Abstract
Perineural invasion (PNI), the neoplastic invasion of nerves, is an often overlooked pathological phenomenon in cervical cancer that is associated with poor clinical outcomes. The occurrence of PNI in cervical cancer patients has limited the promotion of Type C1 surgery. Preoperative prediction of the PNI can help identify suitable patients for Type C1 surgery. However, there is a lack of appropriate preoperative diagnostic methods for PNI, and its pathogenesis remains largely unknown. Here, we dissect the neural innervation of the cervix, analyze the molecular mechanisms underlying the occurrence of PNI, and explore suitable preoperative diagnostic methods for PNI to advance the identification and treatment of this ominous cancer phenotype.
1. Introduction
Nerves are emerging participants in tumor progression. Cancer cells induce the outgrowth of nerves in the tumor microenvironment (TME) through the release of neurotrophic factors. In turn, nerves release neurotransmitters that activate cancer growth and dissemination while also influencing the local environment by regulating angiogenesis and the immune system [1,2]. Research across various cancer types indicates a close association between higher intratumoral neural density and an unfavorable cancer prognosis [3,4]. For example, the presence of innervation in the TME has been found to be associated with tumor aggressiveness in conditions such as salivary adenoid cystic carcinoma [5], breast cancer [6], pancreatic cancer [4], gastric cancer [7], prostate cancer [8], and ovarian cancer [9]. Another mechanism through which the nervous system supports the migration of tumor cells is through perineural invasion (PNI), a process involving the invasion and migration of cancer cells along nerve sheaths. PNI refers to the involvement of tumor cells in more than one-third of the circumference of a nerve or the infiltration of any layer of the three-layer nerve sheath [10] (Figure 1). PNI manifests as a bidirectional tropism between nerves and cancer cells, orchestrated by the expression of specific molecules on both the tumor cells and surrounding peripheral nerves. Once PNI occurs, the affected nerves become sanctuaries for tumor cells. These tumor cells utilize this neural structure as a pathway for metastasis, avoiding clearance by the body and resistance to chemotherapy drugs [11,12]. Research has shown that the incidence of PNI in pancreatic ductal adenocarcinoma can reach 100% when enough pathological tissue sections are carefully analyzed [13,14]. In contrast, the incidence of PNI in cervical cancer patients ranges from only 7.0% to 35.1% [15]. However, cervical cancer patients with PNI also exhibit decreased survival [16]. Due to the propensity for PNI in cervical cancer, there is a consensus among experts that when a cervical biopsy or cervical conization indicates a relevant PNI, it should be considered a contraindication for Type C1 surgery [17]. In this review, our aim is to summarize the current literature on innervation and the PNI in cervical cancer. We focused on the clinical significance of PNI in cervical cancer patients and reviewed the molecular mechanisms underlying its occurrence.
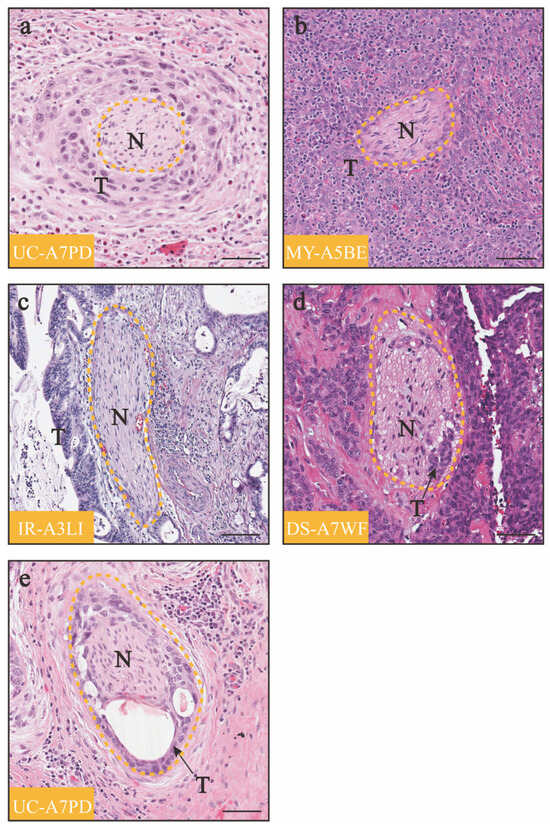
Figure 1.
Variety of histologic appearance patterns of PNI in cervical cancer patients from the TCGA cohort. (a) Tumor cells encircle the nerve outside the main tumor bulk. (b) Nerve is surrounded by tumor cells inside the main tumor bulk. (c) Tumor cells surround at least 33% of the nerve circumference. (d) Tumor cells invade the nerve. (e) Tumor cells invade the nerve and disrupt the integrity of the nerve. “N” represents nerves, “T” represents tumor cells, and the yellow dotted lines show the structure of the nerve; scale bar: 200 μm.
2. Evolution of Surgical Classifications for Cervical Cancer
In 1898, the Austrian surgeon Wertheim performed the world’s first abdominal radical hysterectomy for cervical cancer [18]. In 1974, Professor Piver proposed a five-type classification system for cervical cancer surgery [19]. Subsequently, in 2008, the Querleu–Morrow classification (Q–M classification) for radical hysterectomy was introduced [20]. In 2015, the National Comprehensive Cancer Network (NCCN) guidelines recommended shifting from the Piver classification to favor the Q–M classification [21]. In 2017, the Q–M classification underwent a revision [22] by incorporating the Cibula 3-D concept [23], reflecting the latest anatomical concepts and encompassing new approaches to almost all cervical cancer surgeries. The Q–M classification divides the scope of uterine resection into A, B, C, and D types, with subtypes B1, B2, C1, C2, D1, and D2. The C type, which involves extensive uterine resection, serves as the fundamental procedure for cervical cancer surgery. Based on whether the pelvic autonomous nerves are preserved, the C type is further classified into Type C1 (nerve-sparing radical hysterectomy, NSRH) and Type C2 (radical hysterectomy without preserving autonomic nerves, RH). Conventional extensive uterine resection can cause varying degrees of damage to pelvic autonomous nerve structures, leading to postoperative complications such as bladder dysfunction, rectal dysfunction, and sexual dysfunction. Clinical studies have confirmed that Type C1 surgery and Type C2 surgery are equally effective in treating cervical cancer [24,25], and there is no significant difference in patient prognosis [24,26,27]. To improve the postoperative quality of life for patients, the 2017 Q–M classification recommends promoting Type C1 surgery as the primary procedure for radical treatment of cervical cancer worldwide [22]. It is worth noting that cervical cancer exhibits a trend toward PNI. Therefore, PNI is a contraindication for Type C1 surgery. Chinese experts also recommend implementing Type C1 surgery for stage IB tumors with a diameter ≤4 cm, without deep stromal invasion of the cervix, without lymphovascular space invasion, without vaginal involvement, and without risk factors for lymph node metastasis [17].
3. Anatomic Mapping of Uterine Innervation
The superior hypogastric plexus (SHP) and hypogastric nerves are the main sources of sympathetic innervation to the pelvic organs. The SHP is formed by the continuation of the abdominal aortic plexus, located below the abdominal aortic bifurcation, in the region between the two common iliac arteries [28]. Its lower end extends approximately to the level of the sacral promontory, where it bifurcates into paired hypogastric nerves [28,29]. The left and right hypogastric nerves extend downward to the pelvic floor, on the medial side of the ureter and the lateral side of the uterosacral ligament in Okabayashi’s space [28,30], and combine with splanchnic nerves from S2 to S4 to form the inferior hypogastric plexus (IHP) [28,29]. The IHP sends out branches to supply the physiological functions of the rectum, uterus, vagina, and bladder, including the rectal fibers, uterine fibers, vaginal fibers, and vesical fibers (Figure 2). Among the areas of the human uterus, the nerve fibers of the cervix are the most densely distributed [31,32,33]. Specifically, the cervix exhibits a preference for certain types of nerves, with 79% TH+ autonomic sympathetic fibers, 73% NPY+ sensitive fibers, and 13% VIP+ parasympathetic fibers [32]. The abundant neural innervation results in the highest concentration of almost all neurotransmitters in the uterine cervix compared to the fundus and uterine body [31,33]. These neurotransmitters are involved in pain, vascular formation, and the constriction of pregnancy and childbirth [33]. For cervical cancer patients eligible for Type C1 surgery, excision should be carried out close to the organ to avoid damaging the IHP located on both sides of the organ, thus minimizing the risk of postoperative organ dysfunction.
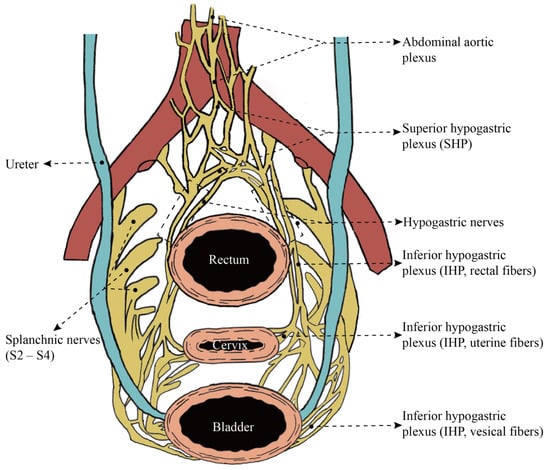
Figure 2.
Pelvic splanchnic nerves. Scheme of female pelvic autonomic nerves, overhead projection.
4. Clinical Studies of Cervical Cancer PNI
Several studies have consistently shown that cervical cancer patients with PNI have a lower overall survival (OS) rate [16,34,35,36,37,38,39], along with a decrease in disease-free survival (DFS) [35,37,38,39] or progression-free survival (PFS) [36] (Table 1). Compared to patients in the matched group, PNI (+) patients had advanced clinical stage [40,41,42,43,44], advanced tumor grade [40], increased tumor size [37,40,41,43], deep cervical stromal invasion [35,36,37,39,40,41,42,44], parametrial invasion [36,37,39,43,44], lymphovascular space invasion [35,37,39,40,43,44], positive lymph nodes [35,36,37,39,40,44], and positive margins [35,36,44]. Moreover, PNI (+) cervical cancer patients were more likely to receive adjuvant therapy after surgery [34,36,37,39,40,43,44] (Table 1). Therefore, the PNI can be regarded as a poor prognostic factor for patients with cervical cancer. However, in the studies reported by Karim S. Elsahwi (PNI was 12.5%, 24 out of 192 patients) [43] and Hyun Chul Cho (PNI was 7%, 13 out of 185 patients) [44], no differences in DFS or OS were observed based on the presence of PNI. Compared to the study by Wan Ting (PNI was 8.8%, 162 out of 1836 patients; possibly the largest study of cervical cancer patients with PNI among published data) [36], the sample sizes of Karim S. Elsahwi and Hyun Chul Cho appear to be relatively small and may leave out a small number of patients with an insignificant PNI. In detail, the study by Wan Ting shows the 3-year PFS of PNI (+) cervical cancer patients and the matched group were 76.4% and 87.8%, respectively, whereas the 3-year OS was 78.6% and 93.9% [36].

Table 1.
Association between the PNI and survival and clinicopathological features in cervical cancer patients.
5. Preoperative Assessment Methods
5.1. Biopsy
Preoperative PNI prediction might help identify populations that could obtain maximum benefits from Type C1 surgery without compromising oncologic safety. Traditionally, the identification of PNI primarily relies on postoperative pathological hematoxylin and eosin (H&E) staining and immunohistochemistry (IHC). However, the inconspicuous PNI status can be easily obscured under HE staining, and nerves severely infiltrated by tumor cells are also challenging to distinguish under HE staining. This often leads to underdiagnosis in PNI detection. Therefore, enhancing the visualization of the PNI becomes clinically significant. IHC examination of S100 neurospecific proteins can assist in diagnosing PNI. S100 is primarily expressed in Schwann cells (SCs) of nerve bundles, and immunohistochemical staining distinctly highlights nerve bundles, aiding in the identification of their location, quantity, and structural relationship with tumor cells [45,46,47,48,49]. In addition, when cancer cell clusters spread around or infiltrate nerves, distinguishing them from inflammatory cells also becomes a challenging task. In doubtful cases, double immunohistochemical staining of S100 and AE1/AE3 can improve the detection of small nerves invaded by diffuse gastric cancer [50], skin cancer [51], and vulvar cancer [52,53]. Double immunohistochemical staining has more advantages than H&E staining in the definitive diagnosis of PNI. However, performing rapid frozen section examination and immunohistochemistry intraoperatively is impractical. How can such a large piece of tumor tissue be rapidly located to identify affected nerve fibers? Furthermore, completing IHC staining within one hour is even more unlikely. Cervical biopsy and cervical conization pathologic results are also limited in guiding surgery, as they generally represent only a small part of the cervical tissue and may not include nerves. Therefore, a “negative” result may not rule out the possibility of pelvic nerve involvement. Some scholars have proposed performing a laparoscopic biopsy of uterine nerve branches a few days before surgery to develop surgical plans [54]. It is also impractical, as no patient would be willing to undergo additional surgery in terms of both physical and financial costs.
5.2. Imaging Methods
The 2018 FIGO staging for cervical cancer has moved beyond sole reliance on clinical staging, introducing a comprehensive evaluation approach that combines clinical examinations, imaging studies, and pathological assessments. Modern techniques featuring high-resolution capabilities are being explored as potential components of noninvasive PNI diagnostics [55]. Capek and colleagues reported instances of visualizing the PNI using MRI, FDG/PET CT, and choline PET/CT [56]. Their findings suggested that affected nerves commonly display enlargement with irregular and nodular contours on T1-weighted sequences, while T2-weighted images show hyperintensity [56]. These developments indicate a promising direction for the use of advanced imaging techniques for PNI assessment in cervical cancer and other pelvic malignancies. Ziv Gil and colleagues demonstrated in an animal model that intraoperative fluorescent stereoscopic imaging showed a significantly enhanced eGFP signal in a mouse PNI model treated with NV1066, identifying the affected nerves that needed to be excised [57]. However, this method is currently limited to the animal level, and its clinical application still has a long way to go.
5.3. Predictive Nomogram
Recently, some studies have focused on nomograms to establish risk assessment models for predicting the tumor PNI based on preoperative indicators, aiding in the formulation of more rational and accurate preoperative surgical plans [58,59,60]. Wan Ting et al. constructed a nomogram including age, adenocarcinoma, tumor size, neoadjuvant chemotherapy, lymph node enlargement, deep stromal invasion, and full-layer invasion to predict the PNI status in cervical cancer patients (AUC of 0.763 for the training set, AUC of 0.860 for the validation set, and AUC of 0.915 for the revised validation set). AUC is the area under the receiver operating characteristic curve [61]. It has satisfactory predictive performance and can help identify cervical cancer patients with false-negative PNI results. Although further large-scale, multicenter studies are needed to validate the predictive nomogram before its extensive use, it demonstrates significant practical advantages compared to biopsies.
6. Mechanisms of PNI in Cervical Cancer
6.1. “Defects” of the Peripheral Nerve Sheaths
The peripheral nerve sheath is composed of the epineurium, perineurium, and endoneurium. The epineurium is connective tissue that surrounds the surface of the nerve, and its surface is formed by several layers of flat epithelial cells. A nerve contains multiple nerve fiber bundles, and the thin layer of connective tissue on the surface of these fiber bundles is called the endoneurium. The extensive connective tissue between the epineurium and endoneurium forms the perineurium. Some scholars believe that the structure of peripheral nerves is a continuation of the development of spinal nerve structures, with the endoneurium, perineurium, and epineurium corresponding to the pia mater, arachnoid mater, and dura mater, respectively [62]. There are potential gaps between them that facilitate the infiltration and spread of cancer cells, creating so-called “low-resistance channels” [62,63]. Because nerves, blood vessels, and lymphatics often travel together, the blood-nerve barrier confers a privileged status to the endoneurial compartment. When hematogenous spread occurs, infiltration into the endoneurium likely occurs through direct spread from the epineurium [64]. However, lymphatic channels do not penetrate the inner parts of the nerve sheath [10,64], so the occurrence of PNI may be associated with hematogenous spread but not with lymphatic metastasis.
6.2. Neurotrophic Factors
Neurotrophic factors secreted by neuronal cells and cancer cells play a crucial role in the field of tumor neuroscience. Neurotrophic factors are divided into three main families: neurotrophins (NTs), ciliary neurotrophic factors (CNTFs), and glial cell-derived neurotrophic factors (GDNFs). The NT family is well characterized and consists of five members: nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), neurotrophin 3 (NT-3), neurotrophin 4/5 (NT-4/5), and neurotrophin 6 (NT-6). NTs interact with two types of receptors: p75 and Trk receptors. The p75 receptor exhibits a low-affinity binding capacity for all NTs. Conversely, Trk receptors display high-affinity binding specificity for different NTs: NGF binds to TrkA, BDNF and NT4/5 bind to TrkB, and NT-3 binds to TrkC [65]. When nerves are injured, SCs can promote the survival and repair of damaged neurons and axons by secreting neurotrophic factors such as NGF, BDNF, NT-3, and GDNF [66,67]. Similarly, within the tumor microenvironment, there is a process of neural repair similar to that observed during nerve damage [68]. This concept evokes the analogy of comparing a tumor to a wound that never heals [69].
Ying Long et al. found that high levels of NGF and TrkA expression correlate with the PNI in early-stage cervical cancer [70]. NGF can induce the proliferation and migration of cervical cancer cells [71]. Moreover, cervical cancer cell proliferation has been identified as a common phenomenon during PNI [72], establishing a basis for cancer cell colonization and metastasis along nerves. NGF secreted by cancer cells can additionally promote axon guidance and recruit nerves [73,74], thereby facilitating PNI in pancreatic cancer. Although studies indicate that exosomes secreted by cervical cancer cells induce their own innervation [75], it remains unclear whether NGF is packaged within exosomes or is required for exosome-mediated neurite outgrowth (Figure 3). Tumor-derived BDNF promotes increased innervation and is associated with poor outcomes in patients with ovarian cancer [9]. Furthermore, SCs facilitate the PNI process in salivary adenoid cystic carcinoma through the BDNF/TrkB axis [76]. Although there is currently no direct evidence of BDNF involvement in the neural innervation or PNI of cervical cancer, experiments have indicated that BDNF can enhance the motility and anoikis resistance of cervical cancer cells [77,78]. High expression of BDNF is also positively correlated with advanced FIGO stage, lymph node metastasis, and a poor prognosis in cervical cancer patients [79,80]. Therefore, BDNF may also play a crucial role in the PNI of cervical cancer patients.
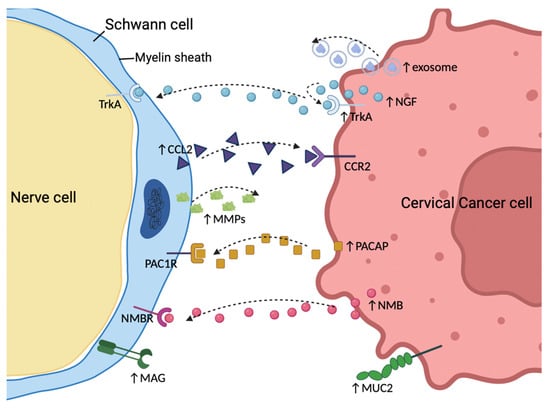
Figure 3.
Signaling molecules are involved in the process of perineural invasion in cervical cancer. Interactions between molecules expressed on cancer cells and peripheral nerves play an important role in perineural invasion (PNI). Cancer-derived exosomes and nerve growth factor (NGF) have been shown to be relevant for tumor innervation and PNI. Schwann cells can secrete CCL2, which acts on its corresponding receptor, CCR2, thus promoting tumor migration and invasion. In turn, cervical cancer cells can reverse the phenotype of Schwann cells to trigger PNI by secreting PACAP and NMB. Transmembrane proteins, such as MUC2 and MAG, may also facilitate tumor-nerve adhesion, providing a potential route for PNI. Additionally, matrix metalloproteinases (MMPs) secreted by Schwann cells could pave the way for tumor cell metastasis. PNI, perineural invasion; NGF, nerve growth factor; PACAP, pituitary adenylate cyclase-activating polypeptide; NMB, neuromedin B; MUC2, mucin 2; MAG, myelin-associated glycoprotein; MMPs, matrix metalloproteinases.
6.3. Chemokines
The aberrant release of chemokines is closely associated with PNI in cancer [14,81]. Nerve-released CCL2 supports the migration and PNI of prostate cancer through CCR2-mediated signaling [82]. Further research by Richard L. Bakst et al. revealed that SCs secrete CCL2, which recruits inflammatory monocytes from the circulation via CCR2, leading to the production of cathepsin B in these monocytes and ultimately disrupting the perineurium [83]. As expected, CCL2 is also a significant participant in PNI in cervical cancer. SCs migrate to the vicinity of the tumor and secrete CCL2 under signals derived from cervical cancer cells, which acts as a potent chemoattractant, inducing CCR2+ cervical cancer cells to undergo epithelial–mesenchymal transition (EMT) and move along neurites. In turn, signals from cancer cells trigger the expression of matrix metalloproteinases (MMPs) in SCs, facilitating extracellular matrix dissolution along the axon [84] (Figure 3).
6.4. Schwann Cells
Schwann cells (SCs) are glial cells in the peripheral nervous system, and their remarkable plasticity enables regeneration of the peripheral nervous system after injury [67]. In this process, SCs undergo two major changes. One of these effects is the upregulation of various neuropeptides that support the survival and axonal elongation of injured neurons. Among these neuropeptides are galanin, substance P (SP), and calcitonin gene-related peptide (CGRP), among others [85]. Neuropeptides are typically expressed at low levels in peripheral nerves but increase following injury and inflammation. A study revealed that following injury or inflammation, neurons release galanin, which activates head and neck cancer to favor PNI; in turn, the release of galanin from head and neck cancer induces neuritogenesis [86]. Moreover, when nerves are invaded by tumor cells, the nerves produce more galanin, thereby enhancing nerve–tumor interactions [86]. Similarly, neurogenic SP and CGRP can enhance the malignant phenotype of cancer cells, contributing to PNI [87,88,89].
Another component of SCs in the injury response is the reversal of myelin differentiation. The demyelination of SCs results in extensive cellular elongation and branching, generating a distinctive repair cell morphology that is favorable for the formation of regeneration tracks [90]. Molecules that characterize demyelinated SCs, including vimentin, nestin, c-Jun, and glial fibrillary acidic protein (GFAP), are upregulated [67]. Notably, when cervical cancer cells were cocultured with SCs, SCs were initially activated and migrated toward cervical cancer before the onset of cancer invasion [84,91]. At the same time, when cocultured with cervical cancer cells, the SCs exhibited an upregulation of demyelination markers, such as GFAP, vimentin, and nestin [91]. Based on these results, a new doctrine is further reinforced: it may be nerves—and not cancer cells—that first attack each other [92,93,94]. Through immunofluorescence staining, our previous research revealed that SCs migrate into the main bulk of the tumor and integrate into the intercellular spaces among cervical cancer cells [91]. This further indicates that signals from cervical cancer cells trigger Schwann cells, making them the precursor cells for PNI in cervical cancer. This interaction may be mediated by cervical cancer-derived pituitary adenylate cyclase-activating polypeptide (PACAP) [91]. Moreover, research by Ting Huang demonstrated that neuromedin B (NMB), derived from cervical cancer cells, triggers the reprogramming of SCs by binding to its membrane receptor NMBR, which in turn promotes axonal regeneration and induces PNI [95] (Figure 3).
6.5. Mucin
During PNI in pancreatic cancer, cancer cells that overexpress membrane-bound mucin 1 (MUC1) can establish strong adhesion with myelin-associated glycoprotein (MAG) on Schwann cells [96]. This selective adhesive advantage facilitates the invasion of cancer cells into the endoneurium of nerves. MUC1 also enhances the invasiveness of pancreatic cancer cells by inducing EMT [97], which may also contribute to the occurrence of PNI. In our previous research [91], we identified elevated expression levels of mucin 2 (MUC2) in PNI (+) cervical cancer patients in the TCGA cohort through the evaluation of perineural invasion and differential expression analysis (log2 fold-change = 3.15, p < 0.001; Figure 3; a volcano plot is shown in Supplementary Figure S1). MUC2 is a major mucin primarily secreted by goblet cells that forms a protective barrier on the surface of the intestinal epithelium and plays a crucial role in colonic protection [98]. Notably, both increased and decreased expression of MUC2 are associated with cancer progression [99,100,101,102,103,104]. Whether MUC2 promotes PNI in cervical cancer through selective adhesion and EMT or by generating a mucous barrier to protect cancer cells from recognition by antitumor immune effectors is not yet known. Our research team is actively exploring this issue.
7. PNI in Other Gynecological Cancers
Firstly, neural activities play a vital role in ovarian cancer progression, among which axon guidance is particularly significant [105]. Sustained adrenergic signaling has been associated with increased tumoral innervation in ovarian cancer [9], and elevated tumor nerve counts may also foster the occurrence of PNI. Zheng Zhen et al. further confirmed that the PNI is a strong predictor of poor prognosis in patients with ovarian cancer [106]. Nonetheless, the mechanisms that initiate PNI in ovarian cancer need further exploration. Secondly, the incidence of PNI in patients with vulvar cancer is approximately 30% [52,107]. Patients with PNI (+) vulvar cancer exhibit significantly shorter DFS and OS [52,107,108,109], indicating that the PNI should be regarded as an independent adverse prognostic factor for an unfavorable course of vulvar cancer [52,53,108,109,110]. However, the underlying mechanisms of PNI occurrence in vulvar cancer remain to be elucidated. Finally, the release of glutamic acid by neurons could promote PNI in endometrial carcinoma through the activation of GluR2 [111].
8. Conclusions
With the standardization and promotion of screening techniques, an increasing number of cervical cancer cases are being detected at an early stage. RH remains the primary treatment option for early-stage cervical cancer, but it has been shown to result in pelvic autonomous nervous system dysfunction, including lower urinary tract dysfunction and sexual dysfunction, significantly reducing patients’ quality of life. Therefore, Type C1 surgery has been used to preserve the pelvic autonomous nerves. However, due to the presence of PNI in cervical cancer patients, the implementation of Type C1 surgery has been limited. Despite the dense innervation of the cervix, the prevalence of PNI in cervical cancer patients remains low, and the reasons for this phenomenon are not yet fully understood. Because of the low incidence of PNI in cervical cancer patients, it has not previously received sufficient attention from surgeons. However, existing clinical studies have consistently shown that PNI (+) cervical cancer patients have a poor prognosis, which compels gynecologic oncologists to no longer ignore this aspect. Hence, studying PNI in cervical cancer is not about negating Type C1 surgery but rather about better clarifying the surgical indications of this procedure and more perfectly demonstrating its superiority for both patient survival and improving quality of life.
PNI is often underreported due to the lack of standardized reporting standards. Specific immunohistochemical staining of SCs using S100, in sharp contrast to counterstaining with HE, allows for a rapid and straightforward improvement in the detection rate of PNI. However, the challenges of specimen collection and the time-consuming staining process mean that its utility in guiding preoperative and intraoperative surgical planning is still limited. Imaging evaluation is also challenging for the timely identification of early PNI. Nomograms, which serve as a clinical tool to predict clinical events and outcomes, show promise for predicting the PNI in cervical cancer patients. We believe that a predictive nomogram can be considered one of the optimal solutions for the preoperative evaluation of PNI in cervical cancer patients.
Regrettably, there is limited research on the mechanism of PNI occurrence in cervical cancer. However, existing clinical studies have highlighted the significant role of SCs in this process. Inflammation accompanies cancer, acting as a catalyst for the progression of cancer development [112,113]. Therefore, neurons and SCs in the inflammatory tumor environment can promote the migration and invasion of tumor cells by secreting chemokines. Notably, the latest viewpoint suggests that tumor cells can actively secrete neuropeptides and other molecules to reverse the phenotype of SCs, thereby hijacking SCs to assist in their own neural metastasis. In conclusion, exploring the potential pathological mechanisms of PNI in cervical cancer through SCs will be significant for the surgical selection and treatment of cervical cancer.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics14141517/s1, Figure S1: Volcano plot of differentially expressed genes associated with the PNI in cervical cancer patients in the TCGA cohort. MUC2 was strongly upregulated in the PNI (+) group (log2 fold-change = 3.15, p < 0.001).
Author Contributions
G.C. designed the study, drafted the manuscript, and drew the figures. H.S. and Y.C. were responsible for the literature retrieval and typeset paper. L.W., O.S., J.Z. and D.L. participated in the discussion. X.L. and L.F. reviewed and edited the paper. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by grants from the Medical and Health Research Projects of Baoan District Medical Association (BAYXH2023001 to Guoqiang Chen), the Pyramid Talent Project—Outstanding Young Physician of Second Affiliated Hospital of Naval Medical University (YQ719 to Hao Sun), the National Social Science Fund of China (2023-SKJJ-B-038 to Xiaojun Liu), and the Science, Technology, and Innovation Commission of Shenzhen Municipality (JCYJ20190809105003741 to Lixia Feng).
Acknowledgments
Figure 2 was drawn by Procreate. Figure 3 is assembled by BioRender.com (https://app.biorender.com/). We appreciate the free use of Procreate and BioRender.com.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| TME | tumor microenvironment |
| PNI | perineural invasion |
| NSRH | nerve-sparing radical hysterectomy |
| RH | radical hysterectomy |
| SHP | superior hypogastric plexus |
| IHP | inferior hypogastric plexus |
| TH | tyrosine hydroxylase |
| NPY | neuropeptide Y |
| VIP | vasointestinal peptide |
| OS | overall survival |
| DFS | disease-free survival |
| PFS | progression-free survival |
| H&E | hematoxylin and eosin |
| IHC | immunohistochemistry |
| SCs | Schwann cells |
| AUC | area under the receiver operating characteristic curve |
| NTs | neurotrophins |
| CNTFs | ciliary neurotrophic factors |
| GDNFs | glial cell-derived neurotrophic factors |
| NGF | nerve growth factor |
| BDNF | brain-derived neurotrophic factor |
| NT-3 | neurotrophin 3 |
| NT-4/5 | neurotrophin 4/5 |
| NT-6 | neurotrophin 6 |
| EMT | Epithelial–mesenchymal transition |
| MMPs | matrix metalloproteinases |
| SP | substance P |
| CGRP | calcitonin gene-related peptide |
| GFAP | glial fibrillary acidic protein |
| PACAP | pituitary adenylate cyclase-activating polypeptide |
| NMB | neuromedin B |
| MUC1 | membrane-bound mucin 1 |
| MAG | myelin-associated glycoprotein |
References
- Jiang, S.H.; Hu, L.P.; Wang, X.; Li, J.; Zhang, Z.G. Neurotransmitters: Emerging targets in cancer. Oncogene 2020, 39, 503–515. [Google Scholar] [CrossRef]
- Reavis, H.D.; Chen, H.I.; Drapkin, R. Tumor Innervation: Cancer Has Some Nerve. Trends Cancer 2020, 6, 1059–1067. [Google Scholar] [CrossRef]
- Le, T.T.; Oudin, M.J. Understanding and modeling nerve-cancer interactions. Dis. Model. Mech. 2023, 16, dmm049729. [Google Scholar] [CrossRef]
- Ferdoushi, A.; Griffin, N.; Marsland, M.; Xu, X.; Faulkner, S.; Gao, F.; Liu, H.; King, S.J.; Denham, J.W.; van Helden, D.F.; et al. Tumor innervation and clinical outcome in pancreatic cancer. Sci. Rep. 2021, 11, 7390. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Gao, T.; Ju, J.; Zhang, Y.; Ni, Q.; Li, Y.; Zhao, Z.; Chai, J.; Yang, X.; Sun, M. Sympathetic innervation contributes to perineural invasion of salivary adenoid cystic carcinoma via the beta2-adrenergic receptor. OncoTargets Ther. 2019, 12, 1475–1495. [Google Scholar] [CrossRef]
- Kamiya, A.; Hayama, Y.; Kato, S.; Shimomura, A.; Shimomura, T.; Irie, K.; Kaneko, R.; Yanagawa, Y.; Kobayashi, K.; Ochiya, T. Genetic manipulation of autonomic nerve fiber innervation and activity and its effect on breast cancer progression. Nat. Neurosci. 2019, 22, 1289–1305. [Google Scholar] [CrossRef]
- Zhao, C.M.; Hayakawa, Y.; Kodama, Y.; Muthupalani, S.; Westphalen, C.B.; Andersen, G.T.; Flatberg, A.; Johannessen, H.; Friedman, R.A.; Renz, B.W.; et al. Denervation suppresses gastric tumorigenesis. Sci. Transl. Med. 2014, 6, 250ra115. [Google Scholar] [CrossRef] [PubMed]
- March, B.; Faulkner, S.; Jobling, P.; Steigler, A.; Blatt, A.; Denham, J.; Hondermarck, H. Tumour innervation and neurosignalling in prostate cancer. Nat. Rev. Urol. 2020, 17, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.K.; Armaiz-Pena, G.N.; Nagaraja, A.S.; Sadaoui, N.C.; Ortiz, T.; Dood, R.; Ozcan, M.; Herder, D.M.; Haemmerle, M.; Gharpure, K.M.; et al. Sustained Adrenergic Signaling Promotes Intratumoral Innervation through BDNF Induction. Cancer Res. 2018, 78, 3233–3242. [Google Scholar] [CrossRef]
- Liebig, C.; Ayala, G.; Wilks, J.A.; Berger, D.H.; Albo, D. Perineural invasion in cancer: A review of the literature. Cancer 2009, 115, 3379–3391. [Google Scholar] [CrossRef]
- Jiang, S.H.; Zhang, X.X.; Hu, L.P.; Wang, X.; Li, Q.; Zhang, X.L.; Li, J.; Gu, J.R.; Zhang, Z.G. Systemic Regulation of Cancer Development by Neuro-Endocrine-Immune Signaling Network at Multiple Levels. Front. Cell Dev. Biol. 2020, 8, 586757. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, S.; Krishnan, A. Neural invasion: A scenic trail for the nervous tumor and hidden therapeutic opportunity. Am. J. Cancer Res. 2020, 10, 2258–2270. [Google Scholar] [PubMed]
- Selvaggi, F.; Melchiorre, E.; Casari, I.; Cinalli, S.; Cinalli, M.; Aceto, G.M.; Cotellese, R.; Garajova, I.; Falasca, M. Perineural Invasion in Pancreatic Ductal Adenocarcinoma: From Molecules towards Drugs of Clinical Relevance. Cancers 2022, 14, 5793. [Google Scholar] [CrossRef] [PubMed]
- Bapat, A.A.; Hostetter, G.; Von Hoff, D.D.; Han, H. Perineural invasion and associated pain in pancreatic cancer. Nat. Rev. Cancer 2011, 11, 695–707. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, G.N.; Shi, Y.; Cui, L.; Leng, X.F.; Huang, J.M. Perineural invasion in cervical cancer: Pay attention to the indications of nerve-sparing radical hysterectomy. Ann. Transl. Med. 2019, 7, 203. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.C.; Meinel, A.; Fischer, U.; Bilek, K.; Hentschel, B. Perineural invasion in carcinoma of the cervix uteri--prognostic impact. J. Cancer Res. Clin. Oncol. 2010, 136, 1557–1562. [Google Scholar] [CrossRef] [PubMed]
- Gynecologic Oncology Group, Chinese Obstetricians and Gynecologists Association; Li, B.; Xiang, Y. Chinese expert consensus on nerve-sparing radical hysterectomy for cervical cancer. Zhonghua Zhong Liu Za Zhi 2021, 43, 736–742. [Google Scholar] [CrossRef]
- Swailes, A.L.; Gockley, A.; Phaeton, R.; Kesterson, J.P. The Wertheim hysterectomy: Development, modifications, and impact in the present day. Gynecol. Oncol. 2017, 145, 3–8. [Google Scholar] [CrossRef]
- Piver, M.S.; Rutledge, F.; Smith, J.P. Five classes of extended hysterectomy for women with cervical cancer. Obstet. Gynecol. 1974, 44, 265–272. [Google Scholar] [CrossRef]
- Querleu, D.; Morrow, C.P. Classification of radical hysterectomy. Lancet Oncol. 2008, 9, 297–303. [Google Scholar] [CrossRef]
- Koh, W.J.; Greer, B.E.; Abu-Rustum, N.R.; Apte, S.M.; Campos, S.M.; Cho, K.R.; Chu, C.; Cohn, D.; Crispens, M.A.; Dorigo, O.; et al. Cervical Cancer, Version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 395–404; quiz 404. [Google Scholar] [CrossRef] [PubMed]
- Querleu, D.; Cibula, D.; Abu-Rustum, N.R. 2017 Update on the Querleu-Morrow Classification of Radical Hysterectomy. Ann. Surg. Oncol. 2017, 24, 3406–3412. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Abu-Rustum, N.R.; Benedetti-Panici, P.; Kohler, C.; Raspagliesi, F.; Querleu, D.; Morrow, C.P. New classification system of radical hysterectomy: Emphasis on a three-dimensional anatomic template for parametrial resection. Gynecol. Oncol. 2011, 122, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Rossetti, D.O.; Ditto, A.; Signorelli, M.; Martinelli, F.; Mosca, L.; Scaffa, C.; Leone Roberti Maggiore, U.; Chiappa, V.; Sabatucci, I.; et al. Nerve-Sparing Approach Improves Outcomes of Patients Undergoing Minimally Invasive Radical Hysterectomy: A Systematic Review and Meta-Analysis. J. Minim. Invasive Gynecol. 2018, 25, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.; Yao, D.S.; Pan, X.W.; Ou, T.Y. Clinical efficacy and safety of nerve-sparing radical hysterectomy for cervical cancer: A systematic review and meta-analysis. PLoS ONE 2014, 9, e94116. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, A.; Kamoi, S.; Ikeda, M.; Yamada, T.; Yoneyama, K.; Takeshita, T. Effectiveness and Long-term Outcomes of Nerve-Sparing Radical Hysterectomy for Cervical Cancer. J. Nippon. Med. Sch. 2021, 88, 386–397. [Google Scholar] [CrossRef] [PubMed]
- van Gent, M.D.; Romijn, L.M.; van Santen, K.E.; Trimbos, J.B.; de Kroon, C.D. Nerve-sparing radical hysterectomy versus conventional radical hysterectomy in early-stage cervical cancer. A systematic review and meta-analysis of survival and quality of life. Maturitas 2016, 94, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Rob, L.; Halaska, M.; Robova, H. Nerve-sparing and individually tailored surgery for cervical cancer. Lancet Oncol. 2010, 11, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Tate, S.; Nishikimi, K.; Shozu, M. Bladder function after modified posterior exenteration for primary gynecological cancer. Gynecol. Oncol. 2013, 129, 229–233. [Google Scholar] [CrossRef]
- Raspagliesi, F.; Ditto, A.; Fontanelli, R.; Solima, E.; Hanozet, F.; Zanaboni, F.; Kusamura, S. Nerve-sparing radical hysterectomy: A surgical technique for preserving the autonomic hypogastric nerve. Gynecol. Oncol. 2004, 93, 307–314. [Google Scholar] [CrossRef]
- Kosmas, I.P.; Malvasi, A.; Vergara, D.; Mynbaev, O.A.; Sparic, R.; Tinelli, A. Adrenergic and Cholinergic Uterine Innervation and the Impact on Reproduction in Aged Women. Curr. Pharm. Des. 2020, 26, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Pinsard, M.; Mouchet, N.; Dion, L.; Bessede, T.; Bertrand, M.; Darai, E.; Bellaud, P.; Loget, P.; Mazaud-Guittot, S.; Morandi, X.; et al. Anatomic and functional mapping of human uterine innervation. Fertil. Steril. 2022, 117, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Di Tommaso, S.; Cavallotti, C.; Malvasi, A.; Vergara, D.; Rizzello, A.; De Nuccio, F.; Tinelli, A. A Qualitative and Quantitative Study of the Innervation of the Human Non Pregnant Uterus. Curr. Protein Pept. Sci. 2017, 18, 140–148. [Google Scholar] [CrossRef]
- Cui, L.; Shi, Y.; Zhang, G.N. Perineural invasion as a prognostic factor for cervical cancer: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2015, 292, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.; Liu, Q.; Yang, X.; Chen, L.; Yu, J.; Qi, X.; Wang, Y. Perineural invasion as a prognostic risk factor in patients with early cervical cancer. Oncol. Lett. 2019, 17, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Wan, T.; Tu, H.; Liu, L.; Huang, H.; Feng, Y.; Liu, J. Perineural Invasion Should Be Regarded as an Intermediate-Risk Factor for Recurrence in Surgically Treated Cervical Cancer: A Propensity Score Matching Study. Dis. Markers 2021, 2021, 1375123. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, G.; Yang, Y.; Cui, L.; Jia, S.; Shi, Y.; Song, S.; Xu, S. Perineural invasion in early-stage cervical cancer and its relevance following surgery. Oncol. Lett. 2018, 15, 6555–6561. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.W.; Wang, H.; Zheng, H.; Chen, J.; Shi, R.X. Survival Impacts of Perineural Invasion on Patients Under Different Radical Hysterectomies Due to Early Cervical Cancer. Front. Oncol. 2022, 12, 889862. [Google Scholar] [CrossRef]
- Chen, X.; Duan, H.; Zhao, H.; He, F.; Yin, L.; Liu, Y.; Wang, X.; Chen, C. Perineural invasion in cervical cancer: A multicenter retrospective study. Eur. J. Surg. Oncol. 2024, 50, 108313. [Google Scholar] [CrossRef]
- Wei, Y.S.; Yao, D.S.; Long, Y. Evaluation of the association between perineural invasion and clinical and histopathological features of cervical cancer. Mol. Clin. Oncol. 2016, 5, 307–311. [Google Scholar] [CrossRef]
- Skret-Magierlo, J.E.; Soja, P.J.; Skret, A.; Kruczek, A.; Kaznowska, E.; Wicherek, L. Perineural space invasion in cervical cancer (FIGO IB1-IIB) accompanied by high-risk factors for recurrence. J. Cancer Res. Ther. 2014, 10, 957–961. [Google Scholar] [CrossRef] [PubMed]
- Meinel, A.; Fischer, U.; Bilek, K.; Hentschel, B.; Horn, L.C. Morphological parameters associated with perineural invasion (PNI) in carcinoma of the cervix uteri. Int. J. Surg. Pathol. 2011, 19, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Elsahwi, K.S.; Barber, E.; Illuzzi, J.; Buza, N.; Ratner, E.; Silasi, D.A.; Santin, A.D.; Azodi, M.; Schwartz, P.E.; Rutherford, T.J. The significance of perineural invasion in early-stage cervical cancer. Gynecol. Oncol. 2011, 123, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.C.; Kim, H.; Cho, H.Y.; Kim, K.; No, J.H.; Kim, Y.B. Prognostic significance of perineural invasion in cervical cancer. Int. J. Gynecol. Pathol. 2013, 32, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Tanaka, Y.; Eto, K.; Ukai, N.; Sonobe, S.; Takahashi, H.; Ikegami, M.; Shimoda, M. S100-stained perineural invasion is associated with worse prognosis in stage I/II colorectal cancer: Its possible association with immunosuppression in the tumor. Pathol. Int. 2022, 72, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Conte, G.A.; Qari, O.; Fasano, G.A.; Guinto, R.K.; Palo, L.; Parker, G.S.; Rangwala, A.F.; Minassian, H.; Greenberg, P.J.; Dewan, A.A.; et al. S100 Staining Adds to the Prognostic Significance of the Combination of Perineural Invasion and Lymphovascular Invasion in Colorectal Cancer. Appl. Immunohistochem. Mol. Morphol. 2020, 28, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.R.; Wang, Y.P.; Chang, J.Y.; Yu, S.Y.; Chen, H.M.; Chiang, C.P. Perineural invasion and expression of nerve growth factor can predict the progression and prognosis of oral tongue squamous cell carcinoma. J. Oral. Pathol. Med. 2014, 43, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Lanzel, E.; Robinson, R.A.; Zimmerman, M.B.; Pourian, A.; Hellstein, J.W. The use of immunohistochemistry in detection of perineural invasion in mucoepidermoid carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Feng, F.; Liu, Z.; Liu, S.; Zheng, G.; Xiao, S.; Cai, L.; Yang, X.; Li, G.; Lian, X.; et al. Prognosis and Progression of ESCC Patients with Perineural Invasion. Sci. Rep. 2017, 7, 43828. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.H.; Xu, G.F.; Zhang, W.J.; Zhao, H.B.; Wu, Y.Y. Reevaluating significance of perineural invasion in gastric cancer based on double immunohistochemical staining. Arch. Pathol. Lab. Med. 2014, 138, 229–234. [Google Scholar] [CrossRef]
- Berlingeri-Ramos, A.C.; Detweiler, C.J.; Wagner, R.F., Jr.; Kelly, B.C. Dual S-100-AE1/3 Immunohistochemistry to Detect Perineural Invasion in Nonmelanoma Skin Cancers. J. Skin. Cancer 2015, 2015, 620235. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, F.; Forte, S.; Ardighieri, L.; Bonetti, E.; Fernando, B.; Sartori, E.; Odicino, F. Multivariate analysis of prognostic factors in primary squamous cell vulvar cancer: The role of perineural invasion in recurrence and survival. Eur. J. Surg. Oncol. 2019, 45, 2115–2119. [Google Scholar] [CrossRef] [PubMed]
- Holthoff, E.R.; Jeffus, S.K.; Gehlot, A.; Stone, R.; Erickson, S.W.; Kelly, T.; Quick, C.M.; Post, S.R. Perineural Invasion Is an Independent Pathologic Indicator of Recurrence in Vulvar Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2015, 39, 1070–1074. [Google Scholar] [CrossRef] [PubMed]
- Skret, A.; Skret-Magierlo, J.E.; Ksiazek, M.; Gawlik, B.; Bielatowicz, J.; Barnas, E. The Diagnosis of Perineural Invasion: A Crucial Factor in Novel Algorithm of Coexistence of Conventional and Nerve-Sparing Radical Hysterectomy. Diagnostics 2021, 11, 1308. [Google Scholar] [CrossRef] [PubMed]
- Penn, R.; Abemayor, E.; Nabili, V.; Bhuta, S.; Kirsch, C. Perineural invasion detected by high-field 3.0-T magnetic resonance imaging. Am. J. Otolaryngol. 2010, 31, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Capek, S.; Howe, B.M.; Amrami, K.K.; Spinner, R.J. Perineural spread of pelvic malignancies to the lumbosacral plexus and beyond: Clinical and imaging patterns. Neurosurg. Focus. 2015, 39, E14. [Google Scholar] [CrossRef] [PubMed]
- Gil, Z.; Kelly, K.J.; Brader, P.; Shah, J.P.; Fong, Y.; Wong, R.J. Utility of a herpes oncolytic virus for the detection of neural invasion by cancer. Neoplasia 2008, 10, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Liu, J.; Wu, G.; Chen, S.; Pc, F.J.; Xie, W.; Tang, W. Development and Validation of a Nomogram for Preoperative Prediction of Perineural Invasion in Colorectal Cancer. Med. Sci. Monit. 2019, 25, 1709–1717. [Google Scholar] [CrossRef]
- Liu, S.H.; Hou, X.Y.; Zhang, X.X.; Liu, G.W.; Xin, F.J.; Wang, J.G.; Zhang, D.L.; Wang, D.S.; Lu, Y. Establishment and validation of a predictive nomogram model for advanced gastric cancer with perineural invasion. Zhonghua Wei Chang Wai Ke Za Zhi 2020, 23, 1059–1066. [Google Scholar] [CrossRef]
- Jia, H.; Li, R.; Liu, Y.; Zhan, T.; Li, Y.; Zhang, J. Preoperative Prediction of Perineural Invasion and Prognosis in Gastric Cancer Based on Machine Learning through a Radiomics-Clinicopathological Nomogram. Cancers 2024, 16, 614. [Google Scholar] [CrossRef]
- Wan, T.; Cai, G.; Gao, S.; Feng, Y.; Huang, H.; Liu, L.; Liu, J. Preoperative Evaluation of Perineural Invasion in Cervical Cancer: Development and Independent Validation of a Novel Predictive Nomogram. Front. Oncol. 2021, 11, 774459. [Google Scholar] [CrossRef] [PubMed]
- Dunn, M.; Morgan, M.B.; Beer, T.W. Perineural invasion: Identification, significance, and a standardized definition. Dermatol. Surg. 2009, 35, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Rodin, A.E.; Larson, D.L.; Roberts, D.K. Nature of the perineural space invaded by prostatic carcinoma. Cancer 1967, 20, 1772–1779. [Google Scholar] [CrossRef] [PubMed]
- Uchida, K.; Kobayashi, S.; Yayama, T.; Muramatsu, J.; Kurokawa, T.; Imamura, Y.; Baba, H. Metastatic involvement of sacral nerve roots from uterine carcinoma: A case report. Spine J. 2008, 8, 849–852. [Google Scholar] [CrossRef] [PubMed]
- Retamales-Ortega, R.; Orostica, L.; Vera, C.; Cuevas, P.; Hernandez, A.; Hurtado, I.; Vega, M.; Romero, C. Role of Nerve Growth Factor (NGF) and miRNAs in Epithelial Ovarian Cancer. Int. J. Mol. Sci. 2017, 18, 507. [Google Scholar] [CrossRef] [PubMed]
- Brushart, T.M.; Aspalter, M.; Griffin, J.W.; Redett, R.; Hameed, H.; Zhou, C.; Wright, M.; Vyas, A.; Hoke, A. Schwann cell phenotype is regulated by axon modality and central-peripheral location, and persists in vitro. Exp. Neurol. 2013, 247, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Jessen, K.R.; Mirsky, R.; Lloyd, A.C. Schwann Cells: Development and Role in Nerve Repair. Cold Spring Harb. Perspect. Biol. 2015, 7, a020487. [Google Scholar] [CrossRef] [PubMed]
- Shurin, G.V.; Kruglov, O.; Ding, F.; Lin, Y.; Hao, X.; Keskinov, A.A.; You, Z.; Lokshin, A.E.; LaFramboise, W.A.; Falo, L.D., Jr.; et al. Melanoma-Induced Reprogramming of Schwann Cell Signaling Aids Tumor Growth. Cancer Res. 2019, 79, 2736–2747. [Google Scholar] [CrossRef]
- Dvorak, H.F. Tumors: Wounds that do not heal-redux. Cancer Immunol. Res. 2015, 3, 1–11. [Google Scholar] [CrossRef]
- Long, Y.; Yao, D.S.; Wei, Y.S.; Wu, G.T. Effects of Nerve Growth Factor Expression on Perineural Invasion and Worse Prognosis in Early-Stage Cervical Cancer. Chin. Med. J. 2018, 131, 2360–2363. [Google Scholar] [CrossRef]
- Wang, L.; Li, J.; Wang, R.; Chen, H.; Wang, R.; Wang, W.; Yang, X. NGF Signaling Interacts With the Hippo/YAP Pathway to Regulate Cervical Cancer Progression. Front. Oncol. 2021, 11, 688794. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Wang, Y.; Wang, Z.; Cui, Y.; Sun, X.; Wang, Y. Weighted Gene Co-Expression Network Analysis Identified Cancer Cell Proliferation as a Common Phenomenon During Perineural Invasion. OncoTargets Ther. 2019, 12, 10361–10374. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; He, R.; Yang, W.; Zhang, Y.; Yuan, Q.; Wang, J.; Liu, Y.; Chen, S.; Zhang, S.; Zhang, W.; et al. Autophagic Schwann cells promote perineural invasion mediated by the NGF/ATG7 paracrine pathway in pancreatic cancer. J. Exp. Clin. Cancer Res. 2022, 41, 48. [Google Scholar] [CrossRef] [PubMed]
- Qin, T.; Xiao, Y.; Qian, W.; Wang, X.; Gong, M.; Wang, Q.; An, R.; Han, L.; Duan, W.; Ma, Q.; et al. HGF/c-Met pathway facilitates the perineural invasion of pancreatic cancer by activating the mTOR/NGF axis. Cell Death Dis. 2022, 13, 387. [Google Scholar] [CrossRef] [PubMed]
- Lucido, C.T.; Wynja, E.; Madeo, M.; Williamson, C.S.; Schwartz, L.E.; Imblum, B.A.; Drapkin, R.; Vermeer, P.D. Innervation of cervical carcinoma is mediated by cancer-derived exosomes. Gynecol. Oncol. 2019, 154, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Shan, C.; Wei, J.; Hou, R.; Wu, B.; Yang, Z.; Wang, L.; Lei, D.; Yang, X. Schwann cells promote EMT and the Schwann-like differentiation of salivary adenoid cystic carcinoma cells via the BDNF/TrkB axis. Oncol. Rep. 2016, 35, 427–435. [Google Scholar] [CrossRef]
- Yuan, Y.; Ye, H.Q.; Ren, Q.C. Upregulation of the BDNF/TrKB pathway promotes epithelial-mesenchymal transition, as well as the migration and invasion of cervical cancer. Int. J. Oncol. 2018, 52, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Ye, H.Q.; Ren, Q.C. Proliferative role of BDNF/TrkB signaling is associated with anoikis resistance in cervical cancer. Oncol. Rep. 2018, 40, 621–634. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Li, W.; Kang, S.; Chen, L.; Hao, M.; Wang, W.; Ling, B.; Cui, Z.; Liang, C.; He, J.; et al. Expression of BDNF, TrkB, VEGF and CD105 is associated with pelvic lymph node metastasis and prognosis in IB2-stage squamous cell carcinoma. Exp. Ther. Med. 2019, 18, 4221–4230. [Google Scholar] [CrossRef]
- Sirico, A.; Simonelli, S.; Pignatiello, S.; Fulgione, C.; Sarno, L.; Chiuso, F.; Maruotti, G.M.; Sansone, M.; Guida, M.; Insabato, L. BDNF and NGF Expression in Preneoplastic Cervical Disease According to HIV Status. Int. J. Mol. Sci. 2023, 24, 729. [Google Scholar] [CrossRef]
- Chen, S.H.; Zhang, B.Y.; Zhou, B.; Zhu, C.Z.; Sun, L.Q.; Feng, Y.J. Perineural invasion of cancer: A complex crosstalk between cells and molecules in the perineural niche. Am. J. Cancer Res. 2019, 9, 1–21. [Google Scholar] [PubMed]
- He, S.; He, S.; Chen, C.H.; Deborde, S.; Bakst, R.L.; Chernichenko, N.; McNamara, W.F.; Lee, S.Y.; Barajas, F.; Yu, Z.; et al. The chemokine (CCL2-CCR2) signaling axis mediates perineural invasion. Mol. Cancer Res. 2015, 13, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Bakst, R.L.; Xiong, H.; Chen, C.H.; Deborde, S.; Lyubchik, A.; Zhou, Y.; He, S.; McNamara, W.; Lee, S.Y.; Olson, O.C.; et al. Inflammatory Monocytes Promote Perineural Invasion via CCL2-Mediated Recruitment and Cathepsin B Expression. Cancer Res. 2017, 77, 6400–6414. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Fan, Q.; Wang, Y.; Cui, Y.; Wang, Z.; Yang, L.; Sun, X.; Wang, Y. Schwann Cell-Derived CCL2 Promotes the Perineural Invasion of Cervical Cancer. Front. Oncol. 2020, 10, 19. [Google Scholar] [CrossRef] [PubMed]
- Navarro, X.; Vivo, M.; Valero-Cabre, A. Neural plasticity after peripheral nerve injury and regeneration. Prog. Neurobiol. 2007, 82, 163–201. [Google Scholar] [CrossRef] [PubMed]
- Scanlon, C.S.; Banerjee, R.; Inglehart, R.C.; Liu, M.; Russo, N.; Hariharan, A.; van Tubergen, E.A.; Corson, S.L.; Asangani, I.A.; Mistretta, C.M.; et al. Galanin modulates the neural niche to favour perineural invasion in head and neck cancer. Nat. Commun. 2015, 6, 6885. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ma, G.; Ma, Q.; Li, W.; Liu, J.; Han, L.; Duan, W.; Xu, Q.; Liu, H.; Wang, Z.; et al. Neurotransmitter substance P mediates pancreatic cancer perineural invasion via NK-1R in cancer cells. Mol. Cancer Res. 2013, 11, 294–302. [Google Scholar] [CrossRef]
- Huang, C.; Li, Y.; Guo, Y.; Zhang, Z.; Lian, G.; Chen, Y.; Li, J.; Su, Y.; Li, J.; Yang, K.; et al. MMP1/PAR1/SP/NK1R paracrine loop modulates early perineural invasion of pancreatic cancer cells. Theranostics 2018, 8, 3074–3086. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, M.; Liu, Z.; Wang, X.; Ji, T. The neuropeptide calcitonin gene-related peptide links perineural invasion with lymph node metastasis in oral squamous cell carcinoma. BMC Cancer 2021, 21, 1254. [Google Scholar] [CrossRef]
- Gomez-Sanchez, J.A.; Pilch, K.S.; van der Lans, M.; Fazal, S.V.; Benito, C.; Wagstaff, L.J.; Mirsky, R.; Jessen, K.R. After Nerve Injury, Lineage Tracing Shows That Myelin and Remak Schwann Cells Elongate Extensively and Branch to Form Repair Schwann Cells, Which Shorten Radically on Remyelination. J. Neurosci. 2017, 37, 9086–9099. [Google Scholar] [CrossRef]
- Chen, G.; Zheng, Z.; Sun, H.; You, J.; Chu, J.; Gao, J.; Qiu, L.; Liu, X. Dedifferentiated Schwann cells promote perineural invasion mediated by the PACAP paracrine signalling in cervical cancer. J. Cell Mol. Med. 2023, 27, 3692–3705. [Google Scholar] [CrossRef]
- Demir, I.E.; Boldis, A.; Pfitzinger, P.L.; Teller, S.; Brunner, E.; Klose, N.; Kehl, T.; Maak, M.; Lesina, M.; Laschinger, M.; et al. Investigation of Schwann cells at neoplastic cell sites before the onset of cancer invasion. J. Natl. Cancer Inst. 2014, 106, dju184. [Google Scholar] [CrossRef] [PubMed]
- Azam, S.H.; Pecot, C.V. Cancer’s got nerve: Schwann cells drive perineural invasion. J. Clin. Invest. 2016, 126, 1242–1244. [Google Scholar] [CrossRef]
- Deborde, S.; Omelchenko, T.; Lyubchik, A.; Zhou, Y.; He, S.; McNamara, W.F.; Chernichenko, N.; Lee, S.Y.; Barajas, F.; Chen, C.H.; et al. Schwann cells induce cancer cell dispersion and invasion. J. Clin. Invest. 2016, 126, 1538–1554. [Google Scholar] [CrossRef] [PubMed]
- Huang, T. Cancer Cell-Derived NMB Initiating the Perineural Invasion of Cervical Cancer. Master’s Thesis, Shanghai Jiao Tong University, Shanghai, China, 2020. [Google Scholar] [CrossRef]
- Swanson, B.J.; McDermott, K.M.; Singh, P.K.; Eggers, J.P.; Crocker, P.R.; Hollingsworth, M.A. MUC1 is a counter-receptor for myelin-associated glycoprotein (Siglec-4a) and their interaction contributes to adhesion in pancreatic cancer perineural invasion. Cancer Res. 2007, 67, 10222–10229. [Google Scholar] [CrossRef] [PubMed]
- Roy, L.D.; Sahraei, M.; Subramani, D.B.; Besmer, D.; Nath, S.; Tinder, T.L.; Bajaj, E.; Shanmugam, K.; Lee, Y.Y.; Hwang, S.I.; et al. MUC1 enhances invasiveness of pancreatic cancer cells by inducing epithelial to mesenchymal transition. Oncogene 2011, 30, 1449–1459. [Google Scholar] [CrossRef]
- Van der Sluis, M.; De Koning, B.A.; De Bruijn, A.C.; Velcich, A.; Meijerink, J.P.; Van Goudoever, J.B.; Buller, H.A.; Dekker, J.; Van Seuningen, I.; Renes, I.B.; et al. Muc2-deficient mice spontaneously develop colitis, indicating that MUC2 is critical for colonic protection. Gastroenterology 2006, 131, 117–129. [Google Scholar] [CrossRef]
- Betge, J.; Schneider, N.I.; Harbaum, L.; Pollheimer, M.J.; Lindtner, R.A.; Kornprat, P.; Ebert, M.P.; Langner, C. MUC1, MUC2, MUC5AC, and MUC6 in colorectal cancer: Expression profiles and clinical significance. Virchows Arch. 2016, 469, 255–265. [Google Scholar] [CrossRef]
- Chiang, J.M.; Yeh, C.Y.; Changchien, C.R.; Chen, J.S.; Tang, R.; Chen, J.R. Mucinous adenocarcinoma showing different clinicopathological and molecular characteristics in relation to different colorectal cancer subgroups. Int. J. Colorectal Dis. 2010, 25, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Gundamaraju, R.; Chong, W.C. Consequence of distinctive expression of MUC2 in colorectal cancers: How much is actually bad? Biochim. Biophys. Acta Rev. Cancer 2021, 1876, 188579. [Google Scholar] [CrossRef]
- Chou, C.L.; Chen, T.J.; Tian, Y.F.; Chan, T.C.; Yeh, C.F.; Li, W.S.; Tsai, H.H.; Li, C.F.; Lai, H.Y. Upregulated MUC2 Is an Unfavorable Prognostic Indicator for Rectal Cancer Patients Undergoing Preoperative CCRT. J. Clin. Med. 2021, 10, 3030. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.J.; Walsh, J.C.; Parfitt, J.; Chakrabarti, S.; Correa, R.J.; MacKenzie, M.J.; Driman, D.K. CDX2 and Muc2 immunohistochemistry as prognostic markers in stage II colon cancer. Hum. Pathol. 2019, 90, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Astashchanka, A.; Shroka, T.M.; Jacobsen, B.M. Mucin 2 (MUC2) modulates the aggressiveness of breast cancer. Breast Cancer Res. Treat. 2019, 173, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Bie, L.; Sun, L.; Yue, Y. Neural activities are unfavorable for the prognosis of ovarian cancer through mRNA expression analysis. Biomark. Med. 2019, 13, 663–673. [Google Scholar] [CrossRef]
- Zheng, Z.; Li, X.; Chen, G.; Chen, J.; Zhu, X.; Teng, Y. Transcriptome analyses reveal new insights on key determinants of perineural invasion in high-grade serous ovarian cancer. Front. Cell Dev. Biol. 2023, 11, 1109710. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.; Yao, D.S.; Wei, Y.S.; Wei, C.H.; Chen, X.Y. Prognostic significance of perineural invasion in vulvar squamous cell carcinoma. Cancer Manag. Res. 2019, 11, 4461–4469. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Angelico, G.; Travaglino, A.; Inzani, F.; Arciuolo, D.; Valente, M.; D’Alessandris, N.; Scaglione, G.; Piermattei, A.; Cianfrini, F.; et al. Prognostic role of perineural invasion in vulvar squamous cell carcinoma: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2022, 48, 2354–2359. [Google Scholar] [CrossRef] [PubMed]
- Salcedo, M.P.; Sood, A.K.; Dos Reis, R.; Ramalingam, P.; Chen, C.; Frumovitz, M.; Jhingran, A.; Pitcher, B.; Ramirez, P.T.; Schmeler, K.M. Perineural invasion (PNI) in vulvar carcinoma: A review of 421 cases. Gynecol. Oncol. 2019, 152, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Pistolesi, S.; Cosio, S.; Naccarato, A.G. Is Perineural Invasion a Novel Prognostic Factor Useful to Tailor Adjuvant Treatment in Patients Treated With Primary Surgery for Cervical and Vulvar Carcinoma? Anticancer Res. 2020, 40, 3031–3037. [Google Scholar] [CrossRef]
- Ni, T.; Huang, T.; Gu, S.L.; Wang, J.; Liu, Y.; Sun, X.; Wang, Y.D. DRG Neurons Promote Perineural Invasion of Endometrial Cancer via GluR2. J. Cancer 2020, 11, 2518–2528. [Google Scholar] [CrossRef]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Deivendran, S.; Marzook, K.H.; Radhakrishna Pillai, M. The role of inflammation in cervical cancer. Adv. Exp. Med. Biol. 2014, 816, 377–399. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).