
Hepatic Encephalopathy Confirmed by Magnetic Resonance Imaging in a Patient with Unobvious Cause of Chronic Liver Disease Decompensation

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
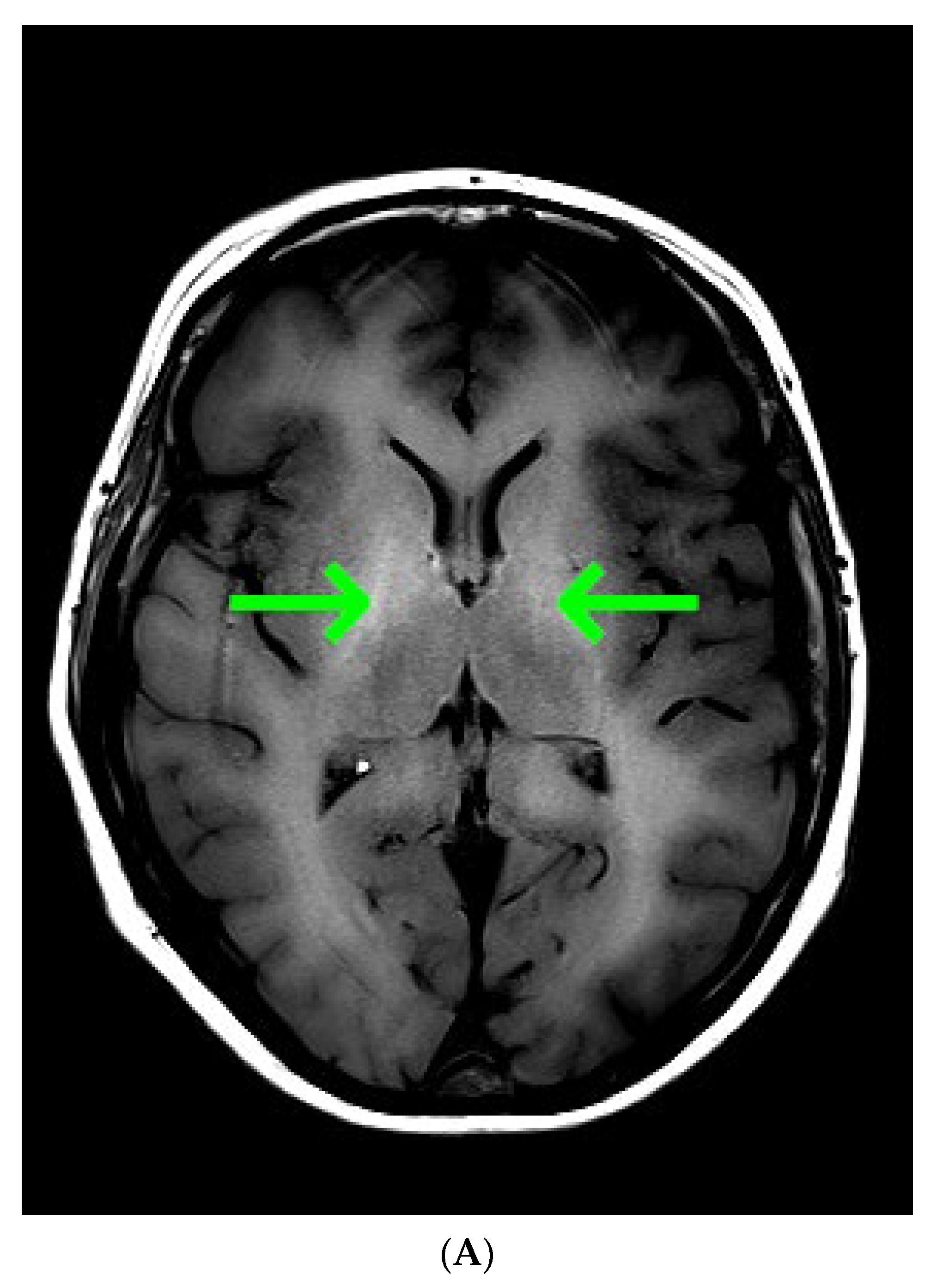
:1. Case Presentation
2. Differential Diagnosis of Impaired Consciousness
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013, 144, 1426–1437. [Google Scholar] [CrossRef] [PubMed]
- Bernal, W.; Hall, C.; Karvellas, C.J.; Auzinger, G.; Sizer, E.; Wendon, J. Arterial ammonia and clinical risk factors for encephalopathy and intracranial hypertension in acute liver failure. Hepatology 2007, 46, 1844–1852. [Google Scholar] [CrossRef] [PubMed]
- Aksan, F.; Andrade, C.; Hertan, H. Multiple Jejunal Intussusceptions in a Patient With Portal Hypertension and Decompensated Liver Cirrhosis. Am. J. Gastroenterol. 2021, 116, 1229–1230. [Google Scholar] [CrossRef]
- Behrooz, A.; Cleasby, M. Gastrogastric intussusception in adults: A case report with review of the literature. BJR Case Rep. 2018, 4, 20180006. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czempik, P.F.; Pluta, M.P.; Hofman, M.; Liberski, P.S.; Jaworski, T.; Szczepańska, A.; Bożek, O. Hepatic Encephalopathy Confirmed by Magnetic Resonance Imaging in a Patient with Unobvious Cause of Chronic Liver Disease Decompensation. Diagnostics 2023, 13, 753. https://doi.org/10.3390/diagnostics13040753
Czempik PF, Pluta MP, Hofman M, Liberski PS, Jaworski T, Szczepańska A, Bożek O. Hepatic Encephalopathy Confirmed by Magnetic Resonance Imaging in a Patient with Unobvious Cause of Chronic Liver Disease Decompensation. Diagnostics. 2023; 13(4):753. https://doi.org/10.3390/diagnostics13040753
Chicago/Turabian StyleCzempik, Piotr F., Michał P. Pluta, Mariusz Hofman, Piotr S. Liberski, Tomasz Jaworski, Anna Szczepańska, and Oskar Bożek. 2023. "Hepatic Encephalopathy Confirmed by Magnetic Resonance Imaging in a Patient with Unobvious Cause of Chronic Liver Disease Decompensation" Diagnostics 13, no. 4: 753. https://doi.org/10.3390/diagnostics13040753