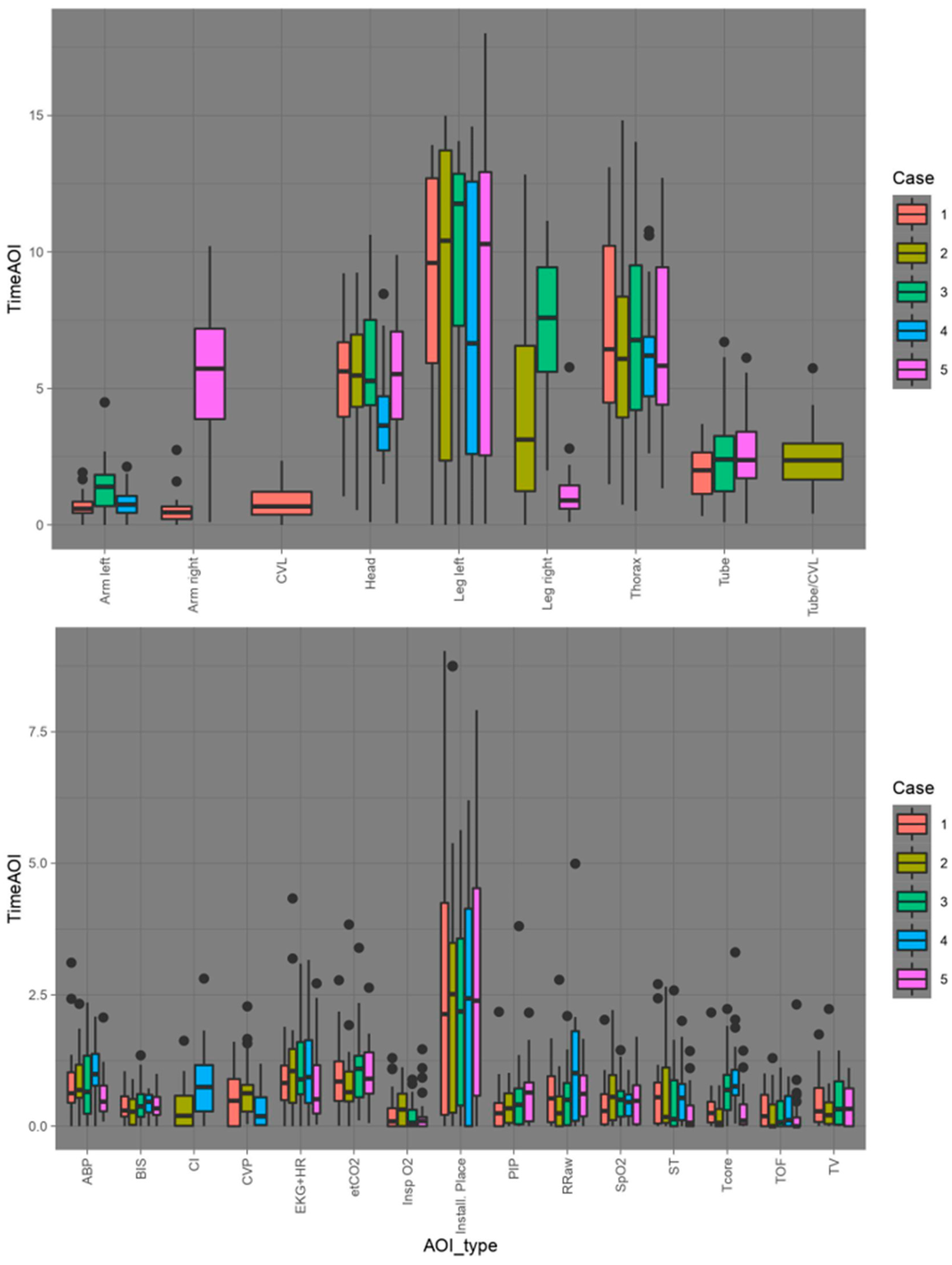
3.2. Areas of Interest
3.3. Alarms
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gelb, A.W.; Morriss, W.W.; Johnson, W.; Merry, A.F. World Health Organization-World Federation of Societies of Anaesthesiologists (WHO-WFSA) International Standards for a Safe Practice of Anesthesia. Can. J. Anaesth. 2018, 65, 698–708. [Google Scholar] [CrossRef] [PubMed]
- Weiser, T.G.; Haynes, A.B.; Molina, G.; Lipsitz, S.R.; Esquivel, M.M.; Uribe-Leitz, T.; Fu, R.; Azad, T.; Chao, T.E.; Berry, W.R.; et al. Size and distribution of the global volume of surgery in 2012. Bull. World Health Organ. 2016, 94, 201F–209F. [Google Scholar] [CrossRef]
- Schulz, C.M.; Endsley, M.R.; Kochs, E.F.; Gelb, A.W.; Wagner, K.J. Situation awareness in anesthesia: Concept and RESEARCH. Anesthesiology 2013, 118, 729–742. [Google Scholar] [CrossRef] [PubMed]
- Endsley, M.R. Designing for Situation Awareness: An Approach to User-Centered Design; CRC Press: Boca Raton, FL, USA, 2012; 396p, ISBN 1420063553. [Google Scholar]
- Mack, A.; Pappas, Z.; Silverman, M.; Gay, R. What we see: Inattention and the capture of attention by meaning. Conscious Cogn. 2002, 11, 488–506. [Google Scholar] [CrossRef] [PubMed]
- De Cassai, A.; Negro, S.; Geraldini, F.; Boscolo, A.; Sella, N.; Munari, M.; Navalesi, P. Inattentional blindness in anesthesiology: A gorilla is worth one thousand words. PLoS ONE 2021, 16, e0257508. [Google Scholar] [CrossRef]
- Simons, D.J.; Chabris, C.F. Gorillas in our midst: Sustained inattentional blindness for dynamic events. Perception 1999, 28, 1059–1074. [Google Scholar] [CrossRef]
- Ahmed, A.H.; Giri, J.; Kashyap, R.; Singh, B.; Dong, Y.; Kilickaya, O.; Erwin, P.J.; Murad, M.H.; Pickering, B.W. Outcome of adverse events and medical errors in the intensive care unit: A systematic review and meta-analysis. Am. J. Med Qual. 2013, 30, 23–30. [Google Scholar] [CrossRef] [PubMed]
- A Makary, M.; Daniel, M. Medical error—The third leading cause of death in the US. BMJ 2016, 353, i2139. [Google Scholar] [CrossRef]
- Garrouste-Orgeas, M.; Timsit, J.F.; Vesin, A.; Schwebel, C.; Arnodo, P.; Lefrant, J.Y.; Souweine, B.; Tabah, A.; Charpentier, J.; Gontier, O.; et al. Selected medical errors in the intensive care unit: Results of the iatroref study: Parts I and II. Am. J. Respir. Crit. Care Med. 2010, 181, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Drews, F.A.; Westenskow, D.R. The right picture is worth a thousand numbers: Data displays in anesthesia. Hum. Factors: J. Hum. Factors Ergon. Soc. 2006, 48, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Ford, S.; Birmingham, E.; King, A.; Lim, J.; Ansermino, J.M.; Ford, S.; Birmingham, E.; King, A.; Lim, J.; Ansermino, J.M. At-a-glance monitoring: Covert observations of anesthesiologists in the operating room. Obstet. Anesth. Dig. 2010, 111, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Hofmaenner, D.A.; Herling, A.; Klinzing, S.; Wegner, S.; Lohmeyer, Q.; Schuepbach, R.A.; Buehler, P.K. Use of eye tracking in analyzing distribution of visual attention among critical care nurses in daily professional life: An observational study. J. Clin. Monit. Comput. 2020, 35, 1511–1518. [Google Scholar] [CrossRef]
- Schulz, C.M.; Krautheim, V.; Hackemann, A.; Kreuzer, M.; Kochs, E.F.; Wagner, K.J. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol. 2015, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Endsley, M.R. Toward a Theory of situation awareness in dynamic systems. Hum. Factors J. Hum. Factors Ergon. Soc. 1995, 37, 32–64. [Google Scholar] [CrossRef]
- Garot, O.; Rössler, J.; Pfarr, J.; Ganter, M.T.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Avatar-based versus conventional vital sign display in a central monitor for monitoring multiple patients: A multicenter computer-based laboratory study. BMC Med. Inform. Decis. Mak. 2020, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Pfarr, J.; Ganter, M.T.; Spahn, D.R.; Noethiger, C.B.; Tscholl, D.W. Avatar-based patient monitoring with peripheral vision: A multicenter comparative eye-tracking study. J. Med. Internet Res. 2019, 21, e13041. [Google Scholar] [CrossRef]
- Roche, T.R.; Said, S.; Braun, J.; Maas, E.J.; Machado, C.; Grande, B.; Kolbe, M.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Avatar-based patient monitoring in critical anaesthesia events: A randomised high-fidelity simulation study. Br. J. Anaesth. 2021, 126, 1046–1054. [Google Scholar] [CrossRef]
- Tscholl, D.; Handschin, L.; Neubauer, P.; Weiss, M.; Seifert, B.; Spahn, D.; Noethiger, C. Using an animated patient avatar to improve perception of vital sign information by anaesthesia professionals. Br. J. Anaesth. 2018, 121, 662–671. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Rössler, J.; Handschin, L.; Seifert, B.; Spahn, D.R.; Nöthiger, C.B. The Mechanisms responsible for improved information transfer in avatar-based patient monitoring: Multicenter comparative eye-tracking study. J. Med. Internet Res. 2020, 22, e15070. [Google Scholar] [CrossRef] [PubMed]
- Tscholl, D.W.; Rössler, J.; Said, S.; Kaserer, A.; Spahn, D.R.; Nöthiger, C.B. Situation awareness-oriented patient monitoring with visual patient technology: A qualitative review of the primary research. Sensors 2020, 20, 2112. [Google Scholar] [CrossRef]
- Wittgenstein, L. Tractatus Logico-Philosophicus: [Reprinted, with a Few Corrections]; Harcourt, Brace: New York, NY, USA, 1933. [Google Scholar]
- Bergauer, L.; Braun, J.; Roche, T.R.; Meybohm, P.; Hottenrott, S.; Zacharowski, K.; Raimann, F.J.; Rivas, E.; López-Baamonde, M.; Ganter, M.T.; et al. Avatar-based patient monitoring improves information transfer, diagnostic confidence and reduces perceived workload in intensive care units: Computer-based, multicentre comparison study. Sci. Rep. 2023, 13, 5908. [Google Scholar] [CrossRef] [PubMed]
- Klausen, A.; Röhrig, R.; Lipprandt, M. Feasibility of eyetracking in critical care environments—A systematic review. Stud. Health Technol. Inform. 2016, 228, 604–608. [Google Scholar] [CrossRef]
- Holmqvist, K.; Andersson, R. Eye-Tracking: A Comprehensive Guide to Methods, Paradigms and Measures; Lund Eye-Tracking Research Institute, Lund University: Lund, Sweden, 2017; ISBN 978-1979484893. [Google Scholar]
- Schulz, C.; Schneider, E.; Fritz, L.; Vockeroth, J.; Hapfelmeier, A.; Wasmaier, M.; Kochs, E. Eye tracking for assessment of workload: A pilot study in an anaesthesia simulator environment. Br. J. Anaesth. 2011, 106, 44–50. [Google Scholar] [CrossRef] [PubMed]
- de Winter, J.C.F.; Eisma, Y.B.; Cabrall, C.D.D.; Hancock, P.A.; Stanton, N.A. Situation awareness based on eye movements in relation to the task environment. Cogn. Technol. Work. 2018, 21, 99–111. [Google Scholar] [CrossRef]
- Harezlak, K.; Kasprowski, P. Application of eye tracking in medicine: A survey, research issues and challenges. Comput. Med Imaging Graph. 2017, 65, 176–190. [Google Scholar] [CrossRef] [PubMed]
- Just, M.A.; Carpenter, P.A. A theory of reading: From eye fixations to comprehension. Psychol. Rev. 1980, 87, 329–354. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.G.; Staveland, L.E. Development of NASA-TLX (Task Load Index): Results of Empirical and Theoretical Research. In Advances in Psychology; Meshkati, N., Hancock, P.A., Eds.; North-Holland: Amsterdam, The Netherlands, 1988; pp. 139–183. [Google Scholar]
- Said, S.; Gozdzik, M.; Roche, T.R.; Braun, J.; Rössler, J.; Kaserer, A.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Validation of the Raw National Aeronautics and Space Administration Task Load Index (NASA-TLX) Questionnaire to Assess Perceived Workload in Patient Monitoring Tasks: Pooled Analysis Study Using Mixed Models. J. Med. Internet Res. 2020, 22, e19472. [Google Scholar] [CrossRef] [PubMed]
- Grier, R.A.; Warm, J.S.; Dember, W.N.; Matthews, G.; Galinsky, T.L.; Szalma, J.L.; Parasuraman, R. The vigilance decrement reflects limitations in effortful attention, not mindlessness. Hum. Factors J. Hum. Factors Ergon. Soc. 2003, 45, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.L.; Reed, V.S.; Walling, J.R. Pictorial superiority effect. J. Exp. Psychol. Hum. Learn. 1976, 2, 523–528. [Google Scholar] [CrossRef]
- Degani, A.; Jorgensen, C.; Iverson, D.; Shafto, M.; Olson, L. On Organization of Information: Approach and Early Work; NASA Ames Research Center: Mountain View, CA, USA, 2009. [Google Scholar]
- Ljubenovic, A.; Said, S.; Braun, J.; Grande, B.; Kolbe, M.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W.; Roche, T.R. Anesthesia providers’ visual attention in simulated anesthesia emergencies using conventional number-based and avatar-based patient monitoring: A prospective, eye-tracking study. JMIR Serious Games 2022, 10, e35642. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viautour, J.; Naegeli, L.; Braun, J.; Bergauer, L.; Roche, T.R.; Tscholl, D.W.; Akbas, S. The Visual Patient Avatar ICU Facilitates Information Transfer of Written Information by Visualization: A Multicenter Comparative Eye-Tracking Study. Diagnostics 2023, 13, 3432. https://doi.org/10.3390/diagnostics13223432
Viautour J, Naegeli L, Braun J, Bergauer L, Roche TR, Tscholl DW, Akbas S. The Visual Patient Avatar ICU Facilitates Information Transfer of Written Information by Visualization: A Multicenter Comparative Eye-Tracking Study. Diagnostics. 2023; 13(22):3432. https://doi.org/10.3390/diagnostics13223432
Chicago/Turabian StyleViautour, Julie, Lukas Naegeli, Julia Braun, Lisa Bergauer, Tadzio R. Roche, David W. Tscholl, and Samira Akbas. 2023. "The Visual Patient Avatar ICU Facilitates Information Transfer of Written Information by Visualization: A Multicenter Comparative Eye-Tracking Study" Diagnostics 13, no. 22: 3432. https://doi.org/10.3390/diagnostics13223432
APA StyleViautour, J., Naegeli, L., Braun, J., Bergauer, L., Roche, T. R., Tscholl, D. W., & Akbas, S. (2023). The Visual Patient Avatar ICU Facilitates Information Transfer of Written Information by Visualization: A Multicenter Comparative Eye-Tracking Study. Diagnostics, 13(22), 3432. https://doi.org/10.3390/diagnostics13223432