Abstract
Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) is useful for the diagnosis of pancreatic masses. According to three meta-analyses, the sensitivity, specificity, and accuracy of EUS-FNA are 84–92%, 96–98%, and 86–91%, respectively. However, the occurrence of false-negative and false-positive results indicates that the diagnostic performance of EUS-FNA needs to be improved. Contrast-enhanced harmonic endoscopic ultrasonography (CH-EUS) is used for the characterization of pancreatic masses and can be applied to improve the performance of EUS-FNA. When CH-EUS is used to evaluate intratumor blood flow, an avascular area inside the pancreatic mass that is considered to be fibrosis is often detected. This area can be avoided by performing EUS-FNA under CH-EUS guidance. In this review, we summarize the data on contrast-enhanced harmonic endoscopic ultrasound-guided fine-needle aspiration (CH-EUS-FNA), which suggest that its benefit is still a matter of debate. Of eight studies analyzed, only one showed that CH-EUS improved the sensitivity of EUS-FNA. The future challenge is to determine under what circumstances CH-EUS-FNA is useful.
1. Introduction
Endoscopic ultrasonography (EUS) allows detailed visualization of the pancreas and the localization of pancreatic solid masses. Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) was first applied clinically by Vilmann et al. in 1992 [1], and is currently widely used for the pathological diagnosis of pancreatic solid masses. According to three meta-analyses evaluating the diagnostic performance of EUS-FNA for pancreatic masses, its sensitivity, specificity, and accuracy range between 84–92%, 96–98%, and 86–91%, respectively [2]. Thus, EUS-FNA is associated with a few false-negative and false-positive results. Contrast-enhanced harmonic endoscopic ultrasonography (CH-EUS) allows the visualization of intratumor blood flow using an ultrasound contrast agent, such as Perflubutane microspheres, and is applied for the identification and characterization of pancreatobiliary masses [3,4]. Although EUS-FNA is usually performed under EUS guidance, CH-EUS can be used to guide the needle to a specific site in the tumor to improve specimen collection. In this review, we summarize the literature on the methods and implications of contrast-enhanced harmonic endoscopic ultrasound-guided fine-needle aspiration (CH-EUS-FNA), and discuss the potential of CH-EUS-FNA for improving the diagnostic performance of EUS-FNA in patients with pancreatic cancer. In recent years, the efficacy of ultrasound contrast agents has been reported in regards to procedures such as endoscopic ultrasound-guided biliary drainage (EUS-BD) utilizing EUS. The effectiveness of ultrasound contrast agents in EUS-related procedures will also be reviewed.
2. The CH-EUS-FNA Technique
In selecting the literature, the following search terms were used in PubMed: contrast (title or abstract) OR contrast-enhanced (title or abstract) OR contrast-enhanced harmonic (title or abstract) OR CE-EUS (title or abstract) OR CH-EUS (title or abstract) OR CEH-EUS (title or abstract) AND endoscopic ultrasound (title or abstract) OR EUS (title or abstract) OR endosonography (title or abstract or MeSH terms) OR endoscopic ultrasonography (title or abstract) AND FNA (title or abstract) OR FNB (title or abstract) OR fine needle aspiration (title or abstract) OR fine needle biopsy (title or abstract) OR sampling (title or abstract). Then, after sequential screening of abstracts and texts, eight studies were determined as shown in Table 1 [5,6,7,8,9,10,11,12]. In most studies, CH-EUS-FNA was performed in the late phase of CH-EUS (Table 1), suggesting that CH-EUS-FNA was performed after evaluation of blood flow in the pancreatic mass in late-phase CH-EUS. However, in one study, CH-EUS-FNA was performed in the early arterial phase [12].

Table 1.
Studies on CH-EUS-FNA for pancreatic masses.
A prolonged contrast period is important for EUS-FNA, which normally requires more than two passes. Second-generation ultrasound contrast agents such as Sulphur hexafluoride microbubbles, Perflutren lipid microspheres, and Perflubutane microspheres resonate under low acoustic power and generate a second harmonic component, which provides at least several minutes of contrast effect [13,14]. Unlike other contrast medias, perflubutane microspheres have the advantage of obtaining a Kupffer image. Perflubutane microspheres allow contrast-enhanced ultrasound evaluations at early phase, late phase, and Kupffer phase. The early, late, and Kupffer phases are defined as 10–30 s, 30–120 s, and 10 min after injection of the contrast agent, respectively [15]. There are no Kupffer cells in the pancreas; therefore, early and late phases are used for CH-EUS evaluations for pancreatic lesions and the significance of this advantage in the diagnosis of pancreatic tumors is not presently known. Thus, any second-generation ultrasound contrast agents can be used for the diagnosis of pancreatic tumors. In EUS-FNA, the fanning technique (sampling multiple areas with each needle pass) is recommended to obtain tumor tissue from a hot spot [16]. However, CH-EUS-FNA has the advantage that any avascular area can be avoided and the fanning technique is not always applicable. It remains unclear whether the early or late phase of CH-EUS is more appropriate for identifying the avascular area, with only one study showing that the diagnostic sensitivity of CH-EUS-FNA performed in the early phase was better than that of conventional EUS-FNA (Table 1). Nevertheless, the endosonographers are required to observe both the early and late phases for comprehensive assessment in actual clinical practice: the contrast effect of both phased should be taken into consideration when determining the portion of pancreatic masses to undergo EUS-FNA.
3. Avascular Areas on CH-EUS
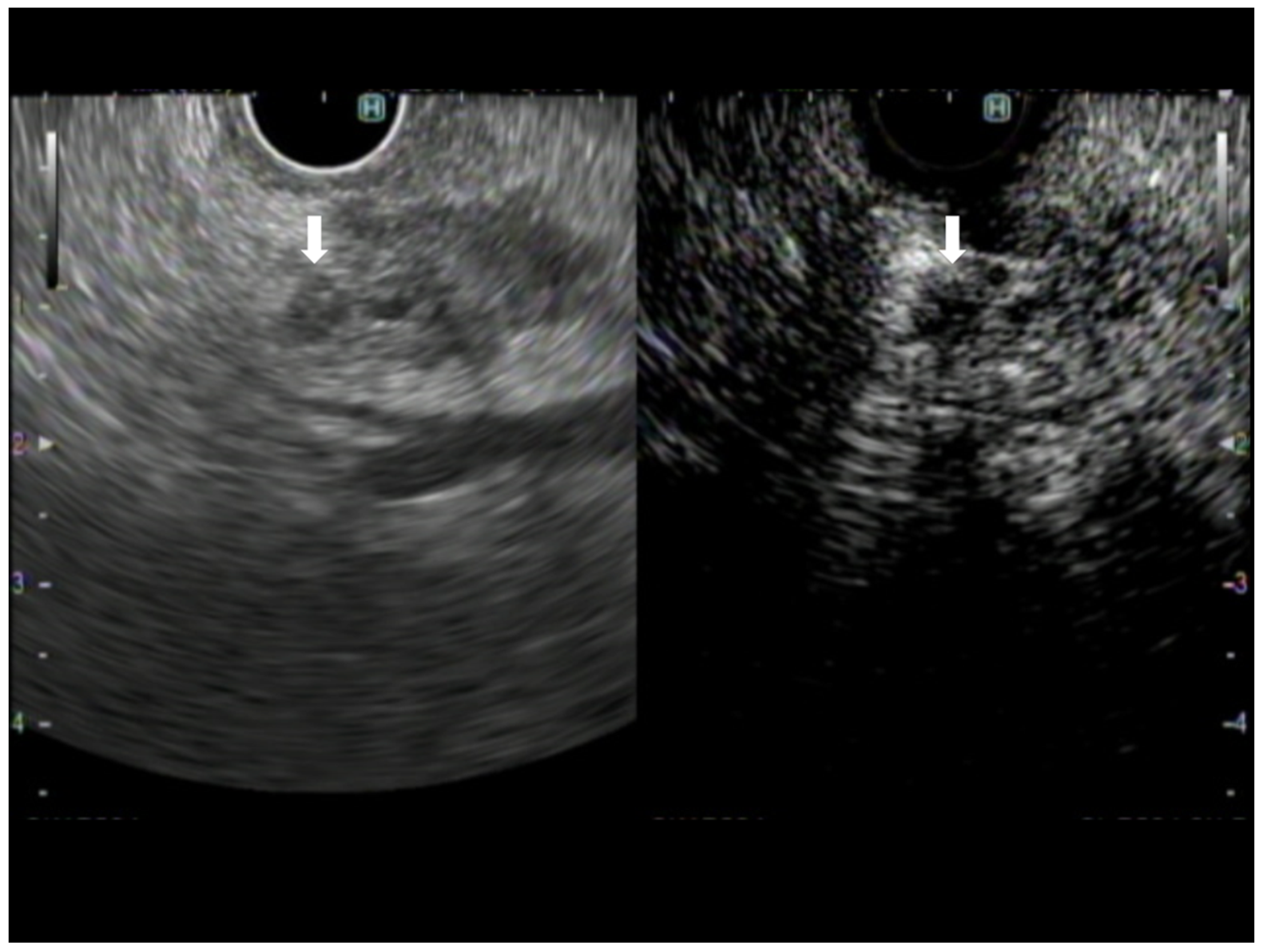
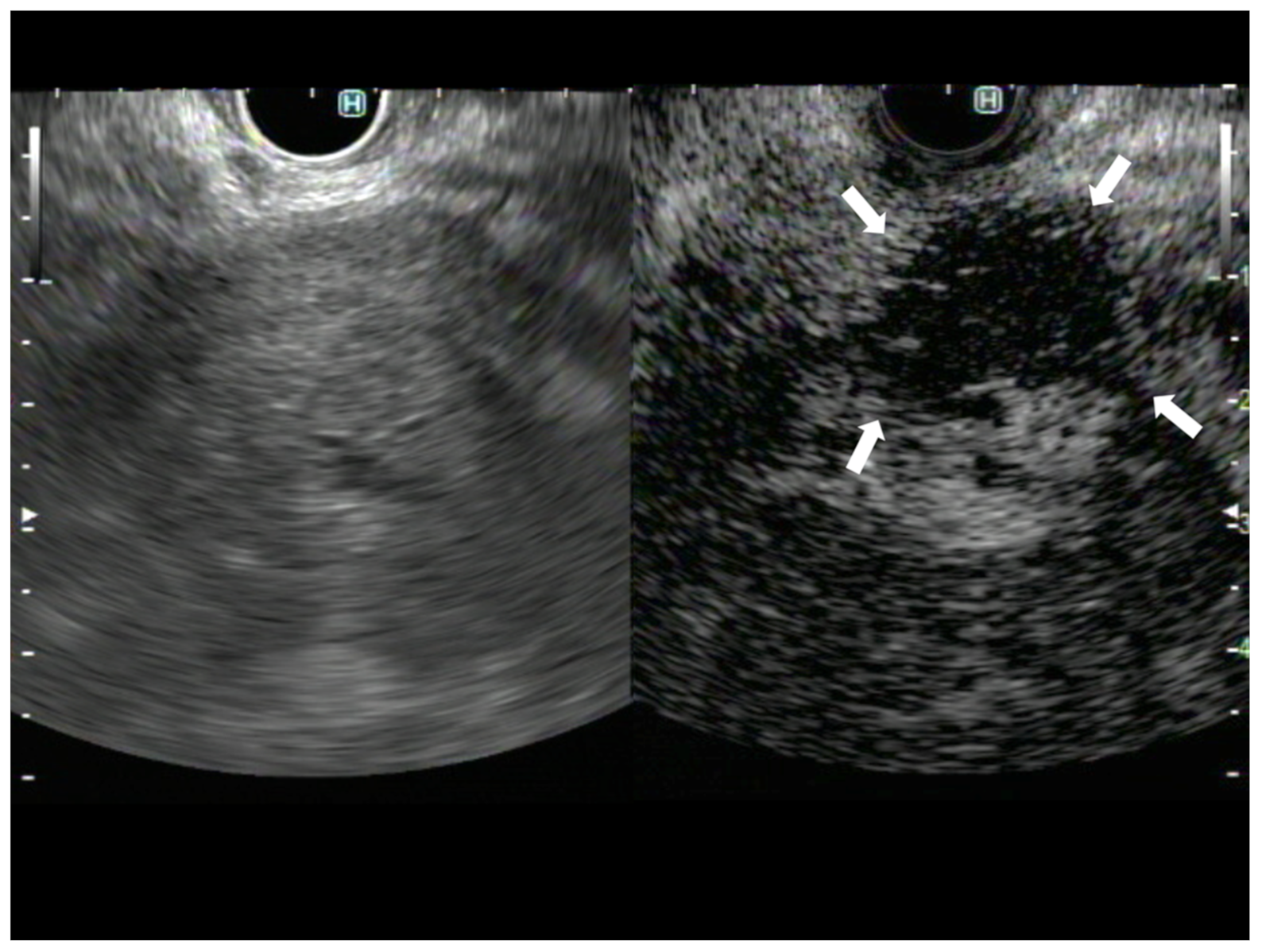
Although EUS can detect pancreatic lesions, it is not accurate for the differential diagnosis of pancreatic masses. However, CH-EUS can characterize pancreatic masses by comparing the enhancement between solid pancreatic lesions and surrounding pancreatic tissues [6,17,18]. Four contrast patterns of internal blood flow define pancreatic solid lesions: iso-enhancement in mass-forming pancreatitis, hypo-enhancement in pancreatic adenocarcinoma, hyperenhancement in pancreatic neuroendocrine tumors, and nonenhancement in necrosis [4]. The typical CH-EUS image of pancreatic cancer is characterized by hypo-enhancement of most of the tumor, with a non-enhancing area (i.e., an avascular area) detected in part of the tumor. Numata et al. compared transabdominal contrast-enhanced ultrasound images of pancreatic cancer with pathological images of resected specimens and found that tumors with poor contrast enhancement contained a greater number of necrotic and fibrotic cells [19]. Furthermore, it is known that pancreatic neuroendocrine neoplasms with hypo-enhancement on CH-EUS have lower vessel density and greater fibrosis [20]. These reports also support the idea that CH-EUS-FNA helps to puncture hot spots in the tumor. Kamata et al. reported that the sensitivity of EUS-FNA for the diagnosis of pancreatic adenocarcinoma was significantly lower in cases with avascular areas than in those without (72.9% vs. 94.3%) [21]. One case report showed that EUS-FNA specimens from the avascular area were not suitable for detecting malignancy, whereas specimens obtained from the vascular area showed malignant findings [22]. In this report, EUS-FNA samples obtained from the avascular area was necrosis by pathological evaluations. This suggests that the avascular area on CH-EUS represents mostly necrotic or fibrotic tissue, and CH-EUS-FNA can help avoid this area. In certain cases, an avascular area on CH-EUS is recognized on normal EUS as an area within the tumor that is hypoechoic compared with the surrounding lesion (Figure 1). However, avascular areas identified on CH-EUS may often not be detected on normal EUS (Figure 2). A difference in the degree of echogenicity within the tumor on EUS is not necessarily identified as an avascular area on CH-EUS. Thus, the area imaged as the avascular area in CH-EUS may be an inappropriate specimen. Therefore, in order to obtain an appropriate specimen for diagnosis, it is necessary to puncture the area, avoiding the avascular area. Although no reports specifically describe the technique to avoid the avascular area during CH-EUS-FNA, it would be better to puncture the areas with blood flow in the tumor, changing the angle of the EUS-FNA needle using forceps to raise up or down the angle of the endoscopy.
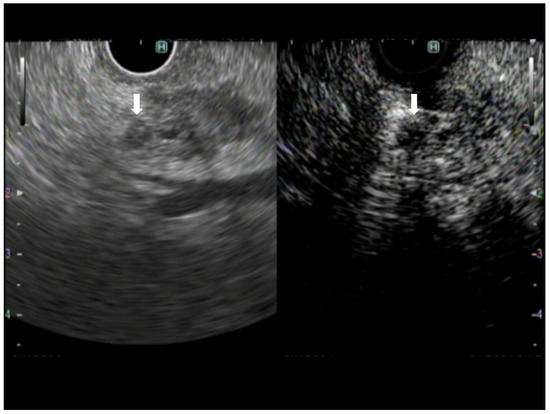
Figure 1.
A case of pancreatic adenocarcinoma. The image on the left shows B-mode EUS, and the image on the right shows CH-EUS. The avascular area observed in the CH-EUS image is recognized on B-mode EUS as a hypoechoic area compared with the surrounding lesion within the tumor (arrow).
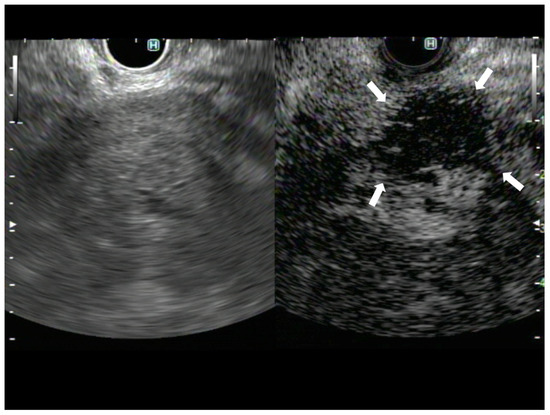
Figure 2.
A case of pancreatic adenocarcinoma. The image on the left shows B-mode EUS, and the image on the right shows CH-EUS. The avascular area observed in the CH-EUS image was not identified on B-mode EUS (arrows).
4. Diagnostic Capability of CH-EUS-FNA
Three meta-analyses that included a large number of studies reported that CH-EUS shows superior performance for the diagnosis of solid masses [14,23,24]. Eight reports evaluated the pathological diagnostic performance of CH-EUS-FNA for pancreatic masses (Table 1) [5,6,7,8,9,10,11,12], with these including six prospective studies and two retrospective ones, although two of the prospective studies were single-arm designs. The number of patients in these studies ranged from 35 to 225. Most studies did not describe the number of cases with avascular areas, but Sugimoto et al. reported that 20 consecutive cases evaluated with CH-EUS-FNA had avascular areas, and Itonaga et al. reported that 41.5% (34/93) of cases had an avascular area. However, the definition of avascular area was ambiguous in these two studies. Previously, Kamata et al. defined tumors with an avascular area as those with a non-enhancing area ≥5 mm on CH-EUS, and reported that 16.4% (48/292) of pancreatic masses had an avascular area [21]. The variation in the proportion of cases with an avascular area could be due to differences in the definition. In the eight studies listed in Table 1, CH-EUS-FNA was performed by expert endosonographers using a 22-gauge EUS-FNA needle, whereas data obtained using an EUS-fine needle biopsy (FNB) needle are lacking. Regarding the puncture site, most studies reported avoiding avascular areas, and three studies reported detecting a hypo-enhanced area. Puncturing the hypo-enhanced area, which indicates pancreatic cancer, is reasonable, especially in pancreatic masses without an avascular area. Two prospective studies (Napoleon et al., 2010 and Gincul et al., 2014) demonstrated the feasibility of CH-EUS-FNA in a single-arm study [5,6], whereas six studies compared the diagnostic accuracy of CH-EUS-FNA and EUS-FNA. Among these studies, two performed both CH-EUS-FNA and EUS-FNA in the same patients (Seicean et al., 2015 and Itonaga et al., 2020) [9,12]. The sensitivity of CH-EUS-FNA ranged from 79% to 96%, and its specificity from 90% to 100%. Six studies showed that the sensitivity of CH-EUS-FNA was higher than that of EUS-FNA, but only one study showed that the difference was significant (p = 0.003; Table 1). However, in this study showing a significant difference, the sensitivity of normal EUS-FNA was particularly low at 68.8%, which could be attributed to the fact that a single pass was used to compare the diagnostic performance of the two methods, rather than the multiple passes used in other studies. Moreover, the first pass was performed using EUS-FNA and the second pass using early-phase CH-EUS with the avascular area confirmed. The specimen obtained by single pass was used for evaluation, and EUS-FNA was performed prior to CH-EUS-FNA. In summary, the added value of CH-EUS-FNA in comparison with EUS-FNA remains unclear, and further studies are needed.
The precision of EUS-FNA is considered to be contingent upon the proficiency of the endosonographers. Additionally, the assessment of pancreatic lesions through CH-EUS and the detection of the avascular area are also subject to their examination skills. Thus, standardization of the procedures and diagnostic proficiency is imperative to gauge the impact of ultrasound contrast agents in CH-EUS. In addition, improvements in examination equipment such as endoscopes and EUS-FNA needles may also have an impact on CH-EUS-FNA in the future.
5. Detection of Subtle Lesions
In some cases, CH-EUS depicts pancreatic tumors that are difficult to identify on normal EUS. This may be due to the fact that the contrast effect achieves clearer margins to pancreatic tumors.
Kitano et al. performed CH-EUS on 277 patients with pancreatic tumors, and among them, six cases of ductal carcinoma were depicted on CH-EUS but not on EUS [18]. Kamata et al. evaluated the utility of CH-EUS for the surveillance of remnant pancreas after surgery for intraductal papillary mucinous neoplasm (IPMN) [25]. One hundred and thirty-four patients were followed-up for a median of 29 months, and CH-EUS was useful to identify two cases of small IPMN concomitant with pancreatic ductal adenocarcinoma that developed during the follow-up period. Fusaroli et al. also mentioned that CH-EUS was useful for detecting pancreatic masses, especially in patients with a bile duct stent or chronic pancreatitis [17].
Thus, there are some pancreatic masses that are detected only on CH-EUS, and not on ordinary EUS. The prognosis for advanced pancreatic cancer is poor, and early detection and treatment are critical. Given the difficulty in detecting certain lesions through ordinary EUS, it is also important to conduct a comprehensive screening of the pancreas using CH-EUS rather than just limiting the examination to lesions that are detectable through ordinary EUS.
CH-EUS also allows for clearer imaging of the tumor margins of lesions, which leads to reliable puncture of the tumor on EUS-FNA.
6. Risks Related to CH-EUS-FNA
There are few risks associated with the use of ultrasound contrast agents or performing EUS-FNA under CH-EUS guidance. The color Doppler mode is generally used to identify vessels on the puncture line during EUS-FNA, although this method is often limited by blooming artifact [26]. There are no reports indicating that EUS-FNA with CH-EUS guidance increases the incidence of adverse events; however, it is more difficult to identify vessels using CH-EUS than using color Doppler mode. If CH-EUS detects a pancreatic mass without an avascular area, it might be possible to switch to normal EUS-FNA. The blooming artifact associated with the color Doppler mode occurs more frequently after the administration of ultrasound contrast medium. Another limitation of CH-EUS-FNA is that the tip of the EUS-FNA needle can be difficult to visualize in deep areas away from the EUS probe. The side effects of the ultrasound contrast medium are rarely a clinical problem [27,28]; mild allergy-like symptoms can occur, but there are no reports of serious events [27,28].
7. Future Perspectives
Although several studies have described the utility of CH-EUS-FNA, only one study demonstrated the value of CH-EUS-FNA for improving diagnostic performance. It is therefore important to clarify the specific cases that would benefit from CH-EUS-FNA.
CH-EUS-FNA may be particularly valuable in cases in which it is difficult to obtain an accurate diagnosis—for example, in cases in which EUS-FNA is performed with a small-gauge needle, by beginners, or using a single puncture. Recently developed EUS-FNB needles, such as fork-tip or shark-core needles, have improved the quality and quantity of pancreatic specimens collected [29,30], and improvements in the diagnostic performance of EUS-FNA may decrease the impact of CH-EUS guidance for EUS-FNA in the future. However, precision medicine is attracting increased attention, and the ability to perform oncogene panel testing on EUS-FNA specimens is essential [31]. For such testing, it is important to collect cancer tissues from a site with a high cell count. In this sense, CH-EUS-FNA is still expected to play an important role in pancreatic cancer tissue collection.
Pancreatic cancer is likely to metastasize to the lymph nodes and its staging depends on the presence of lymph node metastasis [32]. However, the correct diagnosis of lymph node metastases remains challenging [33]. Kurita et al. compared the diagnostic performance of EUS-FNA and PET-CT for para-aortic lymph node metastasis in pancreatobiliary cancer [34]. Fifty-two patients had enlarged para-aortic lymph nodes, and postoperative diagnosis of lymph node metastasis was made in 21 patients (40.4%). In this study, EUS-FNA showed superior accuracy to PET-CT in the diagnosis of malignancy in lymph nodes (95.2% vs. 57.1%).
If there are many enlarged lymph nodes, it is hard to perform EUS-FNA on all of them in clinical practice. Therefore, it is useful to estimate the malignancy of enlarged lymph nodes by CH-EUS in order to determine the optimum target for EUS-FNA.
Miyata et al. examined enlarged intra-abdominal lymph nodes associated with pancreatobiliary cancers in 143 patients. Heterogeneous enhancement on CH-EUS was a sign of malignancy, and CH-EUS had a sensitivity of 83% and specificity of 91% [35]. Recently, a meta-analysis including 336 cases in four studies showed that CH-EUS had a sensitivity of 82.1% and specificity of 90.7% for diagnosing malignant lymph nodes [36].
In recent years, EUS-BD has become a popular method of bile duct drainage. Several cases were reported in which CH-EUS improved the visibility of bile ducts that were poorly viewed on normal EUS because of debris or sludge during EUS-BD procedures [37,38].
Minaga et al. also mentioned that CH-EUS was helpful for EUS-guided cyst drainage for pancreatic pseudocyst or walled-off necrosis (WON) [39]. CH-EUS allows for real-time evaluation of blood flow and can assist in distinguishing WON from other luminal organs, which leads to a safer procedure in EUS-guided drainage.
The utilization and development of artificial intelligence (AI) in the medical field is ongoing. Numerous studies examining the diagnostic efficacy of AI in ordinary EUS for pancreatic cancer have yielded favorable outcomes [40,41,42,43]. AI-based examination of CH-EUS images also has been explored, although not applied to the analysis of pancreatic lesions. Tanaka et al. applied AI to differentiate gastrointestinal stromal tumors and leiomyomas in the identification of gastric submucosal tumors, yielding favorable results [44]. If AI could accurately differentiate gastric submucosal tumors through CH-EUS, it is within the realm of possibility that it could also distinguish pancreatic masses. Research on AI-based analysis and diagnosis of CH-EUS images for pancreatic lesions is also expected to advance in the future.
Thus, CH-EUS might be useful for performing EUS-FNA or EUS-guided drainage for pancreaticobiliary lesions, and further research including large-scale randomized clinical trials is desired. As mentioned above, there are few side effects associated with ultrasound contrast agents, and the benefits might far exceed the risks. In addition, the administration is easy because an intravenous route for sedation is generally secured during EUS examinations. Nevertheless, CH-EUS is still not covered by insurance in any of the regions, and CH-EUS is not allowed to be performed in general practice. Further evidence on the usefulness of CH-EUS is needed to achieve insurance approval for CH-EUS.
Author Contributions
Y.O. drafted the manuscript. K.K. and M.K. reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vilmann, P.; Jacobsen, G.K.; Henriksen, F.W.; Hancke, S. Endoscopic ultrasonography with guided fine needle aspiration biopsy in pancreatic disease. Gastrointest. Endosc. 1992, 38, 172–173. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, L.; Qu, C.; Liang, S.; Zeng, B.; Luo, Z. Endoscopic ultrasound-guided fine needle core biopsy for the diagnosis of pancreatic malignant lesions: A systematic review and Meta-Analysis. Sci. Rep. 2016, 6, 22978. [Google Scholar] [CrossRef] [PubMed]
- Imazu, H.; Uchiyama, Y.; Matsunaga, K.; Ikeda, K.-I.; Kakutani, H.; Sasaki, Y.; Sumiyama, K.; Ang, T.L.; Omar, S.; Tajiri, H. Contrast-enhanced harmonic EUS with novel ultrasonographic contrast (Sonazoid) in the preoperative T-staging for pancreaticobiliary malignancies. Scand. J. Gastroenterol. 2010, 45, 732–738. [Google Scholar] [CrossRef]
- Kitano, M.; Kamata, K.; Imai, H.; Miyata, T.; Yasukawa, S.; Yanagisawa, A.; Kudo, M. Contrast-enhanced harmonic endoscopic ultrasonography for pancreatobiliary diseases. Dig. Endosc. 2015, 27, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Napoleon, B.; Alvarez-Sanchez, M.V.; Gincoul, R.; Pujol, B.; Lefort, C.; Lepilliez, V.; Labadie, M.; Souquet, J.C.; Queneau, P.E.; Scoazec, J.Y.; et al. Contrast-enhanced harmonic endoscopic ultrasound in solid lesions of the pancreas: Results of a pilot study. Endoscopy 2010, 42, 564–570. [Google Scholar] [CrossRef]
- Gincul, R.; Palazzo, M.; Pujol, B.; Tubach, F.; Palazzo, L.; Lefort, C.; Fumex, F.; Lombard, A.; Ribeiro, D.; Fabre, M.; et al. Contrast-harmonic endoscopic ultrasound for the diagnosis of pancreatic adenocarcinoma: A prospective multicenter trial. Endoscopy 2014, 46, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.; Jin, Z.; Xu, C.; Zhang, M.; Zhu, J.; Jiang, F.; Li, Z. Contrast-Enhanced Harmonic Endoscopic Ultrasound-Guided Fine-Needle Aspiration in the Diagnosis of Solid Pancreatic Lesions: A Retrospective Study. PLoS ONE 2015, 10, e0121236. [Google Scholar] [CrossRef]
- Sugimoto, M.; Takagi, T.; Hikichi, T.; Suzuki, R.; Watanabe, K.; Nakamura, J.; Kikuchi, H.; Konno, N.; Waragai, Y.; Watanabe, H.; et al. Conventional versus contrast-enhanced harmonic endoscopic ultrasonography-guided fine-needle aspiration for diagnosis of solid pancreatic lesions: A prospective randomized trial. Pancreatology 2015, 15, 538–541. [Google Scholar] [CrossRef]
- Seicean, A.; Badea, R.; Moldovan-Pop, A.; Vultur, S.; Botan, E.C.; Zaharie, T.; Săftoiu, A.; Mocan, T.; Iancu, C.; Graur, F.; et al. Harmonic Contrast-Enhanced Endoscopic Ultrasonography for the Guidance of Fine-Needle Aspiration in Solid Pancreatic Masses. Ultraschall der Med.-Eur. J. Ultrasound 2015, 38, 174–182. [Google Scholar] [CrossRef]
- Facciorusso, A.; Cotsoglou, C.; Chierici, A.; Mare, R.; Crinò, S.F.; Muscatiello, N. Contrast-Enhanced Harmonic Endoscopic Ultrasound-Guided Fine-Needle Aspiration versus Standard Fine-Needle Aspiration in Pancreatic Masses: A Propensity Score Analysis. Diagnostics 2020, 10, 792. [Google Scholar] [CrossRef] [PubMed]
- Seicean, A.; Samarghitan, A.; Bolboacă, S.D.; Pojoga, C.; Rusu, I.; Rusu, D.; Sparchez, Z.; Gheorghiu, M.; Al Hajjar, N.; Seicean, R. Contrast-enhanced harmonic versus standard endoscopic ultrasound-guided fine-needle aspiration in solid pancreatic lesions: A single-center prospective randomized trial. Endoscopy 2020, 52, 1084–1090. [Google Scholar] [CrossRef] [PubMed]
- Itonaga, M.; Kitano, M.; Kojima, F.; Hatamaru, K.; Yamashita, Y.; Tamura, T.; Nuta, J.; Kawaji, Y.; Shimokawa, T.; Tanioka, K.; et al. The usefulness of EUS-FNA with contrast-enhanced harmonic imaging of solid pancreatic lesions: A prospective study. J. Gastroenterol. Hepatol. 2020, 35, 2273–2280. [Google Scholar] [CrossRef] [PubMed]
- Kitano, M.; Kudo, M.; Maekawa, K.; Suetomi, Y.; Sakamoto, H.; Fukuta, N.; Nakaoka, R.; Kawasaki, T. Dynamic imaging of pancreatic diseases by contrast enhanced coded phase inversion harmonic ultrasonography. Gut 2004, 53, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Shimokawa, T.; Napoléon, B.; Fusaroli, P.; Gincul, R.; Kudo, M.; Kitano, M. Value of contrast-enhanced harmonic endoscopic ultrasonography with enhancement pattern for diagnosis of pancreatic cancer: A meta-analysis. Dig. Endosc. 2018, 31, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Kitano, M.; Yamashita, Y.; Kamata, K.; Ang, T.L.; Imazu, H.; Ohno, E.; Hirooka, Y.; Fusaroli, P.; Seo, D.-W.; Napoléon, B.; et al. The Asian Federation of Societies for Ultrasound in Medicine and Biology (AFSUMB) Guidelines for Contrast-Enhanced Endoscopic Ultrasound. Ultrasound Med. Biol. 2021, 47, 1433–1447. [Google Scholar] [CrossRef]
- Bang, J.Y.; Magee, S.H.; Ramesh, J.; Trevino, J.M.; Varadarajulu, S. Randomized trial comparing fanning with standard technique for endoscopic ultrasound-guided fine-needle aspiration of solid pancreatic mass lesions. Endoscopy 2013, 45, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Fusaroli, P.; Spada, A.; Mancino, M.G.; Caletti, G. Contrast Harmonic Echo–Endoscopic Ultrasound Improves Accuracy in Diagnosis of Solid Pancreatic Masses. Clin. Gastroenterol. Hepatol. 2010, 8, 629–634e2. [Google Scholar] [CrossRef] [PubMed]
- Kitano, M.; Kudo, M.; Yamao, K.; Takagi, T.; Sakamoto, H.; Komaki, T.; Kamata, K.; Imai, H.; Chiba, Y.; Okada, M.; et al. Characterization of Small Solid Tumors in the Pancreas: The Value of Contrast-Enhanced Harmonic Endoscopic Ultrasonography. Am. J. Gastroenterol. 2012, 107, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Numata, K.; Ozawa, Y.; Kobayashi, N.; Kubota, T.; Shimada, H.; Nozawa, A.; Nakatani, Y.; Sugimori, K.; Matsuo, K.; Imada, T.; et al. Contrast-enhanced sonography of pancreatic carcinoma: Correlations with pathological findings. J. Gastroenterol. 2005, 40, 631–640. [Google Scholar] [CrossRef]
- Ishikawa, R.; Kamata, K.; Hara, A.; Tanaka, H.; Okamoto, A.; Yamazaki, T.; Nakai, A.; Omoto, S.; Minaga, K.; Yamao, K.; et al. Utility of contrast-enhanced harmonic endoscopic ultrasonography for predicting the prognosis of pancreatic neuroendocrine neoplasms. Dig. Endosc. 2020, 33, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Kamata, K.; Takenaka, M.; Omoto, S.; Miyata, T.; Minaga, K.; Yamao, K.; Imai, H.; Sakurai, T.; Nishida, N.; Chikugo, T.; et al. Impact of avascular areas, as measured by contrast-enhanced harmonic EUS, on the accuracy of FNA for pancreatic adenocarcinoma. Gastrointest. Endosc. 2017, 87, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Yamashita, Y.; Itonaga, M. Real-time contrast-enhanced endoscopic ultrasonography-guided fine-needle aspiration (with video). Dig. Endosc. 2012, 25, 631. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, M.; Biagioli, E.; Gerardi, C.; Canestrini, S.; Rulli, E.; Crosara, S.; De Robertis, R.; Floriani, I. Diagnostic Performance of Contrast-Enhanced Ultrasound (CEUS) and Contrast-Enhanced Endoscopic Ultrasound (ECEUS) for the Differentiation of Pancreatic Lesions: A Systematic Review and Meta-Analysis. Ultraschall der Med. Eur. J. Ultrasound 2014, 35, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Fusaroli, P.; Napoleon, B.; Gincul, R.; Lefort, C.; Palazzo, L.; Palazzo, M.; Kitano, M.; Minaga, K.; Caletti, G.; Lisotti, A. The clinical impact of ultrasound contrast agents in EUS: A systematic review according to the levels of evidence. Gastrointest. Endosc. 2016, 84, 587–596e10. [Google Scholar] [CrossRef] [PubMed]
- Kamata, K.; Takenaka, M.; Minaga, K.; Omoto, S.; Miyata, T.; Yamao, K.; Imai, H.; Nakai, A.; Tanaka, H.; Chiba, Y.; et al. Value of additional endoscopic ultrasonography for surveillance after surgical removal of intraductal papillary mucinous neoplasms. Dig. Endosc. 2018, 30, 659–666. [Google Scholar] [CrossRef]
- Sakamoto, H.; Kitano, M.; Suetomi, Y.; Maekawa, K.; Takeyama, Y.; Kudo, M. Utility of Contrast-Enhanced Endoscopic Ultrasonography for Diagnosis of Small Pancreatic Carcinomas. Ultrasound Med. Biol. 2008, 34, 525–532. [Google Scholar] [CrossRef]
- Moriyasu, F.; Itoh, K. Efficacy of Perflubutane Microbubble-Enhanced Ultrasound in the Characterization and Detection of Focal Liver Lesions: Phase 3 Multicenter Clinical Trial. Am. J. Roentgenol. 2009, 193, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Chou, Y.-H.; Liang, J.-D.; Wang, S.-Y.; Hsu, S.-J.; Hu, J.-T.; Yang, S.-S.; Wang, H.-K.; Lee, T.-Y.; Tiu, C.-M. Safety of Perfluorobutane (Sonazoid) in Characterizing Focal Liver Lesions. J. Med. Ultrasound 2019, 27, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Di Leo, M.; Crinò, S.F.; Bernardoni, L.; Rahal, D.; Auriemma, F.; Correale, L.; Donato, G.; Massidda, M.; Anderloni, A.; Manfrin, E.; et al. EUS-guided core biopsies of pancreatic solid masses using a new fork-tip needle: A multicenter prospective study. Dig. Liver Dis. 2019, 51, 1275–1280. [Google Scholar] [CrossRef]
- Witt, B.L.; Factor, R.E.; Chadwick, B.E.; Caron, J.; Siddiqui, A.A.; Adler, D.G. Evaluation of the SharkCore® needle for EUS-guided core biopsy of pancreatic neuroendocrine tumors. Endosc. Ultrasound 2018, 7, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Manrai, M.; Tilak, T.V.S.V.G.K.; Dawra, S.; Srivastava, S.; Singh, A. Current and emerging therapeutic strategies in pancreatic cancer: Challenges and opportunities. World J. Gastroenterol. 2021, 27, 6572–6589. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Uemura, K.; Sudo, T.; Hashimoto, Y.; Yuasa, Y.; Sueda, T. Prognostic Impact of Para-aortic Lymph Node Metastasis in Pancreatic Ductal Adenocarcinoma. World J. Surg. 2010, 34, 1900–1907. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z. FDG-PET in diagnosis, staging and prognosis of pancreatic carcinoma: A meta-analysis. World J. Gastroenterol. 2013, 19, 4808–4817. [Google Scholar] [CrossRef]
- Kurita, A.; Kodama, Y.; Nakamoto, Y.; Isoda, H.; Minamiguchi, S.; Yoshimura, K.; Kuriyama, K.; Sawai, Y.; Uza, N.; Hatano, E.; et al. Impact of EUS-FNA for preoperative para-aortic lymph node staging in patients with pancreatobiliary cancer. Gastrointest. Endosc. 2016, 84, 467–475.e1. [Google Scholar] [CrossRef] [PubMed]
- Miyata, T.; Kitano, M.; Omoto, S.; Kadosaka, K.; Kamata, K.; Imai, H.; Sakamoto, H.; Nisida, N.; Harwani, Y.; Murakami, T.; et al. Contrast-enhanced harmonic endoscopic ultrasonography for assessment of lymph node metastases in pancreatobiliary carcinoma. World J. Gastroenterol. 2016, 22, 3381–3391. [Google Scholar] [CrossRef] [PubMed]
- Lisotti, A.; Ricci, C.; Serrani, M.; Calvanese, C.; Sferrazza, S.; Brighi, N.; Casadei, R.; Fusaroli, P. Contrast-enhanced endoscopic ultrasound for the differential diagnosis between benign and malignant lymph nodes: A meta-analysis. Endosc. Int. Open 2019, 07, E504–E513. [Google Scholar] [CrossRef] [PubMed]
- Minaga, K.; Takenaka, M.; Kamata, K.; Miyata, T.; Yamao, K.; Imai, H.; Kudo, M. Endoscopic ultrasound-guided choledochoduodenostomy with novel use of contrast-enhanced harmonic imaging. Endoscopy 2017, 49, E281–E282. [Google Scholar] [CrossRef]
- Tamura, T.; Kitano, M. Role of CH-EUS as guidance for EUS-biliary drainage malignant obstruction. Minerva Gastroenterol. 2022, 68, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Minaga, K.; Takenaka, M.; Omoto, S.; Miyata, T.; Kamata, K.; Yamao, K.; Imai, H.; Watanabe, T.; Kitano, M.; Kudo, M. A case of successful transluminal drainage of walled-off necrosis under contrast-enhanced harmonic endoscopic ultrasonography guidance. J. Med. Ultrason. 2017, 45, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.-M.; Yang, H.; Jin, Z.-D.; Yu, J.-G.; Cai, Z.-Y.; Li, Z.-S. Differential diagnosis of pancreatic cancer from normal tissue with digital imaging processing and pattern recognition based on a support vector machine of EUS images. Gastrointest. Endosc. 2010, 72, 978–985. [Google Scholar] [CrossRef]
- Ozkan, M.; Cakiroglu, M.; Kocaman, O.; Kurt, M.; Yilmaz, B.; Can, G.; Korkmaz, U.; Dandil, E.; Eksi, Z. Age-based computer-aided diagnosis approach for pancreatic cancer on endoscopic ultrasound images. Endosc. Ultrasound 2016, 5, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, T.; Hara, K.; Mizuno, N.; Okuno, N.; Matsumoto, S.; Obata, M.; Kurita, Y.; Koda, H.; Toriyama, K.; Onishi, S.; et al. Usefulness of Deep Learning Analysis for the Diagnosis of Malignancy in Intraductal Papillary Mucinous Neoplasms of the Pancreas. Clin. Transl. Gastroenterol. 2019, 10, 1–8. [Google Scholar] [CrossRef]
- Goyal, H.; Sherazi, S.A.A.; Gupta, S.; Perisetti, A.; Achebe, I.; Ali, A.; Tharian, B.; Thosani, N.; Sharma, N.R. Application of artificial intelligence in diagnosis of pancreatic malignancies by endoscopic ultrasound: A systemic review. Ther. Adv. Gastroenterol. 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Kamata, K.; Ishihara, R.; Handa, H.; Otsuka, Y.; Yoshida, A.; Yoshikawa, T.; Ishikawa, R.; Okamoto, A.; Yamazaki, T.; et al. Value of artificial intelligence with novel tumor tracking technology in the diagnosis of gastric submucosal tumors by contrast-enhanced harmonic endoscopic ultrasonography. J. Gastroenterol. Hepatol. 2022, 37, 841–846. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).