
An Automated Real-Time PCR Assay versus Next-Generation Sequencing in the Detection of BRAF V600 Mutations in Melanoma Tissue Samples

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Samples and Mutation Testing
2.3. Next-Generation Sequencing (NGS) Protocol
2.4. IdyllaTM Protocol
2.5. Statistics
2.6. Ethics Statement
3. Results
3.1. Patient Characteristics
3.2. Technical Data
3.3. Comparative Results of BRAF Testing Using NGS and the IdyllaTM Platform
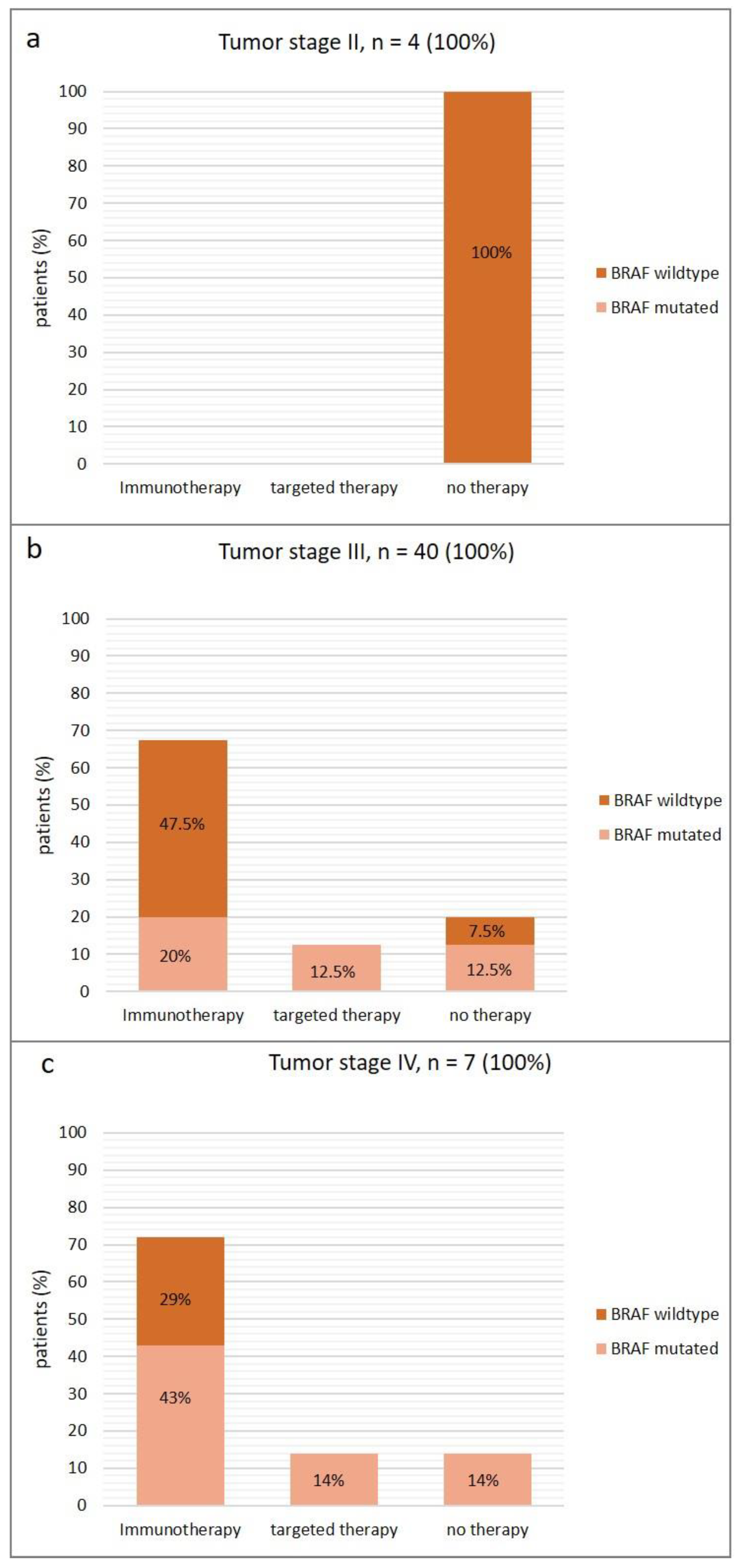
3.4. Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sosman, J.A.; Kim, K.B.; Schuchter, L.; Gonzalez, R.; Pavlick, A.C.; Weber, J.S.; McArthur, G.A.; Hutson, T.E.; Moschos, S.J.; Flaherty, K.T.; et al. Survival in BRAF V600-mutant advanced melanoma treated with vemurafenib. N. Engl. J. Med. 2012, 366, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Kirkwood, J.M.; Grob, J.-J.; Simeone, E.; Grimaldi, A.M.; Maio, M.; Palmieri, G.; Testori, A.; Marincola, F.M.; Mozzillo, N. The role of BRAF V600 mutation in melanoma. J. Transl. Med. 2012, 10, 85. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Grob, J.-J.; Nathan, P.; Ribas, A.; Robert, C.; Schadendorf, D.; Lane, S.R.; Mak, C.; Legenne, P.; Flaherty, K.T.; et al. Factors predictive of response, disease progression, and overall survival after dabrafenib and trametinib combination treatment: A pooled analysis of individual patient data from randomised trials. Lancet Oncol. 2016, 17, 1743–1754. [Google Scholar] [CrossRef] [PubMed]
- Schummer, P.; Schilling, B.; Gesierich, A. Long-Term Outcomes in BRAF-Mutated Melanoma Treated with Combined Targeted Therapy or Immune Checkpoint Blockade: Are We Approaching a True Cure? Am. J. Clin. Dermatol. 2020, 21, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Reiman, A.; Kikuchi, H.; Scocchia, D.; Smith, P.; Tsang, Y.W.; Snead, D.; Cree, I.A. Validation of an NGS mutation detection panel for melanoma. BMC Cancer 2017, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.L.; Zhou, L.; Sadri, N. Comparison of targeted next generation sequencing (NGS) versus isolated BRAF V600E analysis in patients with metastatic melanoma. Virchows. Archiv. 2018, 473, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Barel, F.; Guibourg, B.; Lambros, L.; Le Flahec, G.; Marcorelles, P.; Uguen, A. Evaluation of a Rapid, Fully Automated Platform for Detection of BRAF and NRAS Mutations in Melanoma. Acta Derm. Venereol. 2018, 98, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Marine, R.L.; Magaña, L.C.; Castro, C.J.; Zhao, K.; Montmayeur, A.M.; Schmidt, A.; Diez-Valcarce, M.; Ng, T.F.F.; Vinjé, J.; Burns, C.C.; et al. Comparison of Illumina MiSeq and the Ion Torrent PGM and S5 platforms for whole-genome sequencing of picornaviruses and caliciviruses. J. Virol. Methods 2020, 280, 113865. [Google Scholar] [CrossRef]
- Vanni, I.; Tanda, E.T.; Spagnolo, F.; Andreotti, V.; Bruno, W.; Ghiorzo, P. The Current State of Molecular Testing in the BRAF-Mutated Melanoma Landscape. Front. Mol. Biosci. 2020, 7, 113. [Google Scholar] [CrossRef]
- Tos, T.; Klyver, H.; Drzewiecki, K.T. Extensive screening for primary tumor is redundant in melanoma of unknown primary. J. Surg. Oncol. 2011, 104, 724–727. [Google Scholar] [CrossRef] [PubMed]
- Schiefer, A.-I.; Parlow, L.; Gabler, L.; Mesteri, I.; Koperek, O.; von Deimling, A.; Streubel, B.; Preusser, M.; Lehmann, A.; Kellner, U.; et al. Multicenter Evaluation of a Novel Automated Rapid Detection System of BRAF Status in Formalin-Fixed, Paraffin-Embedded Tissues. J. Mol. Diagn. 2016, 18, 370–377. [Google Scholar] [CrossRef]
- Behnke, A.; Cayre, A.; De Maglio, G.; Giannini, G.; Habran, L.; Tarsitano, M.; Chetta, M.; Cappellen, D.; Lespagnol, A.; Le Naoures, C.; et al. FACILITATE: A real-world, multicenter, prospective study investigating the utility of a rapid, fully automated real-time PCR assay versus local reference methods for detecting epidermal growth factor receptor variants in NSCLC. Pathol. Oncol. Res. 2023, 29, 1610707. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Mandalà, M.; Ferrucci, P.F.; Guidoboni, M.; Rutkowski, P.; Ferraresi, V.; Arance, A.; Guida, M.; Maiello, E.; Gogas, H.; et al. Sequencing of Ipilimumab Plus Nivolumab and Encorafenib Plus Binimetinib for Untreated BRAF-Mutated Metastatic Melanoma (SECOMBIT): A Randomized, Three-Arm, Open-Label Phase II Trial. J. Clin. Oncol. 2023, 41, 212–221. [Google Scholar] [CrossRef]
- Atkins, M.B.; Lee, S.J.; Chmielowski, B.; Tarhini, A.A.; Cohen, G.I.; Truong, T.-G.; Moon, H.H.; Davar, D.; O’Rourke, M.; Stephenson, J.J.; et al. Combination Dabrafenib and Trametinib Versus Combination Nivolumab and Ipilimumab for Patients With Advanced BRAF-Mutant Melanoma: The DREAMseq Trial-ECOG-ACRIN EA6134. J. Clin. Oncol. 2023, 41, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Menzer, C.; Menzies, A.M.; Carlino, M.S.; Reijers, I.; Groen, E.J.; Eigentler, T.; de Groot, J.W.B.; van der Veldt, A.A.; Johnson, D.B.; Meiss, F.; et al. Targeted Therapy in Advanced Melanoma With Rare BRAF Mutations. J. Clin. Oncol. 2019, 37, 3142–3151. [Google Scholar] [CrossRef] [PubMed]
- Melchior, L.; Grauslund, M.; Bellosillo, B.; Montagut, C.; Torres, E.; Moragón, E.; Micalessi, I.; Frans, J.; Noten, V.; Bourgain, C.; et al. Multi-center evaluation of the novel fully-automated PCR-based Idylla BRAF Mutation Test on formalin-fixed paraffin-embedded tissue of malignant melanoma. Exp. Mol. Pathol. 2015, 99, 485–491. [Google Scholar] [CrossRef]
- Luke, J.J.; Rutkowski, P.; Queirolo, P.; Del Vecchio, M.; Mackiewicz, J.; Chiarion-Sileni, V.; de la Cruz Merino, L.; Khattak, M.A.; Schadendorf, D.; Long, G.V.; et al. Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): A randomised, double-blind, phase 3 trial. Lancet 2022, 399, 1718–1729. [Google Scholar] [CrossRef]
- Balch, C.M.; Gershenwald, J.E.; Soong, S.-J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final version of 2009 AJCC melanoma staging and classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef]
- Weber, J.; Mandalà, M.; Del Vecchio, M.; Gogas, H.J.; Arance, A.M.; Cowey, C.L.; Dalle, S.; Schenker, M.; Chiarion-Sileni, V.; Marquez-Rodas, I.; et al. Adjuvant Nivolumab versus Ipilimumab in Resected Stage III or IV Melanoma. N. Engl. J. Med. 2017, 377, 1824–1835. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Blank, C.U.; Mandalà, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Lichinitser, M.; Khattak, A.; Carlino, M.S.; et al. Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N. Engl. J. Med. 2018, 378, 1789–1801. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandalà, M.; Chiarion-Sileni, V.; Larkin, J.; Nyakas, M.; Dutriaux, C.; Haydon, A.; et al. Adjuvant Dabrafenib plus Trametinib in Stage III BRAF-Mutated Melanoma. N. Engl. J. Med. 2017, 377, 1813–1823. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Value |
|---|---|
| Total, n | 51 |
| Age, years, mean, (SD; range) | 67 (14; 31–92) |
| Sex, n (%) | |
| Male | 18 (35) |
| Female | 33 (65) |
| Localization of primary tumor, n (%) | |
| Trunk | 9 (18) |
| Head | 2 (4) |
| Arms | 13 (25) |
| Legs | 17 (33) |
| Occult | 10 (20) |
| Tumor subtype, n (%) | |
| Nodular melanoma | 18 (35) |
| Superficial spreading melanoma | 17 (33) |
| Acral lentiginous melanoma | 3 (6) |
| Occult melanoma | 10 (20) |
| No subtype specified | 3 (6) |
| Ulceration, n (%) | |
| Yes | 17 (33) |
| No | 23 (45) |
| Not specified | 11 (22) |
| Breslow tumor thickness, mm, mean (SD; range) | 3.5 (3; 0.9–17) |
| Breslow tumor thickness/T-stage (TNM classification, AJCC 2018), number of patients (%) | |
| ≤1.0 mm/T1 | 2 (4) |
| >1.0–2.0 mm/T2 | 14 (27) |
| >2.0–4.0 mm/T3 | 11 (22) |
| >4.0 mm/T4 | 13 (25) |
| Occult/no T-stage specified | 11 (22) |
| Melanoma stage (8th edition, AJCC 2018) | |
| II, n (%) | 4 (8) |
| III, n (%) | 40 (78) |
| IV, n (%) | 7 (14) |
| Characteristics | Number |
|---|---|
| Tumor tissue | |
| Primary tumor n (%) | 30 (59) |
| Metastases, n (%), thereof | 21 (41) |
| 4 (19) |
| 17 (81) |
| Percentage of tumor cells, mean (SD; range) | 81 (15; 15–95) |
| Tumor surface in mm2, mean (SD; range) | 88 (77; 10–400) |
| DNA amount for NGS, ng/µL, mean (SD; range) | 56 (30; 5–120) |
| Number of sections, mean (SD; range) | |
| NGS | 6 (5; 1–20) |
| IdyllaTM | 3 (3; 1–14) |
| Characteristics | NGS | IdyllaTM |
|---|---|---|
| BRAF mutated, n (%) | 23 (45) | 23 (45) |
| 42 (20; 6–84) | |
| BRAF p.V600E | 21 (91) | |
| BRAF p.V600K | 2 (9) | |
| BRAF wildtype, n (%) | 28 (55) | 28 (55) |
| NRAS mutation | 17 (33) | |
| Atypical BRAF mutation | 1 (2) | |
| 1 | |
| Atypical BRAF and NRAS mutation | 2 (4) | |
| 1 | |
| 1 | |
| KRAS mutation | 1 (2) | |
| MAP2K mutation | 1 (2) | |
| Atypical BRAF and MAP2K mutation | 1 (2) | |
| 1 | |
| No mutation detected | 5 (10) | |
| Mean analytical time, days (SD) | 12.2 (4.7) | 0.2 (0.7) |
| Mean clinical time, days (SD) | 17.5 (7.3) | 5.5 (6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenders, D.; Bonzheim, I.; Hahn, M.; Gassenmaier, M.; Aebischer, V.; Forschner, A.; Lenders, M.M.; Flatz, L.; Forchhammer, S. An Automated Real-Time PCR Assay versus Next-Generation Sequencing in the Detection of BRAF V600 Mutations in Melanoma Tissue Samples. Diagnostics 2024, 14, 1644. https://doi.org/10.3390/diagnostics14151644
Lenders D, Bonzheim I, Hahn M, Gassenmaier M, Aebischer V, Forschner A, Lenders MM, Flatz L, Forchhammer S. An Automated Real-Time PCR Assay versus Next-Generation Sequencing in the Detection of BRAF V600 Mutations in Melanoma Tissue Samples. Diagnostics. 2024; 14(15):1644. https://doi.org/10.3390/diagnostics14151644
Chicago/Turabian StyleLenders, Daniela, Irina Bonzheim, Matthias Hahn, Maximilian Gassenmaier, Valentin Aebischer, Andrea Forschner, Max Matthias Lenders, Lukas Flatz, and Stephan Forchhammer. 2024. "An Automated Real-Time PCR Assay versus Next-Generation Sequencing in the Detection of BRAF V600 Mutations in Melanoma Tissue Samples" Diagnostics 14, no. 15: 1644. https://doi.org/10.3390/diagnostics14151644
APA StyleLenders, D., Bonzheim, I., Hahn, M., Gassenmaier, M., Aebischer, V., Forschner, A., Lenders, M. M., Flatz, L., & Forchhammer, S. (2024). An Automated Real-Time PCR Assay versus Next-Generation Sequencing in the Detection of BRAF V600 Mutations in Melanoma Tissue Samples. Diagnostics, 14(15), 1644. https://doi.org/10.3390/diagnostics14151644