

The Anthropometric Measurement of Nasal Landmark Locations by Digital 2D Photogrammetry Using the Convolutional Neural Network



Abstract
:1. Introduction
2. Materials and Methods
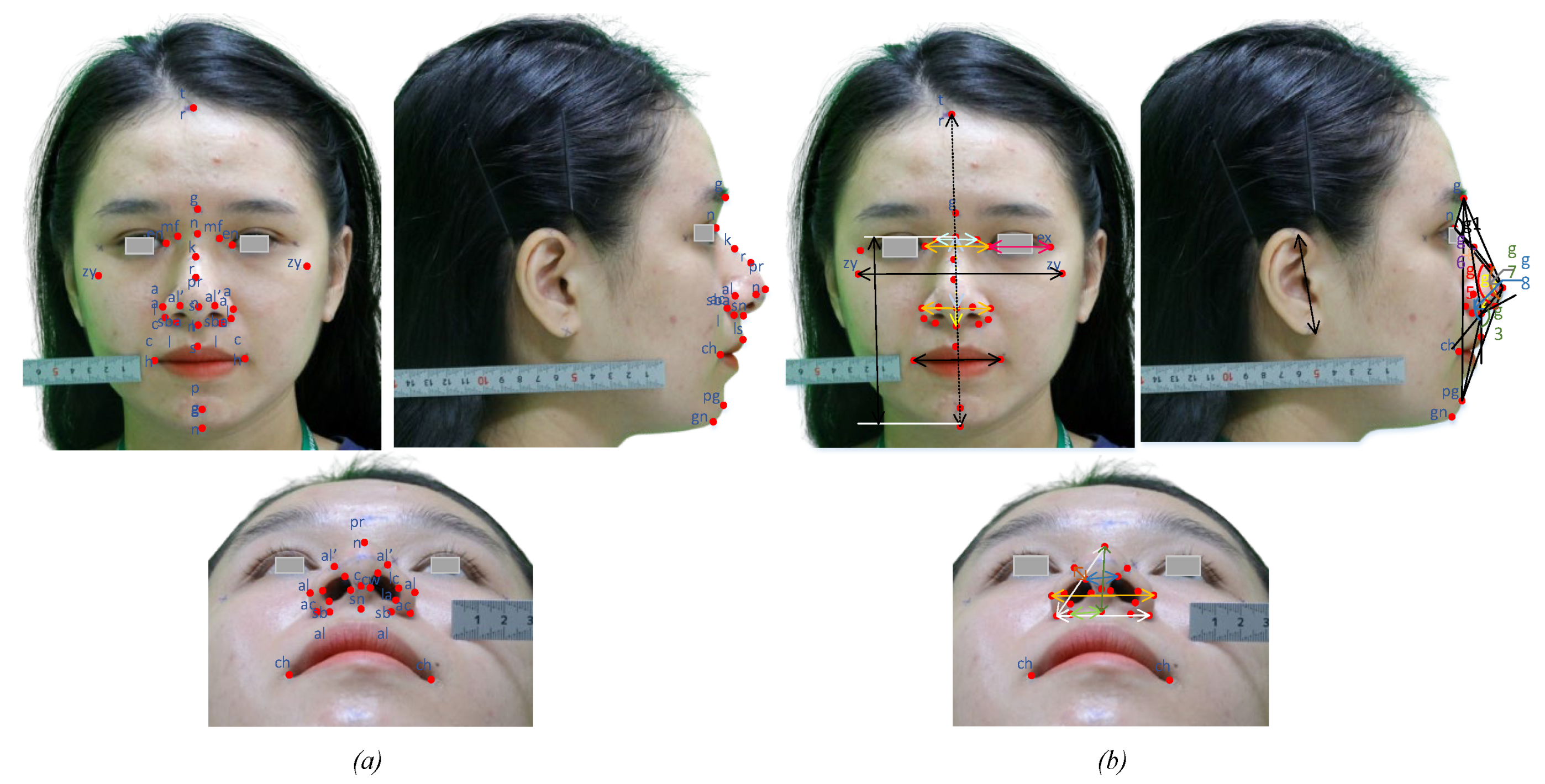
2.1. Nasal Landmarks and Anthropometric Measurements
2.2. Concept of the CNN Model for Determining the Location of Nasal Landmarks
2.2.1. Data and Pre-Processing
2.2.2. Automatic Anthropometric Measurements Based on Facial Landmarks
3. Results and Discussion
3.1. Dataset for Evaluation
3.2. Evaluation of the Accuracy of Landmark Extraction
3.3. Evaluation of the Accuracy of Anthropometric Measurements
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boddy, J. Re-thinking the zero tolerance approach to FGM/C: The debate around female genital cosmetic surgery. Curr. Sex. Health Rep. 2020, 12, 302–313. [Google Scholar] [CrossRef]
- Martin, S.; Long, R.; Hill, C.; Sinclair, S. Cosmetic tourism in Northern Ireland. Ann. Plast. Surg. 2019, 83, 618–621. [Google Scholar] [CrossRef] [PubMed]
- Busby, E.; Fattahi, T. Facial cosmetic surgery in male patients: Trends and experience from an academic esthetic oral-maxillofacial surgery practice. J. Oral Maxillofac. Surg. 2021, 79, 1922–1926. [Google Scholar] [CrossRef] [PubMed]
- Heider, N.; Spruyt, A.; De Houwer, J. Body dissatisfaction revisited: On the importance of implicit beliefs about actual and ideal body image. Psychol. Belg. 2018, 57, 158–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vries, D.A.; Vossen, H.G.M. Social media and body dissatisfaction: Investigating the attenuating role of positive parent–adolescent relationships. J. Youth Adolesc. 2019, 48, 527–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broer, P.N.M.; Juran, S.M.; Liu, Y.-J.; Weichman, K.; Tanna, N.M.; Walker, M.E.M.; Ng, R.M.; Persing, J.A. The impact of geographic, ethnic, and demographic dynamics on the perception of beauty. J. Craniofacial Surg. 2014, 25, e157–e161. [Google Scholar] [CrossRef]
- Yarosh, D.B. Perception and deception: Human beauty and the brain. Behav. Sci. 2019, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- Farkas, L.G.; Kolar, J.C.; Munro, I.R. Geography of the nose: A morphometric study. Aesthetic Plast. Surg. 1986, 10, 191–223. [Google Scholar] [CrossRef]
- Zucchini, S.; Brancatelli, S.; Piccinato, A.; Marcuzzo, A.V.; Bianchi, M.; Tirelli, G. Evaluation of surgical outcome in rhinoplasty: A comparison between rasp and osteotome in dorsal hump removal. Ear Nose Throat J. 2019, 100 (Suppl. S5), 436S–442S. [Google Scholar] [CrossRef] [Green Version]
- Piombino, P.; Zace, P.; Grassia, M.G.; Cataldo, R.; Marino, M.; De Riu, G.; Testa, D.; Bonavolontà, P.; Califano, L. Anthropometric parameters for nose evaluation and nasal surgery planning. J. Craniofacial Surg. 2020, 31, 1620–1624. [Google Scholar] [CrossRef]
- Suhk, J.; Park, J.; Nguyen, A.H. Nasal analysis and anatomy: Anthropometric proportional assessment in Asians—Aesthetic balance from forehead to chin, part I. In Seminars in Plastic Surgery; Thieme Medical Publishers: New York, NY, USA, 2015; Volume 29. [Google Scholar]
- Golpinar, M.; Nahir, M.; Ozdemir, F.; Sahin, B. Photographic Nasal Soft Tissue Analysis From Preadolescence to Young Adulthood: Anthropometric Measurements. J. Craniofacial Surg. 2021, 33, 575–578. [Google Scholar] [CrossRef] [PubMed]
- Yas, N.K. Anthropometric study on the nasofrontal angle in human skulls. J. Fac. Med. Baghdad 2012, 54, 106–109. [Google Scholar]
- Cao, Q.; Shen, L.; Xie, W.; Parkhi, O.M.; Zisserman, A. VGGFace2: A dataset for recognising faces across pose and age. In Proceedings of the 2018 13th IEEE International Conference on Automatic Face & Gesture Recognition, Xi’an, China, 15–19 May 2018. [Google Scholar]
- Jain, D.K.; Shamsolmoali, P.; Sehdev, P. Extended deep neural network for facial emotion recognition. Pattern Recognit. Lett. 2019, 120, 69–74. [Google Scholar] [CrossRef]
- Parkhi, O.M.; Vedaldi, A.; Zisserman, A. Deep Face Recognition; British Machine Vision Association: Durham, UK, 2015; pp. 1–12. [Google Scholar]
- AbdAlmageed, W.; Mirzaalian, H.; Guo, X.; Randolph, L.M.; Tanawattanacharoen, V.K.; Geffner, M.E.; Ross, H.M.; Kim, M.S. Assessment of Facial Morphologic Features in Patients With Congenital Adrenal Hyperplasia Using Deep Learning. JAMA Netw. Open 2020, 3, e2022199. [Google Scholar] [CrossRef] [PubMed]
- Peters, F.; Mücke, M.; Möhlhenrich, S.C.; Bock, A.; Stromps, J.-P.; Kniha, K.; Hölzle, F.; Modabber, A. Esthetic outcome after nasal reconstruction with paramedian forehead flap and bilobed flap. J. Plast. Reconstr. Aesthetic Surg. 2020, 74, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.-S.; Jo, K.-H.; Kim, J.-Y.; Kwon, J.-H. Comparing reliability between 3D imaging and 2D photography for external nasal anthropometry. Sci. Rep. 2022, 12, 4531. [Google Scholar] [CrossRef]
- Cohen, M.B.; HEzzat, W. Aesthetic facial analysis. In Sataloff’s Comprehensive Textbook of Otolaryngology: Head & Neck Surgery; Facial Plastic and Reconstructive Surgery 3: Lutherville, MD, USA, 2015; p. 101. [Google Scholar]
- Cummins, D.M.; Bishara, S.E.; Jakobsen, J.R. A computer assisted photogrammetric analysis of soft tissue changes after orthodontic treatment. Part I: Methodology and reliability. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 633–639. [Google Scholar]
- Lindner, C.; Tim, F.; Cootes, T. Fully automatic cephalometric evaluation using Random Forest regression-voting. In Proceedings of the IEEE International Symposium on Biomedical Imaging (ISBI), Brooklyn Bridge, NY, USA, 16–19 April 2015. [Google Scholar]
- Ibragimov, B.; Boštjan, L.; Pernus, F.; Tomaž Vrtovec, T. Computerized cephalometry by game theory with shape-and appearance-based landmark refinement. In Proceedings of the IEEE International Symposium on Biomedical Imaging (ISBI), Brooklyn Bridge, NY, USA, 16–19 April 2015. [Google Scholar]
- Arik, S.Ö.; Bulat, I.; Lei, X.T. Fully automated quantitative cephalometry using convolutional neural networks. J. Med. Imaging 2017, 4, 014501. [Google Scholar] [CrossRef]
- Lee, H.; Park, M.; Kim, J. Cephalometric landmark detection in dental x-ray images using convolutional neural networks. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis, Orlando, FL, USA, 3 March 2017. [Google Scholar]
- Qian, J.; Cheng, M.; Tao, Y.; Lin, J.; Lin, H. CephaNet: An Improved Faster R-CNN for Cephalometric Landmark Detection. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 868–871. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster r-cnn: Towards real-time object detection with region proposal networks. In Proceedings of the Advances in Neural Information Processing Systems (NIPS), Montreal, QC, Canada, 7–12 December 2015; pp. 91–99. [Google Scholar]
- Rao, G.K.L.; Srinivasa, A.C.; Iskandar, Y.H.P.; Mokhtar, N. Identification and analysis of photometric points on 2D facial images: A machine learning approach in orthodontics. Health Technol. 2019, 9, 715–724. [Google Scholar] [CrossRef]
- Sohail, A.S.M.; Bhattacharya, P. Detection of facial feature points using anthropometric face model. In Signal Processing for Image Enhancement and Multimedia Processing; Springer: Boston, MA, USA, 2008; pp. 189–200. [Google Scholar]
- Farkas, L.G.; Posnick, J.C.; Hreczko, T. Anthropometry of the Head and Face, 2nd ed.; Raven: New York, NY, USA, 1994. [Google Scholar]
- Deutsch, C.K.; Shell, A.R.; Francis, R.W.; Bird, B.D. The Farkas system of craniofacial anthropometry: Methodology and normative databases. In Handbook of Anthropometry; Springer: New York, NY, USA, 2012; pp. 561–573. [Google Scholar]
- Sforza, C.; Elamin, F.; Rosati, R.; Lucchini, M.A.; Tommasi, D.G.; Ferrario, V.F. Three-dimensional assessment of nose and lip morphology in North Sudanese subjects with Down syndrome. Angle Orthod. 2011, 81, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.; Okada, K.; Rosenbaum, K.; Kehoe, L.; Zand, D.J.; Sze, R.; Summar, M.; Linguraru, M.G. Digital facial dysmorphology for genetic screening: Hierarchical constrained local model using ICA. Med. Image Anal. 2014, 18, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Lazovic, G.D.; Daniel, R.K.; Janosevic, L.B.; Kosanovic, R.M.; Colic, M.M.; Kosins, A.M. Rhinoplasty: The nasal bones–anatomy and analysis. Aesthetic Surg. J. 2015, 35, 255–263. [Google Scholar] [CrossRef] [PubMed]
- He, Z.-J.; Jian, X.-C.; Wu, X.-S.; Gao, X.; Zhou, S.-H.; Zhong, X.-H. Anthropometric measurement and analysis of the external nasal soft tissue in 119 young Han Chinese adults. J. Craniofacial Surg. 2009, 20, 1347–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, T.T.; Farkas, L.G.; Ngim, R.C.; Levin, L.S.; Forrest, C.R. Proportionality in Asian and North American Caucasian faces using neoclassical facial canons as criteria. Aesthetic Plast. Surg. 2002, 26, 64–69. [Google Scholar] [CrossRef]
- Porter, J.P.; Olson, K.L. Anthropometric facial analysis of the African American woman. Arch. Facial Plast. Surg. 2001, 3, 191–197. [Google Scholar] [CrossRef]
- Lindemann, J.; Stupp, F.; Scheithauer, M.; Schmadl, A.; Goldberg-Bockhorn, E.; Halbig, A.-S.; Hoffmann, T.K.; Sommer, F. Anthropometric evaluation of photographic images before and after functional nasal surgery in patients with deviated noses. Am. J. Rhinol. Allergy 2021, 35, 615–623. [Google Scholar] [CrossRef]
- Sotnik, S.; Lyashenko, V. Overview of Innovative Walking Robots. Int. J. Acad. Eng. Res. (IJAER) 2022, 6, 3–7. [Google Scholar]
- Albawi, S.; Mohammed, T.A.; Al-Zawi, S. Understanding of a convolutional neural network. In Proceedings of the 2017 International Conference on Engineering and Technology (ICET), Antalya, Turkey, 21–23 August 2017; pp. 1–6. [Google Scholar]
- Minh Trieu, N.; Thinh, N.T. Quality Classification of Dragon Fruits Based on External Performance Using a Convolutional Neural Network. Appl. Sci. 2021, 11, 10558. [Google Scholar] [CrossRef]
- Shugar, A.N.; Drake, B.L.; Kelley, G. Rapid identification of wood species using XRF and neural network machine learning. Sci. Rep. 2021, 11, 17533. [Google Scholar] [CrossRef]
- Li, H.; Jin, Y.; Zhong, J.; Zhao, R. A Fruit Tree Disease Diagnosis Model Based on Stacking Ensemble Learning. Complexity 2021, 2021, 6868592. [Google Scholar] [CrossRef]
- Sadiq, M.; Shi, D. Attentive occlusion-adaptive deep network for facial landmark detection. Pattern Recognit. 2022, 125, 108510. [Google Scholar] [CrossRef]
- Liu, Y.; Shen, H.; Si, Y.; Wang, X.; Zhu, X.; Shi, H.; Hong, Z.; Guo, H.; Guo, Z.; Chen, Y.; et al. Grand challenge of 106-point facial landmark localization. In Proceedings of the 2019 IEEE International Conference on Multimedia & Expo Workshops (ICMEW), Shanghai, China, 8–12 July 2019; pp. 613–616. [Google Scholar]
- Lin, Q.; He, R.; Jiang, P. Feature Guided CNN for Baby’s Facial Expression Recognition. Complexity 2020, 2020, 8855885. [Google Scholar] [CrossRef]
- Russo, F. A method for estimation and filtering of Gaussian noise in images. IEEE Trans. Instrum. Meas. 2003, 52, 1148–1154. [Google Scholar] [CrossRef]
- Park, J.; Byun, S.-C.; Lee, B.-U. Lens distortion correction using ideal image coordinates. IEEE Trans. Consum. Electron. 2009, 55, 987–991. [Google Scholar] [CrossRef]
- Vu, N.H.; Trieu, N.M.; Tuan, H.N.A.; Khoa, T.D.; Thinh, N.T. Review: Facial Anthropometric, Landmark Extraction, and Nasal Reconstruction Technology. Appl. Sci. 2022, 12, 9548. [Google Scholar] [CrossRef]
- Tuan, H.N.A.; Hai, N.D.X.; Thinh, N.T. Shape Prediction of Nasal Bones by Digital 2D-Photogrammetry of the Nose Based on Convolution and Back-Propagation Neural Network. Comput. Math. Methods Med. 2022, 2022, 5938493. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Landmark | Symbol | Number | Landmark | Symbol |
|---|---|---|---|---|---|
| 1 | Trichion | tr | 13 | Labiale superius | ls |
| 2 | Glabella | g | 14 | Pogonion | pg |
| 3 | Nasion | n | 15 | Zygion | zy |
| 4 | Endocanthion | en | 16 | Maxillofrontale | mf |
| 5 | Exocanthion | ex | 17 | Subalare | sbal |
| 6 | Pronasale | prn | 18 | Columellar peak | c |
| 7 | Kyphion | k | 19 | Columellar waist | cw |
| 8 | Rhinion | r | 20 | Lateral crus | lc |
| 9 | Subnasale | sn | 21 | Lateral alar | la |
| 10 | Alare | al | 22 | Soft triangle | c’ |
| 11 | Alare’ | al’ | 23 | Cheilion | ch |
| 12 | Alar curvature | ac |
| Symbol | Measurements | Distance |
|---|---|---|
| d1 | Nasal root | mf–mf |
| d2 | Nasal height | n–sn |
| d3 | Nasal length | n–prn |
| d4 | Nasal tip protrusion | sn–prn |
| d5 | Nasal width | al–al |
| d6 | Anatomical width | ac–ac |
| d7 | Inter canthal width | en–en |
| d8 | Ala length | ac–prn |
| d9 | Nostril floor width | sbal–sn |
| d10 | Columella width | c’–c’ |
| d11 | Superior width of the columella | cw–cw |
| d12 | Ala thickness | al’–c’ |
| Symbol | Name | Angle | |
|---|---|---|---|
| g1 | Lateral view | Nasofrontal | g–n–prn |
| g2 | Nasomental | n–prn–pg | |
| g3 | Facial convexity | g–sn–pg | |
| g4 | Nasal tip | n–prn–sn | |
| g5 | Nasolabial | c–sn–ls | |
| g6 | Nasofacial | n–prn and g–pg | |
| g7 | Kyphion | n–k–r | |
| g8 | Mental view | Alar slope | al–prn–al |
| g9 | Interaxial | nostril axis-nostril axis | |
| g10 | Nostril axis | nostril axis-horizontal plane |
| Standard | Symbol | |
|---|---|---|
| 1 | Orbitonasal Canon | en–en = al–al |
| 2 | Orbital Canon | en–en = ex–en |
| 3 | Naso-oral Canon | ch–ch = 1.5 (al–al) |
| 4 | Nasofacial Canon | al–al = 0.25 (zy–zy) |
| 5 | Threesection Facial Profile Canon | n–sn = 1/3 (tr–gn) |
| 6 | Nose Height Equal to Ear Length | n–sn = sa–sba |
| 7 | Nose height approx. 0.43 (n–gn) | n–sn = 0.43(n–gn) |
| 8 | Distance of the corner of the mouth to nasal alare of equal distance to the corner of the mouth to the center of the pupil | ch–en = ch–center (pupil) (Horizontally) |
| Characteristic | Training Dataset | Evaluation Dataset |
|---|---|---|
| Number of participants | n = 1000 | n = 203 |
| Number of Images | 3000 | 609 |
| Male | 152 | 78 |
| Female | 848 | 125 |
| Age | 28.09 ± 12.32 | 23.09 ± 12.32 |
| Failure Rate (%) | NME (%) | |
|---|---|---|
| Z. Hong et al. [44] | 0.1 | 1.31 |
| Our | 0.00 | 1.05 |
| Layers | Filter Numbers | Filter Size | Stride |
|---|---|---|---|
| Conv2d_1 | 32 | 5 × 5 | 1 |
| Conv2d_2 | 32 | 3 × 3 | 1 |
| Conv2d_3 | 64 | 3 × 3 | 1 |
| Conv2d_4 | 64 | 3 × 3 | 1 |
| Conv2d_5 | 128 | 3 × 3 | 1 |
| Conv2d_6 | 256 | 3 × 3 | 1 |
| All pooling layer | - | 2 × 2 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minh Trieu, N.; Truong Thinh, N. The Anthropometric Measurement of Nasal Landmark Locations by Digital 2D Photogrammetry Using the Convolutional Neural Network. Diagnostics 2023, 13, 891. https://doi.org/10.3390/diagnostics13050891
Minh Trieu N, Truong Thinh N. The Anthropometric Measurement of Nasal Landmark Locations by Digital 2D Photogrammetry Using the Convolutional Neural Network. Diagnostics. 2023; 13(5):891. https://doi.org/10.3390/diagnostics13050891
Chicago/Turabian StyleMinh Trieu, Nguyen, and Nguyen Truong Thinh. 2023. "The Anthropometric Measurement of Nasal Landmark Locations by Digital 2D Photogrammetry Using the Convolutional Neural Network" Diagnostics 13, no. 5: 891. https://doi.org/10.3390/diagnostics13050891