

Point-of-Care Ultrasound in Airway Evaluation and Management: A Comprehensive Review
 , , and
, , and
Abstract
1. Introduction
2. Methods
3. Probe Selection and Technique
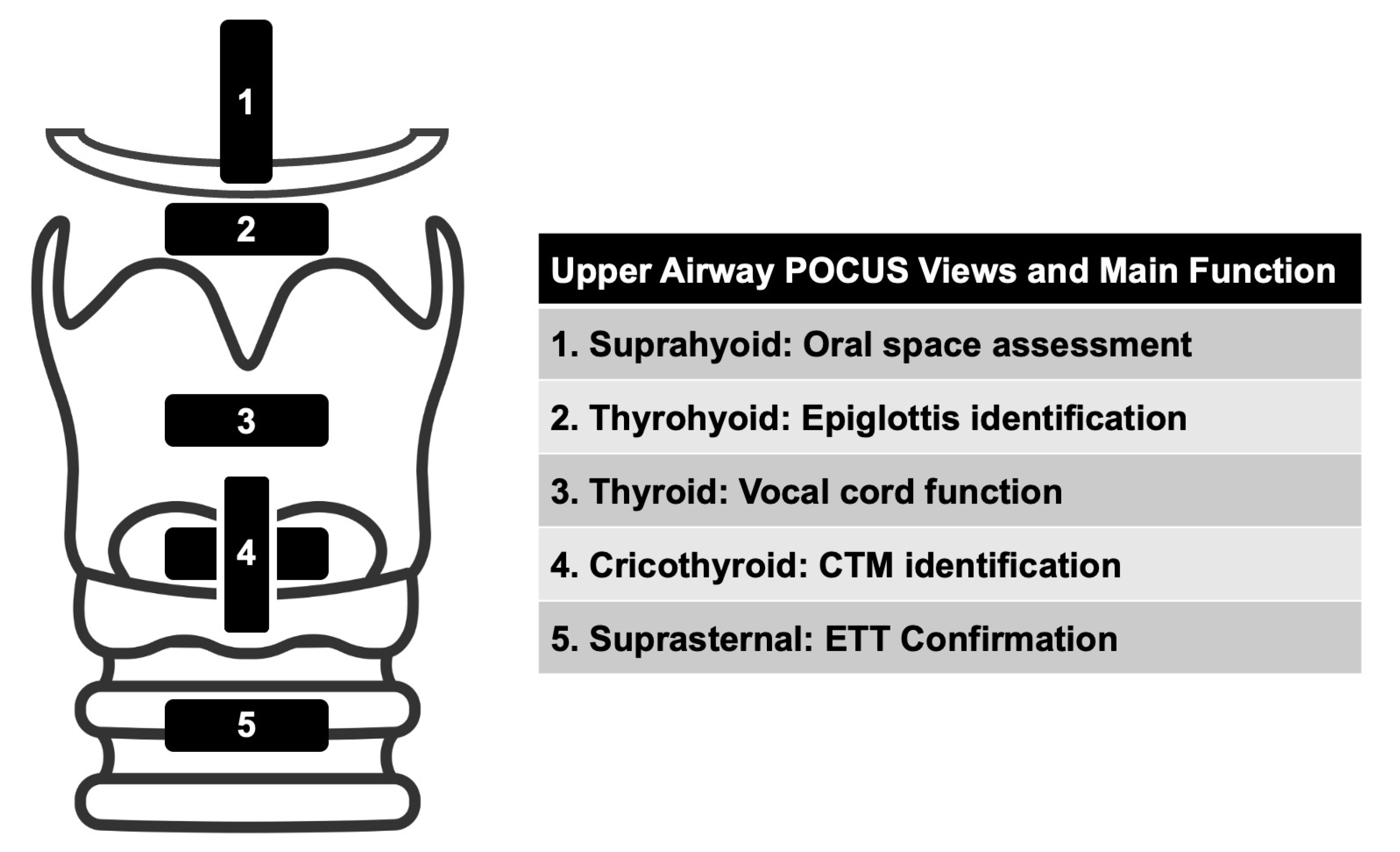
4. Upper Airway Sono-Anatomy
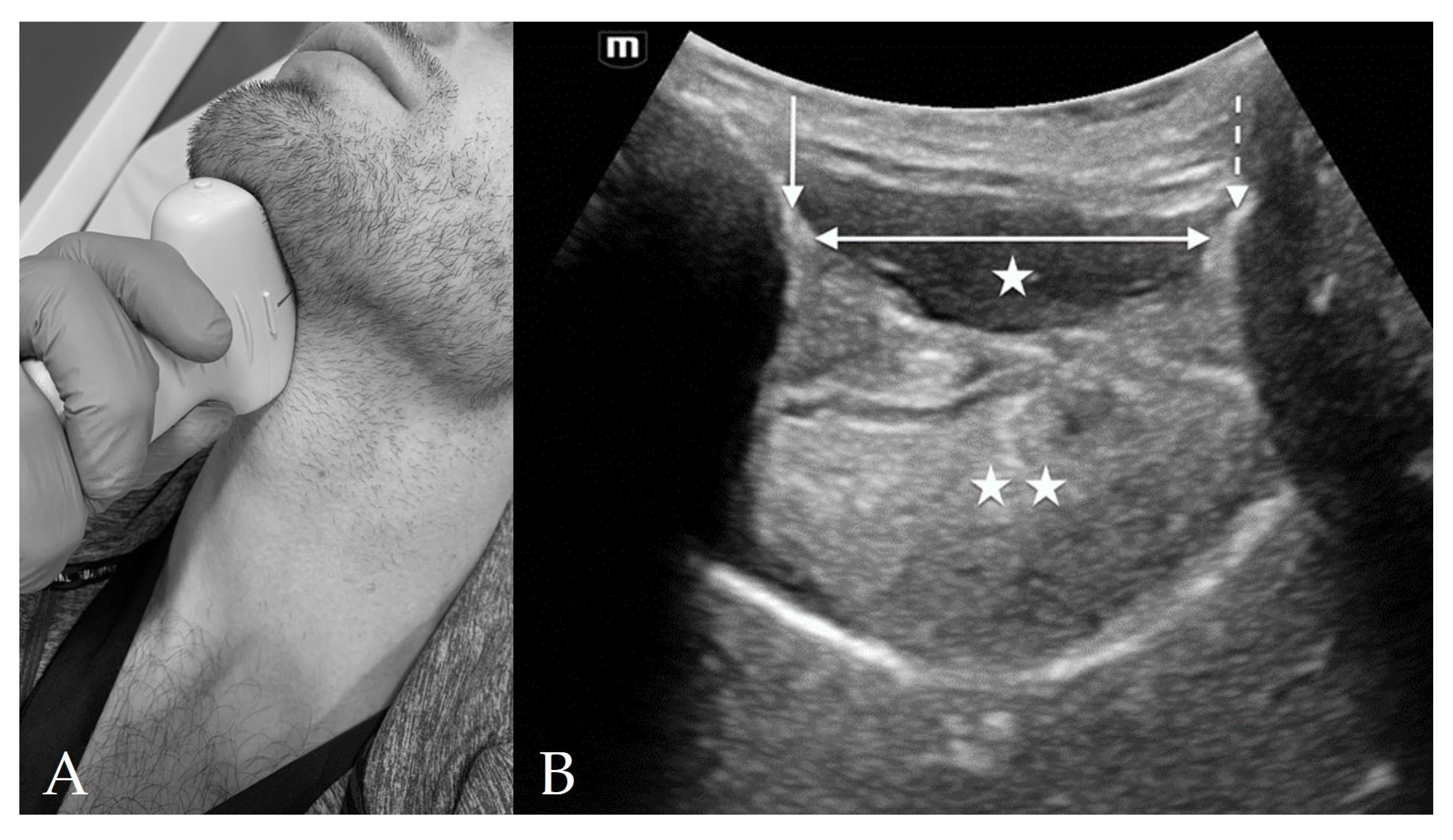
4.1. Suprahyoid View
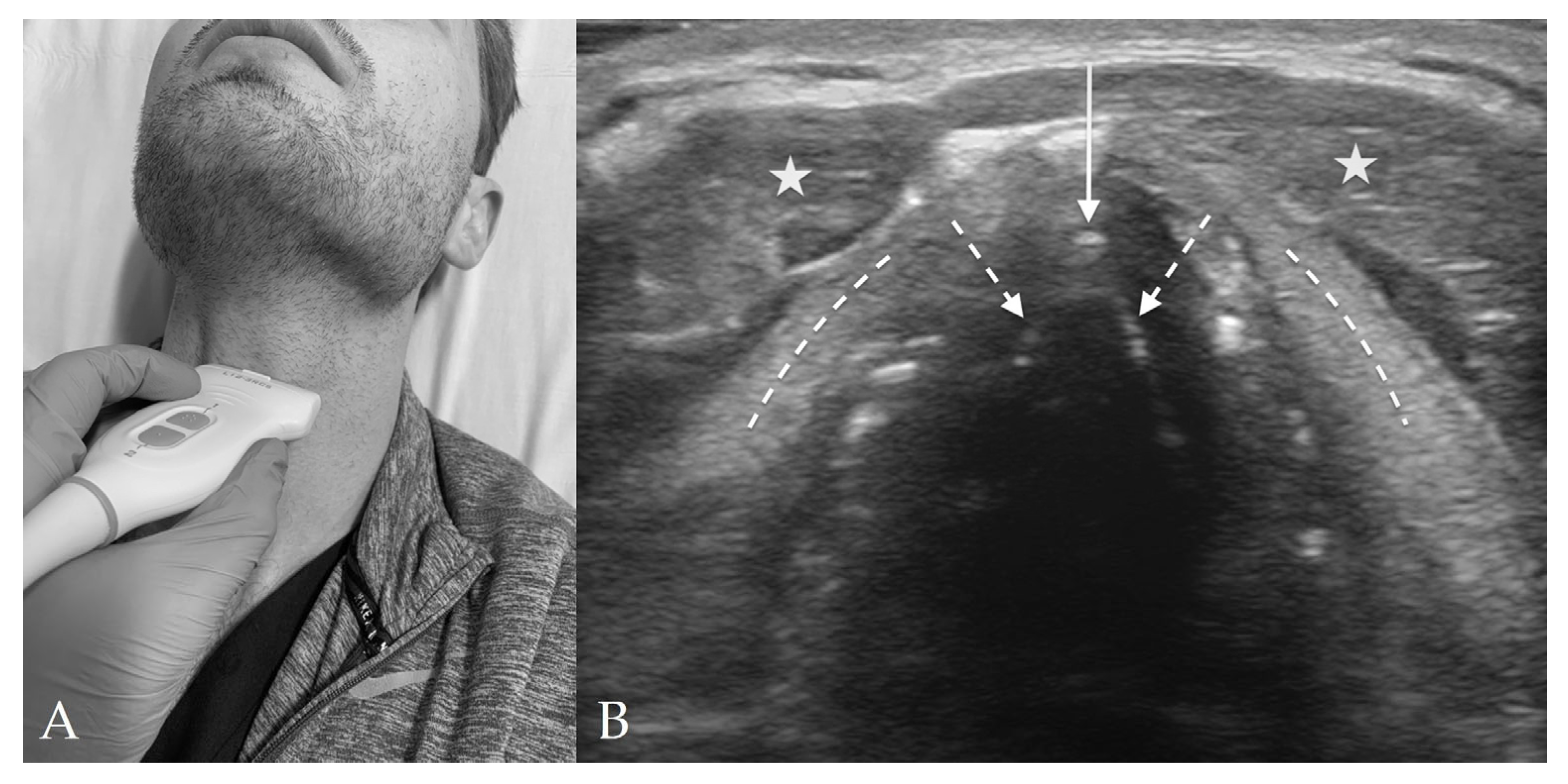
4.2. Thyrohyoid View
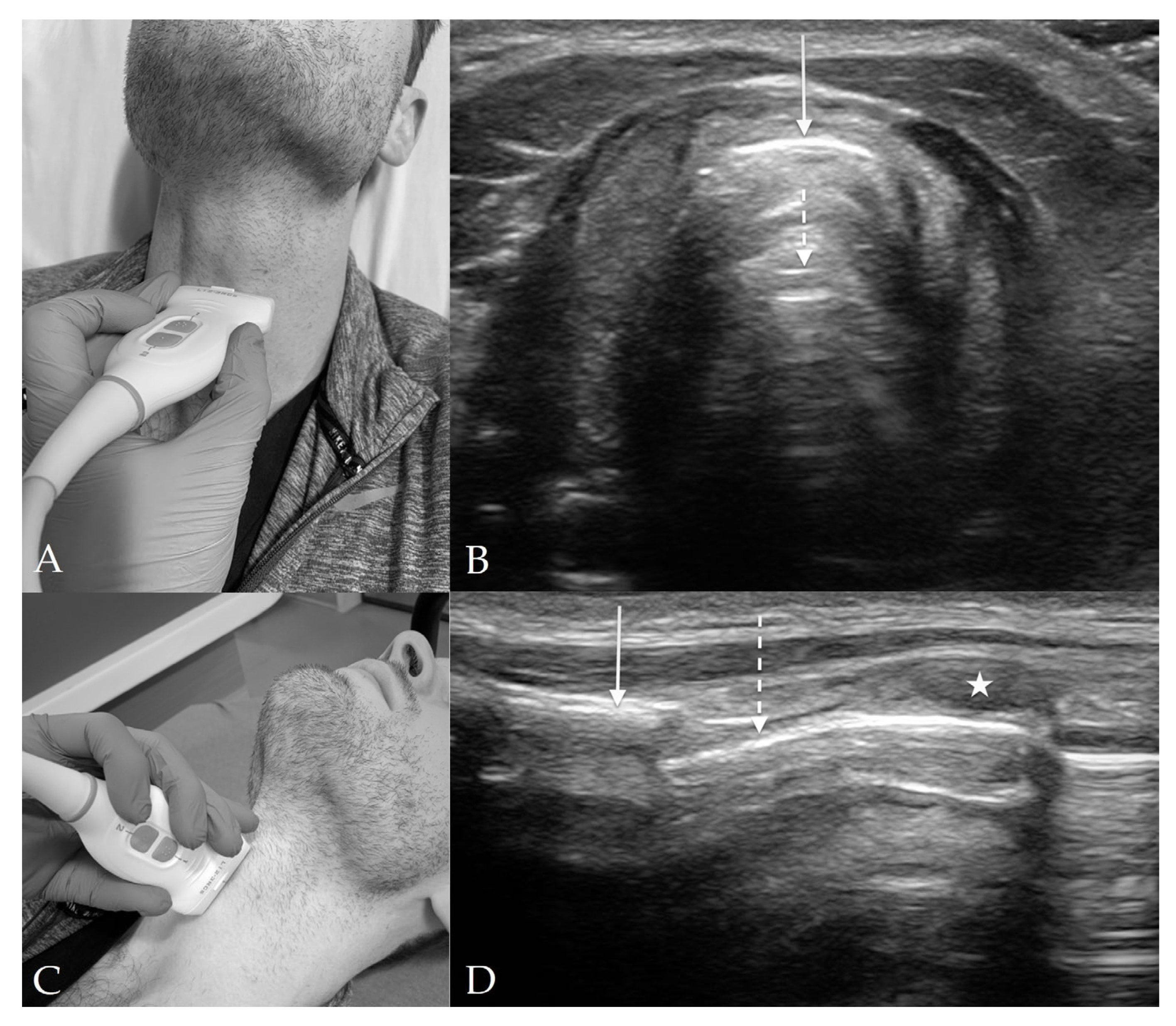
4.3. Thyroid View
4.4. Cricothyroid View
4.5. Suprasternal View
5. Sonographic Assessment of the Difficult Airway
6. Confirmation of Endotracheal Intubation
7. Assessment of Laryngeal Edema
8. Preparation for Cricothyrotomy
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nee, P.A.; Benger, J.; Walls, R.M. Airway management. Emerg. Med. J. 2008, 25, 98–102. [Google Scholar] [CrossRef] [PubMed]
- O’Dell, K. Predictors of difficult intubation and the otolaryngology perioperative consult. Anesth. Clin. 2015, 33, 279–290. [Google Scholar] [CrossRef]
- Brown, C.A., 3rd; Bair, A.E.; Pallin, D.J.; Walls, R.M.; Near III Investigators. Techniques, success, and adverse events of emergency department adult intubations. Ann. Emerg. Med. 2015, 65, 363–370.e1. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Gomez, J.L.; Mayo, P.H.; Koenig, S.J. Point-of-Care Ultrasonography. N. Engl. J. Med. 2021, 385, 1593–1602. [Google Scholar] [CrossRef]
- Ultrasound Guidelines: Emergency, Point-of-Care and Clinical Ultrasound Guidelines in Medicine. Ann. Emerg. Med. 2017, 69, e27–e54. [CrossRef]
- Gottlieb, M.; Holladay, D.; Burns, K.M.; Nakitende, D.; Bailitz, J. Ultrasound for airway management: An evidence-based review for the emergency clinician. Am. J. Emerg. Med. 2020, 38, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.H.; Simoes, A.M.; Nunes, A.M.; Pereira, M.V.; Teoh, W.H.; Costa, P.S.; Kristensen, M.S.; Teixeira, P.M.; Pego, J.M. Useful Ultrasonographic Parameters to Predict Difficult Laryngoscopy and Difficult Tracheal Intubation-A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 671658. [Google Scholar] [CrossRef]
- Sahu, A.K.; Bhoi, S.; Aggarwal, P.; Mathew, R.; Nayer, J.; Amrithanand, V.T.; Mishra, P.R.; Sinha, T.P. Endotracheal Tube Placement Confirmation by Ultrasonography: A Systematic Review and Meta-Analysis of more than 2500 Patients. J. Emerg. Med. 2020, 59, 254–264. [Google Scholar] [CrossRef]
- Chou, H.C.; Tseng, W.P.; Wang, C.H.; Ma, M.H.; Wang, H.P.; Huang, P.C.; Sim, S.S.; Liao, Y.C.; Chen, S.Y.; Hsu, C.Y.; et al. Tracheal rapid ultrasound exam (T.R.U.E.) for confirming endotracheal tube placement during emergency intubation. Resuscitation 2011, 82, 1279–1284. [Google Scholar] [CrossRef]
- Ramsingh, D.; Frank, E.; Haughton, R.; Schilling, J.; Gimenez, K.M.; Banh, E.; Rinehart, J.; Cannesson, M. Auscultation versus Point-of-care Ultrasound to Determine Endotracheal versus Bronchial Intubation: A Diagnostic Accuracy Study. Anesthesiology 2016, 124, 1012–1020. [Google Scholar] [CrossRef]
- Alerhand, S. Ultrasound for identifying the cricothyroid membrane prior to the anticipated difficult airway. Am. J. Emerg. Med. 2018, 36, 2078–2084. [Google Scholar] [CrossRef]
- Beale, T.; Twigg, V.M.; Horta, M.; Morley, S. High-Resolution Laryngeal US: Imaging Technique, Normal Anatomy, and Spectrum of Disease. RadioGraphics 2020, 40, 775–790. [Google Scholar] [CrossRef]
- Jain, K.; Yadav, M.; Gupta, N.; Thulkar, S.; Bhatnagar, S. Ultrasonographic assessment of airway. J. Anaesthesiol. Clin. Pharm. 2020, 36, 5–12. [Google Scholar]
- Lun, H.-M.; Zhu, S.-Y.; Liu, R.-C.; Gong, J.-G.; Liu, Y.-L. Investigation of the Upper Airway Anatomy With Ultrasound. Ultrasound Q. 2016, 32, 86–92. [Google Scholar] [CrossRef]
- Fernandez-Vaquero, M.A.; Charco-Mora, P.; Garcia-Aroca, M.A.; Greif, R. Preoperative airway ultrasound assessment in the sniffing position: A prospective observational study. Braz. J. Anesthesiol. Engl. Ed. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Falcetta, S.; Cavallo, S.; Gabbanelli, V.; Pelaia, P.; Sorbello, M.; Zdravkovic, I.; Donati, A. Evaluation of two neck ultrasound measurements as predictors of difficult direct laryngoscopy. Eur. J. Anaesthesiol. 2018, 35, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Teoh, W.H.; Kristensen, M.S. Ultrasound in Airway Management. Curr. Anesthesiol. Rep. 2020, 10, 317–326. [Google Scholar] [CrossRef]
- Plata, P.; Gaszyński, T. Ultrasound-guided percutaneous tracheostomy. Anaesthesiol. Intensive Ther. 2019, 51, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Lien, W.-C. Comments to Role of upper airway ultrasound in airway management. J. Intensive Care 2017, 5, 10. [Google Scholar] [CrossRef]
- Cook, T.M.; MacDougall-Davis, S.R. Complications and failure of airway management. Br. J. Anaesth. 2012, 109, i68–i85. [Google Scholar] [CrossRef]
- Mouri, M.; Krishnan, S.; Maani, C.V. Airway Assessment. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology 2022, 136, 31–81. [Google Scholar] [CrossRef] [PubMed]
- Kollmeier, B.R.; Boyette, L.C.; Beecham, G.B.; Desai, N.M.; Khetarpal, S. Difficult Airway. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Detsky, M.E.; Jivraj, N.; Adhikari, N.K.; Friedrich, J.O.; Pinto, R.; Simel, D.L.; Wijeysundera, D.N.; Scales, D.C. Will This Patient Be Difficult to Intubate? JAMA 2019, 321, 493. [Google Scholar] [CrossRef]
- Roth, D.; Pace, N.L.; Lee, A.; Hovhannisyan, K.; Warenits, A.-M.; Arrich, J.; Herkner, H. Airway physical examination tests for detection of difficult airway management in apparently normal adult patients. Cochrane Database Syst. Rev. 2018, 5, CD008874. [Google Scholar] [CrossRef]
- Bhargava, V.; Rockwell, N.A.; Tawfik, D.; Haileselassie, B.; Petrisor, C.; Su, E. Prediction of Difficult Laryngoscopy Using Ultrasound: A Systematic Review and Meta-Analysis. Crit. Care Med. 2023, 51, 117–126. [Google Scholar] [CrossRef]
- Petrișor, C.; Trancă, S.; Szabo, R.; Simon, R.; Prie, A.; Bodolea, C. Clinical versus Ultrasound Measurements of Hyomental Distance Ratio for the Prediction of Difficult Airway in Patients with and without Morbid Obesity. Diagnostics 2020, 10, 140. [Google Scholar] [CrossRef] [PubMed]
- Carsetti, A.; Sorbello, M.; Adrario, E.; Donati, A.; Falcetta, S. Airway Ultrasound as Predictor of Difficult Direct Laryngoscopy: A Systematic Review and Meta-analysis. Anesth. Analg. 2022, 134, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Alessandri, F.; Antenucci, G.; Piervincenzi, E.; Buonopane, C.; Bellucci, R.; Andreoli, C.; Alunni Fegatelli, D.; Ranieri, M.V.; Bilotta, F. Ultrasound as a new tool in the assessment of airway difficulties: An observational study. Eur. J. Anaesthesiol. 2019, 36, 509–515. [Google Scholar] [CrossRef]
- Sotoodehnia, M.; Rafiemanesh, H.; Mirfazaelian, H.; Safaie, A.; Baratloo, A. Ultrasonography indicators for predicting difficult intubation: A systematic review and meta-analysis. BMC Emerg. Med. 2021, 21, 76. [Google Scholar] [CrossRef] [PubMed]
- Altun, D.; Kara, H.; Bozbora, E.; Ali, A.; Dinç, T.; Sonmez, S.; Buget, M.; Aydemir, L.; Basaran, B.; Tuğrul, M.; et al. The Role of Indirect Laryngoscopy, Clinical and Ultrasonographic Assessment in Prediction of Difficult Airway. Laryngoscope 2021, 131, E555–E560. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, R.S.; Pannirselvam, S.; Thirumaaran, U. Measurement of Neck Circumference, Tongue thickness and Skin to Epiglottis Distance as Predictors of Difficult Intubation: A Prospective Study. J. Pharm. Negat. Results 2022, 13, 1181–1185. [Google Scholar] [CrossRef]
- Andruszkiewicz, P.; Wojtczak, J.; Sobczyk, D.; Stach, O.; Kowalik, I. Effectiveness and Validity of Sonographic Upper Airway Evaluation to Predict Difficult Laryngoscopy. J. Ultrasound Med. 2016, 35, 2243–2252. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Jain, G.; Agarwal, A.; Govil, N. Effectiveness of four ultrasonographic parameters as predictors of difficult intubation in patients without anticipated difficult airway. Korean J. Anesth. 2021, 74, 134–141. [Google Scholar] [CrossRef]
- Bindu, H.M.; Dogra, N.; Makkar, J.K.; Bhatia, N.; Meena, S.; Gupta, R. Limited condylar mobility by ultrasonography predicts difficult direct laryngoscopy in morbidly obese patients: An observational study. Indian J. Anaesth. 2021, 65, 612–618. [Google Scholar]
- Bouzid, K.; Ketata, S.; Zouche, I.; Keskes, M.; Kammoun, A.; Moncef, S.; Karoui, A. Ultrasonography predicts difficult airway management: A prospective double blinded study. Trends Anaesth. Crit. Care 2022, 46, 18–24. [Google Scholar] [CrossRef]
- Chan, S.M.M.; Wong, W.Y.; Lam, S.K.T.; Wong, O.F.; Law, W.S.S.; Shiu, W.Y.Y.; Mak, P.Y.E. Use of ultrasound to predict difficult intubation in Chinese population by assessing the ratio of the pre-epiglottis space distance and the distance between epiglottis and vocal folds. Hong Kong J. Emerg. Med. 2018, 25, 152–159. [Google Scholar] [CrossRef]
- Daggupati, H.; Maurya, I.; Singh, R.D.; Ravishankar, M. Development of a scoring system for predicting difficult intubation using ultrasonography. Indian J. Anaesth. 2020, 64, 187–192. [Google Scholar]
- Falsafi, F.; Shafikhani, A.A.; Nasseh, N.; Kayalha, H. Relationship Between Upper Airway Ultrasound Parameters and Degree of Difficult Laryngoscopy for Endotracheal Intubation. J. Cell. Mol. Anesth. 2022, 8, 40–47. [Google Scholar]
- Lin, H.Y.; Tzeng, I.S.; Hsieh, Y.L.; Kao, M.C.; Huang, Y.C. Submental Ultrasound Is Effective in Predicting Difficult Mask Ventilation but Not in Difficult Laryngoscopy. Ultrasound Med. Biol. 2021, 47, 2243–2249. [Google Scholar] [CrossRef]
- Moura, E.C.R.; Filho, A.S.M.; de Oliveira, E.; Freire, T.T.; da Cunha Leal, P.; de Sousa Gomes, L.M.R.; Servin, E.T.N.; de Oliveira, C.M.B. Comparative Study of Clinical and Ultrasound Parameters for Defining a Difficult Airway in Patients with Obesity. Obes. Surg. 2021, 31, 4118–4124. [Google Scholar] [CrossRef] [PubMed]
- Ni, H.; Guan, C.; He, G.; Bao, Y.; Shi, D.; Zhu, Y. Ultrasound measurement of laryngeal structures in the parasagittal plane for the prediction of difficult laryngoscopies in Chinese adults. BMC Anesth. 2020, 20, 134. [Google Scholar] [CrossRef] [PubMed]
- Prathep, S.; Jitpakdee, W.; Woraathasin, W.; Oofuvong, M. Predicting difficult laryngoscopy in morbidly obese Thai patients by ultrasound measurement of distance from skin to epiglottis: A prospective observational study. BMC Anesth. 2022, 22, 145. [Google Scholar] [CrossRef]
- Rana, S.; Verma, V.; Bhandari, S.; Sharma, S.; Koundal, V.; Chaudhary, S.K. Point-of-care ultrasound in the airway assessment: A correlation of ultrasonography-guided parameters to the Cormack-Lehane Classification. Saudi J. Anaesth. 2018, 12, 292–296. [Google Scholar] [PubMed]
- Reddy, P.B.; Punetha, P.; Chalam, K.S. Ultrasonography—A viable tool for airway assessment. Indian J. Anaesth. 2016, 60, 807–813. [Google Scholar] [CrossRef]
- Wang, L.; Feng, Y.-K.; Hong, L.; Xie, W.-L.; Chen, S.-Q.; Yin, P.; Wu, Q.-P. Ultrasound for diagnosing new difficult laryngoscopy indicator: A prospective, self-controlled, assessor blinded, observational study. Chin. Med. J. 2019, 132, 2066–2072. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, Y.; Zheng, Z.-W.; Liu, Y.-R.; Ma, W.-H. Ultrasound measurements for evaluation of changes in upper airway during anaesthesia induction and prediction difficult laryngoscopy: A prospective observational study. Sci. Rep. 2022, 12, 18564. [Google Scholar] [CrossRef]
- Wu, J.; Dong, J.; Ding, Y.; Zheng, J. Role of anterior neck soft tissue quantifications by ultrasound in predicting difficult laryngoscopy. Med. Sci. Monit. 2014, 20, 2343–2350. [Google Scholar]
- Wu, Y.M.; Su, Y.H.; Huang, S.Y.; Wang, C.W.; Shen, S.C.; Chen, J.T.; Lo, P.H.; Cherng, Y.G.; Wu, H.L.; Tai, Y.H. Morphometric and ultrasonographic determinants of difficult laryngoscopy in obese patients: A prospective observational study. J. Chin. Med. Assoc. 2022, 85, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Yadav, N.K.; Rudingwa, P.; Mishra, S.K.; Pannerselvam, S. Ultrasound measurement of anterior neck soft tissue and tongue thickness to predict difficult laryngoscopy—An observational analytical study. Indian J. Anaesth. 2019, 63, 629–634. [Google Scholar]
- Yao, W.; Wang, B. Can tongue thickness measured by ultrasonography predict difficult tracheal intubation? Br. J. Anaesth. 2017, 118, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Yao, W.; Zhou, Y.; Wang, B.; Yu, T.; Shen, Z.; Wu, H.; Jin, X.; Li, Y. Can Mandibular Condylar Mobility Sonography Measurements Predict Difficult Laryngoscopy? Anesth. Analg. 2017, 124, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Ma, W.; Du, R. Effectiveness and validity of midsagittal tongue cross-sectional area and width measured by ultrasound to predict difficult airways. Minerva Anestesiol. 2021, 87, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Shetty, S.R.; Smruthi, V.T. Validation of clinical versus ultrasound parameters in assessment of airway. Trends Anaesth. Crit. Care 2020, 35, 21–27. [Google Scholar] [CrossRef]
- Yadav, U.; Singh, R.B.; Chaudhari, S.; Srivastava, S. Comparative Study of Preoperative Airway Assessment by Conventional Clinical Predictors and Ultrasound-Assisted Predictors. Anesth. Essays Res. 2020, 14, 213–218. [Google Scholar]
- Abdelhady, B.S.; Elrabiey, M.A.; Abd Elrahman, A.H.; Mohamed, E.E. Ultrasonography versus conventional methods (Mallampati score and thyromental distance) for prediction of difficult airway in adult patients. Egypt. J. Anaesth. 2020, 36, 83–89. [Google Scholar] [CrossRef]
- Koundal, V.; Rana, S.; Thakur, R.; Chauhan, V.; Ekke, S.; Kumar, M. The usefulness of point of care ultrasound (POCUS) in preanaesthetic airway assessment. Indian J. Anaesth. 2019, 63, 1022–1028. [Google Scholar]
- Martínez-García, A.; Guerrero-Orriach, J.L.; Pino-Gálvez, M.A. Ultrasonography for predicting a difficult laryngoscopy. Getting closer. J. Clin. Monit. Comput. 2020, 35, 269–277. [Google Scholar] [CrossRef]
- Xu, L.; Dai, S.; Sun, L.; Shen, J.; Lv, C.; Chen, X. Evaluation of 2 ultrasonic indicators as predictors of difficult laryngoscopy in pregnant women: A prospective, double blinded study. Medicine 2020, 99, e18305. [Google Scholar] [CrossRef] [PubMed]
- Petrisor, C.; Szabo, R.; Constantinescu, C.; Prie, A.; Hagau, N. Ultrasound-based assessment of hyomental distances in neutral, ramped, and maximum hyperextended positions, and derived ratios, for the prediction of difficult airway in the obese population: A pilot diagnostic accuracy study. Anaesthesiol. Intensive 2018, 50, 110–116. [Google Scholar] [CrossRef]
- Wu, H.; Wang, H. Diagnostic Efficacy and Clinical Value of Ultrasonography in Difficult Airway Assessment: Based on a Prospective Cohort Study. Contrast Media Mol. Imaging 2022, 2022, 4706438. [Google Scholar] [CrossRef]
- Verification of Endotracheal Tube Placement. Ann. Emerg. Med. 2016, 68, 152. [CrossRef] [PubMed]
- Zechner, P.M.; Breitkreutz, R. Ultrasound instead of capnometry for confirming tracheal tube placement in an emergency? Resuscitation 2011, 82, 1259–1261. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Holladay, D.; Peksa, G.D. Ultrasonography for the Confirmation of Endotracheal Tube Intubation: A Systematic Review and Meta-Analysis. Ann. Emerg. Med. 2018, 72, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Chou, E.H.; Dickman, E.; Tsou, P.Y.; Tessaro, M.; Tsai, Y.M.; Ma, M.H.; Lee, C.C.; Marshall, J. Ultrasonography for confirmation of endotracheal tube placement: A systematic review and meta-analysis. Resuscitation 2015, 90, 97–103. [Google Scholar] [CrossRef]
- Sim, S.S.; Lien, W.C.; Chou, H.C.; Chong, K.M.; Liu, S.H.; Wang, C.H.; Chen, S.Y.; Hsu, C.Y.; Yen, Z.S.; Chang, W.T.; et al. Ultrasonographic lung sliding sign in confirming proper endotracheal intubation during emergency intubation. Resuscitation 2012, 83, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.J.; Gurley, K.; Hoffmann, B. Bedside Ultrasound for Tracheal Tube Verification in Pediatric Emergency Department and ICU Patients: A Systematic Review. Pediatr. Crit. Care Med. 2016, 17, e469–e476. [Google Scholar] [CrossRef]
- Abdelrahman, T.N.; Abdelhameed, G.A.; Armanious, S.H. Evaluation of real-time tracheal ultrasound versus colorimetric capnography as a point of care tool for confirmation of endotracheal intubation: A randomized controlled study. Ain-Shams J. Anesthesiol. 2020, 12, 66. [Google Scholar] [CrossRef]
- Afzalimoghaddam, M.; Basiri, K.; Dvarani, S.; Bagheri, F.; Karimialavijeh, E. The effectiveness of a short training course for emergency medicine residents to confirm tracheal tube placement by ultrasound. Crit. Care Shock 2019, 22, 1–8. [Google Scholar]
- Arafa, S.; Abouzkry, A.; Mohamady, A. Accuracy of bedside upper airway ultrasonography vs standard auscultation for assuring the location of endotracheal tube after tracheal intubation: Comparative study controlled by quantitative waveform capnography. J. Anesth. Clin. Res. 2017, 9. [Google Scholar] [CrossRef]
- Arya, R.; Schrift, D.; Choe, C.; Al-Jaghbeer, M. Real-time Tracheal Ultrasound for the Confirmation of Endotracheal Intubations in the Intensive Care Unit: An Observational Study. J. Ultrasound Med. 2019, 38, 491–497. [Google Scholar] [CrossRef]
- Chen, X.; Zhai, W.; Yu, Z.; Geng, J.; Li, M. Determining correct tracheal tube insertion depth by measuring distance between endotracheal tube cuff and vocal cords by ultrasound in Chinese adults: A prospective case-control study. BMJ Open 2018, 8, e023374. [Google Scholar] [CrossRef]
- Chen, W.; Chen, J.; Wang, H.; Chen, Y. Application of bedside real-time tracheal ultrasonography for confirmation of emergency endotracheal intubation in patients in the intensive care unit. J. Int. Med. Res. 2020, 48, 300060519894771. [Google Scholar] [CrossRef] [PubMed]
- Chou, H.C.; Chong, K.M.; Sim, S.S.; Ma, M.H.; Liu, S.H.; Chen, N.C.; Wu, M.C.; Fu, C.M.; Wang, C.H.; Lee, C.C.; et al. Real-time tracheal ultrasonography for confirmation of endotracheal tube placement during cardiopulmonary resuscitation. Resuscitation 2013, 84, 1708–1712. [Google Scholar] [CrossRef]
- Chowdhury, A.R.; Punj, J.; Pandey, R.; Darlong, V.; Sinha, R.; Bhoi, D. Ultrasound is a reliable and faster tool for confirmation of endotracheal intubation compared to chest auscultation and capnography when performed by novice anaesthesia residents—A prospective controlled clinical trial. Saudi J. Anaesth. 2020, 14, 15–21. [Google Scholar] [PubMed]
- Inangil, G.; Deniz, S.; Temircan, S.; Bakal, Ö.; Sen, H.; Özkan, S. Validation of tracheal intubation of wire-reinforced endotracheal tube with ultrasonography. Signa Vitae J. Intesive Care Emerg. Med. 2018, 14, 20–23. [Google Scholar]
- Kabil, A.E.; Ewis, A.M.; Al-Ashkar, A.M.; Abdelatif, M.A.; Nour, M.O. Real-time tracheal ultrasonography for confirming endotracheal tube placement. Egypt. J. Bronchol. 2018, 12, 323–328. [Google Scholar] [CrossRef]
- Kad, N.; Sikarwar, A.; Kumar, V.; Kumari, D. A study to confirm the position of endotracheal tube using ultrasonography and standard auscultation method. Int. J. Contemp. Med. Res. 2018, 5, L12–L16. [Google Scholar] [CrossRef]
- Lahham, S.; Baydoun, J.; Bailey, J.; Sandoval, S.; Wilson, S.P.; Fox, J.C.; Slattery, D.E. A Prospective Evaluation of Transverse Tracheal Sonography During Emergent Intubation by Emergency Medicine Resident Physicians. J. Ultrasound Med. 2017, 36, 2079–2085. [Google Scholar] [CrossRef] [PubMed]
- Masoumi, B.; Azizkhani, R.; Emam, G.H.; Asgarzadeh, M.; Kharazi, B.Z. Predictive Value of Tracheal Rapid Ultrasound Exam Performed in the Emergency Department for Verification of Tracheal Intubation. Open Access Maced. J. Med. Sci. 2017, 5, 618–623. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Sayyari Doughabadi, M.; Alamdaran, S.A.; Sadrzadeh, S.M.; Zakeri, H.; VafadarMoradi, E. Diagnostic Accuracy of Suprasternal Versus Subxiphoid Ultrasonography for Endotracheal Intubation. Anesth. Pain Med. 2022, 12, e118592. [Google Scholar] [CrossRef]
- Patil, V.; Bhosale, S.; Kulkarni, A.; Prabu, N.; Bhagat, V.; Chaudhary, H.; Sarawar, S.; Narkhede, A.; Divatia, J. Utility of ultrasound of upper airway for confirmation of endotracheal intubation and confirmation of the endotracheal tube position in the intensive care unit patients. J. Emerg. Crit. Care Med. 2019, 3, 15. [Google Scholar] [CrossRef]
- Rahmani, F.; Parsian, Z.; Shahsavarinia, K.; Pouraghaei, M.; Negargar, S.; Mehdizadeh Esfanjani, R.; Soleimanpour, H. Diagnostic Value of Sonography for Confirmation of Endotracheal Intubation in the Emergency Department. Anesth. Pain Med. 2017, 7, e58350. [Google Scholar] [CrossRef] [PubMed]
- Rahul, K.; Cara, K.; Ahmad, A. Using ultrasound to confirm endotracheal tube position in the Intensive Care Unit. J. Anesth. Intensive Care Med. 2016, 1, 555560. [Google Scholar]
- Sethi, A.K.; Salhotra, R.; Chandra, M.; Mohta, M.; Bhatt, S.; Kayina, C.A. Confirmation of placement of endotracheal tube—A comparative observational pilot study of three ultrasound methods. J. Anaesthesiol. Clin. Pharm. 2019, 35, 353–358. [Google Scholar]
- Thomas, V.K.; Paul, C.; Rajeev, P.C.; Palatty, B.U. Reliability of ultrasonography in confirming endotracheal tube placement in an emergency setting. Indian J. Crit. Care Med. 2017, 21, 257. [Google Scholar] [CrossRef]
- Yang, Y.; Yue, Y.; Zhang, D. The sensitivity and specificity of ultrasonic localization of endotracheal intubation. Int. J. Clin. Exp. Med. 2017, 10, 10143–10151. [Google Scholar]
- Zamani Moghadam, H.; Sharifi, M.D.; Rajabi, H.; Mousavi Bazaz, M.; Alamdaran, A.; Jafari, N.; Hashemian, S.A.; Talebi Deloei, M. Screening Characteristics of Bedside Ultrasonography in Confirming Endotracheal Tube Placement; a Diagnostic Accuracy Study. Emergency 2017, 5, e19. [Google Scholar]
- Zamani, M.; Esfahani, M.N.; Joumaa, I.; Heydari, F. Accuracy of Real-time Intratracheal Bedside Ultrasonography and Waveform Capnography for Confirmation of Intubation in Multiple Trauma Patients. Adv. Biomed. Res. 2018, 7, 95. [Google Scholar] [PubMed]
- Hsieh, K.S.; Lee, C.L.; Lin, C.C.; Huang, T.C.; Weng, K.P.; Lu, W.H. Secondary confirmation of endotracheal tube position by ultrasound image. Crit. Care Med. 2004, 32, S374–S377. [Google Scholar] [CrossRef] [PubMed]
- Kerrey, B.T.; Geis, G.L.; Quinn, A.M.; Hornung, R.W.; Ruddy, R.M. A prospective comparison of diaphragmatic ultrasound and chest radiography to determine endotracheal tube position in a pediatric emergency department. Pediatrics 2009, 123, e1039–e1044. [Google Scholar] [CrossRef] [PubMed]
- Soar, J.; Callaway, C.W.; Aibiki, M.; Böttiger, B.W.; Brooks, S.C.; Deakin, C.D.; Donnino, M.W.; Drajer, S.; Kloeck, W.; Morley, P.T.; et al. Part 4: Advanced life support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2015, 95, e71–e120. [Google Scholar] [CrossRef] [PubMed]
- Soar, J.; Berg, K.M.; Andersen, L.W.; Böttiger, B.W.; Cacciola, S.; Callaway, C.W.; Couper, K.; Cronberg, T.; D’Arrigo, S.; Deakin, C.D.; et al. Adult Advanced Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2020, 156, A80–A119. [Google Scholar] [CrossRef]
- Kaminski, A.; Dike, N.O.; Bachista, K.; Boniface, M.; Dove, C.; Simon, L.V. Differences Between Esophageal and Tracheal Intubation Ultrasound View Proficiency: An Educational Study of Novice Prehospital Providers. Cureus 2020, 12, e8686. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Bailitz, J.M.; Christian, E.; Russell, F.M.; Ehrman, R.R.; Khishfe, B.; Kogan, A.; Ross, C. Accuracy of a novel ultrasound technique for confirmation of endotracheal intubation by expert and novice emergency physicians. West. J. Emerg. Med. 2014, 15, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Tsung, J.W.; Fenster, D.; Kessler, D.O.; Novik, J. Dynamic anatomic relationship of the esophagus and trachea on sonography: Implications for endotracheal tube confirmation in children. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2012, 31, 1365–1370. [Google Scholar] [CrossRef]
- Gottlieb, M.; Nakitende, D.; Sundaram, T.; Serici, A.; Shah, S.; Bailitz, J. Comparison of Static versus Dynamic Ultrasound for the Detection of Endotracheal Intubation. West. J. Emerg. Med. 2018, 19, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Holladay, D.; Burns, K.; Gore, S.R.; Wulff, C.; Shah, S.; Bailitz, J. Accuracy of ultrasound for endotracheal intubation between different transducer types. Am. J. Emerg. Med. 2019, 37, 2182–2185. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Burns, K.; Holladay, D.; Chottiner, M.; Shah, S.; Gore, S.R. Impact of endotracheal tube twisting on the diagnostic accuracy of ultrasound for intubation confirmation. Am. J. Emerg. Med. 2020, 38, 1332–1334. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Patel, D.; Jung, C.; Murray, D.; Hartrich, M.; Schraft, E.; Ginn, J.; Peksa, G.D.; Sundaram, T. Comparison of saline versus air for identifying endotracheal intubation with ultrasound. Am. J. Emerg. Med. 2022, 58, 131–134. [Google Scholar] [CrossRef]
- Mori, T.; Nomura, O.; Hagiwara, Y.; Inoue, N. Diagnostic Accuracy of a 3-Point Ultrasound Protocol to Detect Esophageal or Endobronchial Mainstem Intubation in a Pediatric Emergency Department. J. Ultrasound Med. 2019, 38, 2945–2954. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Holladay, D.; Serici, A.; Shah, S.; Nakitende, D. Comparison of color flow with standard ultrasound for the detection of endotracheal intubation. Am. J. Emerg. Med. 2018, 36, 1166–1169. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S.K.; Ciubotaru, R.L.; Wong, J.B. Effect of Failed Extubation on the Outcome of Mechanical Ventilation. Chest 1997, 112, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Frutos-Vivar, F.; Esteban, A.; Apezteguia, C.; González, M.; Arabi, Y.; Restrepo, M.I.; Gordo, F.; Santos, C.; Alhashemi, J.A.; Pérez, F.; et al. Outcome of reintubated patients after scheduled extubation. J. Crit. Care 2011, 26, 502–509. [Google Scholar] [CrossRef]
- Seymour, C.W.; Martinez, A.; Christie, J.D.; Fuchs, B.D. The outcome of extubation failure in a community hospital intensive care unit: A cohort study. Crit. Care 2004, 8, R322–R327. [Google Scholar] [CrossRef]
- Wittekamp, B.H.J.; van Mook, W.N.K.A.; Tjan, D.H.T.; Zwaveling, J.H.; Bergmans, D.C.J.J. Clinical review: Post-extubation laryngeal edema and extubation failure in critically ill adult patients. Crit. Care 2009, 13, 233. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.L.; Cole, R.P. Association Between Reduced Cuff Leak Volume and Postextubation Stridor. Chest 1996, 110, 1035–1040. [Google Scholar] [CrossRef]
- Kriner, E.J.; Shafazand, S.; Colice, G.L. The endotracheal tube cuff-leak test as a predictor for postextubation stridor. Respir. Care 2005, 50, 1632–1638. [Google Scholar]
- De Bast, Y.; De Backer, D.; Moraine, J.-J.; Lemaire, M.; Vandenborght, C.; Vincent, J.-L. The cuff leak test to predict failure of tracheal extubation for laryngeal edema. Intensive Care Med. 2002, 28, 1267–1272. [Google Scholar] [CrossRef]
- Kuriyama, A.; Jackson, J.L.; Kamei, J. Performance of the cuff leak test in adults in predicting post-extubation airway complications: A systematic review and meta-analysis. Crit. Care 2020, 24, 640. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.-H.; Chao, T.-Y.; Chiu, C.-T.; Lin, M.-C. The cuff-leak test is a simple tool to verify severe laryngeal edema in patients undergoing long-term mechanical ventilation. Crit. Care Med. 2006, 34, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Jaber, S.; Chanques, G.; Matecki, S.; Ramonatxo, M.; Vergne, C.; Souche, B.; Perrigault, P.-F.; Eledjam, J.-J. Post-extubation stridor in intensive care unit patients. Intensive Care Med. 2003, 29, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Šustić, A.; Miletić, D.; Protić, A.; Ivančić, A.; Cicvarić, T. Can ultrasound be useful for predicting the size of a left double-lumen bronchial tube? Tracheal width as measured by ultrasonography versus computed tomography. J. Clin. Anesth. 2008, 20, 247–252. [Google Scholar] [CrossRef]
- Mikaeili, H.; Yazdchi, M.; Tarzamni, M.K.; Ansarin, K.; Ghasemzadeh, M. Laryngeal ultrasonography versus cuff leak test in predicting postextubation stridor. J. Cardiovasc. Thorac. Res. 2014, 6, 25–28. [Google Scholar]
- El Amrousy, D.; Elkashlan, M.; Elshmaa, N.; Ragab, A. Ultrasound-Guided Laryngeal Air Column Width Difference as a New Predictor for Postextubation Stridor in Children. Crit. Care Med. 2018, 46, e496–e501. [Google Scholar] [CrossRef]
- Shinohara, M.; Iwashita, M.; Abe, T.; Takeuchi, I. Association between post-extubation upper airway obstruction symptoms and airway size measured by computed tomography: A single-center observational study. BMC Emerg. Med. 2022, 22, 55. [Google Scholar] [CrossRef]
- Ye, R.; Cai, F.; Guo, C.; Zhang, X.; Yan, D.; Chen, C.; Chen, B. Assessing the accuracy of ultrasound measurements of tracheal diameter: An in vitro experimental study. BMC Anesth. 2021, 21, 177. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.W. Laryngeal ultrasound: A useful method in predicting post-extubation stridor. A pilot study. Eur. Respir. J. 2006, 27, 384–389. [Google Scholar] [CrossRef] [PubMed]
- El-Baradey, G.F.; El-Shmaa, N.S.; Elsharawy, F. Ultrasound-guided laryngeal air column width difference and the cuff leak volume in predicting the effectiveness of steroid therapy on postextubation stridor in adult. Are they useful? J. Crit. Care 2016, 36, 272–276. [Google Scholar] [CrossRef]
- Bhargava, T.; Kumar, A.; Bharti, A.; Khuba, S. Comparison of Laryngeal Ultrasound and Cuff Leak Test to Predict Post-Extubation Stridor in Total Thyroidectomy. Turk. J. Anaesthesiol. Reanim. 2021, 49, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.W.; Hung, K.C.; Huang, Y.T.; Yu, C.H.; Lin, C.H.; Chen, I.W.; Sun, C.K. Diagnostic efficacy of sonographic measurement of laryngeal air column width difference for predicting the risk of post-extubation stridor: A meta-analysis of observational studies. Front. Med. 2023, 10, 1109681. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M.; Woodall, N.; Frerk, C. Major complications of airway management in the UK: Results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia. Br. J. Anaesth. 2011, 106, 617–631. [Google Scholar] [CrossRef]
- Kristensen, M.S.; Teoh, W.H.; Rudolph, S.S. Ultrasonographic identification of the cricothyroid membrane: Best evidence, techniques, and clinical impact. Br. J. Anaesth. 2016, 117 (Suppl. S1), i39–i48. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.T.; Kao, Y.S.; Chiu, C.W.; Lin, C.H.; Chou, C.C.; Hsieh, P.Y.; Lin, Y.R. Comparative effectiveness of ultrasound-guided and anatomic landmark percutaneous dilatational tracheostomy: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0258972. [Google Scholar] [CrossRef]
- Rai, Y.; You-Ten, E.; Zasso, F.; de Castro, C.; Ye, X.Y.; Siddiqui, N. The role of ultrasound in front-of-neck access for cricothyroid membrane identification: A systematic review. J. Crit. Care 2020, 60, 161–168. [Google Scholar] [CrossRef]
- Hung, K.C.; Chen, I.W.; Lin, C.M.; Sun, C.K. Comparison between ultrasound-guided and digital palpation techniques for identification of the cricothyroid membrane: A meta-analysis. Br. J. Anaesth. 2021, 126, e9–e11. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, N.; Arzola, C.; Friedman, Z.; Guerina, L.; You-Ten, K.E. Ultrasound Improves Cricothyrotomy Success in Cadavers with Poorly Defined Neck Anatomy: A Randomized Control Trial. Anesthesiology 2015, 123, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.S. Ultrasonography in the management of the airway. Acta Anaesthesiol. Scand. 2011, 55, 1155–1173. [Google Scholar] [CrossRef]
- Kristensen, M.S.; Teoh, W.H.; Rudolph, S.S.; Hesselfeldt, R.; Børglum, J.; Tvede, M.F. A randomised cross-over comparison of the transverse and longitudinal techniques for ultrasound-guided identification of the cricothyroid membrane in morbidly obese subjects. Anaesthesia 2016, 71, 675–683. [Google Scholar] [CrossRef]
- Rudas, M.; Seppelt, I.; Herkes, R.; Hislop, R.; Rajbhandari, D.; Weisbrodt, L. Traditional landmark versus ultrasound guided tracheal puncture during percutaneous dilatational tracheostomy in adult intensive care patients: A randomised controlled trial. Crit. Care 2014, 18, 514. [Google Scholar] [CrossRef]
- Nicholls, S.E.; Sweeney, T.W.; Ferre, R.M.; Strout, T.D. Bedside sonography by emergency physicians for the rapid identification of landmarks relevant to cricothyrotomy. Am. J. Emerg. Med. 2008, 26, 852–856. [Google Scholar] [CrossRef]
- Mallin, M.; Curtis, K.; Dawson, M.; Ockerse, P.; Ahern, M. Accuracy of ultrasound-guided marking of the cricothyroid membrane before simulated failed intubation. Am. J. Emerg. Med. 2014, 32, 61–63. [Google Scholar] [CrossRef]
- Bowness, J.; Teoh, W.H.; Kristensen, M.S.; Dalton, A.; Saint-Grant, A.L.; Taylor, A.; Crawley, S.; Chisholm, F.; Varsou, O.; McGuire, B. A marking of the cricothyroid membrane with extended neck returns to correct position after neck manipulation and repositioning. Acta Anaesthesiol. Scand. 2020, 64, 1422–1425. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Date, and Country | Setting | Patient Group | Study Design | Outcome Variable | Sample Size | Outcome Count | Key Results |
|---|---|---|---|---|---|---|---|
| Alessandri, 2019, Italy [29] | OR, elective surgery | Italian adults undergoing elective ENT surgery with general anesthesia | Prospective observational | CL grade; Han scale | 194 | Difficult airway = 34 (17.5% incidence) Difficult mask ventilation = 8 (4.1% incidence) | The best predictor of difficult airway was the minimum distance from the hyoid bone to skin surface |
| Altun, 2021, Turkey [31] | OR, elective surgery | Turkish adults undergoing an elective procedure with general anesthesia | Prospective observational | CL grade | 140 | Difficult laryngoscope = 22 (15.7% incidence) | Significant correlation of US measurements (ESD, HSD, and ToTR) to predict difficult airway, as well as significant correlation of US measurements (MP + HSD or MP + ESD) combined with IL to predict difficult airway (sensitivity 91%, specificity 97%) |
| Ambrose, 2022, India [32] | OR, elective surgery | Indian adults undergoing elective surgery with general anesthesia | Prospective, observational | CL grade | 120 | Difficult intubation = 41 (34.2% incidence) | Distance between skin to epiglottis, tongue thickness, and neck circumference were significantly associated with difficult intubation cases |
| Andruszkiewicz, 2016, Poland [33] | OR, elective surgery | Polish adults undergoing elective surgery | Prospective observational | CL grade | 199 | Difficult laryngoscope = 22 (11.1% incidence) | Strongest predictors were HMD in extension and tongue volume. Significant predictors were (1) HMD in neutral, (2) HMD in extension, (3) HMDR2, (4) tongue cross-sectional area, and (5) tongue volume |
| Agarwal, 2021, India [34] | OR, elective surgery | Indian adults undergoing | Prospective observational | Difficult intubation | 1043 | Difficult to intubate = 58 (5.56% incidence) | Skin to hyoid bone distance was most accurate to predict difficult intubation |
| Bindu, 2022, India [35] | OR, elective surgery | Indian adults with morbid obesity (BMI > 35) undergoing elective surgery with general anesthesia | Prospective observational | CL grade | 70 | Difficult laryngoscopy = 15 (21.4%) | Limited condylar mobility and increased TT were two independent ultrasonographic predictors for difficult direct laryngoscopy |
| Bouzid, 2022, Tunisia [36] | OR, elective surgery | Tunisian adults undergoing general anesthesia | Prospective observational | CL grade; Difficult intubation | 200 | Difficult laryngoscopy = 41 (incidence 20.5%), Difficult intubation = 29 (14.5%) | A combination of clinical criteria and ultrasound measurements increases the ability to predict difficult airway management |
| Chan, 2018, China [37] | OR, elective surgery | Chinese adults undergoing elective surgery with general anesthesia | Prospective observational | CL grade | 113 | Difficult laryngoscope = 39 (34.5% incidence) | Pre-E/aVF ratio (>1) had better accuracy than pre-E/mVF and pre-E/pVF. Pre-E/E-VC cutoff originally intended to study was too high for the population |
| Daggupati, 2022, India [38] | OR, elective surgery | South Indian adults undergoing elective operation with general anesthesia | Prospective observational | CL grade | 310 | Difficult laryngoscope = 62 (20.0% incidence) | Skin to epiglottis distance via US as part of an airway scoring system (using clinical predictors) was reliable in predicting DA (sensitivity 93%, specificity 85%) |
| Falcetta, 2018, Italy [16] | OR, elective surgery | Italian adults undergoing elective surgery with general anesthesia | Prospective observational | CL grade | 301 | Difficult laryngoscope = 28 (9.3% incidence) | US measured at >2.54 cm and PEA >5.04 cm2 may predict difficult laryngoscopes |
| Falsafi, 2023, Iran [39] | OR, elective surgery | Iranian adults undergoing elective surgery with general anesthesia | Prospective observational | CL grade; Mallampati score | 120 | Difficult laryngoscopy by CL = 34 (28.3% incidence) By Mallampati = 37 (30.8% incidence) | Neck circumference was significantly correlated with difficult laryngoscopy by CL. HMDN, HMDE, tongue thickness, OCH, and ST were significant by Mallampati |
| Lin, 2021, Taiwan [40] | OR, elective surgery | Taiwanese adults undergoing elective procedure under general anesthesia | Prospective observational | CL grade | 47 | Difficult laryngoscopy = 20 (42.6% incidence) | Submental ultrasound was not predictive in difficult laryngoscopy, only difficult mask ventilation (sensitivity 50%, specificity 87%) |
| Moura, 2021, Brazil [41] | OR, elective surgery (bariatric surgery) | Obese Adults | Prospective observational | CL grade | 100 | Difficult airway = 25 (25% incidence) | Skin to epiglottis distance (29.3 mm) was predictive for difficult intubation (AUC 0.656, sensitivity 66.7%, specificity 66%) |
| Ni, 2020, China [42] | OR, elective surgery | Chinese adults undergoing elective procedures with general anesthesia | Prospective observational | CL grade | 211 | Difficult laryngoscopy = 44 (20.9% incidence) | Significant predictor of difficult laryngoscopies using DSE (sensitivity 81.8%, specificity 85.6%) |
| Prathep, 2022, Thailand [43] | OR, elective surgery | Obese adults in Thailand | Prospective observational | CL grade | 88 | Difficult laryngoscopy = 13 (14.8% incidence) | Scoring model based on US measurements were predictive of difficult laryngoscopy (AUC 0.77) |
| Rana, 2018, India [44] | OR, elective surgery | Indian adults undergoing elective surgery with general anesthesia | Prospective observational | CL grade | 120 | Difficult airway = 28 (23.3% incidence) | Significant predictors were Pre-E/E-VC ratio and HDMR2. Pre-E/E-VC was stronger |
| Reddy, 2016, India [45] | OR, elective surgery | Indian adults undergoing elective surgery with general anesthesia | Prospective observational | CL grade | 100 | Difficult laryngoscope = 14 (14% incidence) | Significant predictors were skin-to-anterior commissure of VC and Pre-E/E-VC ratio |
| Wang, 2019, China [46] | OR, elective surgery | Chinese adults undergoing elective procedures with general anesthesia | Prospective observational | CL grade | 499 | Difficult laryngoscopy = 47 (9.4% incidence) | Angle between the epiglottis and glottis (less than 50 degrees) had the best sensitivity (81%) and specificity (89%) |
| Wang, 2022, China [47] | OR, elective surgery | Chinese adults undergoing elective procedure under general anesthesia | Prospective observational | Cl grade | 2254 | Difficult laryngoscope = 142 (6.3% incidence) Difficult intubation = 51 (2.3% incidence) | Study nomogram (consisting of US measurements and clinical parameters) had AUC 0.933 for difficult laryngoscopy and 0.974 for difficult intubation |
| Wu, 2014, China [48] | OR, elective surgery | Han Chinese adults aged 20–65, scheduled to undergo general anesthesia | Prospective observational | CL grade | 203 | Difficult laryngoscope = 28 (13.8% incidence) | Independent predictors of difficult airway were the distance from skin to (1) hyoid bone, (2) epiglottis, and (3) anterior commissure of VC |
| Wu, 2022, Taiwan [49] | OR, elective surgery | Taiwanese adults undergoing laparoscopic sleeve gastrectomy | Prospective observational | CL grade | 80 | Difficult laryngoscopy = 17 (21% incidence) | Greater neck circumference was independently associated with difficult laryngoscopy in obese patients. CSA of the tongue base may serve as an index to identify high-risk patients before tracheal intubation |
| Yadav, 2019, India [50] | OR, elective surgery | Indian adults undergoing elective procedures under general anesthesia | Prospective observational | CL grade | 310 | Difficult laryngoscopy = 35 (11.3% incidence) | Tongue thickness as a predictor (sensitivity 69.6%, specificity 77%); skin to hyoid bone distance (sensitivity 68%, specificity 73%) |
| Yao, 2017, China [51] | OR, elective surgery | Han Chinese adults undergoing elective surgery with general anesthesia | Prospective observational | Difficult intubation; CL grade | 2254 | Difficult laryngoscope = 142 (6.3% incidence) Difficult intubation = 51 (2.26% incidence) | Tongue thickness > 6.1 cm is an independent predictor for difficult laryngoscopy (sensitivity 0.75, specificity 0.72). Significant predictors were tongue thickness and tongue thickness/TMD ratio |
| Yao, 2017, China [52] | OR, elective surgery | Han Chinese adults undergoing elective surgery with general anesthesia | Prospective observational | CL grade | 484 | Difficult laryngoscope = 41 (8.5% incidence) Difficult intubation = 5 (1.0% incidence) | Condylar translation was a significant predictor of difficult laryngoscopy. Condylar translation at ≤1 cm is a meaningful TMJ mobility evaluation predicting difficult laryngoscopy |
| Zheng, 2021, China [53] | OR, elective surgery | Han Chinese adults undergoing elective procedures with general anesthesia | Prospective observational | CL grade | 230 | Difficult laryngoscopy = 28 (12.2% incidence) Difficult intubation = 12 (5.2% incidence) | Midsagittal tongue CSA had highest predictor value for difficult laryngoscopy (sensitivity 71%, specificity 60%) and difficult intubation (sensitivity 39%, specificity 89%) |
| Author, Date, and Country | Setting | Patient Population | Study Type | Sample Size | Outcomes | Key Results |
|---|---|---|---|---|---|---|
| Abdelrahman, 2020, Egypt [68] | OR | Adult | Prospective, Randomized | 70 | Ultrasound and Capnography | 93.8% sensitive, 66.7% specific, 91.4% accurate |
| Afzalimoghaddam, 2019, Iran [69] | ED | Adult | Prospective, observational | 90 | Ultrasound and Capnography | 100% sensitive, 100% specific, US is easily taught and learned, US is an effective method for confirming ET tube placement in ED and does not require interruption of chest compressions |
| Arafa, 2018, Egypt [70] | OR | Adult | Prospective observational | 107 | Ultrasound, Capnography, and Auscultation | 97% sensitive, 71.4% specific |
| Arya, 2018, USA [71] | ICU | Adult | Prospective observational | 75 | Ultrasound and Capnography | 83% sensitive, 100% specific, 100% PPV, 97% NPV |
| Chen, 2018, China [72] | OR | Adult | Prospective case-control | 105 | Ultrasound and Direct laryngoscopy | 100% sensitive, 100% specific, 100% accurate, allows proper positioning of ETT cuff and reduces vocal cord injury after intubation |
| Chen, 2020, China [73] | ICU | Adult | Prospective observational | 118 | Ultrasound and Fiberoptic Bronchoscopy | 75% sensitive, 100% specific, 100% PPV, 97.2% NPV, allowed for rapid clinical decision making |
| Chou, 2011, Taiwan [9] | ED | Adult | Prospective observational | 112 | Ultrasound and Capnography | 98.2% accuracy, 98.9% sensitive, 94.1% specific |
| Chou, 2013, Taiwan [74] | ED | Adult (cardiac arrest) | Prospective observational | 89 | Ultrasound, Capnography, and Auscultation | 100% sensitive, 85.7% specific |
| Chowdhury, 2020, India [75] | OR | Adult | Prospective, single blinded clinical trial | 120 | Ultrasound, Capnography, and Auscultation | 100% sensitive, 100% specific, US was fastest method of determining ET intubation, allowed for rapid correction of errors in placement |
| Inangil, 2018, Turkey [76] | OR | Adult | Prospective, paired, single blind | 56 | Ultrasound and Capnography | 95.75% sensitive, 100% specific, faster than capnography |
| Kabil, 2018, Saudi [77] | ICU | Adult | Prospective observational | 40 | Ultrasound and Bronchoscopy | 97.2% sensitive, 100% specific, rapidly informed decision making |
| Kad, 2018, India [78] | OR | Adult | Prospective crossover | 100 | Ultrasound and Auscultation | 88.46% sensitive, 100% specific when “lung sliding” sign is visualized on US, superior to auscultation alone |
| Lahham, 2017, USA [79] | ED | Adult | Prospective cohort | 72 | Ultrasound and Capnography | 98.5% Sensitive, 75% specific |
| Masoumi, 2017, Iran [80] | ED | Adult | Prospective observational | 100 | Ultrasound and Capnography | 98.9% sensitive, 100% specific for US (TRUE method) to detect ETT |
| Mousavi, 2022, Iran [81] | ED | Adult | Cross-sectional | 66 | Ultrasound and Capnography | 98% specific, 66% sensitive, suprasternal view better than subxiphoid for placement confirmation |
| Patil, 2019, India [82] | ICU | Adult | Prospective observational | 89 | Ultrasound and Capnography | 96% sensitive, 100% specific; allowed for real time detection |
| Rahmani, 2017, Iran [83] | ED | Adult | Descriptive analytic | 75 | Ultrasound and Capnography | “Snowstorm” sign was 100% sensitive and 100% specific for detecting ETT |
| Rahul, 2016, USA [84] | ICU | Adult | Prospective, double blind | 20 | Ultrasound, Capnography, and Auscultation | 100% accuracy, Outperformed gold standard, able to detect right main stem intubation |
| Sethi, 2019, India [85] | OR | Adult | Prospective, randomized, observational | 90 | Ultrasound, Capnography, and Auscultation | 100% accuracy, faster than capnography |
| Thomas, 2017, India [86] | ED | Adult | Prospective cohort study | 100 | Ultrasound and Capnography | 97.89% sensitive, 100% specific for diagnosis of esophageal intubation, equal to capnography but quicker |
| Yang, 2017, China [87] | OR | Adult | Prospective, randomized, double blinded | 93 | Ultrasound and Capnography | 100% sensitive, 88.9% specific for US localization of tracheal intubations |
| Zamani, 2017, Iran [88] | ED | Adult | Prospective, cross sectional | 150 | Ultrasound, Auscultation, Direct Laryngoscopy, ETT aspiration, and Pulse Oximetry | 96% sensitive, 88% specific, 98% PPV, 78% NPV for tracheal US in ETT confirmation |
| Zamani, 2018, Iran [89] | ED | Adult trauma | Prospective, single blind | 100 | Ultrasound and Capnography | 97.9% sensitive, 83.3% specific |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, J.; Bellinger, R.; Shedd, A.; Wolfshohl, J.; Walker, J.; Healy, J.; Taylor, J.; Chao, K.; Yen, Y.-H.; Tzeng, C.-F.T.; et al. Point-of-Care Ultrasound in Airway Evaluation and Management: A Comprehensive Review. Diagnostics 2023, 13, 1541. https://doi.org/10.3390/diagnostics13091541
Lin J, Bellinger R, Shedd A, Wolfshohl J, Walker J, Healy J, Taylor J, Chao K, Yen Y-H, Tzeng C-FT, et al. Point-of-Care Ultrasound in Airway Evaluation and Management: A Comprehensive Review. Diagnostics. 2023; 13(9):1541. https://doi.org/10.3390/diagnostics13091541
Chicago/Turabian StyleLin, Judy, Ryan Bellinger, Andrew Shedd, Jon Wolfshohl, Jennifer Walker, Jack Healy, Jimmy Taylor, Kevin Chao, Yi-Hsuan Yen, Ching-Fang Tiffany Tzeng, and et al. 2023. "Point-of-Care Ultrasound in Airway Evaluation and Management: A Comprehensive Review" Diagnostics 13, no. 9: 1541. https://doi.org/10.3390/diagnostics13091541
APA StyleLin, J., Bellinger, R., Shedd, A., Wolfshohl, J., Walker, J., Healy, J., Taylor, J., Chao, K., Yen, Y.-H., Tzeng, C.-F. T., & Chou, E. H. (2023). Point-of-Care Ultrasound in Airway Evaluation and Management: A Comprehensive Review. Diagnostics, 13(9), 1541. https://doi.org/10.3390/diagnostics13091541