
Development and Integration of DOPS as Formative Tests in Head and Neck Ultrasound Education: Proof of Concept Study for Exploration of Perceptions

 , , , ,
, , , ,
Abstract
:1. Background
1.1. Test Formats in Ultrasound Training
1.2. DOPS Tests in Otorhinolaryngology
2. Methods
2.1. Head Neck Ultrasound DOPS Test Development
2.2. Evaluation Tools for the Exploration of Perceptions and Attitudes
2.3. Test Procedure, Participants, and Examiners
2.4. Statistical Analysis
3. Results
3.1. Sample Description
3.2. Results of the Evaluation of DOPS
3.3. Free-Text Comments
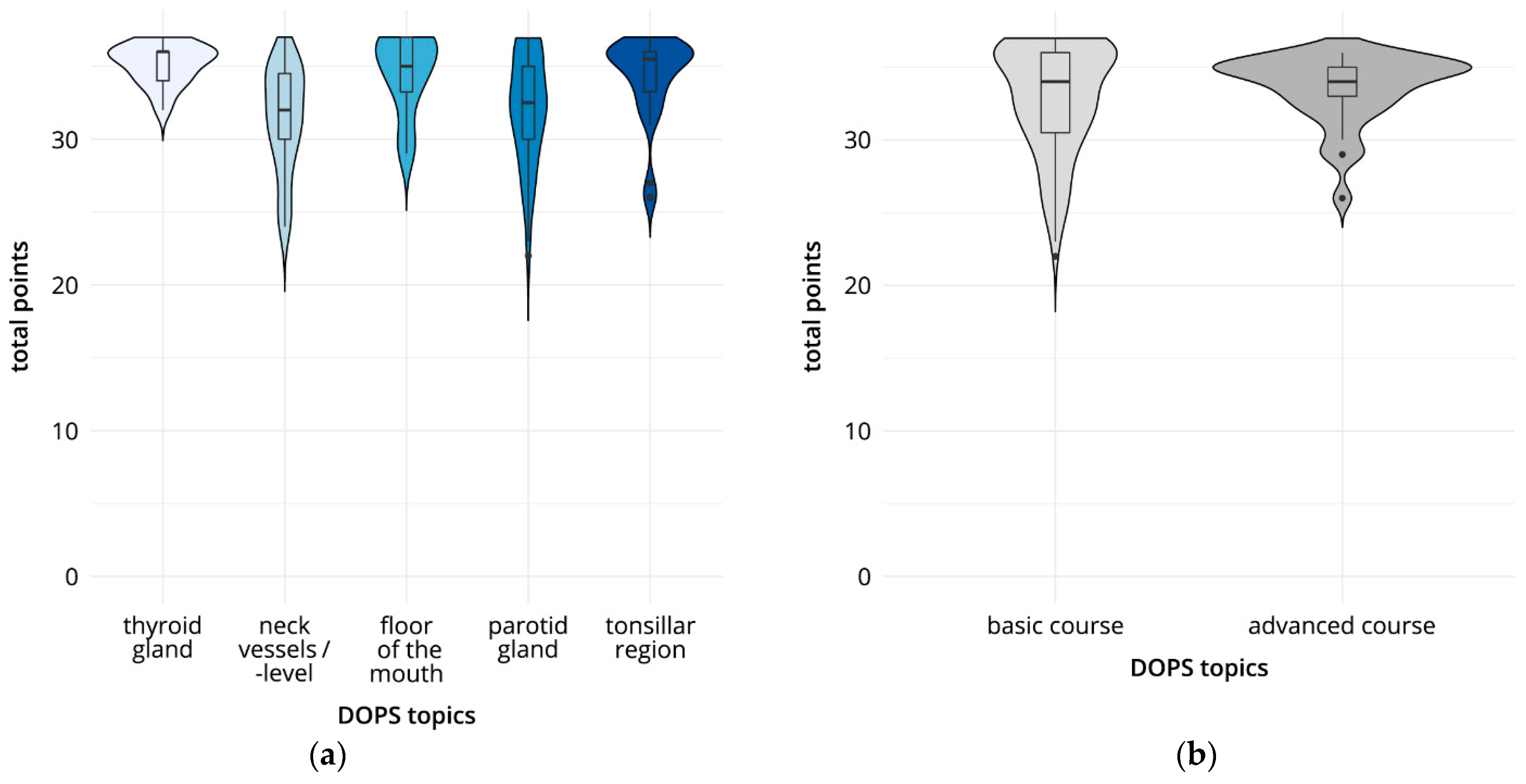
3.4. Results of the DOPS Carried Out
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bundesärztekammer [Federal Medical Association]. (Muster-)Weiterbildungsordnung 2018 in der Fassung vom 26.06.2021; Bundesärztekammer: Berlin, Germany, 2021. [Google Scholar]
- Welle, R.; Seufferlein, T.; Kratzer, W. Current state of under- and postgraduate education in abdominal ultrasonography at German university hospitals. A panel study over 20 years. Z. Gastroenterol. 2021, 59, 225–240. [Google Scholar] [PubMed]
- Recker, F.; Blank, V.; Diederich, H.; Huckauf, S.; Lindner, F.; Minier, M.; Neubauer, B.; Wielandner, A.; Sachs, A. Ultraschallausbildung an deutschsprachigen Universitäten: Wo stehen wir und wo soll es hingehen? Ultraschall Med.—Eur. J. Ultrasound. 2014, 35, 4–12. [Google Scholar] [CrossRef]
- Cantisani, V.; Jenssen, C.; Dietrich, C.F.; Ewertsen, C.; Piscaglia, F. Clinical practice guidance and education in ultrasound: Evidence and experience are two sides of one coin! Ultraschall Med. 2022, 43, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Sektion-Kopf-Hals D. Kurscurriculum der Sektion Kopf—Hals Degum.de: Deutsche Gesellschaft für Ultraschall in der Medizin. 2015. Available online: https://www.degum.de/fileadmin/dokumente/sektionen/kopf-hals/KPF_2015__Kurscurriculum_2015-05-18.pdf (accessed on 10 October 2022).
- Kassenärztliche Bundesvereinigung (KBV). Vereinbarung von Qualitätssicherungsmassnahmen nach § 135 Abs. 2 SGB V zur Ultraschalldiagnostik (Ultraschall-Vereinbarung) vom 31.10.2008 in der ab dem 01.10.2021 geltenden Fassung. 2021. Available online: https://www.kbv.de/media/sp/Ultraschallvereinbarung.pdf (accessed on 21 March 2022).
- Künzel, J.; Bozzato, V.; Ernst, B.P.; Bozzato, A. Musterbefund zur sonografischen Diagnostik im Kopf-Hals-Bereich (Sektion Kopf-Hals der DEGUM). Ultraschall Med.—Eur. J. Ultrasound. 2022. [Google Scholar] [CrossRef] [PubMed]
- Todsen, T.; Ewertsen, C.; Jenssen, C.; Evans, R.; Kuenzel, J. Head and Neck Ultrasound—EFSUMB Training Recommendations for the Practice of Medical Ultrasound in Europe. Ultrasound Int. Open. 2022, 8, E29–E34. [Google Scholar] [CrossRef] [PubMed]
- Schuwirth, L.; van der Vleuten, C. Merging views on assessment. Med. Educ. 2004, 38, 1208–1210. [Google Scholar] [CrossRef] [PubMed]
- Ben-David, M.F. The role of assessment in expanding professional horizons. Med. Teach. 2000, 22, 472–477. [Google Scholar] [CrossRef]
- Miller, G.E. The assessment of clinical skills/competence/performance. Acad. Med. J. Assoc. Am. Med. Coll. 1990, 65 (Suppl. 9), S63–S67. [Google Scholar] [CrossRef]
- Harden, R.M.; Gleeson, F.A. Assessment of clinical competence using an objective structured clinical examination (OSCE). Med. Educ. 1979, 13, 41–54. [Google Scholar] [CrossRef]
- Norcini, J.J.; Blank, L.L.; Duffy, F.D.; Fortna, G.S. The mini-CEX: A method for assessing clinical skills. Ann. Intern. Med. 2003, 138, 476–481. [Google Scholar] [CrossRef]
- Heinzow, H.S.; Friederichs, H.; Lenz, P.; Schmedt, A.; Becker, J.C.; Hengst, K.; Marschall, B.; Domagk, D. Teaching ultrasound in a curricular course according to certified EFSUMB standards during undergraduate medical education: A prospective study. BMC Med. Educ. 2013, 13, 84. [Google Scholar] [CrossRef]
- Erfani Khanghahi, M.; Ebadi Fard Azar, F. Direct observation of procedural skills (DOPS) evaluation method: Systematic review of evidence. Med. J. Islam Repub Iran. 2018, 32, 254–261. [Google Scholar] [CrossRef] [PubMed]
- ul Haq, I.; Jamil, B.; Durrani, M. Procedural skills. Prof. Med. J. 2018, 25, 1207–1212. [Google Scholar] [CrossRef]
- Mohamadirizi, S.; Mardanian, F.; Torabi, F. The effect of direct observation of procedural skills method on learning clinical skills of midwifery students of medical sciences. J. Educ. Health Promot. 2020, 9, 91. [Google Scholar] [PubMed]
- Höhne, E.; Recker, F.; Dietrich, C.F.; Schäfer, V.S. Assessment Methods in Medical Ultrasound Education. Front. Med. 2022, 9, 871957. [Google Scholar] [CrossRef] [PubMed]
- Todsen, T.; Tolsgaard, M.G.; Olsen, B.H.; Henriksen, B.M.; Hillingsø, J.G.; Konge, L.; Jensen, M.L.; Ringsted, C. Reliable and valid assessment of point-of-care ultrasonography. Ann Surg. 2015, 261, 309–315. [Google Scholar] [CrossRef]
- Hofer, M.; Kamper, L.; Sadlo, M.; Sievers, K.; Heussen, N. Evaluation of an OSCE assessment tool for abdominal ultrasound courses. Ultraschall Med. 2011, 32, 184–190. [Google Scholar] [CrossRef]
- Tolsgaard, M.G.; Todsen, T.; Sorensen, J.L.; Ringsted, C.; Lorentzen, T.; Ottesen, B.; Tabor, A. International multispecialty consensus on how to evaluate ultrasound competence: A Delphi consensus survey. PLoS ONE 2013, 8, e57687. [Google Scholar] [CrossRef]
- Todsen, T.; Melchiors, J.; Charabi, B.; Henriksen, B.; Ringsted, C.; Konge, L.; von Buchwald, C. Competency-based assessment in surgeon-performed head and neck ultrasonography: A validity study. Laryngoscope 2018, 128, 1346–1352. [Google Scholar] [CrossRef]
- Rehman, I.; Shah, R.; Kamal, A.; Ahmed, M. Using DOPS (directly observed procedural skills) for pre call assessment of ultrasound proficiency of first year radiology residents: Development and initial analysis. Pak J. Radiol. 2019, 29, 166–172. [Google Scholar]
- Kara, C.O.; Mengi, E.; Tümkaya, F.; Topuz, B.; Ardıç, F.N. Direct observation of procedural skills in otorhinolaryngology training. Turk. Arch. Otorhinolaryngol. 2018, 56, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Bansal, M. Introduction of directly observed procedural skills (DOPS) as a part of competency-based medical education in otorhinolaryngology. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Awad, Z.; Hayden, L.; Muthuswamy, K.; Ziprin, P.; Darzi, A.; Tolley, N.S. Does direct observation of procedural skills reflect trainee’s progress in otolaryngology? Clin. Otolaryngol. 2014, 39, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Weimer, J.M.; Rink, M.; Müller, L.; Arens, C.; Bozzato, A.; Künzel, J. Sonographic diagnostics in the head and neck area, part 2—Transcervical sonography. Laryngorhinootologie 2022, 101, 156–175. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Arbeitskreis “Lehrevaluation” im Fach Psychologie (Gläßer, E., Gollwitzer, M., Kranz, D., Meiniger, C., Schlotz, W., Schnell, T. & Voß, A.) in Zusammenarbeit mit dem Zentrum für Psychologische Diagnostik, Begutachtung und Evaluation (ZDiag). 2002. TRIL. Trierer Inventar zur Lehrevaluation [Verfahrensdokumentation, Fragebogen für je Weibliche und Männliche Dozierende]. In Leibniz-Institut für Psychologie (ZPID) (Hrsg.), Open Test Archive. Trier: ZPID. Available online: https://www.psycharchives.org/en/item/b6adcb29-8e57-45b0-91cb-f1931c0fb552 (accessed on 21 March 2022).
- Pierre, R.B.; Wierenga, A.; Barton, M.; Branday, J.M.; Christie, C.D.C. Student evaluation of an OSCE in paediatrics at the University of the West Indies, Jamaica. BMC Med. Educ. 2004, 4, 22. [Google Scholar] [CrossRef] [PubMed]
- Weisser, F.O.; Dirks, B.; Georgieff, M. Objective Structured Clinical Examination (OSCE): Eine neue Prüfungsform in der notfallmedizinischen Ausbildung. Notf Rett. 2004, 7, 237–243. [Google Scholar]
- Dabir, S.; Hoseinzadeh, M.; Mosaffa, F.; Hosseini, B.; Dahi, M.; Vosoughian, M.; Moshari, M.; Tabashi, S.; Dabbagh, O. The effect of repeated direct observation of procedural skills (R-DOPS) assessment method on the clinical skills of anesthesiology residents. Anesthesiol. Pain Med. 2021, 11, e111074. [Google Scholar] [CrossRef]
- Jang, T.; Aubin, C.; Naunheim, R. Minimum training for right upper quadrant ultrasonography. Am. J. Emerg. Med. 2004, 22, 439–443. [Google Scholar] [CrossRef]
- Duanmu, Y.; Henwood, P.C.; Takhar, S.S.; Chan, W.; Rempell, J.S.; Liteplo, A.S.; Koskenoja, V.; Noble, V.E.; Kimberly, H.H. Correlation of OSCE performance and point-of-care ultrasound scan numbers among a cohort of emergency medicine residents. Ultrasound J. 2019, 11, 3. [Google Scholar] [CrossRef]
- DEGUM. Prüfung Stufe II Anästhesiologie Deutsche Gesellschaft für Ultraschall in der Medizin. 2022. Available online: https://www.degum.de/fachgebiete/sektionen/anaesthesiologie/mehrstufenkonzept-zertifizierung/pruefung-stufe-ii-anae.html (accessed on 21 March 2022).
- Hochlehnert, A.; Schultz, J.-H.; Möltner, A.; Tımbıl, S.; Brass, K.; Jünger, J. Electronic acquisition of OSCE performance using tablets. GMS Z. Med. Ausbild. 2015, 32, Doc41. [Google Scholar]
- Kuhn, S.; Frankenhauser, S.; Tolks, D. Digital learning and teaching in medical education: Already there or still at the beginning? Bundesgesundheitsblatt Gesundh. Gesundh. 2018, 61, 201–209. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Topics | Content | Landmark Structures in Orientation Sections | Assessment |
|---|---|---|---|
| Thyroid gland | |||
| DOPS I | Assessment of thyroid, trachea, esophagus | Thyroid, trachea, esophagus, common carotid artery; internal jugular vein, sternocleidomastoid, omohyoid, spinal column | Thyroid gland volume |
| Cervical vessels and cervical level | |||
| DOPS II | Assessment of cervical vessels and cervical level | Common carotid artery, internal carotid artery, external carotid artery, internal jugular vein. sternocleidomastoid, trapezius, omohyoid, posterior belly of digastric muscle | Intima–media thickness, arterial flow profiles |
| Floor of the mouth | |||
| DOPS III | Assessment of the floor of the mouth and larynx | Anterior belly of digastric muscle, mylohyoid, geniohyoid, sublingual gland, tongue, vallecula of hyoid bone, thyroid cartilage, arytenoid cartilage | Measurement of the sublingual gland, with bilateral comparison |
| Parotid gland | |||
| DOPS IV | Assessment of the parotid gland | Sternocleidomastoid, masseter, posterior belly of digastric muscle, retromandibular vein, mandible | Visualisation of the retromandibular vein in transverse and sagittal section |
| Submandibular fossa | |||
| DOPS V | Assessment of the submandibular fossa | Submandibular gland, tonsils, tongue, mylohyoid | Measurement of the tonsils, with bilateral comparison |
| Item | Description | Participants | Examiners | P | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| DOPS—general aspects | ||||||
| D1 | Practical skills review | 6.4 | 0.9 | 6.5 | 0.7 | 0.95 |
| D2 | Review of theoretical knowledge | 5.8 | 1.1 | 5.1 | 1.2 | 0.08 |
| D3 | Differentiated performance assessment | 5.9 | 1.0 | 5.6 | 1.1 | 0.40 |
| D4 | Good educational tool | 6.1 | 1.2 | 5.8 | 1.0 | 0.21 |
| D5 | Use in any practical ultrasound course | 5.9 | 1.3 | 5.5 | 1.7 | 0.52 |
| D6 | Clear structure | 5.8 | 1.2 | 6.2 | 1.0 | 0.26 |
| D7 | Positive learning effect | 5.9 | 1.3 | 5.9 | 1.4 | 0.98 |
| D8 | Fair performance evaluation | 5.8 | 1.1 | 6.0 | 0.8 | 0.81 |
| D9 | Clinically relevant content and examination procedures | 6.2 | 0.9 | 6.3 | 0.7 | 0.88 |
| Test atmosphere | ||||||
| A1 | Appropriate use of time | 6.3 | 0.9 | 6.2 | 0.6 | 0.33 |
| A2 | Clear wording of instructions and notes | 6.3 | 0.8 | 6.2 | 0.8 | 0.5 |
| A3 | Sufficiently prepared for the test | 5.9 | 1.0 | 6.4 | 0.8 | 0.11 |
| A4 | Relaxed test atmosphere | 6.6 | 0.8 | 6.6 | 0.5 | 0.40 |
| Test tasks | ||||||
| T1 | Understandable tasks | 6.3 | 0.8 | 6.3 | 0.7 | 0.58 |
| T2 | Feasibility of tasks with sufficient preparation | 6.4 | 0.7 | 5.6 | 1.4 | 0.01 |
| T3 | Reasonable level of difficulty | 6.2 | 1.0 | 6.1 | 0.6 | 0.30 |
| T4 | DOPS I–V with comparable level of difficulty | 5.7 | 1.2 | 6.0 | 0.7 | 0.73 |
| T5 | Comprehensible expectations | 6.4 | 0.8 | 6.1 | 0.7 | 0.22 |
| T6 | Clear task definition | 6.2 | 1.0 | 5.9 | 0.7 | 0.11 |
| T7 | Ultrasound views | 6.3 | 0.8 | 5.9 | 0.9 | 0.12 |
| T8 | Case studies | 6.3 | 0.8 | 5.8 | 0.9 | 0.10 |
| T9 | Measurements/assessment tasks | 6.2 | 0.8 | 5.5 | 0.7 | 0.02 |
| T10 | Demonstration tasks | 6.3 | 0.8 | 6.2 | 0.8 | 0.061 |
| Special items for participants | ||||||
| P1 | Appropriate examiner communication | 6.8 | 0.5 | |||
| P2 | Patient consideration | 6.5 | 0.7 | |||
| P3 | Communication with patient | 6.5 | 0.7 | |||
| P4 | Personal strengths and weaknesses | 5.9 | 1.1 | |||
| P5 | Motivation to further improve/deepen skills | 6.1 | 1.1 | |||
| P6 | Role fulfilment of participant | 6.2 | 1.0 | |||
| Special items for the examiners | ||||||
| E1 | Comfortable in the role of the examiner | 6.1 | 0.9 | |||
| E2 | Evaluation sheet structure | 6.1 | 0.7 | |||
| E3 | Content evaluation sheet | 6.1 | 0.6 | |||
| E4 | Clarity of the evaluation scheme | 5.7 | 0.7 | |||
| E5 | Evaluation scheme for examination procedures | 5.9 | 1.0 | |||
| DOPS No. | |||||
|---|---|---|---|---|---|
| I | II | III | IV | V | |
| Subject | Thyroid | Cervical Vessels/Level | Floor of the Mouth | Parotid | Tonsillar Region |
| Total | 17 | 35 | 22 | 60 | 34 |
| Basic course | 12 | 22 | 17 | 55 | 29 |
| Advanced course | 5 | 13 | 5 | 5 | 5 |
| Total score, mean (SD) | 35.2 (1.4) | 31.4 (3.6) | 34.6 (2.7) | 32.0 (3.8) | 34.2 (2.9) |
| Subcategories, mean (SD) | |||||
| Patient management | 5.6 (0.6) | 5.7 (0.7) | 5.9 (0.4) | 5.7 (0.9) | 5.8 (0.7) |
| Transducer handling | 6.0 (0.0) | 5.4 (1.1) | 5.9 (0.2) | 5.5 (0.8) | 5.9 (0.5) |
| Image optimisation | 1.7 (0.5) | 1.7 (0.5) | 1.9 (0.4) | 1.5 (0.5) | 1.9 (0.4) |
| Examination course | 5.6 (0.6) | 4.9 (1.0) | 5.7 (0.6) | 5.1 (1.0) | 5.4 (1.3) |
| Measurements | 5.9 (0.5) | 4.0 (1.8) | 4.9 (1.5) | 4.5 (1.5) | 5.3 (1.1) |
| Image explanation | 5.0 (0.0) | 5.0 (0.0) | 5.0 (0.2) | 5.0 (0.12) | 5.0 (0.0) |
| Overall impression | 5.3 (0.6) | 4.7 (0.7) | 5.3 (0.8) | 4.9 (1.0) | 4.9 (0.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weimer, J.M.; Rink, M.; Müller, L.; Dirks, K.; Ille, C.; Bozzato, A.; Sproll, C.; Weimer, A.M.; Neubert, C.; Buggenhagen, H.; et al. Development and Integration of DOPS as Formative Tests in Head and Neck Ultrasound Education: Proof of Concept Study for Exploration of Perceptions. Diagnostics 2023, 13, 661. https://doi.org/10.3390/diagnostics13040661
Weimer JM, Rink M, Müller L, Dirks K, Ille C, Bozzato A, Sproll C, Weimer AM, Neubert C, Buggenhagen H, et al. Development and Integration of DOPS as Formative Tests in Head and Neck Ultrasound Education: Proof of Concept Study for Exploration of Perceptions. Diagnostics. 2023; 13(4):661. https://doi.org/10.3390/diagnostics13040661
Chicago/Turabian StyleWeimer, Johannes Matthias, Maximilian Rink, Lukas Müller, Klaus Dirks, Carlotta Ille, Alessandro Bozzato, Christoph Sproll, Andreas Michael Weimer, Christian Neubert, Holger Buggenhagen, and et al. 2023. "Development and Integration of DOPS as Formative Tests in Head and Neck Ultrasound Education: Proof of Concept Study for Exploration of Perceptions" Diagnostics 13, no. 4: 661. https://doi.org/10.3390/diagnostics13040661