

Image Quality Analysis of Photon-Counting CT Compared with Dual-Source CT: A Phantom Study for Chest CT Examinations


Abstract
1. Introduction
2. Materials and Methods
2.1. Acquisition and Reconstruction of the Phantom
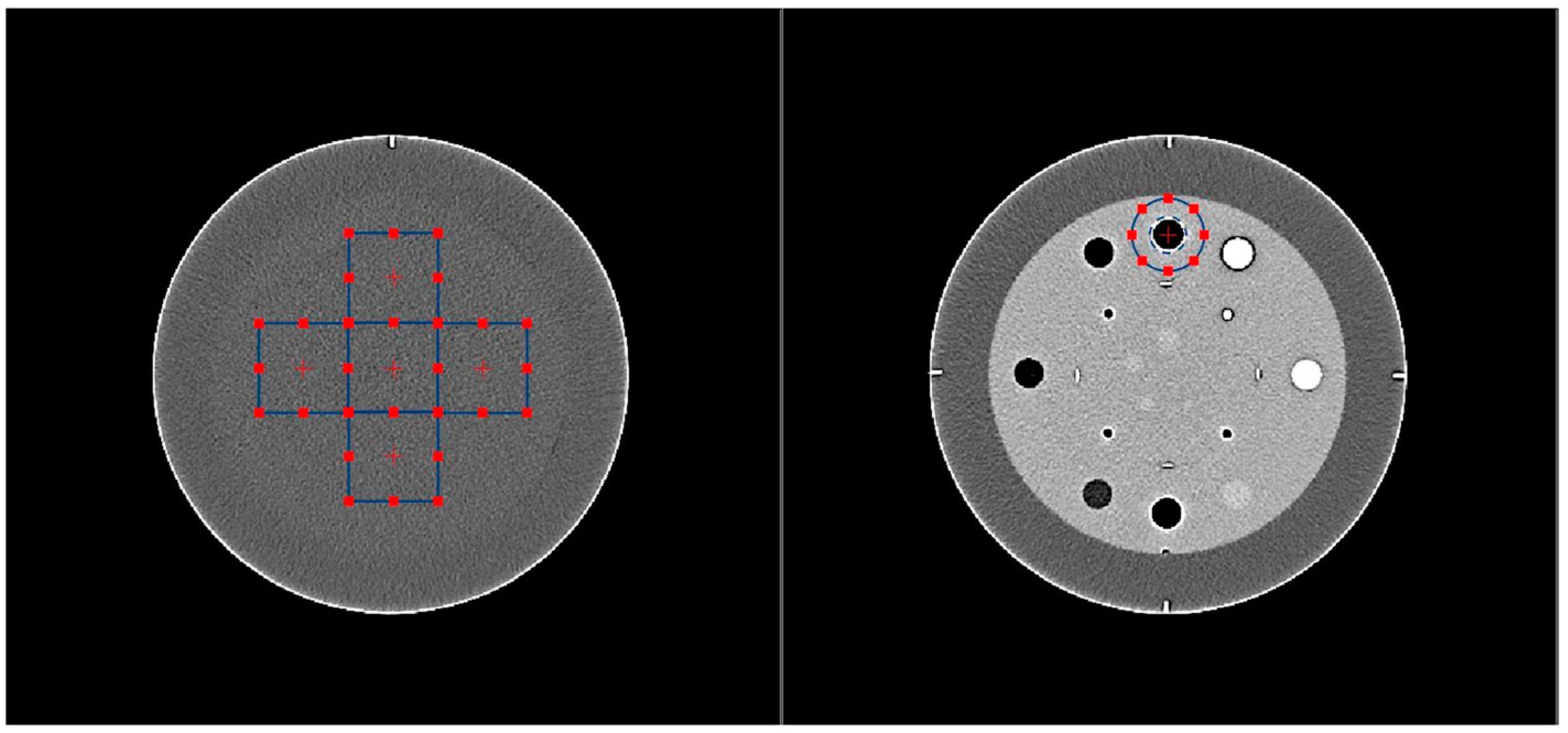
2.2. Physical Metrics
2.2.1. Noise Power Spectrum
2.2.2. Task Transfer Function
2.2.3. Detectability Index
3. Results
3.1. Acquisition and Reconstruction of the Phantom
3.2. Physical Metrics
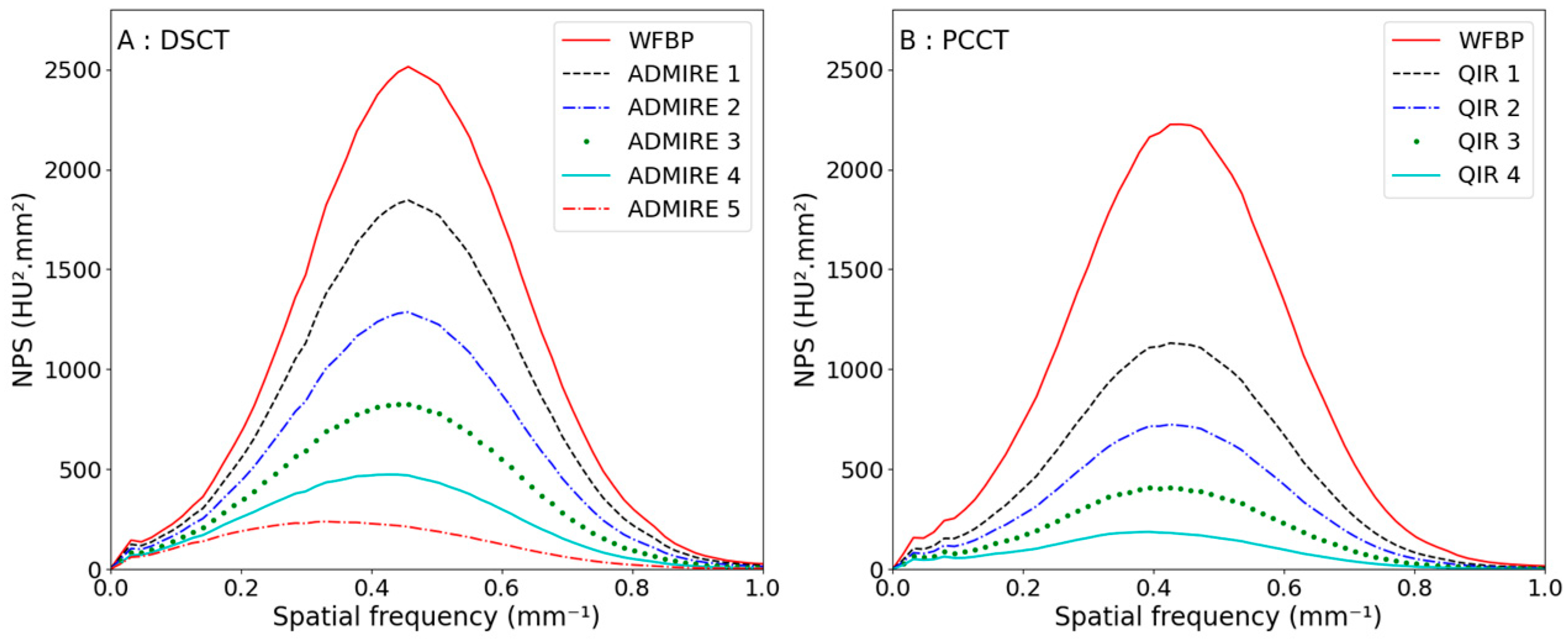
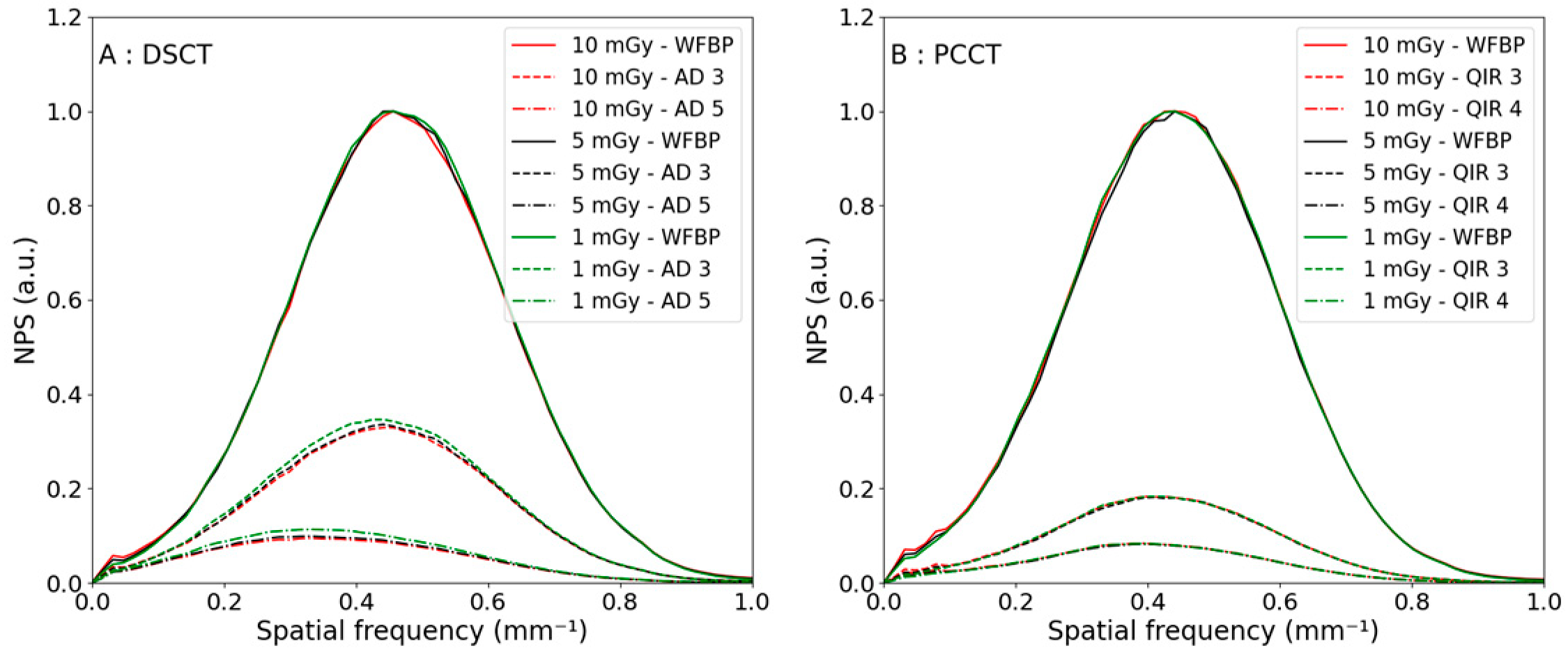
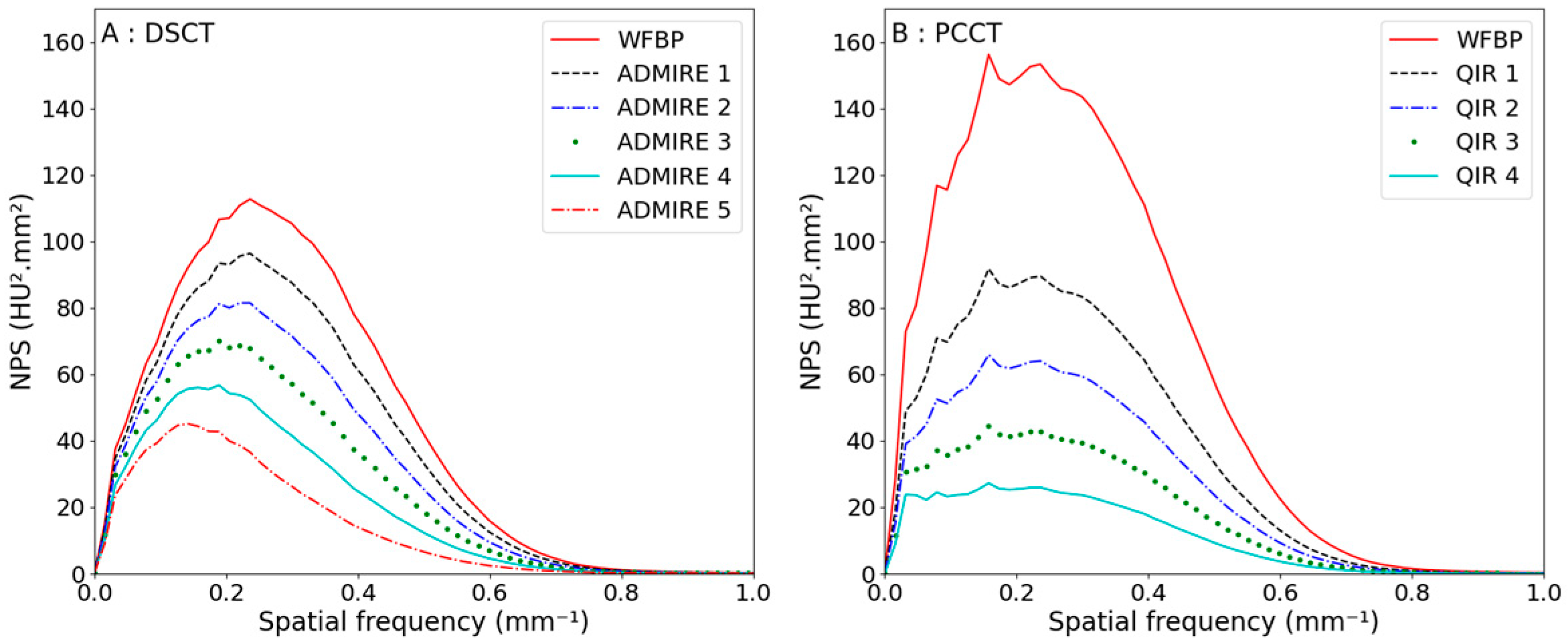
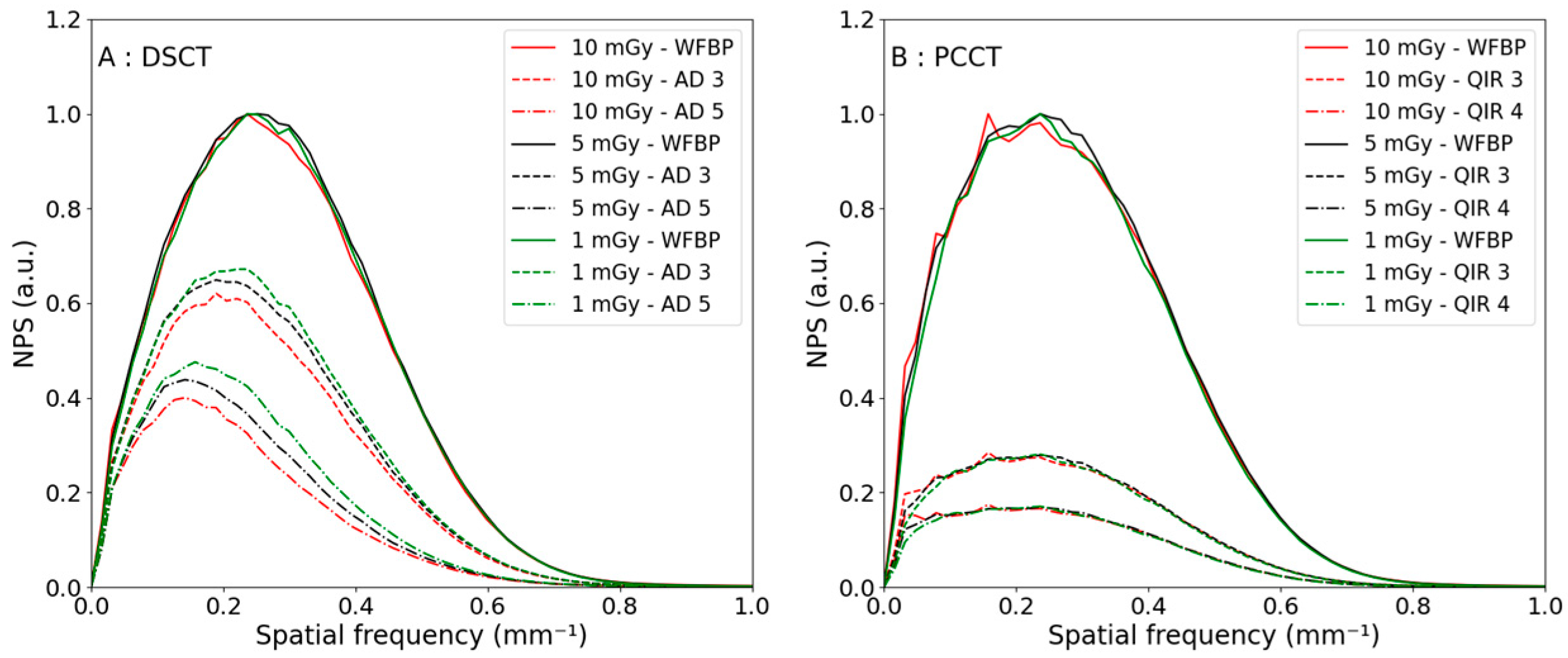
3.2.1. Noise Power Spectrum
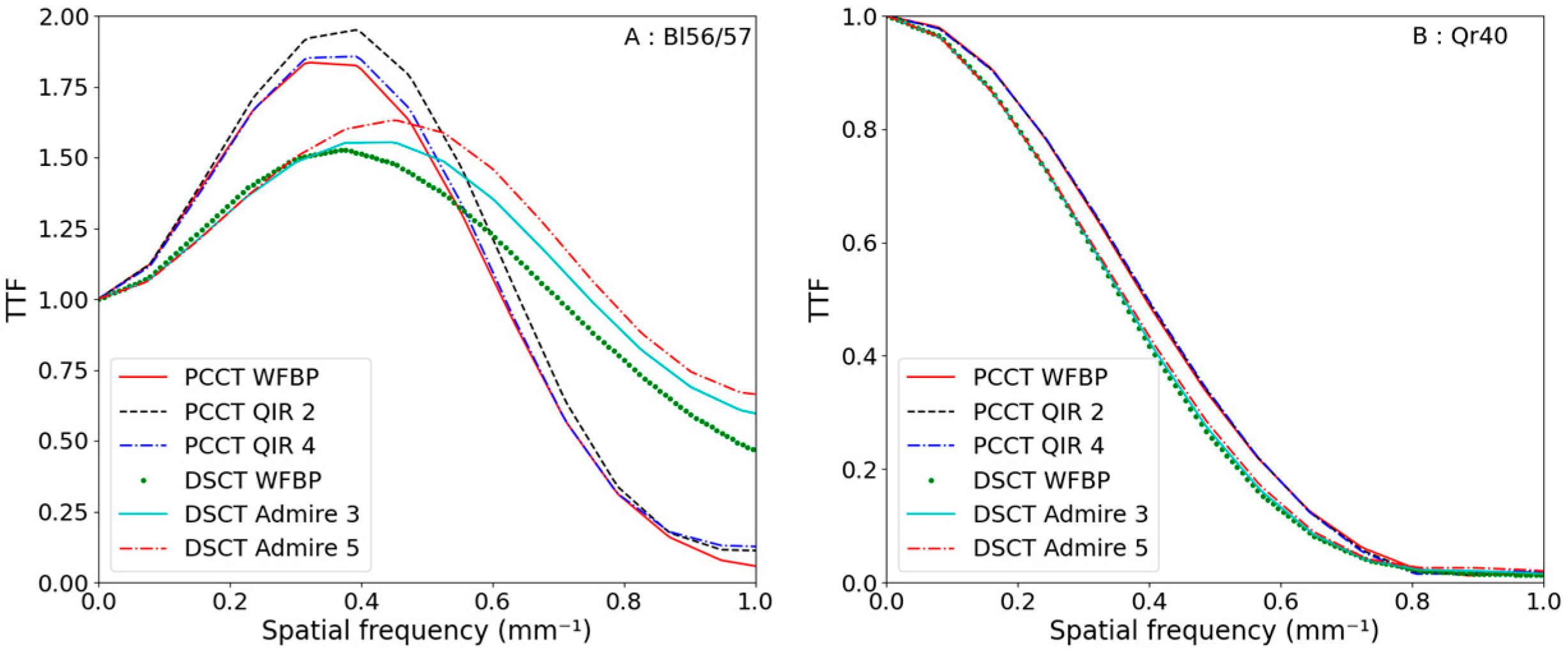
3.2.2. Task-Based Transfer Function
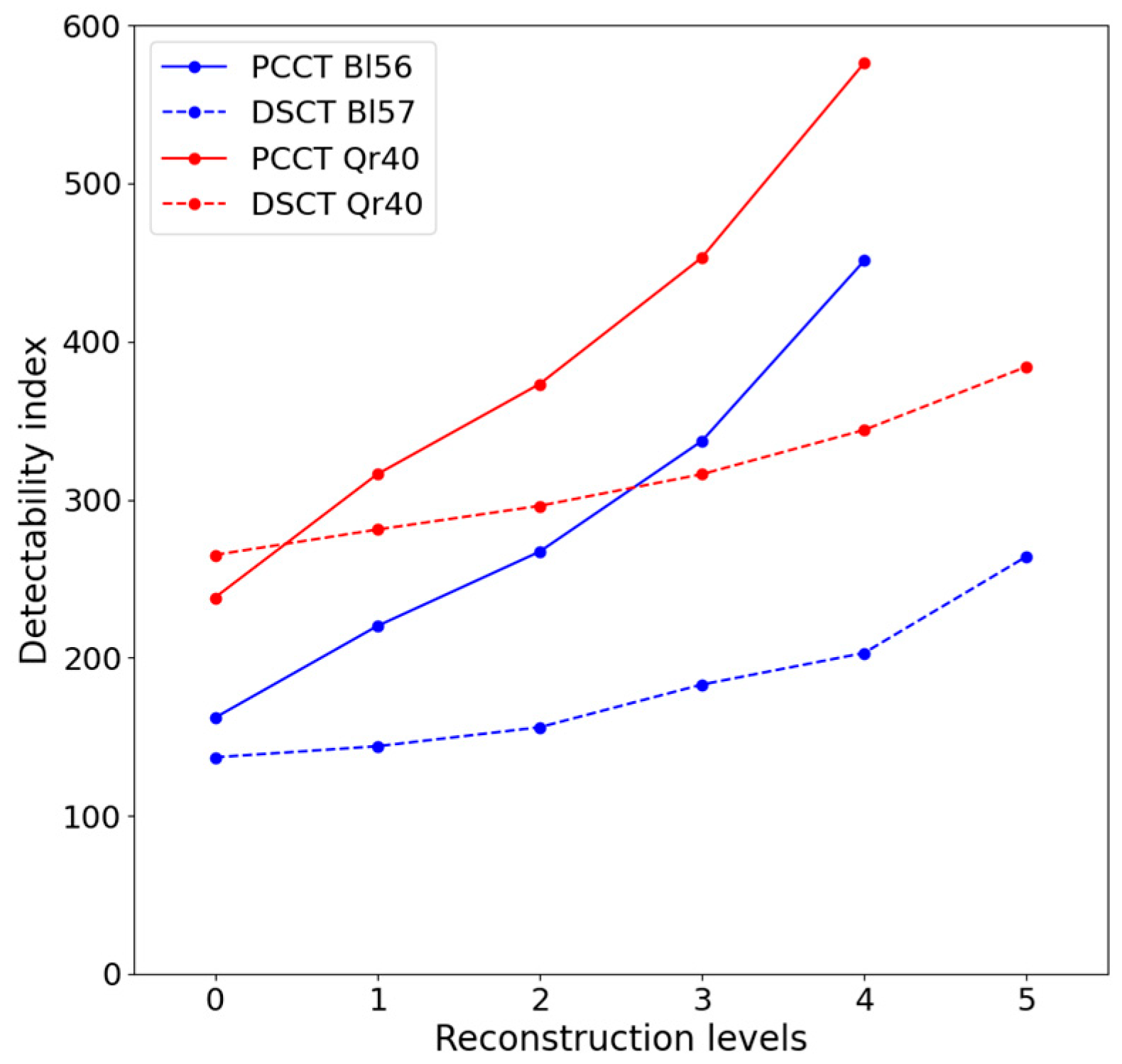
3.2.3. Detectability Index
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Booij, R.; Budde, R.P.J.; Dijkshoorn, M.L.; van Straten, M. Technological developments of X-ray computed tomography over half a century: User’s influence on protocol optimization. Eur. J. Radiol. 2020, 131, 109261. [Google Scholar] [CrossRef] [PubMed]
- Flohr, T.G.; McCollough, C.H.; Bruder, H.; Petersilka, M.; Gruber, K.; Süβ, C.; Grasruck, M.; Stierstorfer, K.; Krauss, B.; Raupach, R.; et al. First performance evaluation of a dual-source CT (DSCT) system. Eur. Radiol. 2006, 16, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Greffier, J.; Villani, N.; Defez, D.; Dabli, D.; Si-Mohamed, S. Spectral CT imaging: Technical principles of dual-energy CT and multi-energy photon-counting CT. In Diagnostic and Interventional Imaging; Elsevier Masson s.r.l.: Amsterdam, The Netherlands, 2022. [Google Scholar] [CrossRef]
- Flohr, T.; Schmidt, B.; Merz, J.; Aulbach, P. Somatom Force Get Two Steps Ahead with Dual Source CT, 2018, Computed Tomography, Siemens Healthcare GmbH, Forchheim, Germany, White Paper. Available online: https://ctmeeting.shpci.org/data/CT_SOMATOM-Force_Whitepaper_DualSource_HOOD05162002908728_152104378.pdf (accessed on 26 March 2023).
- Rajendran, K.; Petersilka, M.; Henning, A.; Shanblatt, E.R.; Schmidt, B.; Flohr, T.G.; Ferrero, A.; Baffour, F.; Diehn, F.E.; Yu, L.; et al. First Clinical Photon-counting Detector CT System: Technical Evaluation. Radiology 2022, 303, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-counting CT: Technical principles and clinical prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef] [PubMed]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-counting CT review. In Physica Medica; Elsevier B.V. for the European Federation of Organisations for Medical Physics (EFOMP) and Associazione Italiana di Fisica Medica (AIFM): Amsterdam, the Netherlands, 2020; Volume 79, pp. 126–136. [Google Scholar] [CrossRef]
- Tortora, M.; Gemini, L.; D’iglio, I.; Ugga, L.; Spadarella, G.; Cuocolo, R. Spectral Photon-Counting Computed Tomography: A Review on Technical Principles and Clinical Applications. J. Imaging 2022, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- Booij, R.; van der Werf, N.R.; Dijkshoorn, M.L.; van der Lugt, A.; van Straten, M. Assessment of Iodine Contrast-To-Noise Ratio in Virtual Monoenergetic Images Reconstructed from Dual-Source Energy-Integrating CT and Photon-Counting CT Data. Diagnostics 2022, 12, 1467. [Google Scholar] [CrossRef] [PubMed]
- Woeltjen, M.M.; Niehoff, J.H.; Michael, A.E.; Horstmeier, S.; Moenninghoff, C.; Borggrefe, J.; Kroeger, J.R. Low-Dose High-Resolution Photon-Counting CT of the Lung: Radiation Dose and Image Quality in the Clinical Routine. Diagnostics 2022, 12, 1441. [Google Scholar] [CrossRef] [PubMed]
- Sartoretti, T.; Racine, D.; Mergen, V.; Jungblut, L.; Monnin, P.; Flohr, T.G.; Martini, K.; Frauenfelder, T.; Alkadhi, H.; Euler, A. Quantum Iterative Reconstruction for Low-Dose Ultra-High-Resolution Photon-Counting Detector CT of the Lung. Diagnostics 2022, 12, 522. [Google Scholar] [CrossRef] [PubMed]
- Hagen, F.; Hofmann, J.; Wrazidlo, R.; Gutjahr, R.; Schmidt, B.; Faby, S.; Nikolaou, K.; Horger, M. Image quality and dose exposure of contrast-enhanced abdominal CT on a 1st generation clinical dual-source photon-counting detector CT in obese patients vs. a 2nd generation dual-source dual energy integrating detector CT. Eur. J. Radiol. 2022, 151, 110325. [Google Scholar] [CrossRef] [PubMed]
- Sartoretti, T.; Landsmann, A.; Nakhostin, D.; Eberhard, M.; Roeren, C.; Mergen, V.; Higashigaito, K.; Raupach, R.; Alkadhi, H.; Euler, A. Quantum Iterative Reconstruction for Abdominal Photon-counting Detector CT Improves Image Quality. Radiology 2022, 303, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Si-Mohamed, S.A.; Greffier, J.; Miailhes, J.; Boccalini, S.; Rodesch, P.-A.; Vuillod, A.; van der Werf, N.; Dabli, D.; Racine, D.; Rotzinger, D.; et al. Comparison of image quality between spectral photon-counting CT and dual-layer CT for the evaluation of lung nodules: A phantom study. Eur. Radiol. 2022, 32, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D.J.; Koo, C.W.; Bartholmai, B.J.; Rajendran, K.; Weaver, J.M.; Halaweish, A.F.; Leng, S.; McCollough, C.H.; Fletcher, J.G. High-Resolution Chest Computed Tomography Imaging of the Lungs: Impact of 1024 Matrix Reconstruction and Photon-Counting Detector Computed Tomography. Investig. Radiol. 2019, 54, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Si-Mohamed, S.A.; Boccalini, S.; Villien, M.; Yagil, Y.; Erhard, K.; Boussel, L.; Douek, P.C. First Experience with a Whole-Body Spectral Photon-Counting CT Clinical Prototype. Investig. Radiol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Ministère des Solidarités et de la Santé. Arrêté du 23 mai 2019 Portant Homologation de la Décision no 2019-DC-0667 de l’Autorité de Sûreté Nucléaire du 18 avril 2019 Relative aux Modalités D’évaluation des Doses de Rayonnements Ionisants Délivrées aux Patients lors d’un acte de Radiologie, de Pratiques Interventionnelles Radioguidées ou de Médecine Nucléaire et à la Mise à jour des Niveaux de Référence Diagnostiques Associés; Ministère des Solidarités et de la Santé: Paris, France, 2019. [Google Scholar]
- Ministère de la santé, de la jeunesse et des sports. Décision du 22 Novembre 2007 Fixant les Modalités du Contrôle de Qualité des Scanographes; Ministère des Solidarités et de la Santé: Paris, France, 2007. [Google Scholar]
- Samei, E.; Bakalyar, D.; Boedeker, K.L.; Brady, S.; Fan, J.; Leng, S.; Myers, K.J.; Popescu, L.M.; Giraldo, J.C.R.; Ranallo, F.; et al. Performance evaluation of computed tomography systems: Summary of AAPM Task Group 233. Med. Phys. 2019, 46, e735–e756. [Google Scholar] [CrossRef] [PubMed]
- Ott, J.G.; Becce, F.; Monnin, P.; Schmidt, S.; Bochud, F.O.; Verdun, F.R. Update on the non-prewhitening model observer in computed tomography for the assessment of the adaptive statistical and model-based iterative reconstruction algorithms (Physics in Medicine & Biology (2014) 59 (4047–4064)). In Physics in Medicine and Biology; Institute of Physics Publishing: Bristol, UK, 2014; Volume 59, p. 5203. [Google Scholar] [CrossRef]
- Solomon, J.B.; Christianson, O.; Samei, E. Quantitative comparison of noise texture across CT scanners from different manufacturers. Med. Phys. 2012, 39, 6048–6055. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.; Wilson, J.; Samei, E. Characteristic image quality of a third generation dual-source MDCT scanner: Noise, resolution, and detectability. Med. Phys. 2015, 42, 4941–4953. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.P.; Shapira, N.; Chen, A.A.; Shinohara, R.T.; Sahbaee, P.; Schnall, M.; Litt, H.I.; Noël, P.B. First-generation clinical dual-source photon-counting CT: Ultra-low-dose quantitative spectral imaging. Eur. Radiol. 2022, 32, 8579–8587. [Google Scholar] [CrossRef] [PubMed]
- Racine, D.; Mergen, V.; Viry, A.; Eberhard, M.M.; Becce, F.; Rotzinger, D.C.; Alkadhi, H.M.; Euler, A. Photon-Counting Detector CT with Quantum Iterative Reconstruction Impact on Liver Lesion Detection and Radiation Dose Reduction. Investig. Radiol. 2022. [Google Scholar] [CrossRef]
- Michael, A.E.; Boriesosdick, J.; Schoenbeck, D.; Woeltjen, M.M.; Saeed, S.; Kroeger, J.R.; Horstmeier, S.; Lennartz, S.; Borggrefe, J.; Niehoff, J.H. Image-Quality Assessment of Polyenergetic and Virtual Monoenergetic Reconstructions of Unenhanced CT Scans of the Head: Initial Experiences with the First Photon-Counting CT Approved for Clinical Use. Diagnostics 2022, 12, 265. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parenchyma | VMI 70 keV | |||
|---|---|---|---|---|
| DSCT (1) * | PCCT (2) * | DSCT (3) * | PCCT (4) * | |
| Tube | A | A | A + B | A |
| High voltage (kV) | 120 | 120 | 80/Sn 150 | 120 |
| Collimation (mm) | 57.6 | 57.6 | 57.6 | 57.6 |
| Pitch | 1.5 | 1.5 | 1 | 1 |
| Exposure time per rotation (s) | 0.5 | 0.5 | 0.25 | 0.25 |
| Field of view (mm) | 300 | 300 | 300 | 300 |
| Matrix size (pixels) | 512 × 512 | 512 × 512 | 512 × 512 | 512 × 512 |
| Reconstruction strength levels | WFBP + ADMIRE 1 to 5 | WFBP + QIR 1 to 4 | WFBP + ADMIRE 1 to 5 | WFBP + QIR 1 to 4 |
| Acquisition | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| HU (air) | −983 | −1042 | −968 | −1007 |
| HU (background) | 98 | 94 | 95 | 97 |
| Contrast | 1081 | 1136 | 1063 | 1104 |
| DSCT | PCCT | |||||
|---|---|---|---|---|---|---|
| Noise (HU) | fpeak (mm−1) | fmean (mm−1) | Noise (HU) | fpeak (mm−1) | fmean (mm−1) | |
| WFBP | 54.8 | 0.46 | 0.47 | 50.0 | 0.44 | 0.44 |
| 1 | 47.1 (−14.1%) * | 0.46 | 0.46 | 35.7 (−28.6%) * | 0.43 | 0.43 |
| 2 | 39.4 (−28.1%) * | 0.46 | 0.45 | 28.5 (−43.0%) * | 0.43 | 0.43 |
| 3 | 31.8 (−42.0%) * | 0.44 | 0.44 | 21.4 (−57.2%) * | 0.41 | 0.42 |
| 4 | 24.2 (−55.8%) * | 0.43 | 0.42 | 14.4 (−71.2%) * | 0.39 | 0.4 |
| 5 | 16.8 (−69.3%) * | 0.35 | 0.38 | - | - | - |
| DSCT | PCCT | |||||
|---|---|---|---|---|---|---|
| Noise (HU) | fpeak (mm−1) | fmean (mm−1) | Noise (HU) | fpeak (mm−1) | fmean (mm−1) | |
| WFBP | 9.0 | 0.25 | 0.29 | 10.7 | 0.19 | 0.28 |
| 1 | 8.2 (−8.9%) * | 0.22 | 0.28 | 8.2 (−23.4%) * | 0.19 | 0.28 |
| 2 | 7.4 (−17.8%) * | 0.22 | 0.27 | 6.9 (−35.5%) * | 0.19 | 0.27 |
| 3 | 6.6 (−26.7%) * | 0.20 | 0.26 | 5.6 (−47.7%) * | 0.19 | 0.27 |
| 4 | 5.6 (−37.8%) * | 0.17 | 0.25 | 4.4 (−58.9%) * | 0.19 | 0.26 |
| 5 | 4.5 (−50.0%) * | 0.16 | 0.23 | - | - | - |
| DSCT-Bl57 | PCCT-Bl56 | |||||
|---|---|---|---|---|---|---|
| 10 mGy | 5 mGy | 1 mGy | 10 mGy | 5 mGy | 1 mGy | |
| WFBP | 0.97 | 0.96 | 0.91 | 0.73 | 0.75 | 0.75 |
| 1 | 1.13 | 1.06 | 1.17 | 0.75 | 0.76 | 0.77 |
| 2 | 1.23 | 1.18 | 1.24 | 0.75 | 0.76 | 0.79 |
| 3 | 1.29 | 1.25 | 1.28 | 0.75 | 0.77 | 0.80 |
| 4 | 1.40 | 1.39 | 1.32 | 0.73 | 0.76 | 0.82 |
| 5 | 1.49 | 1.48 | 1.34 | - | - | - |
| DSCT | PCCT | |||||
|---|---|---|---|---|---|---|
| 10 mGy | 5 mGy | 1 mGy | 10 mGy | 5 mGy | 1 mGy | |
| WFBP | 0.35 | 0.35 | 0.35 | 0.39 | 0.39 | 0.39 |
| 1 | 0.36 | 0.35 | 0.35 | 0.40 | 0.39 | 0.39 |
| 2 | 0.36 | 0.35 | 0.35 | 0.40 | 0.39 | 0.39 |
| 3 | 0.36 | 0.35 | 0.35 | 0.40 | 0.40 | 0.40 |
| 4 | 0.36 | 0.35 | 0.35 | 0.40 | 0.40 | 0.40 |
| 5 | 0.36 | 0.36 | 0.35 | - | - | - |
| Reconstruction Strength Level | 10 mGy | 5 mGy | 1 mGy |
|---|---|---|---|
| 0 | 162 | 110 | 49 |
| 1 | 220 | 153 | 67 |
| 2 | 267 | 184 | 82 |
| 3 | 337 | 233 | 103 |
| 4 | 451 | 311 | 140 |
| Reconstruction Strength Level | 10 mGy | 5 mGy | 1 mGy |
|---|---|---|---|
| 0 | 238 | 175 | 81 |
| 1 | 316 | 227 | 106 |
| 2 | 373 | 268 | 124 |
| 3 | 453 | 325 | 151 |
| 4 | 576 | 413 | 192 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deleu, M.; Maurice, J.-B.; Devos, L.; Remy, M.; Dubus, F. Image Quality Analysis of Photon-Counting CT Compared with Dual-Source CT: A Phantom Study for Chest CT Examinations. Diagnostics 2023, 13, 1325. https://doi.org/10.3390/diagnostics13071325
Deleu M, Maurice J-B, Devos L, Remy M, Dubus F. Image Quality Analysis of Photon-Counting CT Compared with Dual-Source CT: A Phantom Study for Chest CT Examinations. Diagnostics. 2023; 13(7):1325. https://doi.org/10.3390/diagnostics13071325
Chicago/Turabian StyleDeleu, Marine, Jean-Baptiste Maurice, Laura Devos, Martine Remy, and François Dubus. 2023. "Image Quality Analysis of Photon-Counting CT Compared with Dual-Source CT: A Phantom Study for Chest CT Examinations" Diagnostics 13, no. 7: 1325. https://doi.org/10.3390/diagnostics13071325
APA StyleDeleu, M., Maurice, J.-B., Devos, L., Remy, M., & Dubus, F. (2023). Image Quality Analysis of Photon-Counting CT Compared with Dual-Source CT: A Phantom Study for Chest CT Examinations. Diagnostics, 13(7), 1325. https://doi.org/10.3390/diagnostics13071325