
Prognostic Significance of Ultrasound Characteristics and Body Mass Index in Patients with Apparent Early-Stage Cervical Cancer: A Single-Center, Retrospective, Cohort Study

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
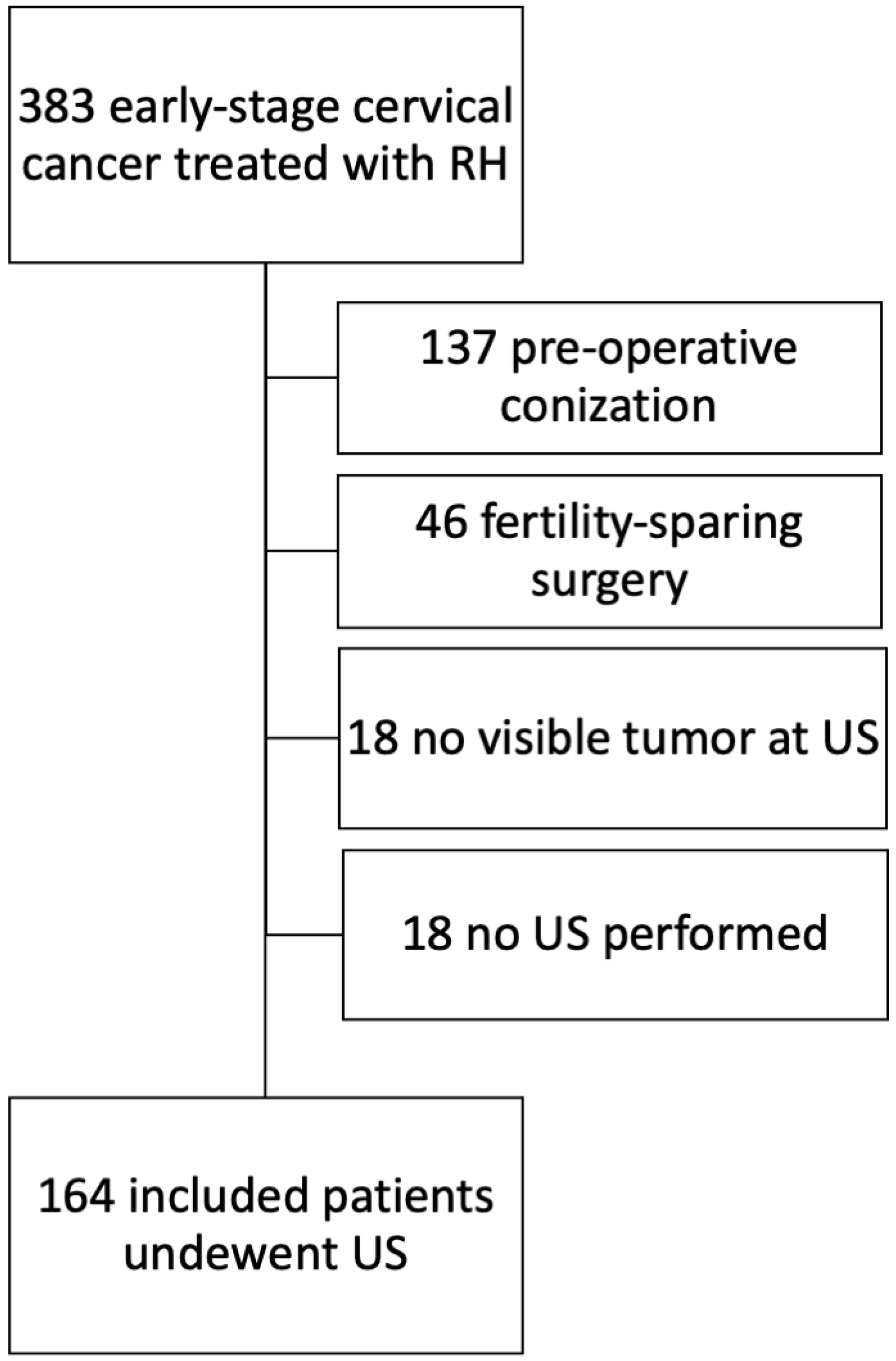
2.1. Study Design and Inclusion/Exclusion Criteria
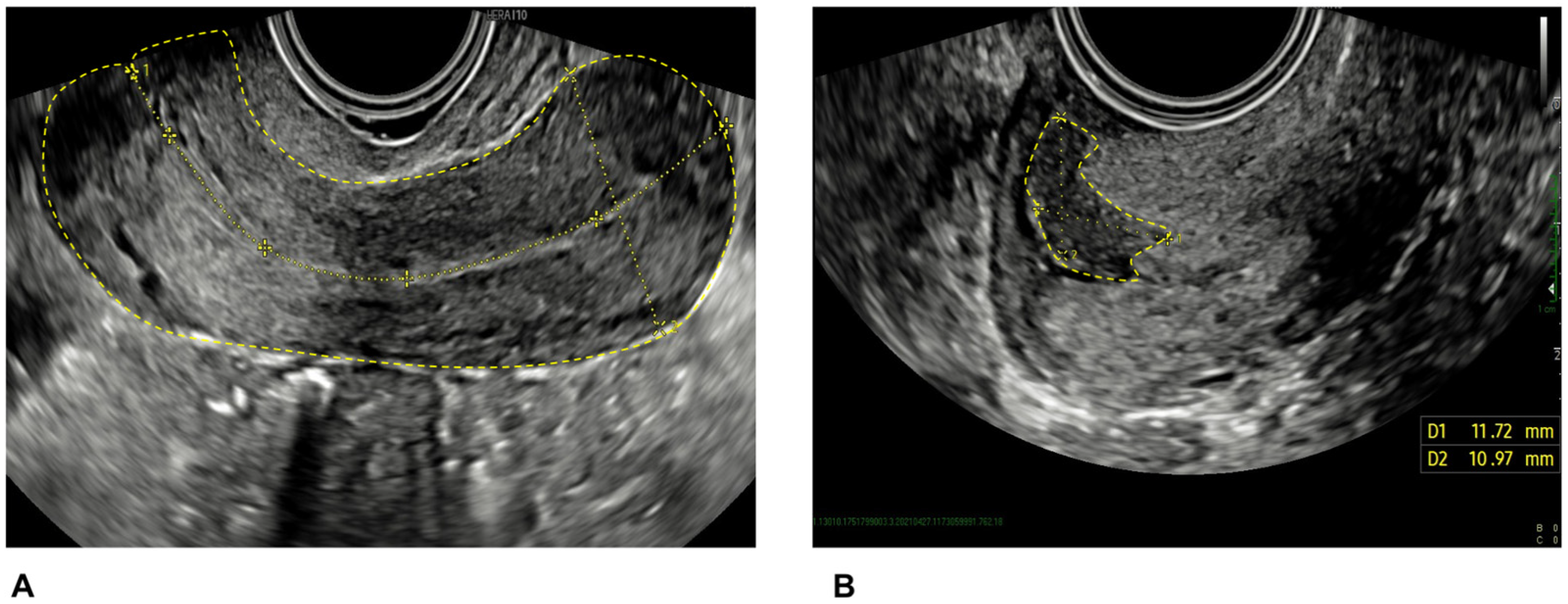
2.2. Ultrasound Scan
2.3. Treatment
2.4. Study Variables
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Ultrasound Scan Findings
3.3. Correlation between Ultrasound and Pathological Findings
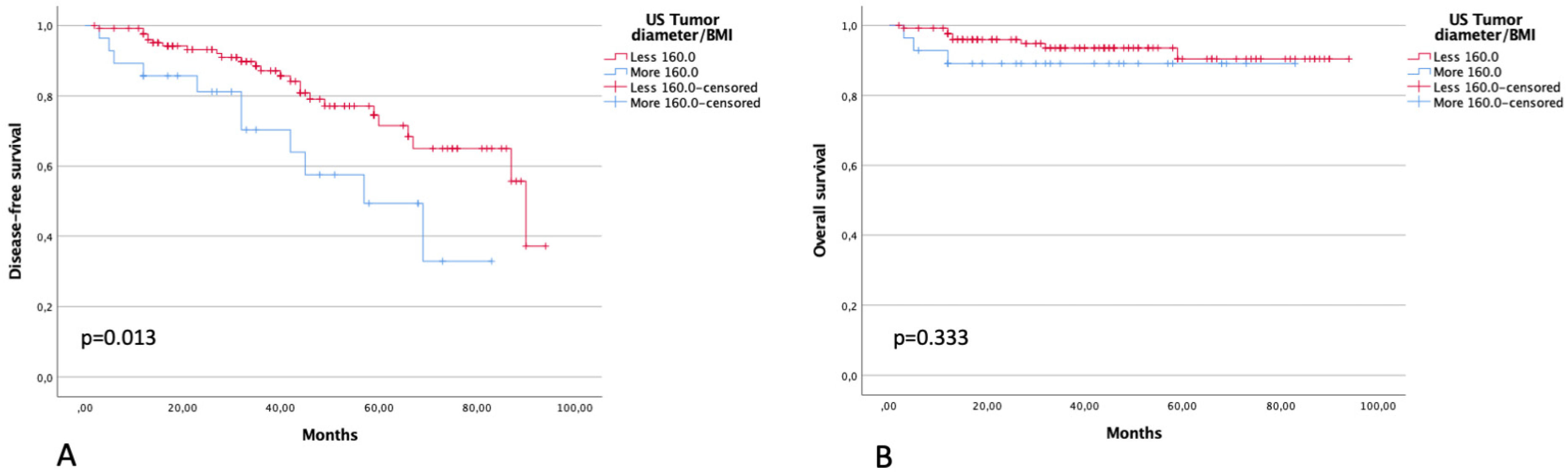
3.4. Survival Analysis
4. Discussion
4.1. Main Findings
4.2. Comparison with Other Related Literature
4.3. Strengths and Limitations
4.4. Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brisson, M.; Kim, J.J.; Canfell, K.; Drolet, M.; Gingras, G.; A Burger, E.; Martin, D.; Simms, K.T.; Bénard, É.; Boily, M.-C.; et al. Impact of HPV vaccination and cervical screening on cervical cancer elimination: A comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet 2020, 395, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Wright, T.C.; Stoler, M.H.; Behrens, C.M.; Sharma, A.; Zhang, G.; Wright, T.L. Primary cervical cancer screening with human papillomavirus: End of study results from the ATHENA study using HPV as the first-line screening test. Gynecol. Oncol. 2015, 136, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. 2), 22–36. [Google Scholar] [CrossRef]
- Matsuo, K.; Machida, H.; Mandelbaum, R.S.; Konishi, I.; Mikami, M. Validation of the 2018 FIGO cervical cancer staging system. Gynecol. Oncol. 2019, 152, 87–93. [Google Scholar] [CrossRef]
- Testa, A.C.; Ludovisi, M.; Manfredi, R.; Zannoni, G.; Gui, B.; Basso, D.; Di Legge, A.; Licameli, A.; Di Bidino, R.; Scambia, G.; et al. Transvaginal ultrasonography and magnetic resonance imaging for assessment of presence, size and extent of invasive cervical cancer. Ultrasound Obstet. Gynecol. 2009, 34, 335–344. [Google Scholar] [CrossRef]
- Gaurilcikas, A.; Vaitkiene, D.; Cizauskas, A.; Inciura, A.; Svedas, E.; Maciuleviciene, R.; Di Legge, A.; Ferrandina, G.; Testa, A.C.; Valentin, L. Early-stage cervical cancer: Agreement between ultrasound and histopathological findings with regard to tumor size and extent of local disease. Ultrasound Obstet. Gynecol. 2011, 38, 707–715. [Google Scholar] [CrossRef]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Meder, C.H.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients With Cervical Cancer. Int. J. Gynecol. Cancer 2018, 28, 641–655. [Google Scholar] [CrossRef]
- Fischerová, D.; Cibula, D. The role of ultrasound in primary workup of cervical cancer staging (ESGO, ESTRO, ESP cervical cancer guidelines). Role ultrazvuku ve stagingu zhoubného nádoru děložního hrdla (doporučení Evropské onkogynekologické, radiační a patologické společnosti). Ceska Gynekol. 2019, 84, 40–48. [Google Scholar]
- López-Hernández, D. Epidemiological Association Between Body Fat Percentage and Cervical Cancer: A Cross-sectional Population-based Survey from Mexico. Arch. Med. Res. 2013, 44, 454–458. [Google Scholar] [CrossRef]
- Poorolajal, J.; Jenabi, E. The association between BMI and cervical cancer risk: A meta-analysis. Eur. J. Cancer Prev. 2016, 25, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.H.; Jackson, A.L.; Soo, A.E.; Orrey, D.C.; Gehrig, P.A.; Kim, K.H. Extremes in body mass index affect overall survival in women with cervical cancer. Gynecol. Oncol. 2016, 141, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Pecorelli, S.; Zigliani, L.; Odicino, F. Revised FIGO staging for carcinoma of the cervix. Int. J. Gynecol. Obstet. 2009, 105, 107–108. [Google Scholar] [CrossRef]
- Fischerova, D. Ultrasound scanning of the pelvis and abdomen for staging of gynecological tumors: A review. Ultrasound Obstet. Gynecol. 2011, 38, 246–266. [Google Scholar] [CrossRef] [PubMed]
- Epstein, E.; Di Legge, A.; Måsbäck, A.; Lindqvist, P.G.; Kannisto, P.; Testa, A.C. Sonographic characteristics of squamous cell cancer and adenocarcinoma of the uterine cervix. Ultrasound Obstet. Gynecol. 2010, 36, 512–516. [Google Scholar] [CrossRef]
- Querleu, D.; Cibula, D.; Abu-Rustum, N.R. 2017 Update on the Querleu–Morrow Classification of Radical Hysterectomy. Ann. Surg. Oncol. 2017, 24, 3406–3412. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observation. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Mantel, N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother. Rep. 1966, 50, 163–170. [Google Scholar]
- Cox, D.R. Models and Life-Tables Regression. J. R. Stat. Soc. Ser. B (Methodol.) 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, M.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.E.; Pappas, L.; Ghia, A.J.; Gaffney, D.K. Impact of tumor size on survival in cancer of the cervix and validation of stage IIA1 and IIA2 subdivisions. Gynecol. Oncol. 2013, 129, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Bizzarri, N.; Anchora, L.P.; Kucukmetin, A.; Ratnavelu, N.; Korompelis, P.; Carbone, V.; Fedele, C.; Bruno, M.; Vizzielli, G.; Gallotta, V.; et al. Protective Role of Conization Before Radical Hysterectomy in Early-Stage Cervical Cancer: A Propensity-Score Matching Study. Ann. Surg. Oncol. 2021, 28, 3585–3594. [Google Scholar] [CrossRef] [PubMed]
- Kizer, N.T.; Thaker, P.H.; Gao, F.; Zighelboim, I.; Powell, M.A.; Rader, J.S.; Mutch, D.G.; Grigsby, P.W. The effects of body mass index on complications and survival outcomes in patients with cervical carcinoma undergoing curative chemoradiation therapy. Cancer 2011, 117, 948–956. [Google Scholar] [CrossRef]
- Calle, E.E.; Kaaks, R. Overweight, obesity and cancer: Epidemiological evidence and proposed mechanisms. Nat. Rev. Cancer 2004, 4, 579–591. [Google Scholar] [CrossRef]
- Morley, J.E.; Thomas, D.R.; Wilson, M.-M.G. Cachexia: Pathophysiology and clinical relevance. Am. J. Clin. Nutr. 2006, 83, 735–743. [Google Scholar] [CrossRef]
- Matsuo, K.; Machida, H.; Blake, E.A.; Takiuchi, T.; Mikami, M.; Roman, L.D. Significance of uterine corpus tumor invasion in early-stage cervical cancer. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 725–734. [Google Scholar] [CrossRef]
- Narayan, K.; Fisher, R.; Bernshaw, D. Significance of tumor volume and corpus uteri invasion in cervical cancer patients treated by radiotherapy. Int. J. Gynecol. Cancer 2006, 16, 623–630. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 164 (Range, %) |
|---|---|
| Age at diagnosis (years) | 48 (25–80) |
| BMI a (kg/m2) | 24.0 (16.9–47.6) |
| Height (cm) | 162 (150–180) |
| Surgical Approach | |
| Laparotomy | 46 (28.0) |
| Laparoscopy | 77 (47.0) |
| Robot | 41 (25.0) |
| Radicality of Radical Hysterectomy | |
| A | 2 (1.2) |
| B | 36 (22.0) |
| C | 126 (76.8) |
| Histology | |
| Squamous cell carcinoma | 104 (63.4) |
| Adenocarcinoma | 45 (27.4) |
| Adeno-squamous | 5 (3.0) |
| Other | 10 (6.1) |
| Grade | |
| 1 | 3 (1.8) |
| 2 | 89 (54.3) |
| 3 | 70 (42.7) |
| Unknown | 2 (1.2) |
| Lymph-Vascular Space Infiltration | |
| Negative | 71 (43.3) |
| Positive | 92 (56.1) |
| Unknown | 1 (0.6) |
| Pathologic Tumor Diameter | |
| ≤20 mm | 46 (28.0) |
| >20 mm | 114 (69.5) |
| Unknown | 4 (2.4) |
| Pathologic Depth of Stromal Infiltration (mm) | 8.2 (0.4–23.0) |
| Largest Pathologic Tumor Diameter (mm) | 26.0 (1.0–55.0) |
| Removed Lymph Nodes | 26 (1–75) |
| Patients with Metastatic Lymph Nodes | 37 (22.5) |
| Pathologic FIGO b Stage 2009 | |
| IA1 | 1 (0.6) |
| IB1 | 113 (68.9) |
| IB2 | 15 (9.1) |
| IIA1 | 7 (4.3) |
| IIA2 | 1 (0.6) |
| IIB | 27 (16.5) |
| Characteristics | n = 164 (Range, %) |
|---|---|
| Uterus volume (mm3) | 74.1 (11.9–966.7) |
| Largest tumor diameter (mm) | 29.0 (1.0–52.0) |
| Tumor volume (mm3) | 6.3 (1.0–58.5) |
| Depth of cervical stromal infiltration | |
| <2/3 | 76 (56.3) |
| >2/3 | 88 (53.7) |
| Echogenicity | |
| Hypoechoic | 122 (74.4) |
| Isoechoic | 26 (15.9) |
| Hyperechoic | 15 (9.1) |
| Not reported | 1 (0.6) |
| Color-Doppler evaluation | |
| No detectable flow (color score 1) | 5 (3.0) |
| Minimal flow (color score 2) | 10 (6.1) |
| Moderate flow (color score 3) | 32 (19.5) |
| Abundant flow (color score 4) | 117 (71.3) |
| Internal uterine orifice involvement | |
| No | 104 (63.4) |
| Yes | 60 (36.6) |
| Pathologic Parametrial Infiltration | |||||
|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | ||||
| Characteristics | Comparison/Measure | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Ultrasound | |||||
| US stromal infiltration | Full thickness vs. superficial/middle third | 1.242 (0.930–1.658) | 0.142 | ||
| Largest tumor diameter (mm) | mm | 1.000 (1.000–1.001) | 0.415 | ||
| Echogenicity | Hypoechoic vs. non-hypoechoic | 0.884 (0.358–2.178) | 0.778 | ||
| US tumor maximum diameter/Uterine CF diameter | ≤37 or >37 | 3.551 (1.350–9.342) | 0.010 | 3.272 (1.231–8.702) | 0.018 |
| Pathologic | |||||
| LVSI | Negative vs. positive | 2.540 (1.008–6.400) | 0.048 | 2.203 (0.857–5.660) | 0.101 |
| Grade | 1–2 vs. 3 | 1.348 (0.889–2.045) | 0.160 | ||
| Pathologic tumor diameter | ≤2 or >2 cm | 2.234 (0.719–6.940) | 0.165 | ||
| RISK OF RECURRENCE | |||
| Characteristics | Comparison/Measure | HR (95% CI) | p-Value |
| Age | ≤50 vs >50 years | 0.608 (0.305–1.215) | 0.159 |
| BMI | ≤20 vs >20 kg/m2 | 0.213 (0.095–0.474) | <0.001 |
| Largest US Tumor diameter | mm | 1.018 (0.983–1.054) | 0.326 |
| Depth of infiltration | Full thickness vs Superficial/Middle third | 1.116 (0.899–1.387) | 0.320 |
| Echogenicity | Hypoechoic vs non-hypoechoic | 1.023 (0.482–2.172) | 0.953 |
| Color-Doppler | Abundant flow vs non-abundant flow | 1.096 (0.909–1.322) | 0.337 |
| Internal uterine os involvement | No vs Yes | 0.863 (0.428–1.741) | 0.681 |
| Tumor Volume | mm3 | 1.035 (1.002–1.069) | 0.038 |
| Tumor Volume/BMI | continuous | 1.010 (1.002–1.018) | 0.011 |
| Largest Tumor diameter/BMI | continuous | 1.009 (1.002–1.017) | 0.017 |
| Tumor Volume/Height of patient | continuous | 1.006 (1.001–1.011) | 0.031 |
| Largest Tumor diameter/Uterine CF diameter | continuous | 1.003 (0.980–1.026) | 0.830 |
| Tumor CF diameter/Uterine CF diameter | continuous | 0.995 (0.971–1.020) | 0.673 |
| RISK OF DEATH | |||
| Characteristics | Comparison/Measure | HR (95% CI) | p-Value |
| Age | ≤50 vs >50 years | 0.455 (0.123–1.683) | 0.238 |
| BMI | ≤20 vs >20 Kg/m2 | 0.205 (0.054–0.784) | 0.021 |
| Largest US Tumor diameter | mm | 0.981 (0.925–1.041) | 0.531 |
| US depth of infiltration | Full thickness vs Superficial/Middle third | 1.260 (0.844–1.881) | 0.258 |
| Echogenicity | Hypoechoic vs non-hypoechoic | 3.505 (0.452–27.183) | 0.230 |
| Color-Doppler | Abundant flow vs non-abundant flow | 0.976 (0.723–1.319) | 0.877 |
| Internal uterine orifice involvement | No vs Yes | 1.041 (0.313–3.465) | 0.948 |
| Tumor Volume | mm3 | 0.975 (0.900–1.055) | 0.527 |
| Tumor Volume/BMI | continuous | 0.998 (0.980–1.016) | 0.824 |
| Largest Tumor diameter/BMI | continuous | 1.005 (0.991–1.018) | 0.499 |
| Tumor Volume/Height of patient | continuous | 0.997 (0.985–1.010) | 0.678 |
| Largest Tumor diameter/Uterine CF diameter | continuous | 0.992 (0.953–1.032) | 0.685 |
| Tumor CF diameter/Uterine CF diameter | continuous | 0.968 (0.924–1.015) | 0.176 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bizzarri, N.; Biscione, A.; Moro, F.; Pedone Anchora, L.; Catinella, V.; Certelli, C.; Teodorico, E.; Fagotti, A.; Fanfani, F.; Kucukmetin, A.; et al. Prognostic Significance of Ultrasound Characteristics and Body Mass Index in Patients with Apparent Early-Stage Cervical Cancer: A Single-Center, Retrospective, Cohort Study. Diagnostics 2023, 13, 583. https://doi.org/10.3390/diagnostics13040583
Bizzarri N, Biscione A, Moro F, Pedone Anchora L, Catinella V, Certelli C, Teodorico E, Fagotti A, Fanfani F, Kucukmetin A, et al. Prognostic Significance of Ultrasound Characteristics and Body Mass Index in Patients with Apparent Early-Stage Cervical Cancer: A Single-Center, Retrospective, Cohort Study. Diagnostics. 2023; 13(4):583. https://doi.org/10.3390/diagnostics13040583
Chicago/Turabian StyleBizzarri, Nicolò, Antonella Biscione, Francesca Moro, Luigi Pedone Anchora, Valeria Catinella, Camilla Certelli, Elena Teodorico, Anna Fagotti, Francesco Fanfani, Ali Kucukmetin, and et al. 2023. "Prognostic Significance of Ultrasound Characteristics and Body Mass Index in Patients with Apparent Early-Stage Cervical Cancer: A Single-Center, Retrospective, Cohort Study" Diagnostics 13, no. 4: 583. https://doi.org/10.3390/diagnostics13040583
APA StyleBizzarri, N., Biscione, A., Moro, F., Pedone Anchora, L., Catinella, V., Certelli, C., Teodorico, E., Fagotti, A., Fanfani, F., Kucukmetin, A., Querleu, D., Ferrandina, G., Scambia, G., & Testa, A. C. (2023). Prognostic Significance of Ultrasound Characteristics and Body Mass Index in Patients with Apparent Early-Stage Cervical Cancer: A Single-Center, Retrospective, Cohort Study. Diagnostics, 13(4), 583. https://doi.org/10.3390/diagnostics13040583