
Bone Marrow Disseminated Tumor Cell Detection Is Beneficial for the Early Finding of Bone Metastasis and Prognosis

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Criterion of Patient Enrolment
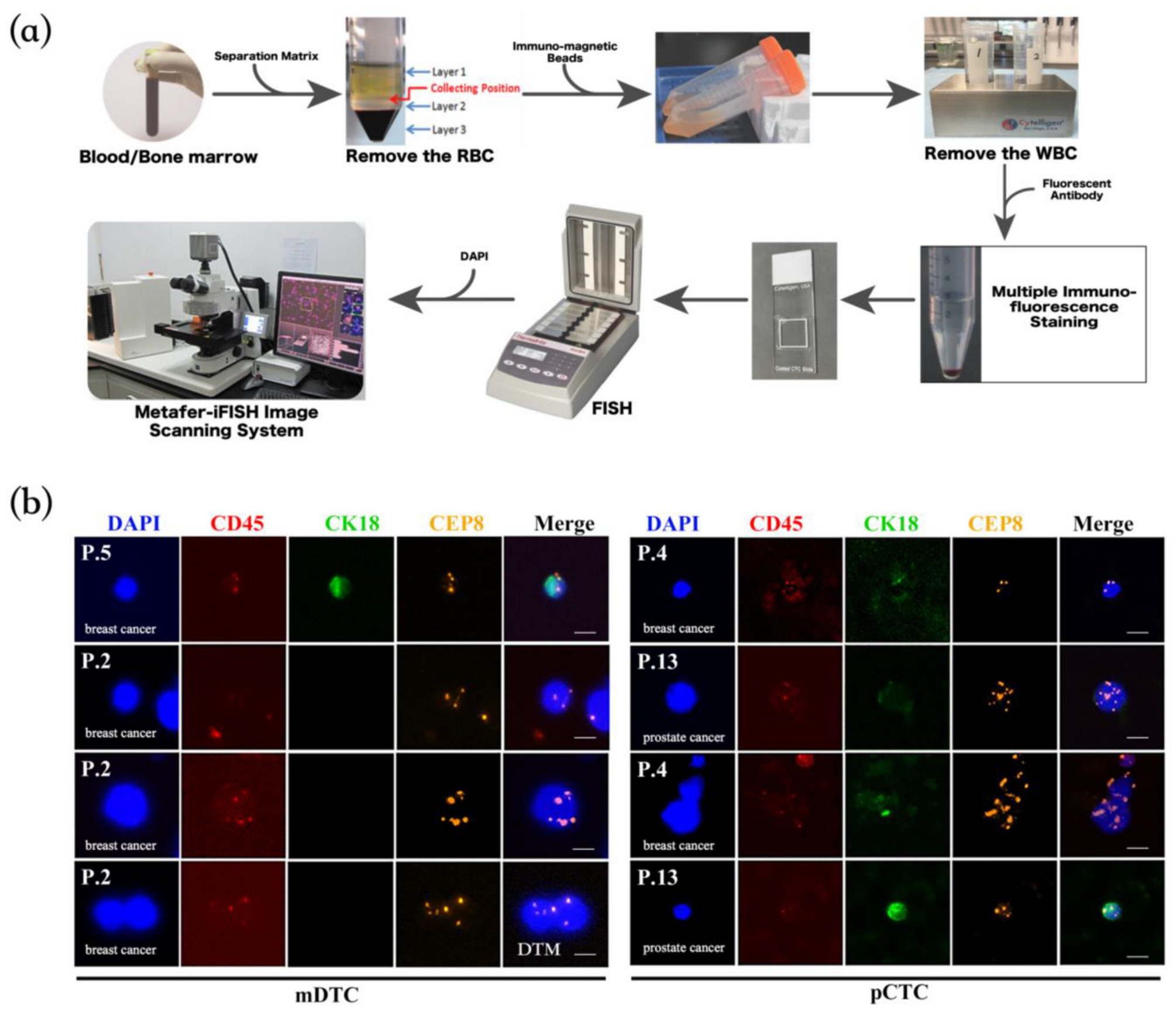
2.2. Detection and Identification of mDTCs and pCTCs by SE-iFISH
3. Statistical Analysis
4. Results
4.1. General Information of Enrolled Patients
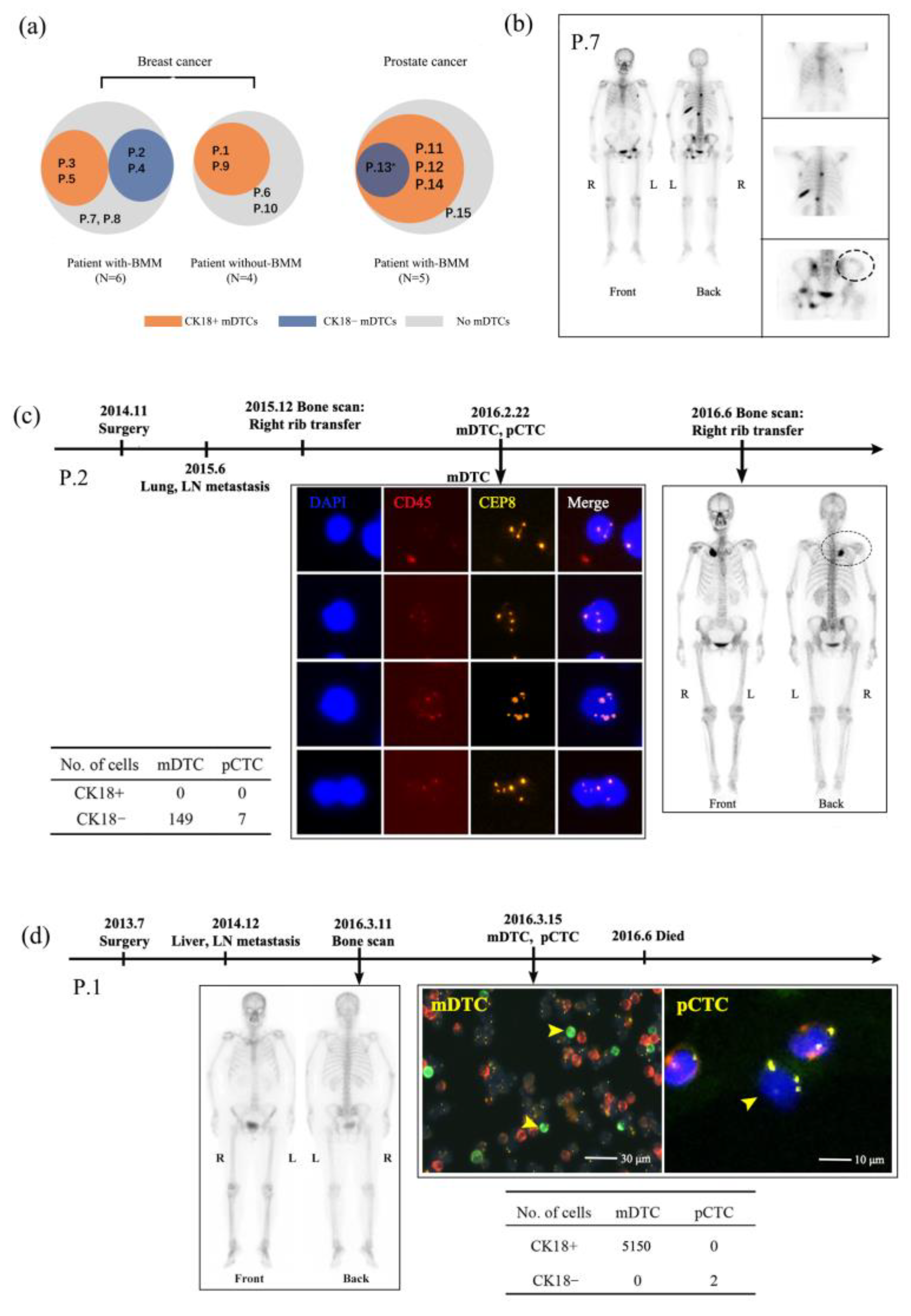
4.2. Characteristics of mDTCs and pCTCs
4.3. Case Analyses of Bone Metastases Detected by SE-iFISH and Traditional Imaging Methods
4.4. mDTCs Counts Correlated with Patients’ Overall Survival (OS)
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Valastyan, S.; Weinberg, R.A. Tumor metastasis: Molecular insights and evolving paradigms. Cell 2011, 147, 275–292. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, M.; Nosrati, R.; Salmaninejad, A.; Dehghani, S.; Shahryari, A.; Saberi, A. Organ-specific metastasis of breast cancer: Molecular and cellular mechanisms underlying lung metastasis. Cell. Oncol. 2018, 41, 123–140. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.A. Parallel progression of primary tumours and metastases. Nat. Rev. Cancer 2009, 9, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, H.; Obradovic, M.M.; Hoffmann, M.; Harper, K.L.; Sosa, M.S.; Werner-Klein, M.; Nanduri, L.K.; Werno, C.; Ehrl, C.; Maneck, M.; et al. Early dissemination seeds metastasis in breast cancer. Nature 2016, 540, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, C.; Toifl, S.; Farlik, M.; Halbritter, F.; Scheicher, R.; Fischer, I.; Sexl, V.; Bock, C.; Baccarini, M. An ERK-Dependent Feedback Mechanism Prevents Hematopoietic Stem Cell Exhaustion. Cell Stem Cell 2018, 22, 879–892.e6. [Google Scholar] [CrossRef]
- Zhang, W.; Bado, I.; Wang, H.; Lo, H.C.; Zhang, X.H. Bone Metastasis: Find Your Niche and Fit in. Trends Cancer 2019, 5, 95–110. [Google Scholar] [CrossRef]
- Sosa, M.S.; Bragado, P.; Aguirre-Ghiso, J.A. Mechanisms of disseminated cancer cell dormancy: An awakening field. Nat. Rev. Cancer 2014, 14, 611–622. [Google Scholar] [CrossRef]
- Risson, E.; Nobre, A.R.; Maguer-Satta, V.; Aguirre-Ghiso, J.A. The current paradigm and challenges ahead for the dormancy of disseminated tumor cells. Nat. Cancer 2020, 10, 672–680. [Google Scholar] [CrossRef]
- Zhang, W.; Bado, I.L.; Hu, J.; Wan, Y.W.; Wu, L.; Wang, H.; Gao, Y.; Jeong, H.H.; Xu, Z.; Hao, X.; et al. The bone microenvironment invigorates metastatic seeds for further dissemination. Cell 2021, 184, 2471–2486 e20. [Google Scholar] [CrossRef]
- Banys, M.; Hartkopf, A.D.; Krawczyk, N.; Kaiser, T.; Meier-Stiegen, F.; Fehm, T.; Neubauer, H. Dormancy in breast cancer. Breast Cancer 2012, 4, 183–191. [Google Scholar] [PubMed]
- Grzelak, C.A.; Ghajar, C.M. Metastasis ‘systems’ biology: How are macro-environmental signals transmitted into microenvironmental cues for disseminated tumor cells? Curr. Opin. Cell Biol. 2017, 48, 79–86. [Google Scholar] [CrossRef]
- Xie, J.; Ruan, Z.; Zheng, J.; Gong, Y.; Wang, Y.; Hu, B.; Cheng, J.; Huang, Q. Detection of circulating rare cells benefitted the diagnosis of malignant solitary pulmonary nodules. J. Cancer Res. Clin. Oncol. 2021, 10, 289–297. [Google Scholar] [CrossRef]
- Hu, B.; Gong, Y.; Wang, Y.; Xie, J.; Cheng, J.; Huang, Q. Comprehensive Atlas of Circulating Rare Cells Detected by SE-iFISH and Image Scanning Platform in Patients With Various Diseases. Front. Oncol. 2022, 12, 821454. [Google Scholar] [CrossRef]
- Yao, H.; Wang, Z.; Yang, J.; Xu, X.; Song, Y. Simultaneous in situ detection of protein expression of multiple tumor markers of circulating tumor cells and heteroploid of chromosome 8 in primary lung cancer. Ann. Transl. Med. 2021, 9, 1772. [Google Scholar] [CrossRef] [PubMed]
- Passerini, V.; Ozeri-Galai, E.; de Pagter, M.S.; Donnelly, N.; Schmalbrock, S.; Kloosterman, W.P.; Kerem, B.; Storchova, Z. The presence of extra chromosomes leads to genomic instability. Nat. Commun. 2016, 7, 10754. [Google Scholar] [CrossRef] [PubMed]
- Fornetti, J.; Welm, A.L.; Stewart, S.A. Understanding the Bone in Cancer Metastasis. J. Bone Miner. Res. 2018, 33, 2099–2113. [Google Scholar] [CrossRef]
- Fonti, R.; Conson, M.; Del Vecchio, S. PET/CT in radiation oncology. Semin. Oncol. 2019, 46, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Langsteger, W.; Rezaee, A.; Pirich, C.; Beheshti, M. (18)F-NaF-PET/CT and (99m)Tc-MDP Bone Scintigraphy in the Detection of Bone Metastases in Prostate Cancer. Semin. Nucl. Med. 2016, 46, 491–501. [Google Scholar] [CrossRef]
- Houssami, N.; Costelloe, C.M. Imaging bone metastases in breast cancer: Evidence on comparative test accuracy. Ann. Oncol. 2012, 23, 834–843. [Google Scholar] [CrossRef]
- Sollini, M.; Cozzi, L.; Ninatti, G.; Antunovic, L.; Cavinato, L.; Chiti, A.; Kirienko, M. PET/CT radiomics in breast cancer: Mind the step. Methods 2021, 188, 122–132. [Google Scholar] [CrossRef]
- Recasens, A.; Munoz, L. Targeting Cancer Cell Dormancy. Trends Pharmacol. Sci. 2019, 40, 128–141. [Google Scholar] [CrossRef]
- Cackowski, F.C.; Heath, E.I. Prostate cancer dormancy and recurrence. Cancer Lett. 2022, 524, 103–108. [Google Scholar] [CrossRef]
- Abderrahman, B.; Jordan, V.C. Rethinking Extended Adjuvant Antiestrogen Therapy to Increase Survivorship in Breast Cancer. JAMA Oncol. 2018, 4, 15–16. [Google Scholar] [CrossRef]
- Agarwal, A.; Balic, M.; El-Ashry, D.; Cote, R.J. Circulating Tumor Cells: Strategies for Capture, Analyses, and Propagation. Cancer J. 2018, 24, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Ben-David, U.; Amon, A. Context is everything: Aneuploidy in cancer. Nat. Rev. Genet. 2020, 21, 44–62. [Google Scholar] [CrossRef] [PubMed]
- Giam, M.; Rancati, G. Aneuploidy and chromosomal instability in cancer: A jackpot to chaos. Cell Div. 2015, 10, 3. [Google Scholar] [CrossRef]
- Doak, S.H.; Jenkins, G.J.S.; Parry, E.M.; D’Souza, F.R.; Griffiths, A.P.; Baxter, J.N.; Parry, J.M. Chromosome 4 hyperploidy represents an early genetic aberration in premalignant Barrett’s oesophagus. Gut 2003, 52, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Cappuzzo, F.; Varella-Garcia, M.; Rossi, E.; Gajapathy, S.; Valente, M.; Drabkin, H.; Gemmill, R. MYC and EIF3H Coamplification Significantly Improve Response and Survival of Non-small Cell Lung Cancer Patients (NSCLC) Treated with Gefitinib. J. Thorac. Oncol. 2009, 4, 472–478. [Google Scholar] [CrossRef]
- Richter, F.; Baratay, A.; Roder, C.; Egberts, J.H.; Kalthoff, H.; Becker, T.; Sebens, S. Comparative Analysis of Blood and Bone Marrow for the Detection of Circulating and Disseminated Tumor Cells and Their Prognostic and Predictive Value in Esophageal Cancer Patients. J. Clin. Med. 2020, 9, 2674. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Gender | Age (yrs) | Stage | Sites of Bone Metastasis | Method Used for Bone Metastasis | Sites of Metastasis Other Than Bone | Treatment Ongoing | Treatment Duration |
|---|---|---|---|---|---|---|---|---|
| Breast cancer patients | ||||||||
| 1 | Female | 59 | IV | No | BS | Li, LN | Chemo | 3 mths |
| 2 | Female | 63 | IV | Right first anterior rib (without ilium) | BS | Lu, LN, AF | Chemo | 2 mths |
| 3 | Female | 56 | IV | Hip joint, lumbar spine, sacral spine, skull, humerus, shoulders, sternum, spine, bilateral ribs, bilateral femurs, and pelvic bones (possibly including ilium) | BS | No | Chemo + Endo | 6 mths |
| 4 | Female | 69 | IV | Thoracic spine, ribs, lower lumbar spine, femur, right humerus, and pelvic bones (possibly including ilium) | BS | LN | Endo | 3 mths |
| 5 | Female | 56 | IV | Ribs, sternum, lumbar vertebrae, and pelvic bones (possibly including ilium) | CT, MRI | No | Chemo | 2 mths |
| 6 | Female | 46 | IV | No | BS | Lu | Before treatment | - |
| 7 | Female | 61 | IV | Multiple ribs, left sacroiliac joint, left ischium, left upper femur, and femoral head (without ilium) | BS | Lu, Li | Chemo + Target | 3 mths |
| 8 | Female | 60 | IV | S1–3 vertebral bodies (without ilium) | PET-CT | Lu, Br, LN, Pl | Endo | 1 year |
| 9 | Female | 65 | II | No | BS | No * | Endo | 6 mths |
| 10 | Female | 69 | II | No | PET-CT | LN | Before-treat | - |
| Prostatic cancer patients | ||||||||
| 11 | Male | 63 | IV | Pelvis, femur, thoracic spine, ribs, and bilateral ilium | BS | No | Chemo | 3 mths |
| 12 | Male | 76 | IV | Lower thoracic lumbar spine, sacrum, and bilateral ilium | BS | No | New diagnostic # | - |
| 13 | Male | 82 | IV | Humerus, clavicle, ribs, sacroiliac joint, and ilium | BS | No | Endo | 8 mths |
| 14 | Male | 75 | IV | L4-S3 vertebrae, scapula, femur, pelvis, and ilium | BS | LN | Endo | 9 mths |
| 15 | Male | 68 | IV | Ribs, thoracic spine, sternum, and pelvic wall (without ilium) | CT, MRI | Li, LN, PC | Endo | 4 mths |
| Number | mDTCs Number | pCTCs Number | Serum Tumor Markers | Primary Tumor Tissue | Metastatic Tissue | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CK+ | CK− | DTM | CK+ | CK− | CTM | CEA | CA724 | CA153 | CA199 | CA125 | PSA | fPSA | fPSA/PSA | ER | PR | HER-2 | ER | PR | HER-2 | |
| Breast cancer patients | ||||||||||||||||||||
| 1 | 5150 | 0 | 0 | 0 | 2 | 0 | 236.7 | 4.2 | 6.9 | 6.5 | 7.0 | / | / | / | + | − | − | NA | NA | NA |
| 2 | 0 | 149 | 4 | 0 | 7 | 0 | 1.4 | 7.1 | 14.4 | 4.5 | 21.4 | / | / | / | − | − | − | − | + | + |
| 3 | 14,370 | 0 | 0 | 0 | 7 | 0 | 3.3 | 14.5 | 22.3 | 24.6 | 29.7 | / | / | / | − | + | − | NA | NA | NA |
| 4 | 0 | 8 | 0 | 0 | 48 | 2 | 138.4 | 1.1 | 187.1 | 53.0 | 204.2 | / | / | / | NA | NA | NA | + | + | + |
| 5 | 21 | 0 | 1 | 13 | 209 | 14 | 24.0 | / | 113.7 | 19.6 | 26.9 | / | / | / | + | + | − | − | − | − |
| 6 | 0 | 0 | 0 | 0 | 29 | 1 | 0.9 | 0.8 | 8.9 | 2.8 | 27.6 | / | / | / | − | − | +++ | − | − | +++ |
| 7 | 0 | 0 | 0 | 0 | 0 | 0 | 253.0 | 1.9 | 257.4 | 22.7 | 597.0 | / | / | / | ++ | ++ | +++ | − | − | +++ |
| 8 | 0 | 0 | 0 | 0 | 4 | 0 | 7.8 | 2.6 | 11.1 | 27.9 | 252.7 | / | / | / | + | − | +++ | NA | NA | NA |
| 9 | 2 | 0 | 0 | 0 | 5 | 1 | 0.9 | 2.0 | 10.7 | 9.2 | 6.5 | / | / | / | NA | NA | NA | + | + | ++ |
| 10 | 0 | 0 | 0 | 0 | 5 | 0 | 3.6 | 3.3 | 5.2 | 22.1 | 14.8 | / | / | / | − | − | ++ | NA | NA | NA |
| Prostate cancer patients | ||||||||||||||||||||
| 11 | 642 | 0 | 0 | 0 | 45 | 3 | 4.6 | 74.1 | 37.5 | 0.8 | 11.7 | 151 | 20.1 | 13.3 | / | / | / | / | / | / |
| 12 | 50 | 0 | 18 | 0 | 2 | 0 | 2.2 | 4.7 | 15.0 | 10.2 | 11.8 | 81.8 | 13.3 | 16.3 | / | / | / | / | / | / |
| 13 | 11 | 35 | 5 | 3 | 34 | 0 | 3.0 | 8.0 | / | 25.3 | 6.2 | 108. | 11.4 | 10.5 | / | / | / | / | / | / |
| 14 | 10 | 0 | 0 | 0 | 28 | 1 | 3.3 | 1.1 | 6.8 | 7.1 | 310.5 | 2.17 | 0.69 | 31.8 | / | / | / | / | / | / |
| 15 | 0 | 0 | 0 | 2 | 50 | 0 | 3.4 | 3.3 | 16.6 | 56.1 | 17.4 | 151 | 20.1 | 13.3 | / | / | / | / | / | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Liu, J.; Gong, Y.; Hu, B.; Xie, J.; Cheng, J.; Huang, Q. Bone Marrow Disseminated Tumor Cell Detection Is Beneficial for the Early Finding of Bone Metastasis and Prognosis. Diagnostics 2024, 14, 1629. https://doi.org/10.3390/diagnostics14151629
Wang Y, Liu J, Gong Y, Hu B, Xie J, Cheng J, Huang Q. Bone Marrow Disseminated Tumor Cell Detection Is Beneficial for the Early Finding of Bone Metastasis and Prognosis. Diagnostics. 2024; 14(15):1629. https://doi.org/10.3390/diagnostics14151629
Chicago/Turabian StyleWang, Yulan, Jun Liu, Yanping Gong, Binjie Hu, Jianzhu Xie, Jin Cheng, and Qian Huang. 2024. "Bone Marrow Disseminated Tumor Cell Detection Is Beneficial for the Early Finding of Bone Metastasis and Prognosis" Diagnostics 14, no. 15: 1629. https://doi.org/10.3390/diagnostics14151629