
How AI and Robotics Will Advance Interventional Radiology: Narrative Review and Future Perspectives

Abstract
:1. Introduction
2. Application of AI in Interventional Therapy
2.1. Interventional Oncology
2.2. Interventional Neuroradiology
2.2.1. Cerebral Angiography
2.2.2. Intracranial Aneurysms
2.2.3. Acute Ischemic Stroke

{kind=link}
{kind=link}
{kind=link}
| Research | Date | Training Data SET | Method | Aim | Result |
|---|---|---|---|---|---|
| H. Zhao et al. [31] | 2022 | 202 cases from different hospitals | Self-supervised Learning | Utilize deep learning to decrease the number of images required for 3D-DSA reconstruction, thereby minimizing radiation | Generated high-quality 3D-DSA from 202 cases |
| Y. Gao et al. [32] | 2019 | 628 pairs of head data and 690 pairs of leg data | RDB, GAN | Employ deep learning techniques to reduce vascular artifacts | Superior performance in human head and leg tests |
| D. Ueda et al. [33] | 2021 | 608 sequences from 40 patients | DL Model | Generate vascular silhouettes from dynamic angiography using deep learning methods to avoid motion artifacts | Avg PSNR 40.2 dB, SSIM 0.97 |
| Y. Zeng et al. [37] | 2019 | 300 sequences from 263 patients | SIF Method | Train deep learning models with 2D image sequences for IA recognition in 3D-RA, reducing training costs | 98.89% accuracy |
| N. Amigo et al. [39] | 2021 | 71 sequences from 71 patients | ML Algorithms | Automate cerebral aneurysm rupture status classification | RF with the highest accuracy of 0.75 |
| Shiraz Bhurwani et al. [42] | 2022 | 80 sequences from 80 Patients | DNN | Predict the occlusion status of aneurysms post-embolization using APIs and DNN models | Accuracy 78.6%, AUROC 0.77 |
| S. Fujimura et al. [43] | 2023 | 2377 aneurysms in 2215 patients | ML Algorithms | Implement the first coil size selection for IA embolization using AI during the procedure | The ML model achieved 96.7% and 100% accuracy in predicting the size and length |
| Islam. N et al. [49] | 2023 | 5110 instances with twelve attributes | AutoML Model | Generate explainable AI models to predict stroke events | The autoML group has a maximum accuracy of 88.23%, better than the traditional ML group |
| O. Bagcilar et al. [46] | 2023 | 2425 cases from 5 centers | NNDetection | Automate the detection of Large Vessel Occlusion (LVO) and collateral scoring on CTA | 98.26% accuracy |
| B. J. Mittmann et al. [52] | 2022 | 1068 DSA sequences from 260 patients | LSTM, GRU Networks | Automatically distinguish whether thrombectomy in ischemic stroke patients produces new emboli using intraoperative 2D images | Highest MCC 0.77, AUC 0.94 |
2.3. Interventional Cardiology
2.3.1. Coronary Heart Disease
2.3.2. Valvular Heart Disease
| Research | Date | Training Data SET | Method | Aim | Result |
|---|---|---|---|---|---|
| Cong C. et al. [60] | 2023 | 2161 videos from 230 participants | DL | Train auto CAG model to reduce the burden on high-capacity medical centers | Accuracy 0.85, sensitivity 0.96, AUC for LCA and RCA 0.68 and 0.70 |
| Miguel Nobre Menezes [54,55] | 2023 | 117 cases from 90 patients | ML and DL | Using multi-center data to validate the feasibility and reliability of automatic segmentation of CAG images | Results are similar to those from single-center studies, with an accuracy of 99.9% |
| Cho et al. [64] | 2021 | 498 IVUS image sets from 498 patients | DL(CNN) | Train models using IVUS to identify high-risk coronary artery lesions. | Ensemble model sensitivity 80%, specificity 96%, overall accuracy 93% |
| Min et al. [66] | 2021 | 28,952 frames from 515 patients | DL (CNN) and XGBoost | Train IVUS models to predict events of inadequate coronary stent expansion | Accuracy 94%, AUC 0.94 |
| Michal Cohen-Shelly et al. [71] | 2021 | 129,788 cases | DL | Use AI-ECG to detect asymptomatic AS, aiding in early discovery and treatment | AUC 0.85, sensitivity 78%, specificity 74% |
| Moyang Wang et al. [72] | 2023 | 230,486 images from 800 candidates | DL | Build models for pre-TAVR CT evaluation and anatomical risk factor detection | High correlation with senior observers, ICC up to 0.998 |
| Taishi Okuno et al. [74] | 2021 | Clinical and MDCT data from 1492 patients | DL Auto-encoder | Train models using combined clinical and radiological features to predict CVE after TAVR | AUC 0.79 |
| Vien T. et al. [75] | 2023 | Data from 557 patients | ML | Train and evaluate ML models to assess the risk of PPI after TAVR and compare with traditional logistic regression models | RF model AUC 0.81, better than logistic regression model AUC 0.69 |
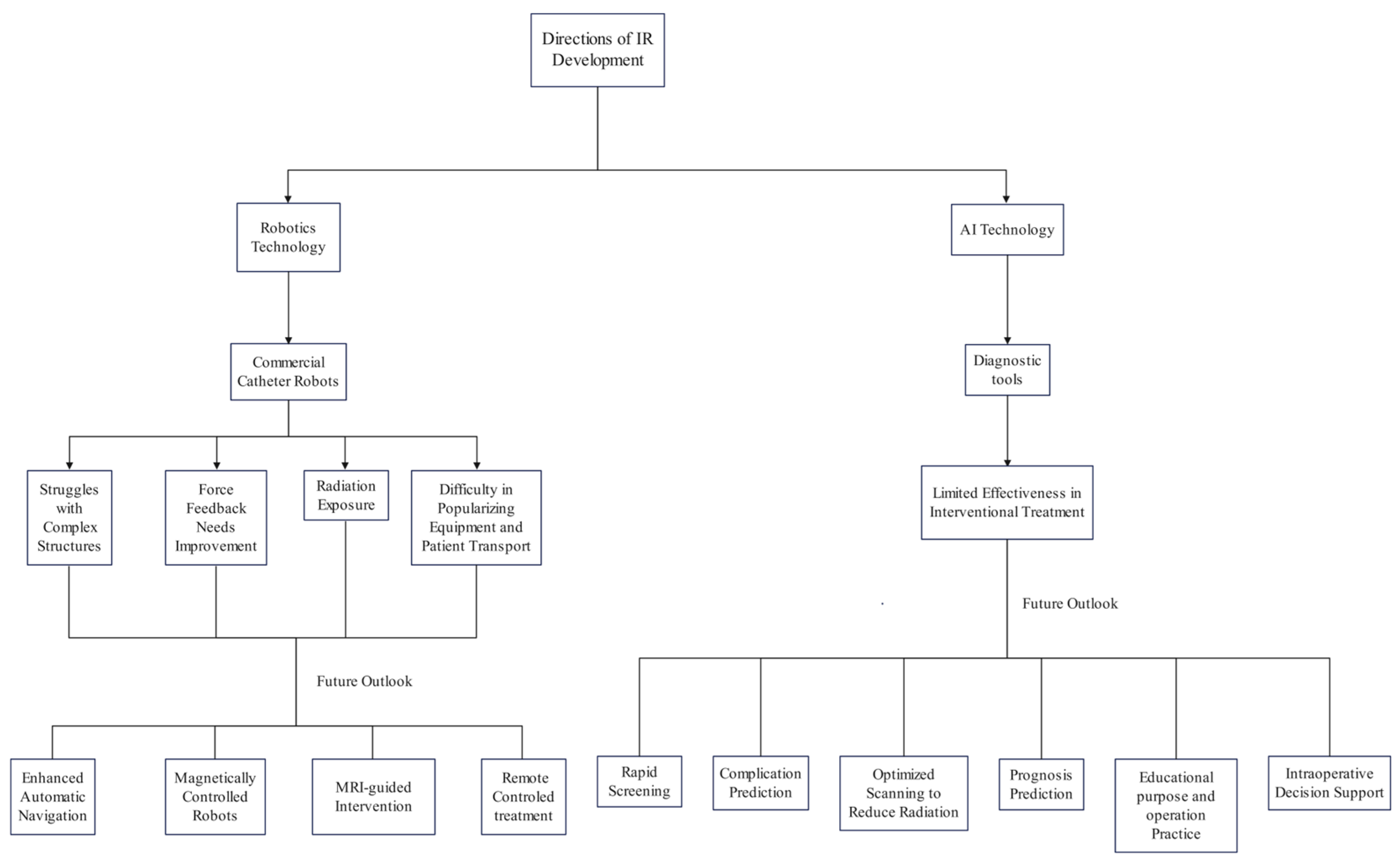
2.4. Development Directions of Interventional AI Application
3. Interventional Robotics and AI
3.1. Development Significance of Interventional Robots
3.2. Existing Interventional Robots
3.3. Development Directions of Interventional Robot
3.3.1. Fully Autonomous Interventional Robots
3.3.2. MRI-Guided Interventional Robotics
3.3.3. Magnetic Controlled Interventional Robotics
- Translating Clinical Needs into Design Specifications: The design process should fully consider specific clinical requirements, such as adjusting the robot’s maximum outer diameter based on the average diameter of the target blood vessel, to ensure that blood flow is not obstructed, thereby avoiding reduced blood flow or stasis.
- Complex Pathway Navigation Ability: The robot should be capable of flexibly navigating through the tortuous and complex pathways of the cardiovascular system, ensuring that it does not damage the blood vessel structure, especially in vessels with arteriosclerosis.
- High Sensitivity and Rapid Response to Magnetic Fields: The robot should be highly sensitive to magnetic fields and capable of rapid responses, enabling intuitive and logical remote operations.
- Good Biocompatibility: Ensure that the robot’s materials and design meet biomedical standards to minimize potential risks to the human body.
- Simplified Recovery and High Reliability: The design should simplify the robot’s recovery process and ensure its high reliability during operations.
- Self-Anchoring Ability: Even in the absence of magnetic field control, the robot should maintain its stability, avoiding displacement or unnecessary damage.
4. Discussion and Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gurgitano, M.; Angileri, S.A.; Rodà, G.M.; Liguori, A.; Pandolfi, M.; Ierardi, A.M.; Wood, B.J.; Carrafiello, G. Interventional Radiology ex-machina: Impact of Artificial Intelligence on practice. Radiol. Med. 2021, 126, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- von Ende, E.; Ryan, S.; Crain, M.A.; Makary, M.S. Artificial Intelligence, Augmented Reality, and Virtual Reality Advances and Applications in Interventional Radiology. Diagnostics 2023, 13, 892. [Google Scholar] [CrossRef] [PubMed]
- Margulis, A.R. Interventional diagnostic radiology—A new subspecialty. Am. J. Roentgenol. 1967, 99, 763–765. [Google Scholar] [CrossRef]
- Wallace, S. Interventional radiology. Cancer 1976, 37, 517–531. [Google Scholar] [CrossRef] [PubMed]
- Sabharwal, T.; Fotiadis, N.; Adam, A. Modern trends in interventional radiology. Br. Med. Bull. 2007, 81–82, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.; Drew, P.J. Artificial intelligence in medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Larentzakis, A.; Lygeros, N. Artificial intelligence (AI) in medicine as a strategic valuable tool. Pan Afr. Med. J. 2021, 38, 184. [Google Scholar] [CrossRef]
- Mintz, Y.; Brodie, R. Introduction to artificial intelligence in medicine. Minim. Invasive Ther. Allied Technol. 2019, 28, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Handelman, G.S.; Kok, H.K.; Chandra, R.V.; Razavi, A.H.; Lee, M.J.; Asadi, H. eDoctor: Machine learning and the future of medicine. J. Intern. Med. 2018, 284, 603–619. [Google Scholar] [CrossRef]
- Xiao, Z.; Ji, D.; Li, F.; Li, Z.; Bao, Z. Application of Artificial Intelligence in Early Gastric Cancer Diagnosis. Digestion 2022, 103, 69–75. [Google Scholar] [CrossRef]
- Viscaino, M.; Torres Bustos, J.; Muñoz, P.; Auat Cheein, C.; Cheein, F.A. Artificial intelligence for the early detection of colorectal cancer: A comprehensive review of its advantages and misconceptions. World J. Gastroenterol. 2021, 27, 6399–6414. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Zeng, B.; Egger, J.; Wang, C.; Smedby, Ö.; Jiang, X.; Chen, X. A review on AI-based medical image computing in head and neck surgery. Phys. Med. Biol. 2022, 67, 17TR01. [Google Scholar] [CrossRef] [PubMed]
- Teuwen, J.; Gouw, Z.A.R.; Sonke, J.J. Artificial Intelligence for Image Registration in Radiation Oncology. Semin. Radiat. Oncol. 2022, 32, 330–342. [Google Scholar] [CrossRef] [PubMed]
- Hasan, F.; Bonatti, J. Robotically assisted percutaneous coronary intervention: Benefits to the patient and the cardiologist. Expert. Rev. Cardiovasc. Ther. 2015, 13, 1165–1168. [Google Scholar] [CrossRef] [PubMed]
- Leal Ghezzi, T.; Campos Corleta, O. 30 Years of Robotic Surgery. World J. Surg. 2016, 40, 2550–2557. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Nakayama, K.I. Artificial intelligence in oncology. Cancer Sci. 2020, 111, 1452–1460. [Google Scholar] [CrossRef]
- Zhang, L.; Jiang, Y.; Jin, Z.; Jiang, W.; Zhang, B.; Wang, C.; Wu, L.; Chen, L.; Chen, Q.; Liu, S.; et al. Real-time automatic prediction of treatment response to transcatheter arterial chemoembolization in patients with hepatocellular carcinoma using deep learning based on digital subtraction angiography videos. Cancer Imaging 2022, 22, 23. [Google Scholar] [CrossRef] [PubMed]
- Abajian, A.; Murali, N.; Savic, L.J.; Laage-Gaupp, F.M.; Nezami, N.; Duncan, J.S.; Schlachter, T.; Lin, M.; Geschwind, J.F.; Chapiro, J. Predicting Treatment Response to Intra-arterial Therapies for Hepatocellular Carcinoma with the Use of Supervised Machine Learning-An Artificial Intelligence Concept. J. Vasc. Interv. Radiol. 2018, 29, 850–857.e851. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.J.; Kim, H.J.; Park, J.H.; Park, D.I.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Kim, M.J. Radiologic response to transcatheter hepatic arterial chemoembolization and clinical outcomes in patients with hepatocellular carcinoma. Liver Int. 2014, 34, 305–312. [Google Scholar] [CrossRef]
- Jin, Z.; Chen, L.; Zhong, B.; Zhou, H.; Zhu, H.; Zhou, H.; Song, J.; Guo, J.; Zhu, X.; Ji, J.; et al. Machine-learning analysis of contrast-enhanced computed tomography radiomics predicts patients with hepatocellular carcinoma who are unsuitable for initial transarterial chemoembolization monotherapy: A multicenter study. Transl. Oncol. 2021, 14, 101034. [Google Scholar] [CrossRef]
- Liu, D.; Liu, F.; Xie, X.; Su, L.; Liu, M.; Xie, X.; Kuang, M.; Huang, G.; Wang, Y.; Zhou, H.; et al. Accurate prediction of responses to transarterial chemoembolization for patients with hepatocellular carcinoma by using artificial intelligence in contrast-enhanced ultrasound. Eur. Radiol. 2020, 30, 2365–2376. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Xu, H.; Ying, X.; Zhang, D.; Lai, L.; Wang, L.; Tu, J.; Ji, J. Radiofrequency Ablation (RFA) Combined with Transcatheter Arterial Chemoembolization (TACE) for Patients with Medium-to-Large Hepatocellular Carcinoma: A Retrospective Analysis of Long-Term Outcome. Med. Sci. Monit. 2020, 26, e923263. [Google Scholar] [CrossRef] [PubMed]
- Xing, S.; Romero, J.C.; Cool, D.W.; Mujoomdar, A.; Chen, E.C.S.; Peters, T.M.; Fenster, A. 3D US-Based Evaluation and Optimization of Tumor Coverage for US-Guided Percutaneous Liver Thermal Ablation. IEEE Trans. Med. Imaging 2022, 41, 3344–3356. [Google Scholar] [CrossRef]
- Wei, W.; Haishan, X.; Alpers, J.; Rak, M.; Hansen, C. A deep learning approach for 2D ultrasound and 3D CT/MR image registration in liver tumor ablation. Comput. Methods Programs Biomed. 2021, 206, 106117. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; He, B.; Hu, Y.; Ren, M.; Chen, Z.; Zhang, Z.; Ma, J.; Ouyang, L.; Chu, H.; Gao, H.; et al. Diagnostic Accuracy of Deep Learning and Radiomics in Lung Cancer Staging: A Systematic Review and Meta-Analysis. Front. Public. Health 2022, 10, 938113. [Google Scholar] [CrossRef]
- Liang, L.; Cool, D.; Kakani, N.; Wang, G.; Ding, H.; Fenster, A. Automatic Radiofrequency Ablation Planning for Liver Tumors With Multiple Constraints Based on Set Covering. IEEE Trans. Med. Imaging 2020, 39, 1459–1471. [Google Scholar] [CrossRef]
- Jiang, B.; Paff, M.; Colby, G.P.; Coon, A.L.; Lin, L.M. Cerebral aneurysm treatment: Modern neurovascular techniques. Stroke Vasc. Neurol. 2016, 1, 93–100. [Google Scholar] [CrossRef]
- Tran, B.X.; Latkin, C.A.; Vu, G.T.; Nguyen, H.L.T.; Nghiem, S.; Tan, M.X.; Lim, Z.K.; Ho, C.S.H.; Ho, R.C.M. The Current Research Landscape of the Application of Artificial Intelligence in Managing Cerebrovascular and Heart Diseases: A Bibliometric and Content Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2699. [Google Scholar] [CrossRef]
- Shlobin, N.A.; Baig, A.A.; Waqas, M.; Patel, T.R.; Dossani, R.H.; Wilson, M.; Cappuzzo, J.M.; Siddiqui, A.H.; Tutino, V.M.; Levy, E.I. Artificial Intelligence for Large-Vessel Occlusion Stroke: A Systematic Review. World Neurosurg. 2022, 159, 207–220.e201. [Google Scholar] [CrossRef]
- Zhang, X.; Deng, Y.; Tian, C.; Chen, S.; Wang, Y.; Zhang, M.; Wang, Q.; Liao, X.; Si, W. Enhancing the depth perception of DSA images with 2D-3D registration. Front. Neurol. 2023, 14, 1122021. [Google Scholar] [CrossRef]
- Zhao, H.; Zhou, Z.; Wu, F.; Xiang, D.; Zhao, H.; Zhang, W.; Li, L.; Li, Z.; Huang, J.; Hu, H.; et al. Self-supervised learning enables 3D digital subtraction angiography reconstruction from ultra-sparse 2D projection views: A multicenter study. Cell Rep. Med. 2022, 3, 100775. [Google Scholar] [CrossRef]
- Gao, Y.; Song, Y.; Yin, X.; Wu, W.; Zhang, L.; Chen, Y.; Shi, W. Deep learning-based digital subtraction angiography image generation. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1775–1784. [Google Scholar] [CrossRef]
- Ueda, D.; Katayama, Y.; Yamamoto, A.; Ichinose, T.; Arima, H.; Watanabe, Y.; Walston, S.L.; Tatekawa, H.; Takita, H.; Honjo, T.; et al. Deep Learning-based Angiogram Generation Model for Cerebral Angiography without Misregistration Artifacts. Radiology 2021, 299, 675–681. [Google Scholar] [CrossRef]
- Chalouhi, N.; Hoh, B.L.; Hasan, D. Review of cerebral aneurysm formation, growth, and rupture. Stroke 2013, 44, 3613–3622. [Google Scholar] [CrossRef]
- Ajiboye, N.; Chalouhi, N.; Starke, R.M.; Zanaty, M.; Bell, R. Unruptured Cerebral Aneurysms: Evaluation and Management. Sci. World J. 2015, 2015, 954954. [Google Scholar] [CrossRef]
- Feng, Y.; Shu, S.J. Diagnostic Value of Low-Dose 256-Slice Spiral CT Angiography, MR Angiography, and 3D-DSA in Cerebral Aneurysms. Dis. Markers 2020, 2020, 8536471. [Google Scholar] [CrossRef]
- Zeng, Y.; Liu, X.; Xiao, N.; Li, Y.; Jiang, Y.; Feng, J.; Guo, S. Automatic Diagnosis Based on Spatial Information Fusion Feature for Intracranial Aneurysm. IEEE Trans. Med. Imaging 2020, 39, 1448–1458. [Google Scholar] [CrossRef]
- Nafees Ahmed, S.; Prakasam, P. A systematic review on intracranial aneurysm and hemorrhage detection using machine learning and deep learning techniques. Prog. Biophys. Mol. Biol. 2023, 183, 1–16. [Google Scholar] [CrossRef]
- Amigo, N.; Valencia, A.; Wu, W.; Patnaik, S.; Finol, E. Cerebral aneurysm rupture status classification using statistical and machine learning methods. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2021, 235, 655–662. [Google Scholar] [CrossRef]
- Chancellor, B.; Raz, E.; Shapiro, M.; Tanweer, O.; Nossek, E.; Riina, H.A.; Nelson, P.K. Flow Diversion for Intracranial Aneurysm Treatment: Trials Involving Flow Diverters and Long-Term Outcomes. Neurosurgery 2020, 86, S36–S45. [Google Scholar] [CrossRef]
- Ghaith, A.K.; Greco, E.; Rios-Zermeno, J.; El-Hajj, V.G.; Perez-Vega, C.; Ghanem, M.; Kashyap, S.; Fox, W.C.; Huynh, T.J.; Sandhu, S.S.; et al. Safety and efficacy of the pipeline embolization device for treatment of small vs. large aneurysms: A systematic review and meta-analysis. Neurosurg. Rev. 2023, 46, 284. [Google Scholar] [CrossRef]
- Wisniewski, A.G.; Shiraz Bhurwani, M.M.; Sommer, K.N.; Monteiro, A.; Baig, A.; Davies, J.; Siddiqui, A.; Ionita, C.N. Quantitative angiography prognosis of intracranial aneurysm treatment failure using parametric imaging and distal vessel analysis. Proc. SPIE Int. Soc. Opt. Eng. 2022, 12036, 86–95. [Google Scholar] [CrossRef]
- Fujimura, S.; Koshiba, T.; Kudo, G.; Takeshita, K.; Kazama, M.; Karagiozov, K.; Fukudome, K.; Takao, H.; Ohwada, H.; Murayama, Y.; et al. Development of Machine Learning Model for Selecting the 1st Coil in the Treatment of Cerebral Aneurysms by Coil Embolization. In Proceedings of the 2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Sydney, Australia, 24–27 July 2023; pp. 1–4. [Google Scholar]
- Ferreti, L.A.; Leitao, C.A.; Teixeira, B.C.A.; Lopes Neto, F.D.N.; Zétola, V.F.; Lange, M.C. The use of e-ASPECTS in acute stroke care: Validation of method performance compared to the performance of specialists. Arq. Neuropsiquiatr. 2020, 78, 757–761. [Google Scholar] [CrossRef]
- Soun, J.E.; Chow, D.S.; Nagamine, M.; Takhtawala, R.S.; Filippi, C.G.; Yu, W.; Chang, P.D. Artificial Intelligence and Acute Stroke Imaging. AJNR Am. J. Neuroradiol. 2021, 42, 2–11. [Google Scholar] [CrossRef]
- Bagcilar, O.; Alis, D.; Alis, C.; Seker, M.E.; Yergin, M.; Ustundag, A.; Hikmet, E.; Tezcan, A.; Polat, G.; Akkus, A.T.; et al. Automated LVO detection and collateral scoring on CTA using a 3D self-configuring object detection network: A multi-center study. Sci. Rep. 2023, 13, 8834. [Google Scholar] [CrossRef]
- Grunwald, I.Q.; Kulikovski, J.; Reith, W.; Gerry, S.; Namias, R.; Politi, M.; Papanagiotou, P.; Essig, M.; Mathur, S.; Joly, O.; et al. Collateral Automation for Triage in Stroke: Evaluating Automated Scoring of Collaterals in Acute Stroke on Computed Tomography Scans. Cerebrovasc. Dis. 2019, 47, 217–222. [Google Scholar] [CrossRef]
- McLouth, J.; Elstrott, S.; Chaibi, Y.; Quenet, S.; Chang, P.D.; Chow, D.S.; Soun, J.E. Validation of a Deep Learning Tool in the Detection of Intracranial Hemorrhage and Large Vessel Occlusion. Front. Neurol. 2021, 12, 656112. [Google Scholar] [CrossRef]
- Islam, N.; Kibria, H.B. Enhancing Stroke Prediction through Interpretable AI: Distinguishing Stroke Cases from Non-Stroke Cases. In Proceedings of the 2023 6th International Conference on Electrical Information and Communication Technology (EICT), Khulna, Bangladesh, 7–9 December 2023; pp. 1–6. [Google Scholar]
- Balami, J.S.; White, P.M.; McMeekin, P.J.; Ford, G.A.; Buchan, A.M. Complications of endovascular treatment for acute ischemic stroke: Prevention and management. Int. J. Stroke 2018, 13, 348–361. [Google Scholar] [CrossRef]
- Krishnan, R.; Mays, W.; Elijovich, L. Complications of Mechanical Thrombectomy in Acute Ischemic Stroke. Neurology 2021, 97, S115–S125. [Google Scholar] [CrossRef]
- Mittmann, B.J.; Braun, M.; Runck, F.; Schmitz, B.; Tran, T.N.; Yamlahi, A.; Maier-Hein, L.; Franz, A.M. Deep learning-based classification of DSA image sequences of patients with acute ischemic stroke. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 1633–1641. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Nobre Menezes, M.; Lourenço-Silva, J.; Silva, B.; Rodrigues, O.; Francisco, A.R.G.; Carrilho Ferreira, P.; Oliveira, A.L.; Pinto, F.J. Development of deep learning segmentation models for coronary X-ray angiography: Quality assessment by a new global segmentation score and comparison with human performance. Rev. Port. Cardiol. 2022, 41, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Nobre Menezes, M.; Silva, J.L.; Silva, B.; Rodrigues, T.; Guerreiro, C.; Guedes, J.P.; Santos, M.O.; Oliveira, A.L.; Pinto, F.J. Coronary X-ray angiography segmentation using Artificial Intelligence: A multicentric validation study of a deep learning model. Int. J. Cardiovasc. Imaging 2023, 39, 1385–1396. [Google Scholar] [CrossRef]
- Wu, W.; Zhang, J.; Xie, H.; Zhao, Y.; Zhang, S.; Gu, L. Automatic detection of coronary artery stenosis by convolutional neural network with temporal constraint. Comput. Biol. Med. 2020, 118, 103657. [Google Scholar] [CrossRef] [PubMed]
- Danilov, V.V.; Klyshnikov, K.Y.; Gerget, O.M.; Kutikhin, A.G.; Ganyukov, V.I.; Frangi, A.F.; Ovcharenko, E.A. Real-time coronary artery stenosis detection based on modern neural networks. Sci. Rep. 2021, 11, 7582. [Google Scholar] [CrossRef]
- Pang, K.; Ai, D.; Fang, H.; Fan, J.; Song, H.; Yang, J. Stenosis-DetNet: Sequence consistency-based stenosis detection for X-ray coronary angiography. Comput. Med. Imaging Graph. 2021, 89, 101900. [Google Scholar] [CrossRef]
- Zhao, C.; Vij, A.; Malhotra, S.; Tang, J.; Tang, H.; Pienta, D.; Xu, Z.; Zhou, W. Automatic extraction and stenosis evaluation of coronary arteries in invasive coronary angiograms. Comput. Biol. Med. 2021, 136, 104667. [Google Scholar] [CrossRef]
- Cong, C.; Kato, Y.; Vasconcellos, H.D.; Ostovaneh, M.R.; Lima, J.A.C.; Ambale-Venkatesh, B. Deep learning-based end-to-end automated stenosis classification and localization on catheter coronary angiography. Front. Cardiovasc. Med. 2023, 10, 944135. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, X.; Wan, W.; Liu, S.; Liu, Y.; Liu, H.; Zeng, X.; Zhang, Q. Two new stenosis detection methods of coronary angiograms. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 521–530. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Kuku, K.O.; Waksman, R.; Garcia-Garcia, H.M. Intravascular ultrasound-guided drug-eluting stent implantation. Minerva Cardioangiol. 2019, 67, 306–317. [Google Scholar] [CrossRef]
- Oosterveer, T.T.M.; van der Meer, S.M.; Scherptong, R.W.C.; Jukema, J.W. Optical Coherence Tomography: Current Applications for the Assessment of Coronary Artery Disease and Guidance of Percutaneous Coronary Interventions. Cardiol. Ther. 2020, 9, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Kang, S.J.; Min, H.S.; Lee, J.G.; Kim, W.J.; Kang, S.H.; Kang, D.Y.; Lee, P.H.; Ahn, J.M.; Park, D.W.; et al. Intravascular ultrasound-based deep learning for plaque characterization in coronary artery disease. Atherosclerosis 2021, 324, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Witzenbichler, B.; Maehara, A.; Weisz, G.; Neumann, F.-J.; Rinaldi, M.J.; Metzger, D.C.; Henry, T.D.; Cox, D.A.; Duffy, P.L.; Brodie, B.R.; et al. Relationship Between Intravascular Ultrasound Guidance and Clinical Outcomes After Drug-Eluting Stents. Circulation 2014, 129, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Min, H.S.; Ryu, D.; Kang, S.J.; Lee, J.G.; Yoo, J.H.; Cho, H.; Kang, D.Y.; Lee, P.H.; Ahn, J.M.; Park, D.W.; et al. Prediction of Coronary Stent Underexpansion by Pre-Procedural Intravascular Ultrasound-Based Deep Learning. JACC Cardiovasc. Interv. 2021, 14, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.J.; Cho, Y.R.; Park, G.M.; Ahn, J.M.; Han, S.B.; Lee, J.Y.; Kim, W.J.; Park, D.W.; Lee, S.W.; Kim, Y.H.; et al. Predictors for functionally significant in-stent restenosis: An integrated analysis using coronary angiography, IVUS, and myocardial perfusion imaging. JACC Cardiovasc. Imaging 2013, 6, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Coffey, S.; Roberts-Thomson, R.; Brown, A.; Carapetis, J.; Chen, M.; Enriquez-Sarano, M.; Zuhlke, L.; Prendergast, B.D. Global epidemiology of valvular heart disease. Nat. Rev. Cardiol. 2021, 18, 853–864. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef]
- Mc Morrow, R.; Kriza, C.; Urbán, P.; Amenta, V.; Amaro, J.A.B.; Panidis, D.; Chassaigne, H.; Griesinger, C.B. Assessing the safety and efficacy of TAVR compared to SAVR in low-to-intermediate surgical risk patients with aortic valve stenosis: An overview of reviews. Int. J. Cardiol. 2020, 314, 43–53. [Google Scholar] [CrossRef]
- Cohen-Shelly, M.; Attia, Z.I.; Friedman, P.A.; Ito, S.; Essayagh, B.A.; Ko, W.Y.; Murphree, D.H.; Michelena, H.I.; Enriquez-Sarano, M.; Carter, R.E.; et al. Electrocardiogram screening for aortic valve stenosis using artificial intelligence. Eur. Heart J. 2021, 42, 2885–2896. [Google Scholar] [CrossRef]
- Wang, M.; Niu, G.; Chen, Y.; Zhou, Z.; Feng, D.; Zhang, Y.; Wu, Y.; Wu, Y.; Wang, M.; Song, G.; et al. Development and validation of a deep learning-based fully automated algorithm for pre-TAVR CT assessment of the aortic valvular complex and detection of anatomical risk factors: A retrospective, multicentre study. eBioMedicine 2023, 96, 104794. [Google Scholar] [CrossRef]
- Maier, O.; Bosbach, G.; Piayda, K.; Afzal, S.; Polzin, A.; Westenfeld, R.; Jung, C.; Kelm, M.; Zeus, T.; Veulemans, V. Cerebrovascular Events after Transcatheter Aortic Valve Replacement: The Difficulty in Predicting the Unpredictable. J. Clin. Med. 2022, 11, 3902. [Google Scholar] [CrossRef] [PubMed]
- Okuno, T.; Overtchouk, P.; Asami, M.; Tomii, D.; Stortecky, S.; Praz, F.; Lanz, J.; Siontis, G.C.M.; Grani, C.; Windecker, S.; et al. Deep learning-based prediction of early cerebrovascular events after transcatheter aortic valve replacement. Sci. Rep. 2021, 11, 18754. [Google Scholar] [CrossRef] [PubMed]
- Truong, V.T.; Beyerbach, D.; Mazur, W.; Wigle, M.; Bateman, E.; Pallerla, A.; Ngo, T.N.M.; Shreenivas, S.; Tretter, J.T.; Palmer, C.; et al. Machine learning method for predicting pacemaker implantation following transcatheter aortic valve replacement. Pacing Clin. Electrophysiol. 2021, 44, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, T.; Al-Kindi, S.; Nadeem, F.; Attizzani, G.F.; Elgudin, Y.; Markowitz, A.; Costa, M.A.; Simon, D.I.; Arruda, M.S.; Mackall, J.A.; et al. Machine Learning Algorithms for Prediction of Permanent Pacemaker Implantation After Transcatheter Aortic Valve Replacement. Circ. Arrhythm. Electrophysiol. 2021, 14, e008941. [Google Scholar] [CrossRef] [PubMed]
- Joseph, F.J.; Vanluchene, H.E.R.; Bervini, D. Simulation training approaches in intracranial aneurysm surgery-a systematic review. Neurosurg. Rev. 2023, 46, 101. [Google Scholar] [CrossRef]
- Hashimoto, D.A.; Rosman, G.; Witkowski, E.R.; Stafford, C.; Navarette-Welton, A.J.; Rattner, D.W.; Lillemoe, K.D.; Rus, D.L.; Meireles, O.R. Computer Vision Analysis of Intraoperative Video: Automated Recognition of Operative Steps in Laparoscopic Sleeve Gastrectomy. Ann. Surg. 2019, 270, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Pangal, D.J.; Kugener, G.; Shahrestani, S.; Attenello, F.; Zada, G.; Donoho, D.A. A Guide to Annotation of Neurosurgical Intraoperative Video for Machine Learning Analysis and Computer Vision. World Neurosurg. 2021, 150, 26–30. [Google Scholar] [CrossRef]
- Fischer, E.; Jawed, K.J.; Cleary, K.; Balu, A.; Donoho, A.; Thompson Gestrich, W.; Donoho, D.A. A methodology for the annotation of surgical videos for supervised machine learning applications. Int. J. Comput. Assist. Radiol. Surg. 2023, 18, 1673–1678. [Google Scholar] [CrossRef]
- Wagner, M.; Müller-Stich, B.P.; Kisilenko, A.; Tran, D.; Heger, P.; Mündermann, L.; Lubotsky, D.M.; Müller, B.; Davitashvili, T.; Capek, M.; et al. Comparative validation of machine learning algorithms for surgical workflow and skill analysis with the HeiChole benchmark. Med. Image Anal. 2023, 86, 102770. [Google Scholar] [CrossRef]
- Barba, P.; Stramiello, J.; Funk, E.K.; Richter, F.; Yip, M.C.; Orosco, R.K. Remote telesurgery in humans: A systematic review. Surg. Endosc. 2022, 36, 2771–2777. [Google Scholar] [CrossRef]
- Duan, W.; Li, Z.; Omisore, O.M.; Du, W.; Akinyemi, T.O.; Chen, X.; Gao, X.; Wang, H.; Wang, L. Development of an Intuitive Interface with Haptic Enhancement for Robot-Assisted Endovascular Intervention. IEEE Trans. Haptics 2023, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bidgoli, M.Z.; Pouya, M.H.; Pishkenari, H.N.; Taheri, A. Design of Fuzzy controller for position control of a magnetic catheter in uniform magnetic fields. In Proceedings of the 2023 11th RSI International Conference on Robotics and Mechatronics (ICRoM), Tehran, Iran, 19–21 December 2023; pp. 390–395. [Google Scholar]
- Venkatesh, S.; Narasimhan, K.; Adalarasu, K. An Overview of Interpretability Techniques for Explainable Artificial Intelligence (XAI) In Deep Learning-Based Medical Image Analysis. In Proceedings of the 2023 9th International Conference on Advanced Computing and Communication Systems (ICACCS), Coimbatore, India, 17–18 March 2023; pp. 175–182. [Google Scholar]
- Song, H.; Kim, S. Explainable artificial intelligence (XAI): How to make image analysis deep learning models transparent. In Proceedings of the 2022 22nd International Conference on Control, Automation and Systems (ICCAS), Jeju, Korea, 27 November–1 December 2022; pp. 1595–1598. [Google Scholar]
- Sajja, K.C.; Sweid, A.; Al Saiegh, F.; Chalouhi, N.; Avery, M.B.; Schmidt, R.F.; Tjoumakaris, S.I.; Gooch, M.R.; Herial, N.; Abbas, R.; et al. Endovascular robotic: Feasibility and proof of principle for diagnostic cerebral angiography and carotid artery stenting. J. Neurointerv. Surg. 2020, 12, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Najafi, G.; Kreiser, K.; Abdelaziz, M.; Hamady, M.S. Current State of Robotics in Interventional Radiology. Cardiovasc. Interv. Radiol. 2023, 46, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Pancholy, S.B.; Shah, S.C.; Patel, T.M. Safety and Efficacy of Robotic-Assisted PCI. Curr. Cardiol. Rep. 2022, 24, 817–821. [Google Scholar] [CrossRef] [PubMed]
- Crinnion, W.; Jackson, B.; Sood, A.; Lynch, J.; Bergeles, C.; Liu, H.; Rhode, K.; Mendes Pereira, V.; Booth, T.C. Robotics in neurointerventional surgery: A systematic review of the literature. J. Neurointerv. Surg. 2022, 14, 539–545. [Google Scholar] [CrossRef]
- Temming, S.; Kocher, M.; Stoelben, E.; Hagmeyer, L.; Chang, D.H.; Frank, K.; Hekmat, K.; Wolf, J.; Baus, W.W.; Semrau, R.; et al. Risk-adapted robotic stereotactic body radiation therapy for inoperable early-stage non-small-cell lung cancer. Strahlenther. Onkol. 2018, 194, 91–97. [Google Scholar] [CrossRef] [PubMed]
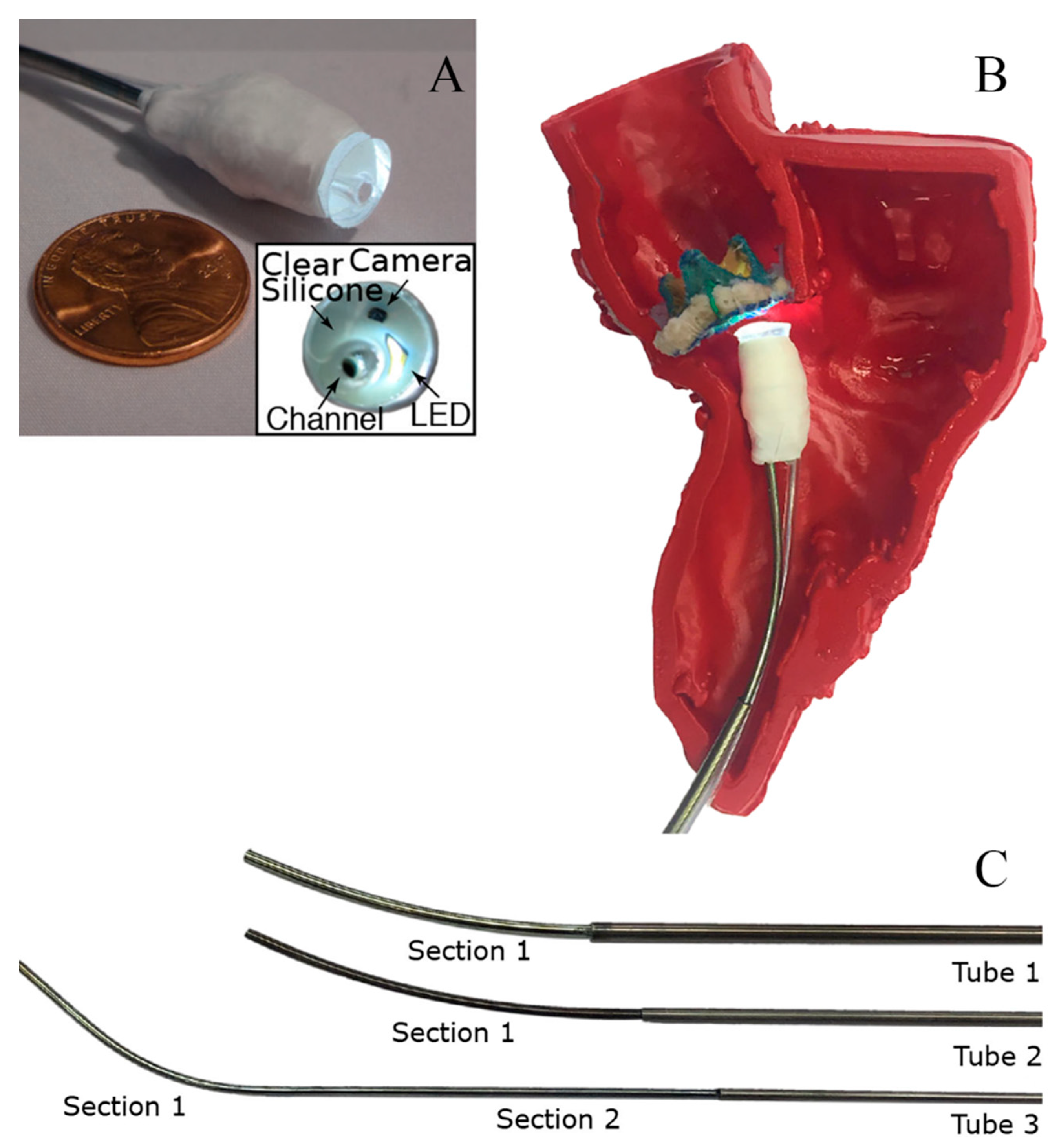
- Fagogenis, G.; Mencattelli, M.; Machaidze, Z.; Rosa, B.; Price, K.; Wu, F.; Weixler, V.; Saeed, M.; Mayer, J.E.; Dupont, P.E. Autonomous Robotic Intracardiac Catheter Navigation Using Haptic Vision. Sci. Robot. 2019, 4, eaaw1977. [Google Scholar] [CrossRef]
- Ziegler, A.; Christiansen, E.; Kriegman, D.; Belongie, S. Locally uniform comparison image descriptor. Adv. Neural Inf. Process. Syst. 2012, 25, 1–9. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Park, U.; Jain, A.K. Face Matching and Retrieval Using Soft Biometrics. IEEE Trans. Inf. Forensics Secur. 2010, 5, 406–415. [Google Scholar] [CrossRef]
- Taigman, Y.; Yang, M.; Ranzato, M.A.; Wolf, L. Deepface: Closing the gap to human-level performance in face verification. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 1701–1708. [Google Scholar]
- Zhao, Z.; Cai, T.; Chang, F.; Cheng, X. Real-time surgical instrument detection in robot-assisted surgery using a convolutional neural network cascade. Healthc. Technol. Lett. 2019, 6, 275–279. [Google Scholar] [CrossRef]
- Lee, D.; Yu, H.W.; Kwon, H.; Kong, H.J.; Lee, K.E.; Kim, H.C. Evaluation of Surgical Skills during Robotic Surgery by Deep Learning-Based Multiple Surgical Instrument Tracking in Training and Actual Operations. J. Clin. Med. 2020, 9, 1964. [Google Scholar] [CrossRef]
- Kirillov, A.; Mintun, E.; Ravi, N.; Mao, H.; Rolland, C.; Gustafson, L.; Xiao, T.; Whitehead, S.; Berg, A.C.; Lo, W.-Y.; et al. Segment Anything. In Proceedings of the IEEE/CVF International Conference on Computer Vision (ICCV), Paris, France, 2–6 October 2023. [Google Scholar]
- Tang, H.; Bober, R.R.; Zhao, C.; Zhang, C.; Zhu, H.; He, Z.; Xu, Z.; Zhou, W. 3D fusion between fluoroscopy angiograms and SPECT myocardial perfusion images to guide percutaneous coronary intervention. J. Nucl. Cardiol. 2022, 29, 1870–1884. [Google Scholar] [CrossRef]
- Campbell-Washburn, A.E.; Tavallaei, M.A.; Pop, M.; Grant, E.K.; Chubb, H.; Rhode, K.; Wright, G.A. Real-time MRI guidance of cardiac interventions. J. Magn. Reson. Imaging 2017, 46, 935–950. [Google Scholar] [CrossRef]
- Ozturk, C.; Guttman, M.; McVeigh, E.R.; Lederman, R.J. Magnetic Resonance Imaging-guided Vascular Interventions. Top. Magn. Reson. Imaging 2005, 16, 369–381. [Google Scholar] [CrossRef]
- Liu, C.Y.; Farahani, K.; Lu, D.S.; Duckwiler, G.; Oppelt, A. Safety of MRI-guided endovascular guidewire applications. J. Magn. Reson. Imaging 2000, 12, 75–78. [Google Scholar] [CrossRef]
- Wacker, F.K.; Hillenbrand, C.M.; Duerk, J.L.; Lewin, J.S. MR-guided endovascular interventions: Device visualization, tracking, navigation, clinical applications, and safety aspects. Magn. Reson. Imaging Clin. N. Am. 2005, 13, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Schleicher, K.E.; Bock, M.; During, K.; Kroboth, S.; Krafft, A.J. Radial MRI with variable echo times: Reducing the orientation dependency of susceptibility artifacts of an MR-safe guidewire. MAGMA 2018, 31, 235–242. [Google Scholar] [CrossRef]
- Lee, K.H.; Fu, K.C.D.; Guo, Z.; Dong, Z.; Leong, M.C.W.; Cheung, C.L.; Lee, A.P.W.; Luk, W.; Kwok, K.W. MR Safe Robotic Manipulator for MRI-Guided Intracardiac Catheterization. IEEE/ASME Trans. Mechatron. 2018, 23, 586–595. [Google Scholar] [CrossRef]
- Abdelaziz, M.E.M.K.; Kundrat, D.; Pupillo, M.; Dagnino, G.; Kwok, T.M.Y.; Chi, W.; Groenhuis, V.; Siepel, F.J.; Riga, C.; Stramigioli, S.; et al. Toward a Versatile Robotic Platform for Fluoroscopy and MRI-Guided Endovascular Interventions: A Pre-Clinical Study. In Proceedings of the 2019 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Macau, China, 3–8 November 2019; pp. 5411–5418. [Google Scholar]
- Tavallaei, M.A.; Lavdas, M.K.; Gelman, D.; Drangova, M. Magnetic resonance imaging compatible remote catheter navigation system with 3 degrees of freedom. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Sun, Z.; Zhang, J.; Zhang, J.; Zheng, J.; Qian, F. A Novel Remote-Controlled Vascular Interventional Robotic System Based on Hollow Ultrasonic Motor. Micromachines 2022, 13, 410. [Google Scholar] [CrossRef]
- Stoianovici, D.; Kim, C.; Petrisor, D.; Jun, C.; Lim, S.; Ball, M.W.; Ross, A.; Macura, K.J.; Allaf, M. MR Safe Robot, FDA Clearance, Safety and Feasibility Prostate Biopsy Clinical Trial. IEEE ASME Trans. Mechatron. 2017, 22, 115–126. [Google Scholar] [CrossRef]
- Datta, G. Broken guidewire–a tale of three cases. Indian Heart J. 2015, 67, S49–S52. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Yang, L.; Zhang, M.; Wang, Q.; Yu, S.C.H.; Zhang, L. Magnetic Control of a Steerable Guidewire Under Ultrasound Guidance Using Mobile Electromagnets. IEEE Robot. Autom. Lett. 2021, 6, 1280–1287. [Google Scholar] [CrossRef]
- Lee, W.; Nam, J.; Kim, J.; Jung, E.; Kim, N.; Jang, G. Steering, Tunneling, and Stent Delivery of a Multifunctional Magnetic Catheter Robot to Treat Occlusive Vascular Disease. IEEE Trans. Ind. Electron. 2021, 68, 391–400. [Google Scholar] [CrossRef]
- Zhang, S.; Yin, M.; Lai, Z.; Huang, C.; Wang, C.; Shang, W.; Wu, X.; Zhang, Y.; Xu, T. Design and Characteristics of 3D Magnetically Steerable Guidewire System for Minimally Invasive Surgery. IEEE Robot. Autom. Lett. 2022, 7, 4040–4046. [Google Scholar] [CrossRef]
- Wang, T.; Ugurlu, H.; Yan, Y.; Li, M.; Li, M.; Wild, A.M.; Yildiz, E.; Schneider, M.; Sheehan, D.; Hu, W.; et al. Adaptive wireless millirobotic locomotion into distal vasculature. Nat. Commun. 2022, 13, 4465. [Google Scholar] [CrossRef]
- Sa, J.; Park, J.; Jung, E.; Kim, N.; Lee, D.; Bae, S.; Lee, Y.; Jang, G. Separable and Recombinable Magnetic Robot for Robotic Endovascular Intervention. IEEE Robot. Autom. Lett. 2023, 8, 1881–1888. [Google Scholar] [CrossRef]
- Rodgers, B.; Rodgers, K.A.; Chick, J.F.B.; Makary, M.S. Public Awareness of Interventional Radiology: Population-Based Analysis of the Current State of and Pathways for Improvement. J. Vasc. Interv. Radiol. 2023, 34, 960–967.e966. [Google Scholar] [CrossRef]
- Kurakin, A.; Goodfellow, I.; Bengio, S. Adversarial machine learning at scale. arXiv 2016, arXiv:1611.01236. [Google Scholar]
- Haug, C.J. Turning the tables—The new European general data protection regulation. N. Engl. J. Med. 2018, 379, 207–209. [Google Scholar] [CrossRef]
- Khalid, N.; Qayyum, A.; Bilal, M.; Al-Fuqaha, A.; Qadir, J. Privacy-preserving artificial intelligence in healthcare: Techniques and applications. Comput. Biol. Med. 2023, 158, 106848. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, Z.M. Ethics and governance of trustworthy medical artificial intelligence. BMC Med. Inform. Decis. Mak. 2023, 23, 7. [Google Scholar] [CrossRef]
- Petersen, S.E.; Abdulkareem, M.; Leiner, T. Artificial Intelligence Will Transform Cardiac Imaging-Opportunities and Challenges. Front. Cardiovasc. Med. 2019, 6, 133. [Google Scholar] [CrossRef]
- van der Velden, B.H.M.; Kuijf, H.J.; Gilhuijs, K.G.A.; Viergever, M.A. Explainable artificial intelligence (XAI) in deep learning-based medical image analysis. Med. Image Anal. 2022, 79, 102470. [Google Scholar] [CrossRef]
- O’Sullivan, S.; Nevejans, N.; Allen, C.; Blyth, A.; Leonard, S.; Pagallo, U.; Holzinger, K.; Holzinger, A.; Sajid, M.I.; Ashrafian, H. Legal, regulatory, and ethical frameworks for development of standards in artificial intelligence (AI) and autonomous robotic surgery. Int. J. Med. Robot. 2019, 15, e1968. [Google Scholar] [CrossRef] [PubMed]
- Geis, J.R.; Brady, A.; Wu, C.C.; Spencer, J.; Ranschaert, E.; Jaremko, J.L.; Langer, S.G.; Kitts, A.B.; Birch, J.; Shields, W.F.; et al. Ethics of artificial intelligence in radiology: Summary of the joint European and North American multisociety statement. Insights Imaging 2019, 10, 101. [Google Scholar] [CrossRef]
- Sheu, R.K.; Pardeshi, M.S. A Survey on Medical Explainable AI (XAI): Recent Progress, Explainability Approach, Human Interaction and Scoring System. Sensors 2022, 22, 8068. [Google Scholar] [CrossRef]

| Product Name | Company Name | DOF | Application Scope | Feedback | Features | Navigation |
|---|---|---|---|---|---|---|
| Corpath GRX | Corindus Vascular Robotics | 5 DOF | Cardiovascular, Peripheral, Neuro | Haptic Feedback | High precision (up to 0.1 mm), Intravascular Endoscopy | Digital geometric imaging and Machine Vision, Dedicated software for automation assistance |
| Magellan | Hansen Medical | 7 DOF | Cardio-vascular, Neuro-vascular, Peripheral | Force Feedback | C-Arm 3D Scanning Localization | Magnetic Field Sensing and Machine Vision |
| Robocath R-One | Robocath | N/A | Cardiovascular | Bidirectional Force Feedback | Enhanced Motion (Continuous Rotation, etc.) | AI algorithms assist in real-time generation of 3D images, Machine Vision |
| Sensei X2 Robotic Catheter System | Hansen Medical | 3 DOF | Cardio-vascular | Haptic Feedback | Automatic detection and tracking of heart position and motion | Digital geometric imaging and Machine Vision |
| Amigo | Catheter Precision | 3 DOF | Cardio-vascular | Haptic Feedback | Open catheter architecture | - |
| Product Name | Company Name | DOF | Application Scope | Imaging |
|---|---|---|---|---|
| AcuBot | Hopkins | 6 DOF | Biopsy, drainage, Tumour ablation, Vertebroplasty | Fluoroscopy, CT |
| B-Rob II | ARC Seibersdorf Research | 7 DOF | Biopsies | CT, US |
| iSYS1 | Medizintechnik | 4 DOF | Biopsy | Fluoroscopy, CT, |
| INNOMOTION | Innomedic | 6 DOF | Biopsy, Tumour ablation, Drainage | CT, MRI |
| EPIONE | Quantum Surgical | 6 DOF | Tumour ablation | CT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Fang, J.; Xu, Y.; Si, G. How AI and Robotics Will Advance Interventional Radiology: Narrative Review and Future Perspectives. Diagnostics 2024, 14, 1393. https://doi.org/10.3390/diagnostics14131393
Zhang J, Fang J, Xu Y, Si G. How AI and Robotics Will Advance Interventional Radiology: Narrative Review and Future Perspectives. Diagnostics. 2024; 14(13):1393. https://doi.org/10.3390/diagnostics14131393
Chicago/Turabian StyleZhang, Jiaming, Jiayi Fang, Yanneng Xu, and Guangyan Si. 2024. "How AI and Robotics Will Advance Interventional Radiology: Narrative Review and Future Perspectives" Diagnostics 14, no. 13: 1393. https://doi.org/10.3390/diagnostics14131393