
A Sequent of Gram-Negative Co-Infectome-Induced Acute Respiratory Distress Syndrome Are Potentially Subtle Aggravators Associated to the SARS-CoV-2 Evolution of Virulence
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Designs
2.2. Supporting Examinations and Tests Performed for Confirmation
- Oxygen: Non-invasive oxygenation was undertaken using supplemental oxygen in patients with signs of hypoxemia (i.e., SpO2 < 90%). Initially, 5 L/min was used, which was then titrated to SpO2 ≥ 90% as required. High oxygenation flowed (10–15 or 50–60 L/min) through a facemask that was attached to a restoration bag for an elevated oxygen level as reported by Borghes and Maroldi [54] Nava et al., 2011 [55] and Keenan et al., 2011 [56] the described procedures were initiated for reasonable levels then elevated gradually, namely, from nasal cannula (~4 L) to a simple facemask (~10 L), then a non-Rebreather mask (~15 L). As required, noninvasive ventilation was used for enhanced flow, e.g., a high-flow nasal cannula (100 L) or Bilevel-positive airway pressure (BiPAP).
- Intubation: Mechanical ventilations increased difficulties with breathing or hypoxemia when needed. This was applied through an endotracheal tube or tracheostomy using an ICU expert according to the NIH NHLBI ARDS Clinical Network’s mechanical ventilation protocol card, available at: http://www.ardsnet.org/system/files/Ventilator%20Protocol%20Card.pd (accessed on 5 December 2021).
- Records of microbial co-infection or superinfection and their antimicrobial susceptibility data during ARDS co-infections.
2.3. Statistical Analysis of the Data
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ashbaugh, D.G.; Bigelow, D.B.; Petty, T.L.; Levine, B.E. Acute Respiratory Distress in Adults. Lancet 1967, 290, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Gajic, O.; Dabbagh, O.; Park, P.K.; Adesanya, A.; Chang, S.Y.; Hou, P.; Anderson, H.; Hoth, J.J.; Mikkelsen, M.E.; Gentile, N.T.; et al. Early Identification of Patients at Risk of Acute Lung Injury: Evaluation of Lung Injury Prediction Score in a Multicenter Cohort Study. Am. J. Respir. Crit. Care Med. 2011, 183, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, L.; Xi, X.; Zhou, J.X. The Association Between Etiologies and Mortality in Acute Respiratory Distress Syndrome: A Multicenter Observational Cohort Study. Front. Med. 2021, 8, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Pelosi, P.; Suter, P.M.; Pedoto, A.; Vercesi, P.; Lissoni, A. Acute Respiratory Distress Syndrome Caused by Pulmonary and Extrapulmonary Disease. Different Syndromes? Am. J. Respir. Crit. Care Med. 1998, 158, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.M.; Jung, H.; Koh, Y.; Lee, J.S.; Shim, T.S.; Lee, S.D.; Kim, W.S.; Kim, D.S.; Kim, W.D. Effect of Alveolar Recruitment Maneuver in Early Acute Respiratory Distress Syndrome According to Antiderecruitment Strategy, Etiological Category of Diffuse Lung Injury, and Body Position of the Patient. Crit. Care Med. 2003, 31, 411–418. [Google Scholar] [CrossRef]
- Tugrul, S.; Akinci, O.; Ozcan, P.E.; Ince, S.; Esen, F.; Telci, L.; Akpir, K.; Cakar, N. Effects of Sustained Inflation and Postinflation Positive End-Expiratory Pressure in Acute Respiratory Distress Syndrome: Focusing on Pulmonary and Extrapulmonary Forms. Crit. Care Med. 2003, 31, 738–744. [Google Scholar] [CrossRef]
- Brun-Buisson, C.; Minelli, C.; Bertolini, G.; Brazzi, L.; Pimentel, J.; Lewandowski, K.; Bion, J.; Romand, J.A.; Villar, J.; Thorsteinsson, A.; et al. Epidemiology and Outcome of Acute Lung Injury in European Intensive Care Units. Results from the ALIVE Study. Intensive Care Med. 2004, 30, 51–61. [Google Scholar] [CrossRef]
- Villar, J.; Blanco, J.; Añón, J.M.; Santos-Bouza, A.; Blanch, L.; Ambrós, A.; Gandía, F.; Carriedo, D.; Mosteiro, F.; Basaldúa, S.; et al. The ALIEN Study: Incidence and Outcome of Acute Respiratory Distress Syndrome in the Era of Lung Protective Ventilation. Intensive Care Med. 2011, 37, 1932–1941. [Google Scholar] [CrossRef]
- Rubenfeld, G.D.; Caldwell, E.; Peabody, E.; Weaver, J.; Martin, D.P.; Neff, M.; Stern, E.J.; Hudson, L.D. Incidence and Outcomes of Acute Lung Injury. N. Engl. J. Med. 2005, 353, 1685–1693. [Google Scholar] [CrossRef]
- Caser, E.B.; Zandonade, E.; Pereira, E.; Gama, A.M.C.; Barbas, C.S.V. Impact of Distinct Definitions of Acute Lung Injury on Its Incidence and Outcomes in Brazilian ICUs: Prospective Evaluation of 7,133 Patients*. Crit. Care Med. 2014, 42, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, L.C.P.; Park, M.; Salluh, J.I.F.; Rea-Neto, A.; Souza-Dantas, V.C.; Varaschin, P.; Oliveira, M.C.; Tierno, P.F.G.M.M.; dal-Pizzol, F.; Silva, U.V.A.; et al. Clinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units: A Multicenter, Prospective, Cohort Study. Crit. Care 2013, 17, R63. [Google Scholar] [CrossRef] [PubMed]
- Cochi, S.E.; Kempker, J.A.; Annangi, S.; Kramer, M.R.; Martin, G.S. Mortality Trends of Acute Respiratory Distress Syndrome in the United States from 1999 to 2013. Ann. Am. Thorac. Soc. 2016, 13, 1742–1751. [Google Scholar] [CrossRef] [PubMed]
- Erickson, S.E.; Martin, G.S.; Davis, J.L.; Matthay, M.A.; Eisner, M.D. Recent Trends in Acute Lung Injury Mortality: 1996–2005. Crit. Care Med. 2009, 37, 1574–1579. [Google Scholar] [CrossRef] [PubMed]
- Sigurdsson, M.I.; Sigvaldason, K.; Gunnarsson, T.S.; Moller, A.; Sigurdsson, G.H. Acute Respiratory Distress Syndrome: Nationwide Changes in Incidence, Treatment and Mortality over 23 Years. Acta Anaesthesiol. Scand. 2013, 57, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.M.P.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Clinics, B.W.-E.M. Lung-Protective Ventilation Strategies and Adjunctive Treatments for the Emergency Medicine Patient with Acute Respiratory Failure. Emerg. Med. Clin. N. Am. 2014, 32, 871–887. [Google Scholar] [CrossRef]
- Baron, R. Recent Advances in Understanding and Treating ARDS. F1000Research 2018, 20. [Google Scholar] [CrossRef]
- Villar, J.; Schultz, M.J.; Kacmarek, R.M. The LUNG SAFE: A Biased Presentation of the Prevalence of ARDS! Crit. Care 2016, 20, 108. [Google Scholar] [CrossRef]
- Zaccardelli, D.S.; Pattishall, E.N. Clinical Diagnostic Criteria of the Adult Respiratory Distress Syndrome in the Intensive Care Unit. Crit. Care Med. 1996, 24, 247–251. [Google Scholar] [CrossRef]
- Pepe, P.E.; Potkin, R.T.; Reus, D.H.; Hudson, L.D.; Carrico, C.J. Clinical Predictors of the Adult Respiratory Distress Syndrome. Am. J. Surg. 1982, 144, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Hudson, L.D.; Milberg, J.A.; Anardi, D.; Maunder, R.J. Clinical Risks for Development of the Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 1995, 151 Pt 1, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Fowler, A.A.; Hamman, R.F.; Good, J.T.; Benson, K.N.; Baird, M.; Eberle, D.J.; Petty, T.L.; Hyers, T.M. Adult Respiratory Distress Syndrome: Risk with Common Predispositions. Ann. Intern. Med. 1983, 98 Pt 1, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Baumann, W.R.; Jung, R.C.; Koss, M.; Boylen, C.T.; Navarro, L.; Sharma, O.P. Incidence and Mortality of Adult Respiratory Distress Syndrome: A Prospective Analysis from a Large Metropolitan Hospital. Crit. Care Med. 1986, 14, 1–4. [Google Scholar] [CrossRef]
- Mannes, G.P.; Boersma, W.G.; Baur, C.H.; Postmus, P.E. Adult Respiratory Distress Syndrome (ARDS) Due to Bacteraemic Pneumococcal Pneumonia. Eur. Respir. J. 1991, 4, 503–504. [Google Scholar] [CrossRef] [PubMed]
- Pachon, J.; Prados, M.D.; Capote, F.; Cuello, J.A.; Garnacho, J.; Verano, A. Severe Community-Acquired Pneumonia. Etiology, Prognosis, and Treatment. Am. Rev. Respir. Dis. 1990, 142, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Serra-Batlles, J.; Ferrer, A.; Jimenez, P.; Celis, R.; Cobo, E.; Rodriguez-Roisin, R. Severe Community-Acquired Pneumonia. Epidemiology and Prognostic Factors. Am. Rev. Respir. Dis. 1991, 144, 312–318. [Google Scholar] [CrossRef]
- Self, W.H.; Wunderink, R.G.; Williams, D.J.; Zhu, Y.; Anderson, E.J.; Balk, R.A.; Fakhran, S.S.; Chappell, J.D.; Casimir, G.; Courtney, D.M.; et al. Staphylococcus Aureus Community-Acquired Pneumonia: Prevalence, Clinical Characteristics, and Outcomes. Clin. Infect Dis. 2016, 63, 300–309. [Google Scholar] [CrossRef]
- David, M.Z.; Daum, R.S. Community-Associated Methicillin-Resistant Staphylococcus Aureus: Epidemiology and Clinical Consequences of an Emerging Epidemic. Clin. Microbiol. Rev. 2010, 23, 616–687. [Google Scholar] [CrossRef]
- Mandell, L.A.; Wunderink, R. Methicillin-Resistant Staphylococcus Aureus and Community-Acquired Pneumonia: An Evolving Relationship. Clin. Infect Dis. 2012, 54, 1134–1136. [Google Scholar] [CrossRef]
- Bhatta, D.R.; Cavaco, L.M.; Nath, G.; Kumar, K.; Gaur, A.; Gokhale, S.; Bhatta, D.R. Association of Panton Valentine Leukocidin (PVL) Genes with Methicillin Resistant Staphylococcus Aureus (MRSA) in Western Nepal: A Matter of Concern for Community Infections (a Hospital Based Prospective Study). BMC Infect Dis. 2016, 16, 199. [Google Scholar] [CrossRef] [PubMed]
- Francis, J.S.; Doherty, M.C.; Lopatin, U.; Johnston, C.P.; Sinha, G.; Ross, T.; Cai, M.; Hansel, N.N.; Perl, T.; Ticehurst, J.R.; et al. Severe Community-Onset Pneumonia in Healthy Adults Caused by Methicillin-Resistant Staphylococcus Aureus Carrying the Panton-Valentine Leukocidin Genes. Clin. Infect Dis. 2005, 40, 100–107. [Google Scholar] [CrossRef]
- Gillet, Y.; Issartel, B.; Vanhems, P.; Fournet, J.C.; Lina, G.; Bes, M.; Vandenesch, F.; Piémont, Y.; Brousse, N.; Floret, D.; et al. Association between Staphylococcus Aureus Strains Carrying Gene for Panton-Valentine Leukocidin and Highly Lethal Necrotising Pneumonia in Young Immunocompetent Patients. Lancet 2002, 359, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Fein, A.M.; Lippmann, M.; Holtzman, H.; Eliraz, A.; Goldberg, S.K. The Risk Factors, Incidence, and Prognosis of ARDS Following Septicemia. Chest 1983, 83, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Reyes, L.F.; Aliberti, S.; Restrepo, M.I. Empirical Coverage of Methicillin-Resistant Staphylococcus Aureus in Community-Acquired Pneumonia: Those Who Do Not Remember the Past Are Doomed to Repeat It. Clin. Infect Dis. 2016, 63, 1145–1146. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Letsiou, E.; Wang, H.; Belvitch, P.; Meliton, L.N.; Brown, M.E.; Bandela, M.; Chen, J.; Garcia, J.G.N.; Dudek, S.M. MRSA-Induced Endothelial Permeability and Acute Lung Injury Are Attenuated by FTY720 S-Phosphonate. Am. J. Physiol. Lung Cell Mol. Physiol. 2022, 322, L149–L161. [Google Scholar] [CrossRef] [PubMed]
- Dugani, S.; Veillard, J.; Kissoon, N. Reducing the Global Burden of Sepsis. CMAJ 2017, 189, E2–E3. [Google Scholar] [CrossRef]
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Lower Respiratory Infections in 195 Countries, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef]
- Naghavi, M.; Wang, H.; Lozano, R.; Davis, A.; Liang, X.; Zhou, M.; Vollset, S.E.; Abbasoglu Ozgoren, A.; Abdalla, S.; Abd-Allah, F.; et al. Global, Regional, and National Age-Sex Specific All-Cause and Cause-Specific Mortality for 240 Causes of Death, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef]
- McLaughlin, J.M.; Johnson, M.H.; Kagan, S.A.; Baer, S.L. Clinical and Economic Burden of Community-Acquired Pneumonia in the Veterans Health Administration, 2011: A Retrospective Cohort Study. Infection 2015, 43, 671–680. [Google Scholar] [CrossRef]
- Fernando, S.M.; Rochwerg, B.; Seely, A.J.E. Clinical Implications of the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). CMAJ 2018, 190, E1058–E1059. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Qian, Y.; Miao, Z.; Zheng, P.; Shi, T.; Jiang, X.; Pan, L.; Qian, F.; Yang, G.; An, H.; et al. Xuebijing Injection Alleviates Pam3CSK4-Induced Inflammatory Response and Protects Mice from Sepsis Caused by Methicillin-Resistant Staphylococcus Aureus. Front. Pharmacol. 2020, 11, 104. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial Cell Infection and Endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Herold, S.; Becker, C.; Ridge, K.M.; Budinger, G.R.S. Influenza Virus-Induced Lung Injury: Pathogenesis and Implications for Treatment. Eur. Respir. J. 2015, 45, 1463–1478. [Google Scholar] [CrossRef] [PubMed]
- Bernard, G.R.; Artigas, A.; Brigham, K.L.; Carlet, J.; Falke, K.; Hudson, L.; Lamy, M.; Legall, J.R.; Morris, A.; Spragg, R.; et al. The American-European Consensus Conference on ARDS. Definitions, Mechanisms, Relevant Outcomes, and Clinical Trial Coordination. Am. J. Respir. Crit. Care Med. 1994, 149, 818–824. [Google Scholar] [CrossRef]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.B.; Wang, D.C.; Mei, J.; et al. Performance of Radiologists in Differentiating COVID-19 from Viral Pneumonia on Chest CT. Radiology 2020, 296, E46–E54. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.Y. Pathological Study of the 2019 Novel Coronavirus Disease (COVID-19) through Postmortem Core Biopsies. Mod. Pathol. 2020, 33, 1007. [Google Scholar] [CrossRef]
- Hani, C.; Trieu, N.H.; Saab, I.; Dangeard, S.; Bennani, S.; Chassagnon, G.; Revel, M.P. COVID-19 Pneumonia: A Review of Typical CT Findings and Differential Diagnosis. Diagn. Interv. Imaging 2020, 101, 263. [Google Scholar] [CrossRef]
- Schwarz, M.I.; Albert, R.K. “Imitators” of the ARDS: Implications for Diagnosis and Treatment. Chest 2004, 125, 1530–1535. [Google Scholar] [CrossRef]
- Putman, R.K.; Hunninghake, G.M.; Dieffenbach, P.B.; Barragan-Bradford, D.; Serhan, K.; Adams, U.; Hatabu, H.; Nishino, M.; Padera, R.F.; Fredenburgh, L.E.; et al. Interstitial Lung Abnormalities Are Associated with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, H.; Schenck, L.A.; Horie, R.; Suzuki, J.; Lee, E.H.; McMenomy, B.P.; Chen, T.E.; Lekah, A.; Mankad, S.V.; Gajic, O. Critical Care Ultrasonography Differentiates ARDS, Pulmonary Edema, and Other Causes in the Early Course of Acute Hypoxemic Respiratory Failure. Chest 2015, 148, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International Evidence-Based Recommendations for Point-of-Care Lung Ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [PubMed]
- Borghesi, A.; Maroldi, R. COVID-19 Outbreak in Italy: Experimental Chest X-Ray Scoring System for Quantifying and Monitoring Disease Progression. Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Nava, S.; Schreiber, A.; Domenighetti, G. Noninvasive Ventilation for Patients with Acute Lung Injury or Acute Respiratory Distress Syndrome. Respir. Care 2011, 56, 1583–1588. [Google Scholar] [CrossRef] [PubMed]
- Keenan, S.P.; Sinuff, T.; Burns, K.E.A.; Muscedere, J.; Kutsogiannis, J.; Mehta, S.; Cook, D.J.; Ayas, N.; Adhikari, N.K.J.; Hand, L.; et al. Clinical Practice Guidelines for the Use of Noninvasive Positive-Pressure Ventilation and Noninvasive Continuous Positive Airway Pressure in the Acute Care Setting. CMAJ 2011, 183, E195–E214. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.E.; Chong, V.C.L.; Chan, S.S.W.; Lim, G.H.; Lim, K.G.E.; Tan, G.B.; Mucheli, S.S.; Kuperan, P.; Ong, K.H. Hematologic Parameters in Patients with COVID-19 Infection. Am. J. Hematol. 2020, 95, E131–E134. [Google Scholar] [CrossRef] [PubMed]
- Kaushansky, K.; Lichtman, M.A.; Prchal, J.T.; Levi, M.M.; Press, O.W.; Burns, L.J.; Caligiuri, M. (Eds.) Williams Hematology, 9e|AccessMedicine|McGraw Hill Medical; McGraw Hill: New York, NY, USA, 2015; Available online: https://accessmedicine.mhmedical.com/book.aspx?bookid=1581&isMissingChapter=true (accessed on 5 December 2021).
- Patel, R.; Powell, M.; Richter, S.; Swenson, J.; Traczewaki, M.; Turnidge, J.; Weinstein, M.; Zimmer, B. Performance Standards for Antimicrobial Susceptibility Testing, 26th ed.; Clinical Laboratory Standards Institute: Wayne, PA, USA, 2016; pp. 52–60. [Google Scholar]
- Asselah, T.; Durantel, D.; Pasmant, E.; Lau, G.; Schinazi, R.F. COVID-19: Discovery, Diagnostics and Drug Development. J. Hepatol. 2021, 74, 168–184. [Google Scholar] [CrossRef]
- Killien, E.Y.; Mills, B.; Vavilala, M.S.; Watson, R.S.; O’Keefe, G.E.; Rivara, F.P. Association between Age and Acute Respiratory Distress Syndrome Development and Mortality Following Trauma. J. Trauma Acute Care Surg. 2019, 86, 844–852. [Google Scholar] [CrossRef]
- Fabião, J.; Sassi, B.; Pedrollo, E.F.; Gerchman, F.; Kramer, C.K.; Leitão, C.B.; Pinto, L.C. Why Do Men Have Worse COVID-19-Related Outcomes? A Systematic review and Meta-Analysis with Sex Adjusted for Age. Braz. J. Med. Biol. Res. 2022, 55, e11711. [Google Scholar] [CrossRef]
- Pachpande, V.; Senapathi, S.H.V.; Williams, K.; Chai, S.; Mandal, S.; Prabhu, S. Demographics, Comorbidities, and Laboratory Parameters in Hospitalized Patients with SARS-CoV2 Infection at a Community Hospital in Rural Pennsylvania. PLoS ONE 2022, 17, e0267468. [Google Scholar] [CrossRef] [PubMed]
- Carabelli, A.M.; Peacock, T.P.; Thorne, L.G.; Harvey, W.T.; Hughes, J.; Peacock, S.J.; Barclay, W.S.; de Silva, T.I.; Towers, G.J.; Robertson, D.L.; et al. SARS-CoV-2 Variant Biology: Immune Escape, Transmission and Fitness. Nat. Rev. Microbiol. 2023, 21, 162–177. [Google Scholar] [CrossRef] [PubMed]
- Molinero, M.; Gómez, S.; Benítez, I.D.; Vengoechea, J.J.; González, J.; Polanco, D.; Gort-Paniello, C.; Moncusí-Moix, A.; García-Hidalgo, M.C.; Perez-Pons, M.; et al. Multiplex protein profiling of bronchial aspirates reveals disease-, mortality- and respiratory sequelae-associated signatures in critically ill patients with ARDS secondary to SARS-CoV-2 infection. Front. Immunol. 2022, 13, 942443. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Xu, C.; Zhang, P.; Wang, Y. Associations of Sedentary Time and Physical Activity with Adverse Health Conditions: Outcome-Wide Analyses Using Isotemporal Substitution Model. EClinicalMedicine 2022, 48, 101424. [Google Scholar] [CrossRef] [PubMed]
- Said, K.B.; Alsolami, A.; Alshammari, F.; Alreshidi, F.S.; Fathuldeen, A.; Alrashid, F.; Bashir, A.I.; Osman, S.; Aboras, R.; Alshammari, A.; et al. Selective COVID-19 Coinfections in Diabetic Patients with Concomitant Cardiovascular Comorbidities Are Associated with Increased Mortality. Pathogens 2022, 11, 508. [Google Scholar] [CrossRef] [PubMed]
- Said, K.B.; Alsolami, A.; Moussa, S.; Alfouzan, F.; Bashir, A.I.; Rashidi, M.; Aborans, R.; Taha, T.E.; Almansour, H.; Alazmi, M.; et al. COVID-19 Clinical Profiles and Fatality Rates in Hospitalized Patients Reveal Case Aggravation and Selective Co-Infection by Limited Gram-Negative Bacteria. Int. J. Environ. Res. Public Health 2022, 19, 5270. [Google Scholar] [CrossRef] [PubMed]
- Butowt, R.; von Bartheld, C.S. Anosmia in COVID-19: Underlying Mechanisms and Assessment of an Olfactory Route to Brain Infection. Neuroscientist 2020, 27, 582–603. [Google Scholar] [CrossRef]
- Brann, D.H.; Tsukahara, T.; Weinreb, C.; Lipovsek, M.; Van Den Berge, K.; Gong, B.; Chance, R.; Macaulay, I.C.; Chou, H.J.; Fletcher, R.B.; et al. Non-Neuronal Expression of SARS-CoV-2 Entry Genes in the Olfactory System Suggests Mechanisms Underlying COVID-19-Associated Anosmia. Sci. Adv. 2020, 6, eabc5801. [Google Scholar] [CrossRef]
- Hosoda, T.; Harada, S.; Okamoto, K.; Ishino, S.; Kaneko, M.; Suzuki, M.; Ito, R.; Mizoguchi, M. COVID-19 and Fatal Sepsis Caused by Hypervirulent Klebsiella Pneumoniae, Japan, 2020. Emerg. Infect Dis. 2021, 27, 556. [Google Scholar] [CrossRef]
- Boschiero, M.N.; Duarte, A.; Palamim, C.V.C.; Alvarez, A.E.; Mauch, R.M.; Marson, F.A.L. Frequency of Respiratory Pathogens Other than SARS-CoV-2 Detected during COVID-19 Testing. Diagn. Microbiol. Infect Dis. 2022, 102, 115576. [Google Scholar] [CrossRef]
- Calcagno, A.; Ghisetti, V.; Burdino, E.; Trunfio, M.; Allice, T.; Boglione, L.; Bonora, S.; Di Perri, G. Co-Infection with Other Respiratory Pathogens in COVID-19 Patients. Clin. Microbiol. Infect. 2021, 27, 297–298. [Google Scholar] [CrossRef] [PubMed]
- Aran, D.; Beachler, D.C.; Lanes, S.; Overhage, J.M. Prior Presumed Coronavirus Infection Reduces COVID-19 Risk: A Cohort Study. J. Infect. 2020, 81, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Reche, P.A. Potential Cross-Reactive Immunity to SARS-CoV-2 From Common Human Pathogens and Vaccines. Front. Immunol. 2020, 11, 586984. [Google Scholar] [CrossRef] [PubMed]
- Pezzuto, A.; Tammaro, A.; Tonini, G.; Conforti, G.; Falangone, F.; Spuntarelli, V.; Teggi, A.; Pennica, A. SARS-Cov-2 pneumonia and concurrent myelodysplasia complicated by Pseudomonas aeruginosa over-infection. J. Virol. Methods 2022, 300, 114419. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | p-Value | |||
|---|---|---|---|---|
| ||||
| Mean | Std. Deviation | Std. Error Mean | ||
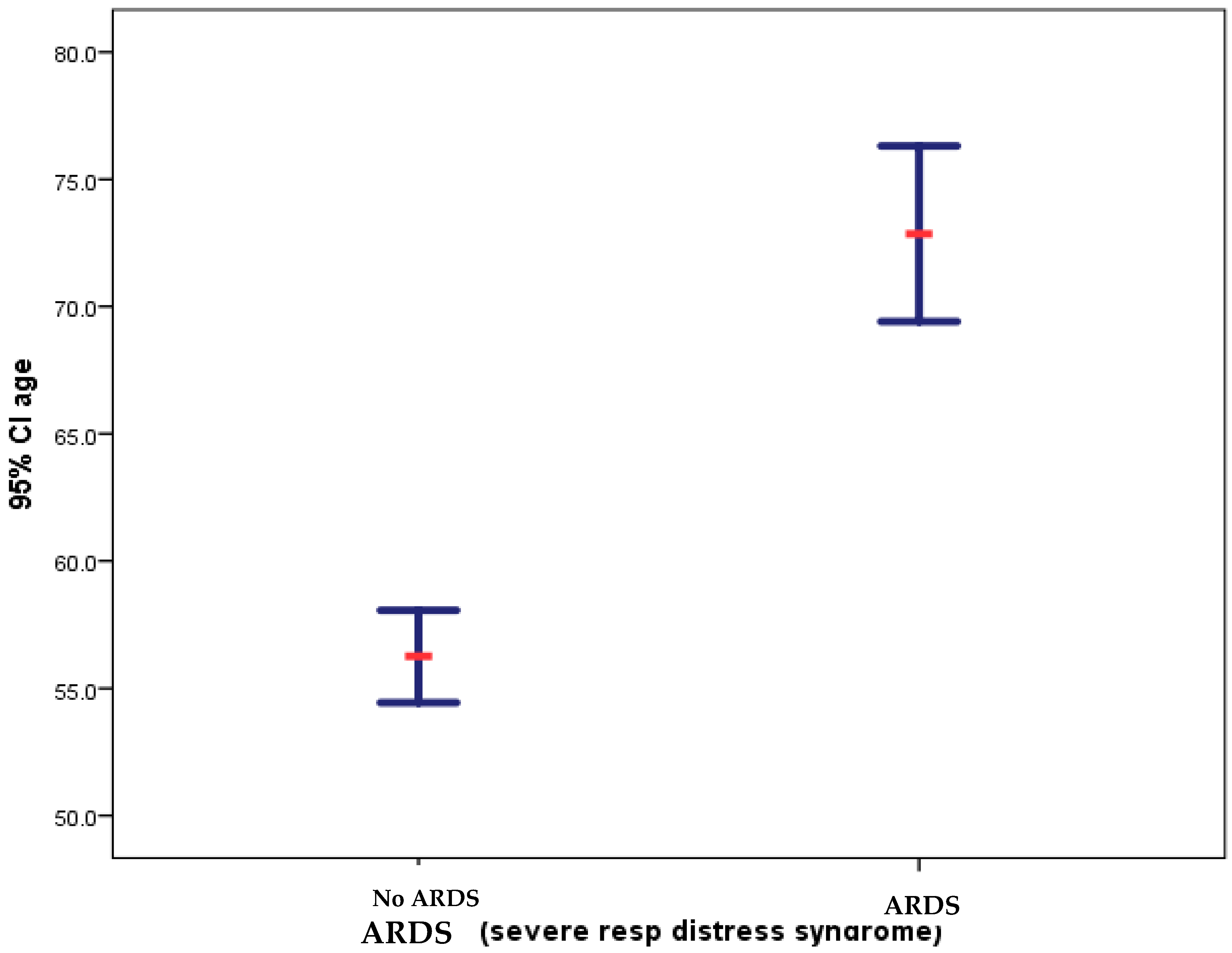
| During COVID-19 (total n = 149) | 57.154 | 15.5058 | 1.2703 | |
| Before COVID-19 (total n = 149) | 58.463 | 15.3286 | 1.2558 | |
| ||||
| Female | Male | p-Value | ||
| During COVID-19 | 50% (n = 68) | 50% (n = 81) | 0.546 | |
| Before COVID-19 | 50% (n = 68) | 50% (n = 81) | ||
| Total | 136 | 162 | ||
| ||||
| Female | Male | Total | p-Value | |
| No ARDS | 91.9% (n = 125) | 89.5% (n = 145) | 90.6% (n = 270) | 0.307 |
| ARDS | 8.1% (n = 11) | 10.5% (n = 17) | 9.4% (n = 28) | |
| Total | 136 | 162 | 298 | |
| ||||
| Female | Male | Total | p-Value | |
| Death | 20.6% (n = 28) | 19.1% (n = 31) | 19.8% (n = 59) | 0.433 |
| Survival | 79.4% (n = 108) | 80.9% (n = 131) | 80.2% (n = 239) | |
| Total | 136 | 162 | 298 | |
| ||||
| No Bacterial co-infection | Bacterial co-infection | p-Value | ||
| No ARDS | 93.8% (n = 120) | 88.2% (n = 150) | 90.6% (n = 270) | 0.77 |
| ARDS | 6.3% (n = 8) | 11.8% (n = 20) | 9.4 (n = 28) | |
| Total | 128 | 170 | 298 | |
| ||||
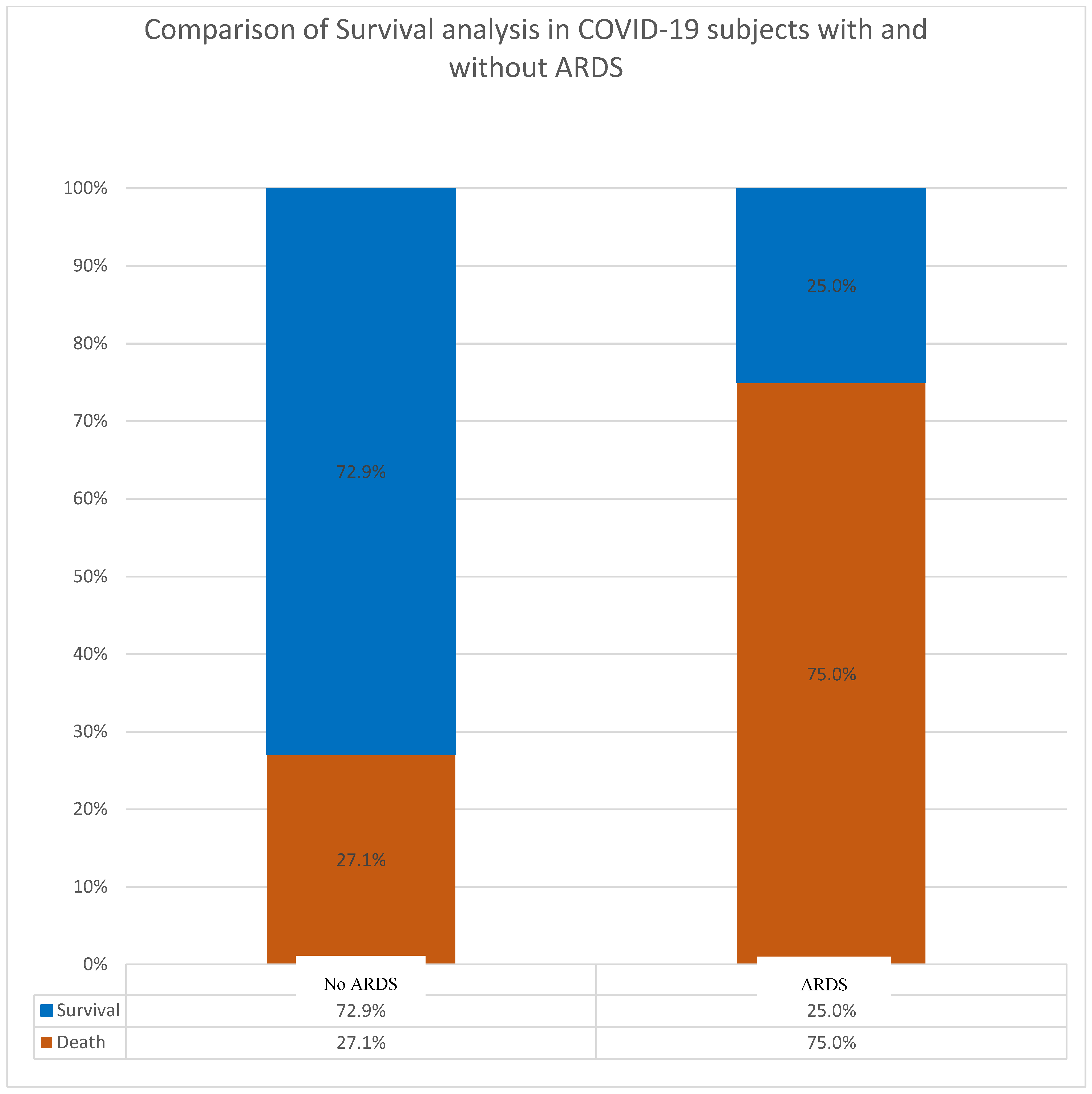
| Death | Survival | Total | ||
| No ARDS | 27.1% (n = 36) | 72.9% (97) | 100% (133) | |
| ARDS | 75.0% (12) | 25.0% (4) | 100% (16) | |
| Total | 32.2% (48) | 67.8% (101) | 100 (149) | |
| ||||
| K. pneuomoniae | A. acinetobacer | E. coli | ||
| Intubations recorded | All were intubated | All were intubated | All were ventilated | |
| Liters oxygen (>4 L) | Variable but much more than 4 | Always much more than 4 | More than 4 | |
| Ventilations recorded | Ventilated before intubation | Ventilated before intubation | Only ventilated | |
| immediate | Mostly immediate | At later stages | |
| <5 (always <3–4) | <5 (always >3–4) | <5 | |
| Yes | Yes | Not conclusive | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, K.B.; Alsolami, A.; Alshammari, K.F.; Alshammari, F.; Alhallabi, S.A.; Alafnan, S.F.; Moussa, S.; Bashir, A.I.; Alshurtan, K.S.; Aboras, R.; et al. A Sequent of Gram-Negative Co-Infectome-Induced Acute Respiratory Distress Syndrome Are Potentially Subtle Aggravators Associated to the SARS-CoV-2 Evolution of Virulence. Diagnostics 2024, 14, 120. https://doi.org/10.3390/diagnostics14010120
Said KB, Alsolami A, Alshammari KF, Alshammari F, Alhallabi SA, Alafnan SF, Moussa S, Bashir AI, Alshurtan KS, Aboras R, et al. A Sequent of Gram-Negative Co-Infectome-Induced Acute Respiratory Distress Syndrome Are Potentially Subtle Aggravators Associated to the SARS-CoV-2 Evolution of Virulence. Diagnostics. 2024; 14(1):120. https://doi.org/10.3390/diagnostics14010120
Chicago/Turabian StyleSaid, Kamaleldin B., Ahmed Alsolami, Khalid F. Alshammari, Fawaz Alshammari, Sulaf A. Alhallabi, Shahad F. Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah S. Alshurtan, Rana Aboras, and et al. 2024. "A Sequent of Gram-Negative Co-Infectome-Induced Acute Respiratory Distress Syndrome Are Potentially Subtle Aggravators Associated to the SARS-CoV-2 Evolution of Virulence" Diagnostics 14, no. 1: 120. https://doi.org/10.3390/diagnostics14010120