

Endoscopic Ultrasound-Guided Gallbladder Drainage versus Percutaneous Gallbladder Drainage for Acute Cholecystitis: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions
- I.
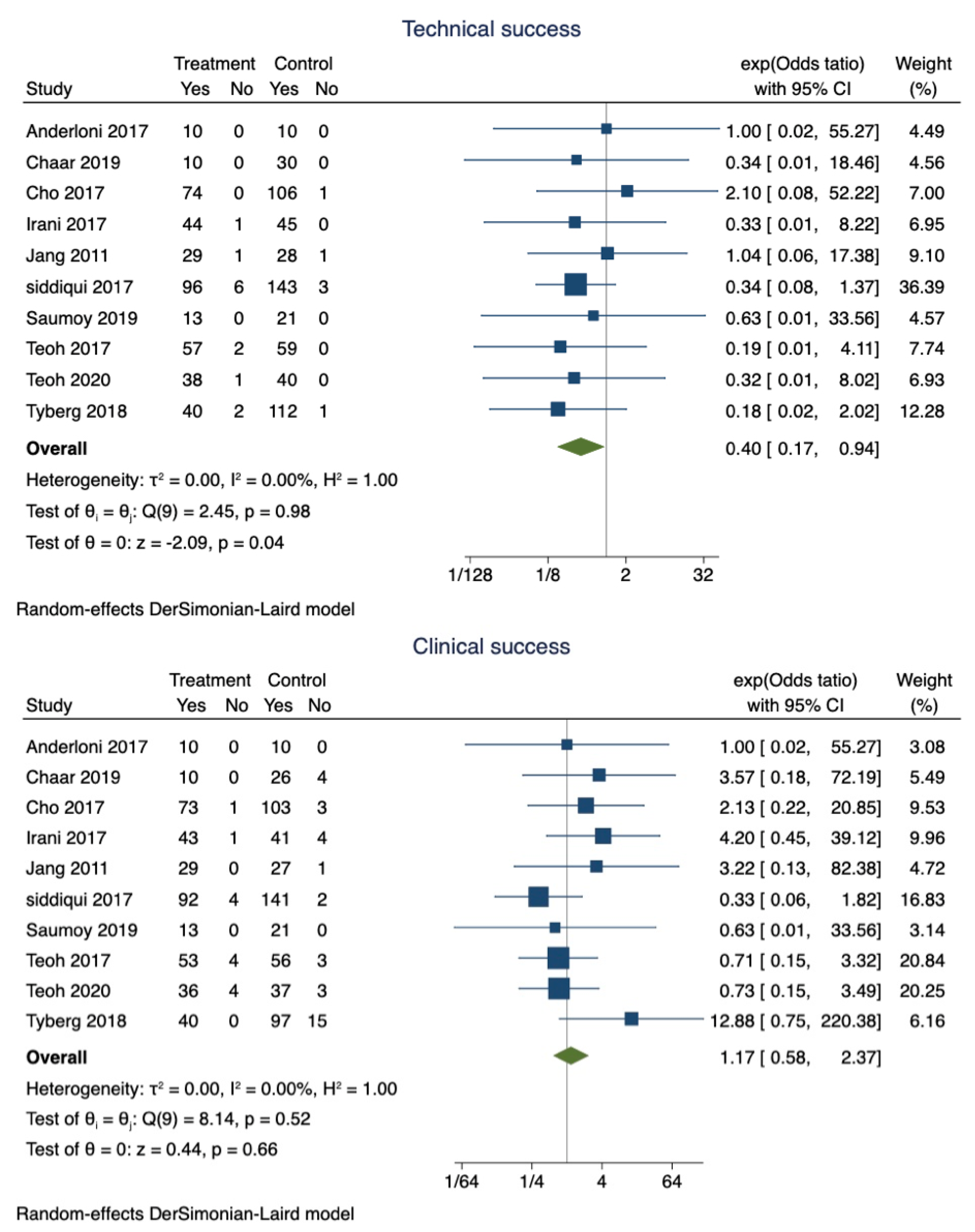
- Technical success: Technical success was defined as successful placement of a drainage catheter or stent placement into the gallbladder, using PT-GBD or EUS-GBD, respectively.
- II.
- Clinical success: Clinical success was defined as the resolution of clinical symptoms of acute cholecystitis (e.g., fever, abdominal pain, and leukocytosis) within 3 days after the procedure.
- III.
- Re-intervention: Reintervention was defined as a repeat procedure due to stent or catheter blockage; a procedure for repositioning or replacement; or a procedure to prevent bleeding or to drain fluid.
2.2. Patients, Intervention, Comparison, and Outcomes (PICO)
- Patients: Patients with acute cholecystitis who were not surgical candidates for cholecystectomy.
- Intervention: Drainage of gallbladder through either EUS-GBD (treatment group).
- Comparison: PT-GBD (control group) for the treatment of acute cholecystitis.
- Outcome: Technical success, clinical success, need for reintervention, and rate of adverse events.
2.3. Selection Criteria
2.4. Search Strategy and Data Extraction
2.5. Outcome Measures
2.6. Quality Assessment
2.7. Statistical Analysis
3. Results
3.1. Search Results and Study Characteristics
3.2. Population and Procedure Characteristics
3.3. Pooled Estimates of Primary Outcomes
- Pooled proportions and odds ratio of technical success:
- b.
- Pooled proportions and odds ratio of clinical success:
- c.
- Pooled proportions and odds ratio of adverse events:
- d.
- Pooled proportions and odds ratio for reintervention:
3.3.1. Secondary Outcomes
- Pooled proportions and odds ratio for readmission:
- b.
- Pooled proportions and odds ratio of mortality:
- c.
- The pooled mean difference in procedure time:
- d.
- The pooled mean difference in length of hospital stays:
- e.
- Pooled proportion of cholecystectomy after successful drainage
3.3.2. Validation of Meta-Analysis Results
- Sensitivity analysis:
- b.
- Heterogeneity:
- c.
- Publication bias:
- d.
- Quality assessment:
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hirota, M.; Takada, T.; Kawarada, Y.; Nimura, Y.; Miura, F.; Hirata, K.; Mayumi, T.; Yoshida, M.; Strasberg, S.; Pitt, H.; et al. Diagnostic criteria and severity assessment of acute cholecystitis: Tokyo Guidelines. J. Hepato Biliary Pancreat. Surg. 2007, 14, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.C.; Markar, S.; Mackenzie, H.; Baser, O.; Wiggins, T.; Askari, A.; Hanna, G.; Faiz, O.; Mayer, E.; Bicknell, C.; et al. An observational study of the timing of surgery, use of laparoscopy and outcomes for acute cholecystitis in the USA and UK. Surg. Endosc. 2018, 32, 3055–3063. [Google Scholar] [CrossRef] [PubMed]
- Houghton, P.W.; Jenkinson, L.R.; Donaldson, L.A. Cholecystectomy in the elderly: A prospective study. Br. J. Surg. 1985, 72, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Boregowda, U.; Umapathy, C.; Nanjappa, A.; Wong, H.; Desai, M.; Roytman, M.; Theethira, T.; Saligram, S. Endoscopic ultrasound guided gallbladder drainage-is it ready for prime time? World J. Gastrointest. Pharmacol. Ther. 2018, 9, 47–54. [Google Scholar] [CrossRef]
- Irani, S.; Ngamruengphong, S.; Teoh, A.; Will, U.; Nieto, J.; Abu Dayyeh, B.K.; Gan, S.I.; Larsen, M.; Yip, H.C.; Topazian, M.D.; et al. Similar Efficacies of Endoscopic Ultrasound Gallbladder Drainage with a Lumen-Apposing Metal Stent versus Percutaneous Transhepatic Gallbladder Drainage for Acute Cholecystitis. Clin. Gastroenterol. Hepatol. 2017, 15, 738–745. [Google Scholar] [CrossRef]
- Tyberg, A.; Saumoy, M.; Sequeiros, E.V.; Giovannini, M.; Artifon, E.; Teoh, A.; Nieto, J.; Desai, A.P.; Kumta, N.A.; Gaidhane, M.; et al. EUS-guided versus Percutaneous Gallbladder Drainage: Isn’t It Time to Convert? J. Clin. Gastroenterol. 2018, 52, 79–84. [Google Scholar] [CrossRef]
- Teoh, A.Y.B.; Serna, C.; Penas, I.; Chong, C.C.N.; Perez-Miranda, M.; Ng, E.K.W.; Lau, J.Y.W. Endoscopic ultrasound-guided gallbladder drainage reduces adverse events compared with percutaneous cholecystostomy in patients who are unfit for cholecystectomy. Endoscopy 2017, 49, 130–138. [Google Scholar] [CrossRef]
- Khan, M.A.; Atiq, O.; Kubiliun, N.; Ali, B.; Kamal, F.; Nollan, R.; Ismail, M.K.; Tombazzi, C.; Kahaleh, M.; Baron, T.H. Efficacy and safety of endoscopic gallbladder drainage in acute cholecystitis: Is it better than percutaneous gallbladder drainage? Gastrointest. Endosc. 2017, 85, 76–87.e73. [Google Scholar] [CrossRef]
- Kedia, P.; Sharaiha, R.Z.; Kumta, N.A.; Widmer, J.; Jamal-Kabani, A.; Weaver, K.; Benvenuto, A.; Millman, J.; Barve, R.; Gaidhane, M.; et al. Endoscopic gallbladder drainage compared with percutaneous drainage. Gastrointest. Endosc. 2015, 82, 1031–1036. [Google Scholar] [CrossRef]
- Ahmed, O.; Rogers, A.C.; Bolger, J.C.; Mastrosimone, A.; Lee, M.J.; Keeling, A.N.; Cheriyan, D.; Robb, W.B. Meta-analysis of outcomes of endoscopic ultrasound-guided gallbladder drainage versus percutaneous cholecystostomy for the management of acute cholecystitis. Surg. Endosc. 2018, 32, 1627–1635. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Anderloni, A.; Fugazza, A.; Costa, G.; Ardito, A.; Mei, S.; Ceolin, M.; Pedicini, V.; Kurihara, H.; Repici, A. Eus-guided versus percutaneous gallbladder drainage in fragile patients with acute cholecystitis: A retrospective analysis. Dig. Liver Dis. 2017, 49, e125. [Google Scholar] [CrossRef]
- Chaar, A.; Zamora-Sifuentes, J.; Nasser, A.; Szpunar, S.; Barawi, M. EUS-Guided versus Percutaneous gallbladder drainage in patients who are unfit for cholecystectomy: A community hospital setting. Gastrointest. Endosc. 2019, 89, AB571. [Google Scholar] [CrossRef]
- Cho, D.H.; Lee, S.S.; Oh, D.; Song, T.J.; Park, D.H.; Seo, D.W.; Lee, S.K.; Kim, M.-H. EUS-Guided Gallbladder Drainage Reduces Late Adverse Event and Need for Re-Intervention Compared with Percutaneous Cholecystostomy in Patents Who Are Not Eligible for Surgery. Gastrointest. Endosc. 2017, 85, AB469. [Google Scholar] [CrossRef]
- Jang, J.W.; Lee, S.S.; Song, T.J.; Hyun, Y.S.; Park, D.H.; Seo, D.-W.; Lee, S.-K.; Kim, M.-H.; Yun, S.-C. Endoscopic Ultrasound-Guided Transmural and Percutaneous Transhepatic Gallbladder Drainage Are Comparable for Acute Cholecystitis. Gastroenterology 2012, 142, 805–811. [Google Scholar] [CrossRef]
- Saumoy, M.; Tyberg, A.; Brown, E.; Eachempati, S.R.; Lieberman, M.; Afaneh, C.; Kunda, R.; Cosgrove, N.; Siddiqui, A.; Gaidhane, M.; et al. Successful Cholecystectomy after Endoscopic Ultrasound Gallbladder Drainage Compared with Percutaneous Cholecystostomy, Can it Be Done? J. Clin. Gastroenterol. 2019, 53, 231–235. [Google Scholar] [CrossRef]
- Shah, R.N.; Khara, H.S.; Iqbal, U.; Confer, B.; Khan, Y.I.; Diehl, D.L.; Berger, A.L.; Bhanushali, A.; Widom, K.A.; Torres, D.M. 731 Endoscopic ultrasound-guided gallbladder drainage (EUS-GB) compared to percutaneous gallbladder drainage (PC-GB) for high-risk non-surgical patients with acute cholecystitis: A large academic tertiary care center experience. Gastrointest. Endosc. 2020, 91, AB65–AB66. [Google Scholar] [CrossRef]
- Siddiqui, A.; Kunda, R.; Tyberg, A.; Arain, M.A.; Noor, A.; Mumtaz, T.; Iqbal, U.; Loren, D.E.; Kowalski, T.E.; Adler, D.G.; et al. Three-way comparative study of endoscopic ultrasound-guided transmural gallbladder drainage using lumen-apposing metal stents versus endoscopic transpapillary drainage versus percutaneous cholecystostomy for gallbladder drainage in high-risk surgical patients with acute cholecystitis: Clinical outcomes and success in an International, Multicenter Study. Surg. Endosc. 2019, 33, 1260–1270. [Google Scholar] [CrossRef]
- Teoh, A.Y.; Kitano, M.; Itoi, T.; Perez-Miranda, M.; Ogura, T.; Chan, S.M.; De la Serna, C.; Omoto, S.; Torres-Yuste, R.; Tsuchiya, T.; et al. 1025 EUS-guided gallbladder drainage reduced adverse events as compared to percutaneous cholecystostomy in patients suffering from acute cholecystitis that were at high risk for cholecystectomy. a randomized controlled trial. Gastrointest. Endosc. 2019, 89, AB130–AB131. [Google Scholar] [CrossRef]
- Kunda, R.; Sharaiha, R.Z.; Siddiqui, A.; Tyberg, A.; Arain, M.A.; Noor, A.; Mumtaz, T.; Iqbal, U.; Loren, D.E.; Kowalski, T.E.; et al. 212 Endoscopic Ultrasound-Guided Transmural Gallbladder Drainage Using Lumen-Apposing Metal Stents versus Endoscopic Transpapillary Drainage versus Percutaneous Cholecystostomy for Gallbladder Drainage in High-Risk Surgical Patients with Acute Cholecystit. Gastrointest. Endosc. 2017, 85, AB60–AB61. [Google Scholar] [CrossRef]
- Zhang, L.; Gerson, L.; Maluf-Filho, F. Systematic review and meta-analysis in GI endoscopy: Why do we need them? How can we read them? Should we trust them? Gastrointest. Endosc. 2018, 88, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Suzuki, K.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Endo, I.; Iwashita, Y.; Hibi, T.; Pitt, H.A.; Umezawa, A.; et al. Tokyo Guidelines 2018: Flowchart for the management of acute cholecystitis. J. Hepato Biliary Pancreat. Sci. 2018, 25, 55–72. [Google Scholar] [CrossRef] [PubMed]
- Anderloni, A.; Buda, A.; Vieceli, F.; Khashab, M.A.; Hassan, C.; Repici, A. Endoscopic ultrasound-guided transmural stenting for gallbladder drainage in high-risk patients with acute cholecystitis: A systematic review and pooled analysis. In Surgical Endoscopy and Other Interventional Techniques; Springer: Berlin/Heidelberg, Germany, 2016; Volume 30, pp. 5200–5208. [Google Scholar]
- Walter, D.; Teoh, A.Y.; Itoi, T.; Perez-Miranda, M.; Larghi, A.; Sanchez-Yague, A.; Siersema, P.D.; Vleggaar, F.P. EUS-guided gall bladder drainage with a lumen-apposing metal stent: A prospective long-term evaluation. Gut 2016, 65, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.M.; Teoh, A.Y.B.; Yip, H.C.; Wong, V.W.Y.; Chiu, P.W.Y.; Ng, E.K.W. Feasibility of per-oral cholecystoscopy and advanced gallbladder interventions after EUS-guided gallbladder stenting (with video). Gastrointest. Endosc. 2017, 85, 1225–1232. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Author | Country | Type of Study | Stent Type | Follow Up Duration in Days | Patients (n) | Technical Success (n) | Clinical Success (n) | Adverse Events (n) | Reintervention (n) | Readmission (n) | Mortality (n) | Procedure Time (min) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anderloni 2017 [12] * | Italy | Retrospective | LAMS | EUS-GBD | NA | 10 | 10 | 10 | 1 | NA | NA | NA | NA |
| PT-GBD | NA | 10 | 10 | 10 | 2 | NA | NA | NA | NA | ||||
| Chaar 2019 [13] * | USA | Retrospective | LAMS | EUS-GBD | 122.3 | 10 | 10 | 10 | 2 | 1 | 2 | 0 | 0 |
| PT-GBD | 151.6 | 30 | 30 | 26 | 13 | 6 | 8 | 5 | 0 | ||||
| Cho 2017 [14] * | Korea | Retrospective | LAMS | EUS-GBD | NA | 74 | 74 | 73 | 5 | 7 | NA | NA | NA |
| PT-GBD | NA | 107 | 106 | 103 | 21 | 23 | NA | NA | NA | ||||
| Irani 2017 [5] | International | Retrospective | LAMS | EUS-GBD | 215 (1–621) | 45 | 44 | 43 | 8 | NA | NA | 1 | 22 |
| PT-GBD | 265 (1–1638) | 45 | 45 | 41 | 14 | NA | NA | 3 | 28 | ||||
| Jang 2017 [15] | Korea | RCT | NBD | EUS-GBD | NA | 30 | 29 | 29 | 2 | NA | NA | NA | 24 |
| PT-GBD | NA | 29 | 28 | 27 | 1 | NA | NA | NA | 23 | ||||
| Siddiqui 2019 [18] | USA | Retrospective | LAMS | EUS-GBD | 156 | 102 | 96 | 92 | 13 | NA | NA | NA | NA |
| PT-GBD | 156 | 146 | 143 | 141 | 29 | NA | NA | NA | NA | ||||
| Saumoy 2019 [16] | USA | Retrospective | LAMS | EUS-GBD | NA | 13 | 13 | 13 | 2 | 8 | 4 | NA | NA |
| PT-GBD | NA | 21 | 21 | 21 | 3 | 15 | 2 | NA | NA | ||||
| Shah 2020 [17] * | USA | Retrospective | LAMS | EUS-GBD | NA | 33 | NA | NA | 2 | 1 | NA | 1 | NA |
| PT-GBD | NA | 79 | NA | NA | 43 | 79 | NA | 4 | NA | ||||
| Teoh 2017 [7] | Japan | Retrospective | LAMS | EUS-GBD | NA | 59 | 57 | 53 | 19 | NA | 4 | 5 | NA |
| PT-GBD | NA | 59 | 59 | 56 | 44 | NA | 42 | 1 | NA | ||||
| Teoh 2019 [19] | International | RCT | LAMS | EUS-GBD | 365 | 39 | 38 | 36 | 5 | 1 | 10 | 3 | 22.7 |
| PT-GBD | 365 | 40 | 40 | 37 | 19 | 12 | 14 | 4 | 27.4 | ||||
| Tyberg 2018 [6] | International | Prospective cohort study | Multiple | EUS-GBD | NA | 42 | 40 | 40 | 7 | 4 | 6 | 0 | NA |
| PT-GBD | NA | 113 | 112 | 97 | 21 | 28 | 27 | 4 | NA |
| Complications | EUS-GBD | PT-GBD |
|---|---|---|
| Abdominal pain | 6 | 47 |
| Drain/stent dislodgement | 3 | 28 |
| Bleeding | 10 | 22 |
| Bile leak | 4 | 11 |
| Infection | 0 | 9 |
| Stent obstruction | 6 | 9 |
| Recurrent cholecystitis | 6 | 8 |
| Pericholecystic collection | 2 | 3 |
| Pneumonia | 4 | 3 |
| Bowel perforation | 3 | 0 |
| Pneumoperitoneum | 2 | 0 |
| Drainage around the catheter | 0 | 2 |
| Peritonitis | 1 | 0 |
| Analysis | Number of Studies | Pooled Proportions (EUS vs. PT) | Pooled Estimates Odds Ratio or Mean Difference (95% CI) | I2 | p-Value |
|---|---|---|---|---|---|
| Primary outcomes | |||||
| Technical success | 10 | 89.9% vs. 87.5% | 0.40 (0.17–0.94) | 0% | p = 0.04 |
| Clinical success | 10 | 97% vs. 94.1% | 1.35 (0.65–2.79) | 0% | p = 0.42 |
| Adverse events | 11 | 14.6% vs. 30% | 0.35 (0.21–0.61) | 54.29% | p = 0.00 |
| Reinterventions | 5 | 15% vs. 67% | 0.18 (0.05–0.57) | 67.48% | p = 0.02 |
| Secondary outcomes | |||||
| Readmission rate | 5 | 16.4% vs. 35.5% | 0.34 (0.08–1.54) | 85.39% | p = 0.16 |
| Mortality | 6 | 4% vs. 5.5% | 0.73 (0.30–1.80) | 0% | p = 0.50 |
| Procedure time | 3 | NA | 0.42 (−6.14, 6.98) | 84.43% | p = 0.90 |
| Recurrent cholecystitis | 3 | 4.3% vs. 8.2% | 0.75 (0.15–3.79) | 55.55% | p = 0.73 |
| Length of hospital stay | 5 | 7.4 ± 5.12 days vs. 11.3 ± 4.7 days | −3.53 (−5.91, −1.15) | 99.05% | p = 0.00 |
| Cholecystectomy | 3 | 22.6% vs. 27.3% | 0.32 (0.08–1.32) | 66.93% | p = 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boregowda, U.; Chen, M.; Saligram, S. Endoscopic Ultrasound-Guided Gallbladder Drainage versus Percutaneous Gallbladder Drainage for Acute Cholecystitis: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 657. https://doi.org/10.3390/diagnostics13040657
Boregowda U, Chen M, Saligram S. Endoscopic Ultrasound-Guided Gallbladder Drainage versus Percutaneous Gallbladder Drainage for Acute Cholecystitis: A Systematic Review and Meta-Analysis. Diagnostics. 2023; 13(4):657. https://doi.org/10.3390/diagnostics13040657
Chicago/Turabian StyleBoregowda, Umesha, Millie Chen, and Shreyas Saligram. 2023. "Endoscopic Ultrasound-Guided Gallbladder Drainage versus Percutaneous Gallbladder Drainage for Acute Cholecystitis: A Systematic Review and Meta-Analysis" Diagnostics 13, no. 4: 657. https://doi.org/10.3390/diagnostics13040657