

Localised Objective Characterisation Assessment of Lymphoedema (LOCAL): Using High-Frequency Ultrasound, Bioelectrical Impedance Spectroscopy and Volume to Evaluate Superficial Tissue Composition

Abstract
:1. Introduction
2. Materials and Methods
2.1. LOCAL Classification
- Segment volume parameters were based on the subclinical diagnostic thresholds utilised by previous authors. The inter-limb volume difference threshold is ≥5% for the dominant [9,10] and ≥3% for the non-dominant lymphoedema-affected limb segment. The latter threshold was considered sufficient for a subclinical change with reference to the non-dominant arm volume reported to average 3.3% smaller than the dominant limb [11]. Where baseline measures are available, a threshold of ≥3% limb segment volume change is used [2,12].
- The BIS R0 measure is most specific to the extracellular fluid volume component of the lymphoedema presentation [13]. R0 values for the LOCAL criteria were derived from diagnostic thresholds of the R0 ratio in segmental measures considering limb dominance [14,15]. Segment thresholds were calculated for the 20 cm segment size by averaging the 10 cm 2SD (standard deviation) R0 diagnostic thresholds for the correlating location. The R0 ratio thresholds in the LOCAL system are intended to distinguish between small and large differences in inter-limb extracellular fluid volume.
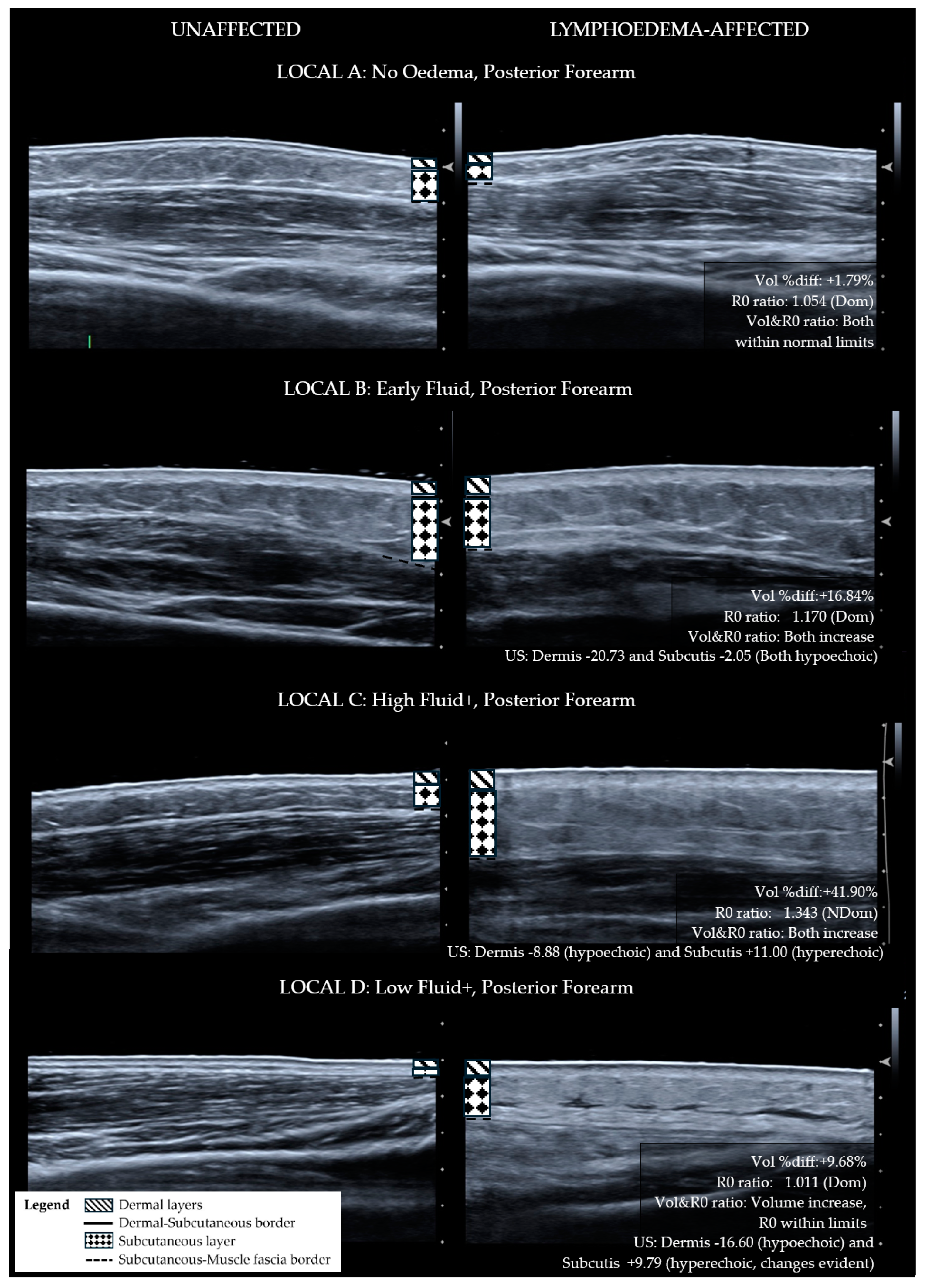
- The ultrasound echogenicity parameter is used to support the presence or absence of tissue compositional change. Lymphoedema tissue has been shown to become hypoechoic (darker) with diffuse fluid influx [15,16] and hyperechoic (lighter) with fibrotic and fatty deposition [17,18,19]. The distribution of hyper-echogenicity may encompass the full or partial cross-section of the tissue layer or appear as scattered flecks [17,18,19]. For this reason, a decrease in the echogenicity of the lymphoedema tissue layers was observed as fluid influx, and an increase in echogenicity escalated the classification to the fibro-fatty groupings.
2.2. LOCAL Verification
2.2.1. Patient Demographics
2.2.2. Ultrasound
2.2.3. BIS
2.2.4. Limb Segment Volume
2.2.5. Distribution of Lymphoedema
2.2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanderson, J.; Tuttle, N.; Box, R.; Reul-Hirche, H.; Laakso, E.-L. Pitting is Not Only a Measure of Oedema Presence: Using High-Frequency Ultrasound to Guide Pitting Test Standardisation for Assessment of Lymphoedema. 2024; Submitted for publication. [Google Scholar]
- International Society of Lymphology. The diagnosis and treatment of peripheral lymphoedema: 2020 consensus document of the International Society of Lymphology. Lymphology 2020, 53, 3–19. [Google Scholar]
- Alitalo, K. The lymphatic vasculature in disease. Nat. Med. 2011, 17, 1371–1380. [Google Scholar] [CrossRef]
- Ridner, S.H. Pathophysiology of lymphedema. Semin. Oncol. Nurs. 2013, 29, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Zampell, J.C.; Aschen, S.; Weitman, E.S.; Yan, A.; Elhadad, S.; De Brot Andrade, M.; Mehrara, B.J. Regulation of adipogenesis by lymphatic fluid stasis: Part I. Adipogenesis, fibrosis, and inflammation. Plast. Reconstr. Surg. 2012, 129, 825–834. [Google Scholar] [CrossRef]
- Brorson, H.; Ohlin, K.; Olsson, G.; Karlsson, M.K. Breast cancer-related chronic arm lymphedema is associated with excess adipose and muscle tissue. Lymphat. Res. Biol. 2009, 7, 3–29. [Google Scholar] [CrossRef]
- Sanderson, J.; Tuttle, N.; Box, R.; Reul-Hirche, H.; Laakso, E.-L. The pitting test: An investigation into an unstandardized assessment of lymphoedema. Lymphology 2015, 48, 175–183. [Google Scholar] [PubMed]
- Sanderson, J.K. A Detailed Investigation into the Pitting Test: Using High-Frequency Ultrasound to Evaluate the Effect of Applying Sustained Thumb Pressure to Lymphoedema Tissue. Ph.D. Thesis, Griffith University, Gold Coast, Southport, Australia, 2 June 2023. Available online: http://hdl.handle.net/10072/423362 (accessed on 3 June 2024).
- Querci della Rovere, G.; Ahmad, I.; Singh, P.; Ashley, S.; Daniels, I.R.; Mortimer, P. An audit of the incidence of arm lymphoedema after prophylactic level I/II axillary dissection without division of the pectoralis minor muscle. Ann. R. Coll. Surg. Engl. 2003, 85, 158–161. [Google Scholar] [CrossRef]
- Giray, E.; Yagci, I. Diagnostic accuracy of interlimb differences of ultrasonographic subcutaneous tissue thickness measurements in breast cancer-related arm lymphedema. Lymphology 2019, 52, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gebruers, N.; Verbelen, H.; De Vrieze, T.; Vos, L.; Devoogdt, N.; Fias, L.; Tjalma, W. Current and future perspectives on the evaluation, prevention and conservative management of breast cancer related lymphoedema: A best practice guideline. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 216, 245–253. [Google Scholar] [CrossRef]
- Stout Gergich, N.L.; Pfalzer, L.A.; McGarvey, C.; Springer, B.; Gerber, L.H.; Soballe, P. Preoperative assessment enables the early diagnosis and successful treatment of lymphedema. Cancer 2008, 112, 2809–2819. [Google Scholar] [CrossRef]
- Cornish, B. Bioimpedance analysis: Scientific background. Lymphat. Res. Biol. 2006, 4, 47–50. [Google Scholar] [CrossRef]
- Svensson, B.J.; Dylke, E.S.; Ward, L.C.; Kilbreath, S.L. Segmental bioimpedance informs diagnosis of breast cancer-related lymphedema. Lymphat. Res. Biol. 2017, 15, 349–355. [Google Scholar] [CrossRef]
- Dylke, E.S.; Yee, J.; Ward, L.C.; Foroughi, N.; Kilbreath, S.L. Normative volume difference between the dominant and nondominant upper limbs in healthy older women. Lymphat. Res. Biol. 2012, 10, 182–188. [Google Scholar] [CrossRef]
- Wratten, C.; Kilmurray, J.; Wright, S.; O‘Brien, P.C.; Back, M.; Hamilton, C.S.; Denham, J.W. Pilot study of high-frequency ultrasound to assess cutaneous oedema in the conservatively managed breast. Int. J. Cancer 2000, 90, 295–301. [Google Scholar] [CrossRef]
- Tassenoy, A.; Mey, J.D.; Ridder, F.D.; Schuerbeeck, P.V.; Vanderhasselt, T.; Lamote, J.; Lievens, P. Postmastectomy lymphoedema: Different patterns of fluid distribution visualised by ultrasound imaging compared with magnetic resonance imaging. Physiotherapy 2011, 97, 234–243. [Google Scholar] [CrossRef]
- van der Veen, P.; Vermeiren, K.; Von Kemp, K.; Lamote, J.; Sacre, R.; Lievens, P. A key to understanding postoperative lymphoedema: A study on the evolution and consistency of oedema of the arm using ultrasound imaging. Breast (Edinb. Scotl.) 2001, 10, 225–230. [Google Scholar] [CrossRef]
- Fumiere, E.; Leduc, O.; Fourcade, S.; Becker, C.; Garbar, C.; Demeure, R.; Wilputte, F.; Leduc, A.; Delcour, C. MR imaging, proton MR spectroscopy, ultrasonographic, histologic findings in patients with chronic lymphedema. Lymphology 2007, 40, 157–162. [Google Scholar]
- Impedimed. Measurement Guide Body Composition Analysis, 5th ed.; ImpediMed. Ltd.: Carlsbad, CA, USA, 2009; Available online: www.impedimed.com/wp-content/uploads/2019/07/SFB7MeasurementGuide.pdf (accessed on 20 October 2023).
- ALA National Council. Guideline for a National Standard Technique of Measurement of Lymphoedematous Limbs. Australas. Lymphology Assoc. 2004. Available online: https://www.lymphoedema.org.au/public/7/files/ALA_Measuring_Standard_Dec2013.pdf (accessed on 21 October 2023).
- Pappalardo, M.; Cheng, M.-H. Lymphoscintigraphy interpretation, staging, and lymphedema grading. In Principles and Practice of Lymphoedema Surgery, 2nd ed.; Cheng, M.-H., Chang, D.W., Patel, K.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2021; pp. 39–51. [Google Scholar]
- Szuba, A.; Shin, W.S.; Strauss, H.W.; Rockson, S. The third circulation: Radionuclide lymphoscintigraphy in the evaluation of lymphedema. J. Nucl. Med. 2003, 44, 43–57. [Google Scholar]
- Cheng, M.-H.; Pappalardo, M.; Lin, C.; Kuo, C.-F.; Lin, C.-Y.; Chung, K.C. Validity of the Novel Taiwan Lymphoscintigraphy Staging and Correlation of Cheng Lymphedema Grading for Unilateral Extremity Lymphedema. Ann. Surg. 2018, 268, 513–525. [Google Scholar] [CrossRef]
- Jørgensen, M.G.; Toyserkani, N.M.; Hansen, F.C.G.; Thomsen, J.B.; Sørensen, J.A. Prospective validation of indocyanine green lymphangiography staging of breast cancer-related lymphedema. Cancers 2021, 13, 1540. [Google Scholar] [CrossRef]
- Yamamoto, T.; Narushima, M.; Doi, K. Characteristic indocyanine green lymphography findings in lower extremity lymphedema: The generation of a novel lymphedema severity staging system using dermal backflow patterns. Plast Reconstr. Surg. 2011, 127, 1979–1986. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.P.; Sibley, R.C.; Friedman, R.; Kim, G.; Singhal, D.; Loening, A.M.; Tsai, L.L. MRI of Lymphedema. J. Magn. Reson. Imaging 2023, 57, 977–991. [Google Scholar] [CrossRef] [PubMed]
- Czerniec, S.A.; Ward, L.C.; Lee, M.-J.; Refshauge, K.M.; Beith, J.; Kilbreath, S.L. Segmental measurement of breast cancer-related arm lymphoedema using perometry and bioimpedance spectroscopy. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2011, 19, 703–710. [Google Scholar] [CrossRef]
- Sandby-Møller, J.; Poulsen, T.; Wulf, H.C. Epidermal thickness at different body sites: Relationship to age, gender, pigmentation, blood content, skin type and smoking habits. Acta Derm. Venereol. 2003, 83, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Crisan, D.; Lupsor, M.; Boca, A.; Crisan, M.; Badea, R. Ultrasonographic assessment of skin structure according to age. Indian J. Dermatol. Venereol. Leprol. 2012, 78, 519–527. [Google Scholar] [CrossRef]
- Lymphoedema Framework. In Best Practice for the Management of Lymphoedema [International Consensus]; MEP Ltd.: London, UK, 2006.
- Dai, M.; Sato, A.; Maeba, H.; Luchi, T.; Matsumoto, M.; Okuwa, M.; Nakatani, T.; Sanada, H.; Sugama, J. Dermal structure in lymphedema patients with history of acute dermatolymphangioadenitis evaluated by histogram analysis of ultrasonography findings: A case-control study. Lymphat. Res. Biol. 2016, 14, 2–7. [Google Scholar] [CrossRef]
- Ridner, S.H.; Dietrich, M.S.; Cowher, M.S.; Taback, B.; McLaughlin, S.; Ajkay, N.; Boyages, J.; Koelmeyer, L.; DeSnyder, S.M.; Wagner, J.; et al. A randomized trial evaluating bioimpedance spectroscopy versus tape measurement for the prevention of lymphedema following treatment for breast cancer: Interim analysis. Ann. Surg. Oncol. 2019, 26, 3250–3259. [Google Scholar] [CrossRef]
- Kaufman, D.I.; Shah, C.; Vicini, F.A.; Rizzi, M. Utilization of bioelectrical impedance spectroscopy in the prevention of chronic breast cancer-related lymphedema. Breast Cancer Res. Treat. 2017, 166, 809–815. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| A No Oedema | B Early Fluid | C High Fluid+ | D Low Fluid+ |
|---|---|---|---|
| Site does not exhibit lymphoedema characteristics | Tissue exhibits extracellular fluid increase without compositional changes | Tissue exhibits fibro-fatty changes with high fluid volume | Tissue exhibits fibro-fatty changes with low fluid volume |
| Volume- Inter-limb segment difference (% difference between lymphoedema to non-lymphoedema segment) OR Limb segment change (% change from baseline) | |||
| Within normal limits Inter-limb segment: <5.0% (Dom) <3.0% (NDom) OR Limb segment change: <3.0% | May or may not meet inter-limb threshold. OR Exceeds threshold for limb segment change: ≥3.0% | Greater than normal limits Inter-limb segment: ≥5.0% (Dom) ≥3.0% (NDom) OR Limb segment change: ≥3.0% | Greater than normal limits Inter-limb segment: ≥5.0% (Dom) ≥3.0% (NDom) OR Limb segment change: ≥3.0% |
| BIS R0- Inter-limb segment ratio (Unaffected/Affected) | |||
| Within normal limits Forearm: ≤1.1385 (Dom) ≤1.0700 (NDom) Upper Arm: ≤1.1335 (Dom) ≤1.0915 (NDom) | Greater than normal limits Forearm: >1.1385 (Dom) >1.0700 (NDom) Upper Arm: >1.1335 (Dom) >1.0915 (NDom) | Greater than normal limits Forearm: >1.1385 (Dom) >1.0700 (NDom) Upper Arm: >1.1335 (Dom) >1.0915 (NDom) | Within normal limits Forearm: ≤1.1385 (Dom) ≤1.0700 (NDom) Upper Arm: ≤1.1335 (Dom) ≤1.0915 (NDom) |
| Volume and R0 relationship | |||
| Both within normal limits | Both exceed thresholds OR R0 ratio increase and volume decrease, e.g., muscle atrophy or musculoskeletal cause | Both exceed thresholds | Both exceed thresholds. Disproportionate change, i.e., physical volume change large and R0 ratio relatively small OR Opposing direction of change, e.g., volume increase AND R0 ratio less than 1.000 |
| Ultrasound Echogenicity—Lymphoedema API compared to Non-lymphoedema API | |||
| N/A | Dermis: Hypoechoic AND Subcutis: Hypoechoic | Dermis: Hyperechoic OR Subcutis: Hyperechoic | Dermis: Hyperechoic OR Subcutis: Hyperechoic |
| Demographics | Range (Mean) | |
|---|---|---|
| Age (years) | 39–70 (58.8) | |
| BMI (kg/m2) | 19.25–43.98 (27.4) | |
| Duration since Lymphoedema Onset (years) | 0.25–10 (4.0) | |
| Arm Dominance | n (%) | |
| Ipsilateral to lymphoedema | 10 (66.7) | |
| Contralateral to lymphoedema | 5 (33.3) | |
| Surgical Procedure | Local breast excision + AD | 5 (33.3) |
| Mastectomy + AD | 9 (60.0) | |
| Double mastectomy + unilateral AD | 1 (6.7) | |
| Adjuvant Treatment | Radiation only | 2 (13.3) |
| Chemotherapy only | 2 (13.3) | |
| Both | 10 (66.7) | |
| Neither | 1 (6.7) | |
| Episodes of Cellulitis | Never | 11 (73.3) |
| Once | 1 (6.7) | |
| Multiple episodes | 3 (20.0) | |
| ISL Stage | 1 | 6 (13.3) |
| 2 | 2 (40.0) | |
| 2—late | 7 (46.7) | |
| 3 | 0 | |
| Tissue Characteristic | Mean (SD) | p-Value # | ||
|---|---|---|---|---|
| Volume | % diff inter-limb segment | 15.74 (16.08) | - | |
| Volume distribution | Uneven ≥ 10% | 53.30% | 0.023 * | |
| Even < 10% | 46.70% | |||
| Volume (mL) | Lymphoedema- affected | Unaffected | ||
| Whole limb | 2825.49 (474.84) | 2493.96 (423.96) | <0.001 * | |
| Distal segment | 887.36 (197.76) | 746.30 (135.81) | <0.001 * | |
| Proximal segment | 1932.79 (337.17) | 1753.01 (337.64) | 0.012 * | |
| Ultrasound echogenicity | Dermal | 174.87 (24.67) | 188.30 (18.27) | <0.001 * |
| Subcutaneous | 115.64 (32.67) | 118.70 (34.42) | 0.119 | |
| BIS | R zero whole limb | 292.61 (61.95) | 334.94 (43.09) | 0.003 * |
| R zero segment | ||||
| Distal | 136.42 (33.93) | 160.02 (28.54) | 0.004 * | |
| Proximal | 176.82 (37.97) | 187.89 (25.45) | 0.109 | |
| R zero ratio | 1.161 (0.209) | - | ||
| LOCAL Category | Anterior Forearm n (%) | Posterior Forearm n (%) | Upper Arm n (%) |
|---|---|---|---|
| A. No Oedema | 1 (6.6) | 1 (6.6) | 4 (26.7) |
| B. Early Fluid | 6 (40.0) | 4 (26.7) | 3 (20.0) |
| C. High Fluid+ | 4 (26.7) | 6 (40.0) | 4 (26.7) |
| D. Low Fluid+ | 4 (26.7) | 4 (26.7) | 4 (26.7) |
| Total (n) | 15 (100) | 15 (100) | 15 (100) |
| Description | Staging Details |
|---|---|
| ISL staging [2] | |
| Staging criteria include pitting, effect of limb elevation on oedema and skin changes. Easy to apply in clinical practice. Refers to tissue compositional changes but does not include objective criteria to confirm classification. | Stage 0—Subclinical, asymptomatic with known lymphatic transport impairment. Subtle symptoms and tissue changes may occur. Stage I—Early accumulation of fluid that improves or temporarily resolves with limb elevation. Pitting may occur. Stage II—Structural changes occurring within tissue layer. Oedema does not subside with elevation alone. Pitting evident up until late Stage II when excess subcutaneous fat and fibrosis develop. Stage III—Further fibrotic and fatty deposition, encompasses lymphostatic elephantiasis. Trophic skin changes. May or may not pit [2]. |
| Lymphoscintigraphy | |
| Involves injection of a radiotracer into the interstitial space of the hand or foot. Images are taken over a period to indicate migration of the tracer from the tissue space through lymphatic vasculature and nodes [22]. Assesses lymphatic fluid transport through vessels and uptake to lymphatic nodes. Assessment is lymphatic-specific for lymphoedema differential diagnosis. Can evaluate lymph transit time, dermal backflow, identify asymmetrical node uptake and collateral vessels. Can identify sentinel nodes for surgery [23]. Does not evaluate tissue layer composition changes. | Multiple protocols published with various staging criteria [22] (p. 42). The Taiwan Lymphoscintigraphy Staging tool for unilateral extremity lymphoedema classifies the imaging results into patterns of lymph node uptake at proximal and intermediate sites on the limb, then subclassifies the drainage pattern into seven stages that are encompassed within three categories: normal drainage (L-0), partial obstruction (P1, P2, P3) and total obstruction (T4, T5, T6) [24]. |
| Indocyanine green lymphangiography (ICG-L) | |
| Indocyanine green is injected intradermally and the fluorescence observed using near-infrared optical imaging. Assesses lymph uptake, transportation, drainage pathways and dermal backflow patterns. Used to inform surgical options [25]. Does not evaluate tissue composition changes. | MD Anderson ICG-L staging has 6 stages that are defined by observations of lymphatic patency and the pattern of dermal backflow. Stage 0: Normal linear lymphatics and no dermal backflow Stage 1: Many patent lymphatics and minimal lymphatic dermal backflow Stage 2: Moderate number of patent lymphatics and segmental dermal backflow Stage 3: Few patent lymphatics and extensive dermal backflow Stage 4: Dermal backflow involving the hand Stage 5: No proximal uptake of ICG from the injection site [25]. Dermal backflow patterns termed splash, stardust and diffuse, have been observed to correlate with lymphoedema severity [26]. |
| Magnetic resonance lymphangiography | |
| Magnets and radio waves are used to produce detailed images of the body including soft tissue, muscle, bone and blood vessels. When a contrasting agent is used lymphatic vessel appearance and function can be evaluated [27]. High-quality imagery technique with sequence options to clearly differentiate tissue layer composition. | Multiple grading options are described to classify components of lymphoedema presentations including fluid, fat, appearance and function of lymph vessels, honeycombing, dermal thickness and oedema distribution. Leg lymphoedema staging published by Salehi et al., 2023): Fluid accumulation grade: 0 = no fluid 1 = honeycombing/reticular pattern of fluid within the subcutaneous fat 2 = continuous visible stripe of fluid between the fat and the muscle fascia Fat accumulation grade: 0 = no excess fat 1 = fat accumulation less than twice the width of the widest fat stripe on the unaffected side 2 = fat accumulation greater than twice the width of the widest fat stripe on the unaffected side [27] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanderson, J.; Tuttle, N.; Box, R.; Reul-Hirche, H.; Laakso, E.-L. Localised Objective Characterisation Assessment of Lymphoedema (LOCAL): Using High-Frequency Ultrasound, Bioelectrical Impedance Spectroscopy and Volume to Evaluate Superficial Tissue Composition. Diagnostics 2024, 14, 1616. https://doi.org/10.3390/diagnostics14151616
Sanderson J, Tuttle N, Box R, Reul-Hirche H, Laakso E-L. Localised Objective Characterisation Assessment of Lymphoedema (LOCAL): Using High-Frequency Ultrasound, Bioelectrical Impedance Spectroscopy and Volume to Evaluate Superficial Tissue Composition. Diagnostics. 2024; 14(15):1616. https://doi.org/10.3390/diagnostics14151616
Chicago/Turabian StyleSanderson, Jennifer, Neil Tuttle, Robyn Box, Hildegard Reul-Hirche, and E-Liisa Laakso. 2024. "Localised Objective Characterisation Assessment of Lymphoedema (LOCAL): Using High-Frequency Ultrasound, Bioelectrical Impedance Spectroscopy and Volume to Evaluate Superficial Tissue Composition" Diagnostics 14, no. 15: 1616. https://doi.org/10.3390/diagnostics14151616