
Measurement of Retrobulbar Blood Flow and Vascular Reactivity—Relevance for Ocular and Cardiovascular Diseases



Abstract
:1. Introduction
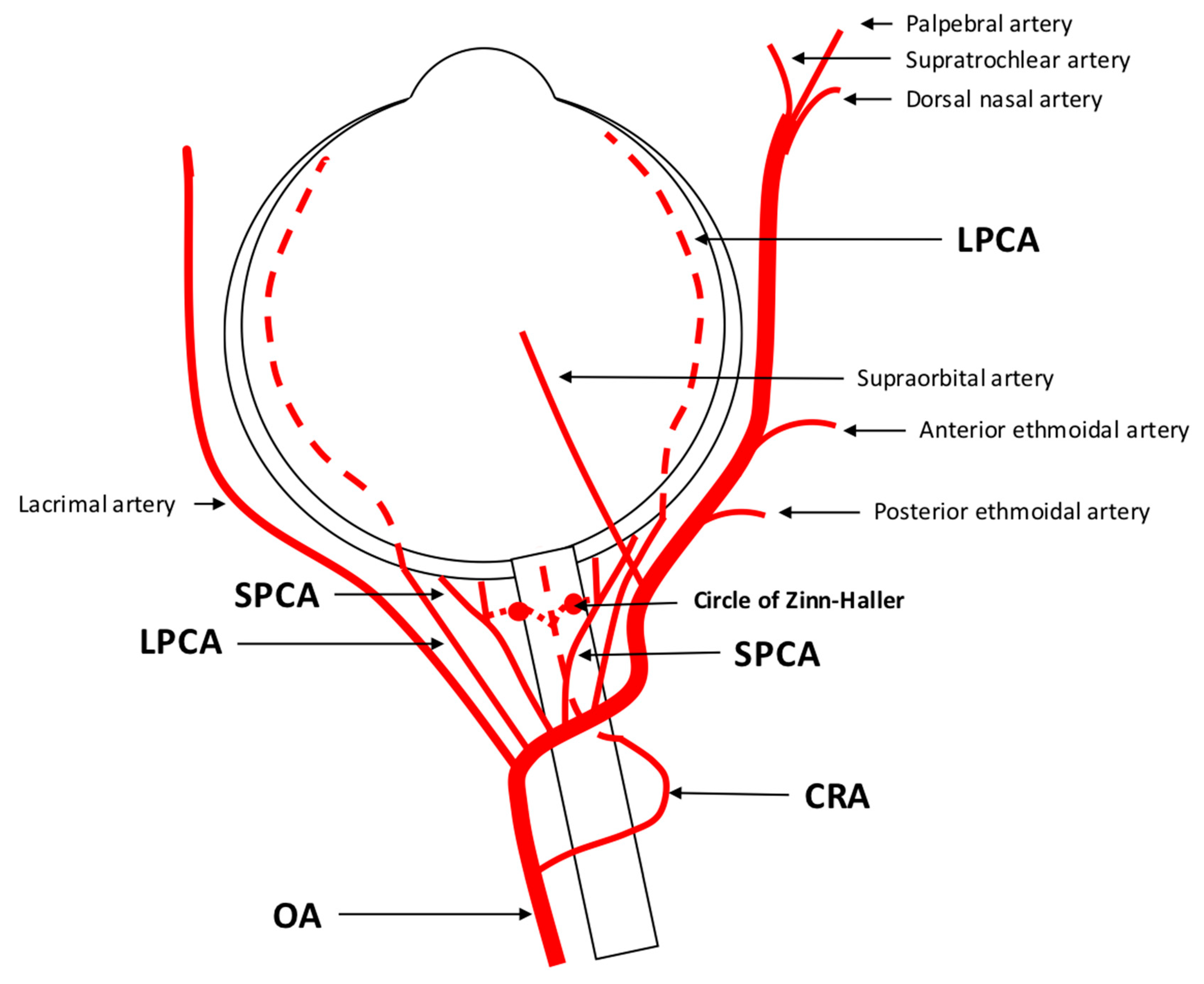
1.1. Anatomy and Regulation of the Retrobulbar Vasculature
1.2. Regulation of Retrobulbar Blood Flow
2. Assessment of Retrobulbar Blood Flow
2.1. Color Doppler Imaging
2.1.1. Technical Aspects
2.1.2. CDI under Physiological Conditions
2.1.3. Clinical and Scientific Relevance of CDI for Ocular and Cardiovascular Diseases
2.2. Computed Tomography Angiography
2.2.1. Technical Aspects
2.2.2. Clinical and Scientific Relevance of CTA for Ocular and Cardiovascular Diseases
2.3. Magnetic Resonance Imaging
2.3.1. Technical Aspects
2.3.2. Clinical and Scientific Relevance of MRI for Ocular and Cardiovascular Diseases
2.4. Evaluation of Retrobulbar Vessels Using Myography
2.4.1. Technical Aspects
2.4.2. Advantages and Limitations of Myography
2.5. Clinical and Scientific Relevance of Measuring Retrobulbar Blood Flow/Vascular Reactivity and Future Directions
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galassi, F.; Sodi, A.; Ucci, F.; Renieri, G.; Pieri, B.; Baccini, M. Ocular hemodynamics and glaucoma prognosis: A color Doppler imaging study. Arch. Ophthalmol. 2003, 121, 1711–1715. [Google Scholar] [CrossRef]
- Martinez, A.; Sanchez, M. Predictive value of colour Doppler imaging in a prospective study of visual field progression in primary open-angle glaucoma. Acta Ophthalmol. Scand. 2005, 83, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Garhofer, G.; Fuchsjager-Mayrl, G.; Vass, C.; Pemp, B.; Hommer, A.; Schmetterer, L. Retrobulbar blood flow velocities in open angle glaucoma and their association with mean arterial blood pressure. Investig. Ophthalmol. Vis. Sci. 2010, 51, 6652–6657. [Google Scholar] [CrossRef] [PubMed]
- Kaup, M.; Plange, N.; Arend, K.O.; Remky, A. Retrobulbar haemodynamics in non-arteritic anterior ischaemic optic neuropathy. Br. J. Ophthalmol. 2006, 90, 1350–1353. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Cui, M.; Yao, F.; Liao, R.; Liu, L. Retrobulbar and common carotid artery haemodynamics and carotid wall thickness in patients with non-arteritic anterior ischaemic optic neuropathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 1141–1146. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, G.; Tamaki, Y.; Kato, S. Retrobulbar circulation in patients with age-related maculopathy. Eye 2002, 16, 580–586. [Google Scholar] [CrossRef]
- Dimitrova, G.; Kato, S.; Yamashita, H.; Tamaki, Y.; Nagahara, M.; Fukushima, H.; Kitano, S. Relation between retrobulbar circulation and progression of diabetic retinopathy. Br. J. Ophthalmol. 2003, 87, 622–625. [Google Scholar] [CrossRef]
- Arai, T.; Numata, K.; Tanaka, K.; Kiba, T.; Kawasaki, S.; Saito, T.; Satoh, S.; Sekihara, H. Ocular arterial flow hemodynamics in patients with diabetes mellitus. J. Ultrasound Med. 1998, 17, 675–681. [Google Scholar] [CrossRef]
- Bohdanecka, Z.; Orgül, S.; Meyer, A.B.; Prünte, C.; Flammer, J. Relationship between blood flow velocities in retrobulbar vessels and laser Doppler flowmetry at the optic disk in glaucoma patients. Ophthalmologica 1999, 213, 145–149. [Google Scholar] [CrossRef]
- Yu, C.; Xu, C.; Wang, Z.; Zhang, X.; Huang, X. Color doppler ultrasound analysis of pathological myopia induced changes in retrobulbar blood flow and its relationship with characteristic changes in myopia. Pak. J. Med. Sci. 2023, 39, 853–857. [Google Scholar] [CrossRef]
- Sirkeci, O.; Erkus Sirkeci, E.; Ergün Süzer, N.; Tatlıparmak, A.C.; Küçükçiloğlu, Y.; Ulaş, T. Can orbital artery resistive indexes detect complications of diabetes in the prediabetic phase? Wien. Klin. Wochenschr. 2023, 135, 343–348. [Google Scholar] [CrossRef]
- Michalinos, A.; Zogana, S.; Kotsiomitis, E.; Mazarakis, A.; Troupis, T. Anatomy of the Ophthalmic Artery: A Review concerning Its Modern Surgical and Clinical Applications. Anat. Res. Int. 2015, 2015, 591961. [Google Scholar] [CrossRef] [PubMed]
- Reiner, A.; Fitzgerald, M.E.C.; Del Mar, N.; Li, C. Neural control of choroidal blood flow. Prog. Retin. Eye Res. 2018, 64, 96–130. [Google Scholar] [CrossRef]
- Varma, D.D.; Cugati, S.; Lee, A.W.; Chen, C.S. A review of central retinal artery occlusion: Clinical presentation and management. Eye 2013, 27, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Thakker, M.M.; Huang, J.; Possin, D.E.; Ahmadi, A.J.; Mudumbai, R.; Orcutt, J.C.; Tarbet, K.J.; Sires, B.S. Human orbital sympathetic nerve pathways. Ophthalmic Plast. Reconstr. Surg. 2008, 24, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Delaey, C.; Van De Voorde, J. Regulatory mechanisms in the retinal and choroidal circulation. Ophthalmic Res. 2000, 32, 249–256. [Google Scholar] [CrossRef]
- Chou, P.; Lu, D.W.; Chen, J.T. Bilateral superior cervical ganglionectomy increases choroidal blood flow in the rabbit. Ophthalmologica 2000, 214, 421–425. [Google Scholar] [CrossRef]
- Steinle, J.J.; Krizsan-Agbas, D.; Smith, P.G. Regional regulation of choroidal blood flow by autonomic innervation in the rat. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 279, R202–R209. [Google Scholar] [CrossRef]
- Kiel, J.W.; Shepherd, A.P. Autoregulation of choroidal blood flow in the rabbit. Investig. Ophthalmol. Vis. Sci. 1992, 33, 2399–2410. [Google Scholar]
- Zagvazdin, Y.; Fitzgerald, M.E.; Reiner, A. Role of muscarinic cholinergic transmission in Edinger-Westphal nucleus-induced choroidal vasodilation in pigeon. Exp. Eye Res. 2000, 70, 315–327. [Google Scholar] [CrossRef]
- Fitzgerald, M.E.; Tolley, E.; Jackson, B.; Zagvazdin, Y.S.; Cuthbertson, S.L.; Hodos, W.; Reiner, A. Anatomical and functional evidence for progressive age-related decline in parasympathetic control of choroidal blood flow in pigeons. Exp. Eye Res. 2005, 81, 478–491. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Shen, Y.M.; Jiang, M.N.; Lou, X.F.; Shen, Y. Ocular Blood Flow Autoregulation Mechanisms and Methods. J. Ophthalmol. 2015, 2015, 864871. [Google Scholar] [CrossRef] [PubMed]
- Schmidl, D.; Garhofer, G.; Schmetterer, L. The complex interaction between ocular perfusion pressure and ocular blood flow—Relevance for glaucoma. Exp. Eye Res. 2011, 93, 141–155. [Google Scholar] [CrossRef]
- Kolodjaschna, J.; Berisha, F.; Lung, S.; Schima, H.; Polska, E.; Schmetterer, L. Comparison of the autoregulatory mechanisms between middle cerebral artery and ophthalmic artery after thigh cuff deflation in healthy subjects. Investig. Ophthalmol. Vis. Sci. 2005, 46, 636–640. [Google Scholar] [CrossRef]
- Kaya, S.; Kolodjaschna, J.; Berisha, F.; Schmetterer, L.; Garhöfer, G. Comparison of the autoregulatory mechanisms between central retinal artery and posterior ciliary arteries after thigh cuff deflation in healthy subjects. Microvasc. Res. 2011, 82, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Kozobolis, V.P.; Detorakis, E.T.; Konstas, A.G.; Achtaropoulos, A.K.; Diamandides, E.D. Retrobulbar blood flow and ophthalmic perfusion in maximum dynamic exercise. Clin. Exp. Ophthalmol. 2008, 36, 123–129. [Google Scholar] [CrossRef]
- Stalmans, I.; Vandewalle, E.; Anderson, D.R.; Costa, V.P.; Frenkel, R.E.; Garhofer, G.; Grunwald, J.; Gugleta, K.; Harris, A.; Hudson, C.; et al. Use of colour Doppler imaging in ocular blood flow research. Acta Ophthalmol. 2011, 89, e609–e630. [Google Scholar] [CrossRef]
- Evans, D.H.; Jensen, J.A.; Nielsen, M.B. Ultrasonic colour Doppler imaging. Interface Focus 2011, 1, 490–502. [Google Scholar] [CrossRef]
- Modrzejewska, M. Guidelines for ultrasound examination in ophthalmology. Part III: Color Doppler ultrasonography. J. Ultrason. 2019, 19, 128–136. [Google Scholar] [CrossRef]
- Xu, S.; Huang, S.; Lin, Z.; Liu, W.; Zhong, Y. Color Doppler Imaging Analysis of Ocular Blood Flow Velocities in Normal Tension Glaucoma Patients: A Meta-Analysis. J. Ophthalmol. 2015, 2015, 919610. [Google Scholar] [CrossRef]
- Founti, P.; Harris, A.; Papadopoulou, D.; Emmanouilidis, P.; Siesky, B.; Kilintzis, V.; Anastasopoulos, E.; Salonikiou, A.; Pappas, T.; Topouzis, F. Agreement among three examiners of colour Doppler imaging retrobulbar blood flow velocity measurements. Acta Ophthalmol. 2011, 89, e631–e634. [Google Scholar] [CrossRef]
- Matthiessen, E.T.; Zeitz, O.; Richard, G.; Klemm, M. Reproducibility of blood flow velocity measurements using colour decoded Doppler imaging. Eye 2004, 18, 400–405. [Google Scholar] [CrossRef]
- Olver, J.M.; Spalton, D.J.; McCartney, A.C. Quantitative morphology of human retrolaminar optic nerve vasculature. Investig. Ophthalmol. Vis. Sci. 1994, 35, 3858–3866. [Google Scholar]
- Kozobolis, V.P.; Detorakis, E.T.; Georgiadis, G.S.; Achtaropoulos, A.A.; Papas, T.T.; Lazarides, M.K. Perimetric and retrobulbar blood flow changes following carotid endarterectomy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2007, 245, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Costa, V.P.; Kuzniec, S.; Molnar, L.J.; Cerri, G.G.; Puech-Leão, P.; Carvalho, C.A. Clinical findings and hemodynamic changes associated with severe occlusive carotid artery disease. Ophthalmology 1997, 104, 1994–2002. [Google Scholar] [CrossRef]
- Williamson, T.H.; Harris, A. Color Doppler ultrasound imaging of the eye and orbit. Surv. Ophthalmol. 1996, 40, 255–267. [Google Scholar] [CrossRef]
- Polska, E.; Kircher, K.; Ehrlich, P.; Vecsei, P.V.; Schmetterer, L. RI in central retinal artery as assessed by CDI does not correspond to retinal vascular resistance. Am. J. Physiol. Heart Circ. Physiol. 2001, 280, H1442–H1447. [Google Scholar] [CrossRef] [PubMed]
- Tublin, M.E.; Bude, R.O.; Platt, J.F. Review. The resistive index in renal Doppler sonography: Where do we stand? AJR Am. J. Roentgenol. 2003, 180, 885–892. [Google Scholar] [CrossRef]
- Böhm, E.W.; Pfeiffer, N.; Wagner, F.M.; Gericke, A. Methods to measure blood flow and vascular reactivity in the retina. Front. Med. 2022, 9, 1069449. [Google Scholar] [CrossRef]
- Orge, F.; Harris, A.; Kagemann, L.; Kopecky, K.; Sheets, C.W.; Rechtman, E.; Zalish, M. The first technique for non-invasive measurements of volumetric ophthalmic artery blood flow in humans. Br. J. Ophthalmol. 2002, 86, 1216–1219. [Google Scholar] [CrossRef] [PubMed]
- Katamay, R.; Fleischlin, C.; Gugleta, K.; Flammer, J.; Orgül, S. Volumetric blood flow measurement in the ophthalmic artery using colour Doppler. Klin. Monatsblatter Augenheilkd. 2009, 226, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Zeitz, O.; Vilchez, S.E.; Matthiessen, E.T.; Richard, G.; Klemm, M. Volumetric colour Doppler imaging: A useful tool for the determination of ocular blood flow in glaucoma patients? Eye 2006, 20, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Roff, E.J.; Harris, A.; Chung, H.S.; Hosking, S.L.; Morrison, A.M.; Halter, P.J.; Kagemann, L. Comprehensive assessment of retinal, choroidal and retrobulbar haemodynamics during blood gas perturbation. Graefe’s Arch. Clin. Exp. Ophthalmol. 1999, 237, 984–990. [Google Scholar] [CrossRef]
- Huber, K.K.; Adams, H.; Remky, A.; Arend, K.O. Retrobulbar haemodynamics and contrast sensitivity improvements after CO2 breathing. Acta Ophthalmol. Scand. 2006, 84, 481–487. [Google Scholar] [CrossRef]
- Hosking, S.L.; Harris, A.; Chung, H.S.; Jonescu-Cuypers, C.P.; Kagemann, L.; Roff Hilton, E.J.; Garzozi, H. Ocular haemodynamic responses to induced hypercapnia and hyperoxia in glaucoma. Br. J. Ophthalmol. 2004, 88, 406–411. [Google Scholar] [CrossRef]
- Schüttauf, F.; Cobet, U.; Klemenz, A.; Krause, A. Duplex ultrasound examinations of retinal circulation after inhalation of various mixed respiratory gases. Ophthalmologe 1998, 95, 225–228. [Google Scholar] [CrossRef]
- Evans, D.W.; Harris, A.; Danis, R.P.; Arend, O.; Martin, B.J. Altered retrobulbar vascular reactivity in early diabetic retinopathy. Br J Ophthalmol 1997, 81, 279–282. [Google Scholar] [CrossRef]
- Schmetterer, L.; Dallinger, S.; Findl, O.; Strenn, K.; Graselli, U.; Eichler, H.G.; Wolzt, M. Noninvasive investigations of the normal ocular circulation in humans. Investig. Ophthalmol. Vis. Sci. 1998, 39, 1210–1220. [Google Scholar]
- Yang, Q.; Shen, J.; Guo, W.; Wen, J.; Wang, Z.; Yu, D. Effect of acute intraocular pressure elevation on blood flow velocity and resistance in the rabbit ophthalmic artery. Vet. Ophthalmol. 2011, 14, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Galambos, P.; Vafiadis, J.; Vilchez, S.E.; Wagenfeld, L.; Matthiessen, E.T.; Richard, G.; Klemm, M.; Zeitz, O. Compromised autoregulatory control of ocular hemodynamics in glaucoma patients after postural change. Ophthalmology 2006, 113, 1832–1836. [Google Scholar] [CrossRef]
- Zeitz, O.; Mayer, J.; Hufnagel, D.; Praga, R.; Wagenfeld, L.; Galambos, P.; Wiermann, A.; Rebel, C.; Richard, G.; Klemm, M. Neuronal activity influences hemodynamics in the paraoptic short posterior ciliary arteries: A comparison between healthy and glaucomatous subjects. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5846–5850. [Google Scholar] [CrossRef] [PubMed]
- Zegadło, A.; Wierzbowska, J. Colour Doppler imaging of retrobulbar circulation in different severity of glaucoma optic neuropathy. Med. Ultrason. 2021, 23, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Meng, N.; Zhang, P.; Huang, H.; Ma, J.; Zhang, Y.; Li, H.; Qu, Y. Color Doppler imaging analysis of retrobulbar blood flow velocities in primary open-angle glaucomatous eyes: A meta-analysis. PLoS ONE 2013, 8, e62723. [Google Scholar] [CrossRef]
- Siesky, B.; Harris, A.; Racette, L.; Abassi, R.; Chandrasekhar, K.; Tobe, L.A.; Behzadi, J.; Eckert, G.; Amireskandari, A.; Muchnik, M. Differences in ocular blood flow in glaucoma between patients of African and European descent. J. Glaucoma 2015, 24, 117–121. [Google Scholar] [CrossRef]
- Barbosa-Breda, J.; Van Keer, K.; Abegão-Pinto, L.; Nassiri, V.; Molenberghs, G.; Willekens, K.; Vandewalle, E.; Rocha-Sousa, A.; Stalmans, I. Improved discrimination between normal-tension and primary open-angle glaucoma with advanced vascular examinations—The Leuven Eye Study. Acta Ophthalmol. 2019, 97, e50–e56. [Google Scholar] [CrossRef] [PubMed]
- Kurysheva, N.I.; Parshunina, O.A.; Shatalova, E.O.; Kiseleva, T.N.; Lagutin, M.B.; Fomin, A.V. Value of Structural and Hemodynamic Parameters for the Early Detection of Primary Open-Angle Glaucoma. Curr. Eye Res. 2017, 42, 411–417. [Google Scholar] [CrossRef]
- Abegão Pinto, L.; Willekens, K.; Van Keer, K.; Shibesh, A.; Molenberghs, G.; Vandewalle, E.; Stalmans, I. Ocular blood flow in glaucoma—The Leuven Eye Study. Acta Ophthalmol. 2016, 94, 592–598. [Google Scholar] [CrossRef]
- Eniola, M.A.; Adeyomoye, A.A.O.; Musa, K.O.; Ishola, A.A.S.; Olatunji, O.O. Ophthalmic artery and central retinal artery doppler patterns in primary open angle glaucoma patients at the Lagos University Teaching Hospital, Nigeria. J. West Afr. Coll. Surg. 2018, 8, 1–21. [Google Scholar]
- Kalayci, M.; Tahtabasi, M. Assessment of Doppler flow parameters of the retrobulbar arteries and internal carotid artery in patients with glaucoma: The significance of ophthalmic artery peak ratio and the intima-media thickness of the internal carotid artery. Int. Ophthalmol. 2020, 40, 3337–3348. [Google Scholar] [CrossRef]
- Huber, K.; Plange, N.; Remky, A.; Arend, O. Comparison of colour Doppler imaging and retinal scanning laser fluorescein angiography in healthy volunteers and normal pressure glaucoma patients. Acta Ophthalmol. Scand. 2004, 82, 426–431. [Google Scholar] [CrossRef]
- Plange, N.; Remky, A.; Arend, O. Colour Doppler imaging and fluorescein filling defects of the optic disc in normal tension glaucoma. Br. J. Ophthalmol. 2003, 87, 731–736. [Google Scholar] [CrossRef]
- Mokbel, T.H.; Shahin, M.M.; El-Said, E.M.; Abd El-Ghaffar, W.M. Potential diagnostic value of fluorescein angiography and color Doppler imaging in primary open angle glaucoma. Eur. J. Ophthalmol. 2009, 19, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Banou, L.; Dastiridou, A.; Giannoukas, A.; Kouvelos, G.; Baros, C.; Androudi, S. The Role of Color Doppler Imaging in the Diagnosis of Glaucoma: A Review of the Literature. Diagnostics 2023, 13, 588. [Google Scholar] [CrossRef]
- Dogan, N.C.; Ozdemir, N.; Aikimbaev, K.; Ciloglu, E. Retrobulbar Short Posterior Ciliary Artery Hemodynamics in Patients with Pseudoexfoliation Glaucoma and Primary Open-Angle Glaucoma. J. Curr. Ophthalmol. 2022, 34, 25–29. [Google Scholar] [CrossRef]
- Montanari, P.; Marangoni, P.; Oldani, A.; Ratiglia, R.; Raiteri, M.; Berardinelli, L. Color Doppler imaging study in patients with primary open-angle glaucoma treated with timolol 0.5% and carteolol 2%. Eur. J. Ophthalmol. 2001, 11, 240–244. [Google Scholar] [CrossRef]
- Altan-Yaycioglu, R.; Türker, G.; Akdöl, S.; Acunaş, G.; Izgi, B. The effects of beta-blockers on ocular blood flow in patients with primary open angle glaucoma: A color Doppler imaging study. Eur. J. Ophthalmol. 2001, 11, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Nivean, P.D.; Ariga, M.; Chithra, M.R.; Gohil, P.; Das, S.; Jaideep, G. Efficacy of dorzolamide in improving ocular blood flow in patients with open-angle glaucoma: The Indian carbonic anhydrase inhibitor trial. Indian J. Ophthalmol. 2022, 70, 4164–4167. [Google Scholar] [CrossRef]
- Inan, U.U.; Ermis, S.S.; Yücel, A.; Oztürk, F. The effects of latanoprost and brimonidine on blood flow velocity of the retrobulbar vessels: A 3-month clinical trial. Acta Ophthalmol. Scand. 2003, 81, 155–160. [Google Scholar] [CrossRef]
- Hommer, A.; Sperl, P.; Resch, H.; Popa-Cherecheanu, A.; Qiao, C.; Schmetterer, L.; Garhöfer, G. A double-masked randomized crossover study comparing the effect of latanoprost/timolol and brimonidine/timolol fixed combination on intraocular pressure and ocular blood flow in patients with primary open-angle glaucoma or ocular hypertension. J. Ocul. Pharmacol. Ther. 2012, 28, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Koz, O.G.; Ozsoy, A.; Yarangumeli, A.; Kose, S.K.; Kural, G. Comparison of the effects of travoprost, latanoprost and bimatoprost on ocular circulation: A 6-month clinical trial. Acta Ophthalmol. Scand. 2007, 85, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Abegão Pinto, L.; Vandewalle, E.; Marques-Neves, C.; Stalmans, I. Visual field loss in optic disc drusen patients correlates with central retinal artery blood velocity patterns. Acta Ophthalmol. 2014, 92, e286–e291. [Google Scholar] [CrossRef] [PubMed]
- Arséne, S.; Giraudeau, B.; Le Lez, M.L.; Pisella, P.J.; Pourcelot, L.; Tranquart, F. Follow up by colour Doppler imaging of 102 patients with retinal vein occlusion over 1 year. Br. J. Ophthalmol. 2002, 86, 1243–1247. [Google Scholar] [CrossRef] [PubMed]
- Ozbek, Z.; Saatci, A.O.; Durak, I.; Kaynak, S.; Ergin, M.H.; Oner, B.; Cingil, G. Colour Doppler assessment of blood flow in eyes with central retinal vein occlusion. Ophthalmologica 2002, 216, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Arsene, S.; Vierron, E.; Le Lez, M.L.; Herault, B.; Gruel, Y.; Pisella, P.J.; Giraudeau, B.; Tranquart, F. Conversion from nonischemic to ischemic retinal vein occlusion: Prediction by venous velocity on color Doppler imaging. Eur. J. Ophthalmol. 2009, 19, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Li, H.; Wang, Y. Implication of Retrobulbar and internal carotid artery blood-flow-volume alterations for the pathogenesis of non-arteritic anterior ischemic optic neuropathy. BMC Ophthalmol. 2021, 21, 309. [Google Scholar] [CrossRef]
- Sanjari, M.S.; Falavarjani, K.G.; Mehrabani, M.; Ghiasian, L.; Zamani, B. Retrobulbar haemodynamics and carotid wall thickness in patients with non-arteritic anterior ischaemic optic neuropathy. Br. J. Ophthalmol. 2009, 93, 638–640. [Google Scholar] [CrossRef]
- Hamidi, C.; Türkcü, F.M.; Göya, C.; Çetinçakmak, M.G.; Yüksel, H.; Teke, M.; Hattapoğlu, S.; Bilici, A. Evaluation of retrobulbar blood flow with color doppler ultrasonography in patients with central serous chorioretinopathy. J. Clin. Ultrasound 2014, 42, 481–485. [Google Scholar] [CrossRef]
- Chen, G.F.; Ma, J.X.; Zhang, T.D.; Wang, C.L.; Li, S.F.; Yang, A.Q. The analysis of fundus fluorescein angiography, indocyanine green angiography and hemodynamics of retrobulbar blood vessels in central serous chorioretinopathy. Zhonghua Yan Ke Za Zhi 2009, 45, 243–247. [Google Scholar]
- Erdem Toslak, I.; Erol, M.K.; Toslak, D.; Cekic, B.; Barc Ergun, M.; Lim-Dunham, J.E. Is the unaffected eye really unaffected? Color Doppler ultrasound findings in unilaterally active central serous chorioretinopathy. J. Med. Ultrason. 2017, 44, 173–181. [Google Scholar] [CrossRef]
- Meng, N.; Liu, J.; Zhang, Y.; Ma, J.; Li, H.; Qu, Y. Color Doppler Imaging Analysis of Retrobulbar Blood Flow Velocities in Diabetic Patients without or with Retinopathy: A Meta-analysis. J. Ultrasound Med. 2014, 33, 1381–1389. [Google Scholar] [CrossRef]
- Kraśnicki, P.; Mariak, Z.; Ustymowicz, A.; Proniewska-Skretek, E. Assessment of blood flow in the ocular circulation in type 2 diabetes patients with Color Doppler imaging. Klin. Ocz. 2006, 108, 294–298. [Google Scholar]
- Gracner, T. Ocular blood flow velocity determined by color Doppler imaging in diabetic retinopathy. Ophthalmologica 2004, 218, 237–242. [Google Scholar] [CrossRef]
- Madhpuriya, G.; Gokhale, S.; Agrawal, A.; Nigam, P.; Wan, Y.L. Evaluation of Hemodynamic Changes in Retrobulbar Blood Vessels Using Color Doppler Imaging in Diabetic Patients. Life 2022, 12, 629. [Google Scholar] [CrossRef]
- Divya, K.; Kanagaraju, V.; Devanand, B.; Jeevamala, C.; Raghuram, A.; Sundar, D. Evaluation of retrobulbar circulation in type 2 diabetic patients using color Doppler imaging. Indian J. Ophthalmol. 2020, 68, 1108–1114. [Google Scholar] [CrossRef]
- Khatri, M.; Saxena, S.; Kumar, M.; Chabbra, A.K.; Bhasker, S.K.; Akduman, E.I.; Pham, H.; Akduman, L. Resistive index of central retinal artery is a bioimaging biomarker for severity of diabetic retinopathy. Int. J. Retin. Vitr. 2019, 5, 38. [Google Scholar] [CrossRef]
- Ashraf, H.; Lotfi, M.; Akbari, M.; Jahanbani-Ardakani, H.; Ghaffari, M.; Khalili, M.R. Effect of calcium dobesilate on retrobulbar blood flow and choroidal thickness in patients with non-proliferative diabetic retinopathy. Int. Ophthalmol. 2021, 41, 3479–3486. [Google Scholar] [CrossRef]
- Dimitrova, G.; Tomita, G.; Kato, S. Correlation between capillary blood flow of retina estimated by SLDF and circulatory parameters of retrobulbar blood vessels estimated by CDI in diabetic patients. Graefe’s Arch. Clin. Exp. Ophthalmol. 2005, 243, 653–658. [Google Scholar] [CrossRef]
- Silverman, R.H.; Urs, R.; Jokl, D.H.; Pinto, L.; Coki, O.; Sahni, R.; Horowitz, J.D.; Brooks, S.E. Ocular Blood Flow in Preterm Neonates: A Preliminary Report. Transl. Vis. Sci. Technol. 2021, 10, 22. [Google Scholar] [CrossRef]
- Hartenstein, S.; Müller, B.; Metze, B.; Czernik, C.; Bührer, C. Blood flow assessed by color Doppler imaging in retinopathy of prematurity. J. Perinatol. 2015, 35, 745–747. [Google Scholar] [CrossRef]
- Niwald, A.; Grałek, M. Evaluation of blood flow in the ophthalmic artery and central retinal artery in children with retinopathy of prematurity. Klin. Ocz. 2006, 108, 32–35. [Google Scholar]
- Zhao, M.; Lam, A.K.; Ying, M.T.; Cheong, A.M. Hemodynamic and morphological changes of the central retinal artery in myopic eyes. Sci. Rep. 2022, 12, 7104. [Google Scholar] [CrossRef]
- Benavente-Pérez, A.; Hosking, S.L.; Logan, N.S.; Broadway, D.C. Ocular blood flow measurements in healthy human myopic eyes. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 248, 1587–1594. [Google Scholar] [CrossRef]
- Dimitrova, G.; Tamaki, Y.; Kato, S.; Nagahara, M. Retrobulbar circulation in myopic patients with or without myopic choroidal neovascularisation. Br. J. Ophthalmol. 2002, 86, 771–773. [Google Scholar] [CrossRef]
- Liu, F.; Niu, L.; Guo, J.; Jian, W.; Shang, J.; Zhao, J.; Xue, K.; Zhou, X. Quantitative evaluation of retinal and choroidal vascularity and retrobulbar blood flow in patients with myopic anisometropia by CDI and OCTA. Br. J. Ophthalmol. 2023, 107, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Grudzińska, E.M.; Zaborski, D.; Modrzejewska, M. Correlation between retrobulbar blood flow parameters and retinal nerve fiber, ganglion cell and inner plexus layer thickness in myopia. Eur. J. Ophthalmol. 2022, 32, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Grudzińska, E.; Modrzejewska, M. Modern Diagnostic Techniques for the Assessment of Ocular Blood Flow in Myopia: Current State of Knowledge. J. Ophthalmol. 2018, 2018, 4694789. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Shah, S.; Sundar, G.; Arora, R.; Gupta, S.; Khullar, T. Orbital and ocular perfusion in thyroid eye disease. Surv. Ophthalmol. 2023, 68, 481–506. [Google Scholar] [CrossRef]
- Jamshidian-Tehrani, M.; Nabavi, A.; Kasaee, A.; Hasanpoor, N.; Elhami, E.; Sharif-Kashani, S.; Masoumi, A.; Nowroozzadeh, M.H.; Sadeghi-Tari, A. Color Doppler imaging in thyroid eye disease and its correlation to disease activity. Orbit 2019, 38, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Yanik, B.; Conkbayir, I.; Acaroglu, G.; Hekimoglu, B. Graves’ ophthalmopathy: Comparison of the Doppler sonography parameters with the clinical activity score. J. Clin. Ultrasound 2005, 33, 375–380. [Google Scholar] [CrossRef]
- Pérez-López, M.; Sales-Sanz, M.; Rebolleda, G.; Casas-Llera, P.; González-Gordaliza, C.; Jarrín, E.; Muñoz-Negrete, F.J. Retrobulbar ocular blood flow changes after orbital decompression in Graves’ ophthalmopathy measured by color Doppler imaging. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5612–5617. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Freitas, D.B.; Meira-Freitas, D.; Melo, L.A., Jr.; Paranhos, A., Jr.; Iared, W.; Ajzen, S. Color Doppler imaging of the ophthalmic artery in patients with chronic heart failure. Arq. Bras. Oftalmol. 2011, 74, 326–329. [Google Scholar] [CrossRef]
- Nicolaides, K.H.; Sarno, M.; Wright, A. Ophthalmic artery Doppler in the prediction of preeclampsia. Am. J. Obstet. Gynecol. 2022, 226, S1098–S1101. [Google Scholar] [CrossRef]
- Diniz, A.L.D.; Menêses, V.; Freitas, M.A.R.; Paes, M.; Naves, W.U.; Sass, N. Performance of ophthalmic artery Doppler velocimetry in the complementary diagnosis of preeclampsia. J. Matern.-Fetal Neonatal Med. 2022, 35, 9078–9085. [Google Scholar] [CrossRef] [PubMed]
- Matias, D.S.; Costa, R.F.; Matias, B.S.; Gordiano, L.; Correia, L.C. Predictive value of ophthalmic artery Doppler velocimetry in relation to development of pre-eclampsia. Ultrasound Obstet. Gynecol. 2014, 44, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.H.; Sheng, W.Y.; Yen, M.Y.; Lai, S.T.; Teng, M.M. Color Doppler imaging of orbital arteries for detection of carotid occlusive disease. Stroke 1993, 24, 1196–1203. [Google Scholar] [CrossRef]
- Reynolds, P.S.; Greenberg, J.P.; Lien, L.M.; Meads, D.C.; Myers, L.G.; Tegeler, C.H. Ophthalmic artery flow direction on color flow duplex imaging is highly specific for severe carotid stenosis. J. Neuroimaging 2002, 12, 5–8. [Google Scholar] [CrossRef]
- Emiroglu, M.Y.; Evlice, M.; Akcakoyun, M.; Velioglu, M.; Agca, M.; Topal, Y.K.; Kargin, R.; Caliskan, M. Effects of Obstructive Carotid Artery Disease on Ocular Circulation and the Safety of Carotid Artery Stenting. Heart Lung Circ. 2017, 26, 1069–1078. [Google Scholar] [CrossRef]
- Altinbas, N.K.; Ustuner, E.; Ozcan, H.; Bilgic, S.; Sancak, T.; Dusunceli, E. Effect of carotid artery stenting on ophthalmic artery flow patterns. J. Ultrasound Med. 2014, 33, 629–638. [Google Scholar] [CrossRef]
- Kawaguchi, S.; Sakaki, T.; Iwahashi, H.; Fujimoto, K.; Iida, J.; Mishima, H.; Nishikawa, N. Effect of carotid artery stenting on ocular circulation and chronic ocular ischemic syndrome. Cerebrovasc. Dis. 2006, 22, 402–408. [Google Scholar] [CrossRef]
- Ma, F.; Su, J.; Shang, Q.; Ma, J.; Zhang, T.; Wang, X.; Ma, H.; Yu, J. Changes in Ocular Hemodynamics after Carotid Artery Angioplasty and Stenting (CAAS) in Patients with Different Severity of Ocular Ischemic Syndrome. Curr. Eye Res. 2018, 43, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Celik, G.; Gunay, M.; Ozcabi, B.; Gulturk, U.; Kizilay, O.; Vural, A.; Ozkul Saglam, N.; Papatya Cakir, E.D.; Palabiyik, F.; Onal Gunay, B.; et al. Evaluation of the impact of childhood obesity on retrobulbar hemodynamics and retinal microvasculature. Eur. J. Ophthalmol. 2022, 32, 3556–3563. [Google Scholar] [CrossRef]
- Tufek, M.; Nalcacioglu, P.; Capraz, M.; Varol, K.; Kaya, A.T.; Aydın, N.; Kara, C. The impact of obesity on ocular hemodynamics and choroidal thickness. Ther. Adv. Ophthalmol. 2023, 15, 25158414231180985. [Google Scholar] [CrossRef]
- Xue, K.; Guo, T.; Lei, B.; Chen, S.; Huang, L.; Zhou, M. Retrobulbar blood flow velocity in systemic lupus erythematosus assessed by color Doppler imaging. Lupus 2022, 31, 582–587. [Google Scholar] [CrossRef]
- Erdogmus, B.; Yazici, S.; Yazici, B.; Ataoglu, S.; Buyukkaya, R.; Yuksel, H.; Cura, S. Orbital blood flow velocities in patients with rheumatoid arthritis. J. Clin. Ultrasound 2007, 35, 367–371. [Google Scholar] [CrossRef]
- Unal, O.; Can, M.E.; Ozcan, A.; Ozcan, M.E.; Erten, S.; Cagil, N. Color Doppler imaging of ocular hemodynamic changes in patients with rheumatoid arthritis unrelated to disease activity. Rheumatol. Int. 2019, 39, 1001–1006. [Google Scholar] [CrossRef]
- Caça, I.; Nazaroğlu, H.; Unlü, K.; Cakmak, S.S.; Ari, S.; Sakalar, Y.B. Color doppler imaging of ocular hemodynamic changes in Behçet’s disease. Jpn. J. Ophthalmol. 2004, 48, 101–105. [Google Scholar] [CrossRef]
- Celebi, S.; Akfirat, M.; Celebi, H.; Alagöz, G. Color Doppler ultrasonography in ocular Behçet’s disease. Acta Ophthalmol. Scand. 2000, 78, 30–33. [Google Scholar] [CrossRef]
- Isik, C.; Yagci, B.; Yildirim, C.; Yaylali, V.; Tatlipinar, S.; Ozden, S. Orbital color Doppler imaging in Behçet’s disease with or without ocular involvement. Int. Ophthalmol. 2007, 27, 37–42. [Google Scholar] [CrossRef]
- Matos, K.T.; Arantes, T.; Souza, A.W.; Ramos, M.H.; Allemann, N.; Muccioli, C. Retinal angiography and colour Doppler of retrobulbar vessels in Takayasu arteritis. Can. J. Ophthalmol. 2014, 49, 80–86. [Google Scholar] [CrossRef]
- Tufek, M.; Capraz, M.; Kaya, A.T.; Aydin, N.; Nalcacioglu, P. Retrobulbar ocular blood flow and choroidal vascular changes in patients recovering from COVID-19 infection. Photodiagnosis Photodyn. Ther. 2022, 39, 102976. [Google Scholar] [CrossRef]
- Zhang, Y.; Stewart, J.M. Retinal and choroidal manifestations of COVID-19. Curr. Opin. Ophthalmol. 2021, 32, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Yorgun, M.A.; Saritas, O.; Ozkan, E.; Tascı Yildiz, Y.; Unal, O.; Toklu, Y. Early effects of inactivated (CoronaVac) SARS-CoV-2 vaccine on retrobulbar vascular blood flow and retinal vascular density. Photodiagnosis Photodyn. Ther. 2023, 42, 103584. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.K.; Huang, Y.H. Ocular Manifestations after Receiving COVID-19 Vaccine: A Systematic Review. Vaccines 2021, 9, 1404. [Google Scholar] [CrossRef]
- Li, T.T.; Shao, G.B.; Jiang, Y.L.; Wang, J.X.; Zhou, X.R.; Ren, M.; Li, L.Q. Ocular surface heat effects on ocular hemodynamics detected by real-time measuring device. Int. J. Ophthalmol. 2018, 11, 1902–1908. [Google Scholar] [CrossRef] [PubMed]
- Li, H.Y.; Leng, Y.; Zhang, T.S.; Hu, Y.; Li, W. A study of hemodynamic changes in the arteries of rabbit’s eye caused by acute high intraocular pressure. Zhonghua Yan Ke Za Zhi 2005, 41, 449–453. [Google Scholar]
- Costa, A.P.; Lima, A.M.; da Silva, L.H.; de Oliveira Alves Carvalho, R.; do Amaral, A.V.; Borges, N.C. Ocular perfusion pressure and color Doppler imaging of the external ophthalmic artery of rabbits treated with sildenafil citrate. BMC Vet. Res. 2016, 12, 149. [Google Scholar] [CrossRef]
- Liu, J.H.; Li, R.; Nelson, T.R.; Weinreb, R.N. Resistance to blood flow in the rabbit ophthalmic artery after topical treatment with timolol. J. Ocul. Pharmacol. Ther. 2007, 23, 103–109. [Google Scholar] [CrossRef]
- Andre, F.; Fortner, P.; Emami, M.; Seitz, S.; Brado, M.; Gückel, F.; Sokiranski, R.; Sommer, A.; Frey, N.; Görich, J.; et al. Factors influencing the safety of outpatient coronary CT angiography: A clinical registry study. BMJ Open 2022, 12, e058304. [Google Scholar] [CrossRef]
- Nyheim, T.; Staxrud, L.E.; Jørgensen, J.J.; Jensen, K.; Olerud, H.M.; Sandbæk, G. Radiation exposure in patients treated with endovascular aneurysm repair: What is the risk of cancer, and can we justify treating younger patients? Acta Radiol. 2017, 58, 323–330. [Google Scholar] [CrossRef]
- Baz, R.A.; Scheau, C.; Niscoveanu, C.; Bordei, P. Morphometry of the Entire Internal Carotid Artery on CT Angiography. Medicina 2021, 57, 832. [Google Scholar] [CrossRef]
- Baz, R.A.; Jurja, S.; Ciuluvica, R.; Scheau, C.; Baz, R. Morphometric study regarding ophthalmic and internal carotid arteries utilizing computed tomography angiography. Exp. Ther. Med. 2022, 23, 112. [Google Scholar] [CrossRef]
- Perrini, P.; Cardia, A.; Fraser, K.; Lanzino, G. A microsurgical study of the anatomy and course of the ophthalmic artery and its possibly dangerous anastomoses. J. Neurosurg. 2007, 106, 142–150. [Google Scholar] [CrossRef]
- Erdogmus, S.; Govsa, F. Anatomic features of the intracranial and intracanalicular portions of ophthalmic artery: For the surgical procedures. Neurosurg. Rev. 2006, 29, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Fan, S.; He, W.; Zhang, T.; Wang, Y. Ophthalmic artery visualization and morphometry by computed tomography angiography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 627–631. [Google Scholar] [CrossRef] [PubMed]
- Rossin, E.J.; Gilbert, A.L.; Koen, N.; Leslie-Mazwi, T.M.; Cunnane, M.E.; Rizzo, J.F., 3rd. Site of Origin of the Ophthalmic Artery Influences the Risk for Retinal Versus Cerebral Embolic Events. J. Neuro-Ophthalmol. 2021, 41, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.T.; Wang, J.L.; Wang, Y.L. Ophthalmic artery changes in type 2 diabetes with and without acute coronary syndrome. J. Transl. Med. 2022, 20, 512. [Google Scholar] [CrossRef]
- Wu, L.T.; Wang, J.L.; Wang, Y.L. Ophthalmic Artery Morphological and Hemodynamic Features in Acute Coronary Syndrome. Investig. Ophthalmol. Vis. Sci. 2021, 62, 7. [Google Scholar] [CrossRef] [PubMed]
- Sawall, S.; Beckendorf, J.; Amato, C.; Maier, J.; Backs, J.; Vande Velde, G.; Kachelrieß, M.; Kuntz, J. Coronary micro-computed tomography angiography in mice. Sci. Rep. 2020, 10, 16866. [Google Scholar] [CrossRef]
- Wang, H.; Zheng, L.F.; Feng, Y.; Xie, X.Q.; Zhao, J.L.; Wang, X.F.; Zhang, G.X. A comparison of 3D-CTA and 4D-CE-MRA for the dynamic monitoring of angiogenesis in a rabbit VX2 tumor. Eur. J. Radiol. 2012, 81, 104–110. [Google Scholar] [CrossRef]
- Currie, G.M.; Kamvosoulis, P.; Bushong, S. PET/MRI, Part 2: Technologic Principles. J. Nucl. Med. Technol. 2021, 49, 217–225. [Google Scholar] [CrossRef]
- Skinner, S. MRI brain imaging. Aust. Fam. Physician 2013, 42, 794–797. [Google Scholar]
- Hom, J.J.; Ordovas, K.; Reddy, G.P. Velocity-encoded cine MR imaging in aortic coarctation: Functional assessment of hemodynamic events. Radiographics 2008, 28, 407–416. [Google Scholar] [CrossRef]
- Maier, I.L.; Hofer, S.; Joseph, A.A.; Merboldt, K.D.; Tan, Z.; Schregel, K.; Knauth, M.; Bähr, M.; Psychogios, M.N.; Liman, J.; et al. Carotid artery flow as determined by real-time phase-contrast flow MRI and neurovascular ultrasound: A comparative study of healthy subjects. Eur. J. Radiol. 2018, 106, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Stamm, A.C.; Wright, C.L.; Knopp, M.V.; Schmalbrock, P.; Heverhagen, J.T. Phase contrast and time-of-flight magnetic resonance angiography of the intracerebral arteries at 1.5, 3 and 7 T. Magn. Reson. Imaging 2013, 31, 545–549. [Google Scholar] [CrossRef]
- Marks, M.P.; Pelc, N.J.; Ross, M.R.; Enzmann, D.R. Determination of cerebral blood flow with a phase-contrast cine MR imaging technique: Evaluation of normal subjects and patients with arteriovenous malformations. Radiology 1992, 182, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, M.; Lindén, C.; Qvarlander, S.; Wåhlin, A.; Ambarki, K.; Hallberg, P.; Eklund, A.; Jóhannesson, G. Feasibility of MRI to assess differences in ophthalmic artery blood flow rate in normal tension glaucoma and healthy controls. Acta Ophthalmol. 2021, 99, e679–e685. [Google Scholar] [CrossRef]
- Tsutsumi, S.; Yasumoto, Y.; Tabuchi, T.; Ito, M. Visualization of the ophthalmic artery by phase-contrast magnetic resonance angiography: A pilot study. Surg. Radiol. Anat. 2012, 34, 833–838. [Google Scholar] [CrossRef]
- Tsutsumi, S.; Ono, H.; Ishii, H. Central retinal artery delineation using magnetic resonance imaging. Surg. Radiol. Anat. 2022, 44, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, S.; Nakamura, M.; Tabuchi, T.; Yasumoto, Y. The superior ophthalmic vein: Delineation with high-resolution magnetic resonance imaging. Surg. Radiol. Anat. 2015, 37, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Uchino, A.; Saito, N.; Takahashi, M.; Kozawa, E.; Mizukoshi, W.; Nakajima, R.; Okano, N. Persistent dorsal ophthalmic artery and ophthalmic artery arising from the middle meningeal artery diagnosed by MR angiography at 3 T. Surg. Radiol. Anat. 2013, 35, 775–782. [Google Scholar] [CrossRef]
- Hibert, M.L.; Chen, Y.I.; Ohringer, N.; Feuer, W.J.; Waheed, N.K.; Heier, J.S.; Calhoun, M.W.; Rosenfeld, P.J.; Polimeni, J.R. Altered Blood Flow in the Ophthalmic and Internal Carotid Arteries in Patients with Age-Related Macular Degeneration Measured Using Noncontrast MR Angiography at 7T. AJNR Am. J. Neuroradiol. 2021, 42, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Promelle, V.; Bouzerar, R.; Daouk, J.; Iscar, C.; Milazzo, S.; Balédent, O. Ophthalmic Artery and Superior Ophthalmic Vein Blood Flow Dynamics in Glaucoma Investigated by Phase Contrast Magnetic Resonance Imaging. J. Glaucoma 2021, 30, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Jóhannesson, G.; Qvarlander, S.; Wåhlin, A.; Ambarki, K.; Hallberg, P.; Eklund, A.; Lindén, C. Intraocular Pressure Decrease Does Not Affect Blood Flow Rate of Ophthalmic Artery in Ocular Hypertension. Investig. Ophthalmol. Vis. Sci. 2020, 61, 17. [Google Scholar] [CrossRef]
- Tsai, C.L.; Lee, J.T.; Cheng, C.A.; Liu, M.T.; Chen, C.Y.; Hu, H.H.; Peng, G.S. Reversal of ophthalmic artery flow as a predictor of intracranial hemodynamic compromise: Implication for prognosis of severe carotid stenosis. Eur. J. Neurol. 2013, 20, 564–570. [Google Scholar] [CrossRef]
- Sung, Y.F.; Tsai, C.L.; Lee, J.T.; Chu, C.M.; Hsu, C.H.; Lin, C.C.; Peng, G.S. Reversal of ophthalmic artery flow and stroke outcomes in Asian patients with acute ischemic stroke and unilateral severe cervical carotid stenosis. PLoS ONE 2013, 8, e80675. [Google Scholar] [CrossRef]
- Sekine, T.; Takagi, R.; Amano, Y.; Murai, Y.; Orita, E.; Fukushima, Y.; Matsumura, Y.; Kumita, S.I. 4D Flow MR Imaging of Ophthalmic Artery Flow in Patients with Internal Carotid Artery Stenosis. Magn. Reson. Med. Sci. 2018, 17, 13–20. [Google Scholar] [CrossRef]
- Wang, J.L.; Cheng, X.R.; Meng, Z.Y.; Wang, Y.L. Impact of total cerebral small vessel disease score on ophthalmic artery morphologies and hemodynamics. J. Transl. Med. 2023, 21, 65. [Google Scholar] [CrossRef]
- Fouquet, J.P.; Lebel, R.; Cahill, L.S.; Sled, J.G.; Tremblay, L.; Lepage, M. Cerebrovascular MRI in the mouse without an exogenous contrast agent. Magn. Reson. Med. 2020, 84, 405–415. [Google Scholar] [CrossRef]
- van Bochove, G.S.; Straathof, R.; Krams, R.; Nicolay, K.; Strijkers, G.J. MRI-determined carotid artery flow velocities and wall shear stress in a mouse model of vulnerable and stable atherosclerotic plaque. Magma 2010, 23, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Justić, H.; Barić, A.; Šimunić, I.; Radmilović, M.; Ister, R.; Škokić, S.; Dobrivojević Radmilović, M. Redefining the Koizumi model of mouse cerebral ischemia: A comparative longitudinal study of cerebral and retinal ischemia in the Koizumi and Longa middle cerebral artery occlusion models. J. Cereb. Blood Flow Metab. 2022, 42, 2080–2094. [Google Scholar] [CrossRef]
- Schmetterer, L.; Garhofer, G. How can blood flow be measured? Surv. Ophthalmol. 2007, 52 (Suppl. 2), S134–S138. [Google Scholar] [CrossRef]
- Haefliger, I.O.; Flammer, J.; Lüscher, T.F. Nitric oxide and endothelin-1 are important regulators of human ophthalmic artery. Investig. Ophthalmol. Vis. Sci. 1992, 33, 2340–2343. [Google Scholar]
- Zadeh, J.K.; Ruemmler, R.; Hartmann, E.K.; Ziebart, A.; Ludwig, M.; Patzak, A.; Xia, N.; Li, H.; Pfeiffer, N.; Gericke, A. Responses of retinal arterioles and ciliary arteries in pigs with acute respiratory distress syndrome (ARDS). Exp. Eye Res. 2019, 184, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Kringelholt, S.; Simonsen, U.; Bek, T. Dual effect of prostaglandins on isolated intraocular porcine ciliary arteries. Acta Ophthalmol. 2013, 91, 498–504. [Google Scholar] [CrossRef]
- Chuman, H.; Sugimoto, T.; Nao, I.N. Vasodilatory effect of L-arginine on isolated rabbit and human posterior ciliary arteries in vitro and increased optic disc blood flow in vivo. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 2381–2388. [Google Scholar] [CrossRef]
- Faraci, F.M.; Sigmund, C.D. Vascular biology in genetically altered mice: Smaller vessels, bigger insight. Circ. Res. 1999, 85, 1214–1225. [Google Scholar] [CrossRef]
- Gericke, A.; Goloborodko, E.; Pfeiffer, N.; Manicam, C. Preparation Steps for Measurement of Reactivity in Mouse Retinal Arterioles Ex Vivo. J. Vis. Exp. 2018, 135, e56199. [Google Scholar] [CrossRef]
- Gericke, A.; Kordasz, M.L.; Steege, A.; Sanbe, A.; Goloborodko, E.; Vetter, J.M.; Patzak, A.; Pfeiffer, N. Functional role of alpha1-adrenoceptor subtypes in murine ophthalmic arteries. Investig. Ophthalmol. Vis. Sci. 2011, 52, 4795–4799. [Google Scholar] [CrossRef] [PubMed]
- Böhmer, T.; Manicam, C.; Steege, A.; Michel, M.C.; Pfeiffer, N.; Gericke, A. The α₁B -adrenoceptor subtype mediates adrenergic vasoconstriction in mouse retinal arterioles with damaged endothelium. Br. J. Pharmacol. 2014, 171, 3858–3867. [Google Scholar] [CrossRef] [PubMed]
- Laspas, P.; Goloborodko, E.; Sniatecki, J.J.; Kordasz, M.L.; Manicam, C.; Wojnowski, L.; Li, H.; Patzak, A.; Pfeiffer, N.; Gericke, A. Role of nitric oxide synthase isoforms for ophthalmic artery reactivity in mice. Exp. Eye Res. 2014, 127, 1–8. [Google Scholar] [CrossRef]
- Manicam, C.; Staubitz, J.; Brochhausen, C.; Grus, F.H.; Pfeiffer, N.; Gericke, A. The Gatekeepers in the Mouse Ophthalmic Artery: Endothelium-Dependent Mechanisms of Cholinergic Vasodilation. Sci. Rep. 2016, 6, 20322. [Google Scholar] [CrossRef] [PubMed]
- Manicam, C.; Ginter, N.; Li, H.; Xia, N.; Goloborodko, E.; Zadeh, J.K.; Musayeva, A.; Pfeiffer, N.; Gericke, A. Compensatory Vasodilator Mechanisms in the Ophthalmic Artery of Endothelial Nitric Oxide Synthase Gene Knockout Mice. Sci. Rep. 2017, 7, 7111. [Google Scholar] [CrossRef]
- Gericke, A.; Goloborodko, E.; Sniatecki, J.J.; Steege, A.; Wojnowski, L.; Pfeiffer, N. Contribution of nitric oxide synthase isoforms to cholinergic vasodilation in murine retinal arterioles. Exp. Eye Res. 2013, 109, 60–66. [Google Scholar] [CrossRef]
- Gericke, A.; Wolff, I.; Musayeva, A.; Zadeh, J.K.; Manicam, C.; Pfeiffer, N.; Li, H.; Xia, N. Retinal arteriole reactivity in mice lacking the endothelial nitric oxide synthase (eNOS) gene. Exp. Eye Res. 2019, 181, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Gericke, A.; Mann, C.; Zadeh, J.K.; Musayeva, A.; Wolff, I.; Wang, M.; Pfeiffer, N.; Daiber, A.; Li, H.; Xia, N.; et al. Elevated Intraocular Pressure Causes Abnormal Reactivity of Mouse Retinal Arterioles. Oxidative Med. Cell. Longev. 2019, 2019, 9736047. [Google Scholar] [CrossRef] [PubMed]
- Moore, N.A.; Harris, A.; Wentz, S.; Verticchio Vercellin, A.C.; Parekh, P.; Gross, J.; Hussain, R.M.; Thieme, C.; Siesky, B. Baseline retrobulbar blood flow is associated with both functional and structural glaucomatous progression after 4 years. Br. J. Ophthalmol. 2017, 101, 305–308. [Google Scholar] [CrossRef]
- Jianu, D.C.; Jianu, S.N.; Munteanu, M.; Vlad, D.; Rosca, C.; Petrica, L. Color Doppler imaging features in patients presenting central retinal artery occlusion with and without giant cell arteritis. Vojnosanit. Pregl. 2016, 73, 397–401. [Google Scholar] [CrossRef]
- Pournaras, C.J.; Riva, C.E.; Bresson-Dumont, H.; De Gottrau, P.; Bechetoille, A. Regulation of optic nerve head blood flow in normal tension glaucoma patients. Eur. J. Ophthalmol. 2004, 14, 226–235. [Google Scholar] [CrossRef]
- Grieshaber, M.C.; Mozaffarieh, M.; Flammer, J. What is the link between vascular dysregulation and glaucoma? Surv. Ophthalmol. 2007, 52 (Suppl. 2), S144–S154. [Google Scholar] [CrossRef]
- Schmetterer, L.; Strenn, K.; Findl, O.; Breiteneder, H.; Graselli, U.; Agneter, E.; Eichler, H.G.; Wolzt, M. Effects of antiglaucoma drugs on ocular hemodynamics in healthy volunteers. Clin. Pharmacol. Ther. 1997, 61, 583–595. [Google Scholar] [CrossRef]
- Mendivil, A. Ocular blood flow velocities in patients with proliferative diabetic retinopathy after panretinal photocoagulation. Surv. Ophthalmol. 1997, 42 (Suppl. 1), S89–S95. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, P.; Pournaras, J.A.; Makowiecka, K.; Krivosic, V.; Kedra, A.W.; Le Gargasson, J.F.; Gaudric, A.; Levy, B.I.; Cohen, Y.S.; Tadayoni, R.; et al. Ultrasound assessment of ocular vascular effects of repeated intravitreal injections of ranibizumab for wet age-related macular degeneration. Acta Ophthalmol. 2014, 92, e382–e387. [Google Scholar] [CrossRef] [PubMed]
- Gok, M.; Kapti, H.B. Effect of intravitreal aflibercept (Eylea®) on retrobulbar hemodynamics in patients with neovascular age-related macular degeneration. Int. Ophthalmol. 2018, 38, 713–719. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | Study Condition | Principle of Measurement | Main Content |
|---|---|---|---|
| CDI | In vivo | Combination of B-scan ultrasonography with Doppler technology | Anatomical information Blood flow velocity Visualization of blood flow direction |
| CTA | In vivo | X-rays and advanced computer processing to generate detailed cross-sectional images | Morphological information Determination of vessel diameter |
| MRI | In vivo | Magnetic field to align the protons within water molecules in the body | Morphological information Determination of vessel diameter Volumetric blood flow Blood flow velocity |
| Myography | Ex vivo | Ophthalmic artery isolation and measurement of vascular reactivity by transmitted light microscopy | Vessel diameter Vascular reactivity |
| Methods | Advantages | Limitations |
|---|---|---|
| CDI | Commercially available | No volumetric blood flow data |
| Non-invasive and rapid method | No information about vessel diameter | |
| Studies in laboratory animals available | Angle of incidence as common source of error | |
| Training mandatory to ameliorate reproducibility | ||
| CTA | Rapid and reliable method | Potential adverse effects associated with intravenous contrast agents |
| Reproducible data on blood vessel morphology and course | Limitation in functional studies | |
| Radiation exposure | ||
| Limited use in laboratory animals due to small vessel size and affection by general anesthesia | ||
| MRI | Non-invasive | Expensive |
| High-resolution 3D images with superior soft tissue contrast | Potential adverse effects associated with intravenous contrast agents | |
| Methods without use of contrast agents available | Exposure to noise, claustrophobia and presence of electronic implants as limiting factors for patients | |
| No radiation exposure | Limited use in laboratory animals due to small vessel size and affection by general anesthesia | |
| Myography | Investigation of local mechanisms of vascular reactivity in small laboratory animals | Difficult isolation and preparation of retrobulbar vessels |
| No affection by general anesthesia in laboratory animals | No longitudinal studies available | |
| Studies in genetically modified animals available |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Böhm, E.W.; Grauhan, N.F.; Pfeiffer, N.; Gericke, A. Measurement of Retrobulbar Blood Flow and Vascular Reactivity—Relevance for Ocular and Cardiovascular Diseases. Diagnostics 2023, 13, 3514. https://doi.org/10.3390/diagnostics13233514
Böhm EW, Grauhan NF, Pfeiffer N, Gericke A. Measurement of Retrobulbar Blood Flow and Vascular Reactivity—Relevance for Ocular and Cardiovascular Diseases. Diagnostics. 2023; 13(23):3514. https://doi.org/10.3390/diagnostics13233514
Chicago/Turabian StyleBöhm, Elsa Wilma, Nils F. Grauhan, Norbert Pfeiffer, and Adrian Gericke. 2023. "Measurement of Retrobulbar Blood Flow and Vascular Reactivity—Relevance for Ocular and Cardiovascular Diseases" Diagnostics 13, no. 23: 3514. https://doi.org/10.3390/diagnostics13233514
APA StyleBöhm, E. W., Grauhan, N. F., Pfeiffer, N., & Gericke, A. (2023). Measurement of Retrobulbar Blood Flow and Vascular Reactivity—Relevance for Ocular and Cardiovascular Diseases. Diagnostics, 13(23), 3514. https://doi.org/10.3390/diagnostics13233514