
Evaluation of Progressive Architectural Distortion in Idiopathic Pulmonary Fibrosis Using Deformable Registration of Sequential CT Images
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
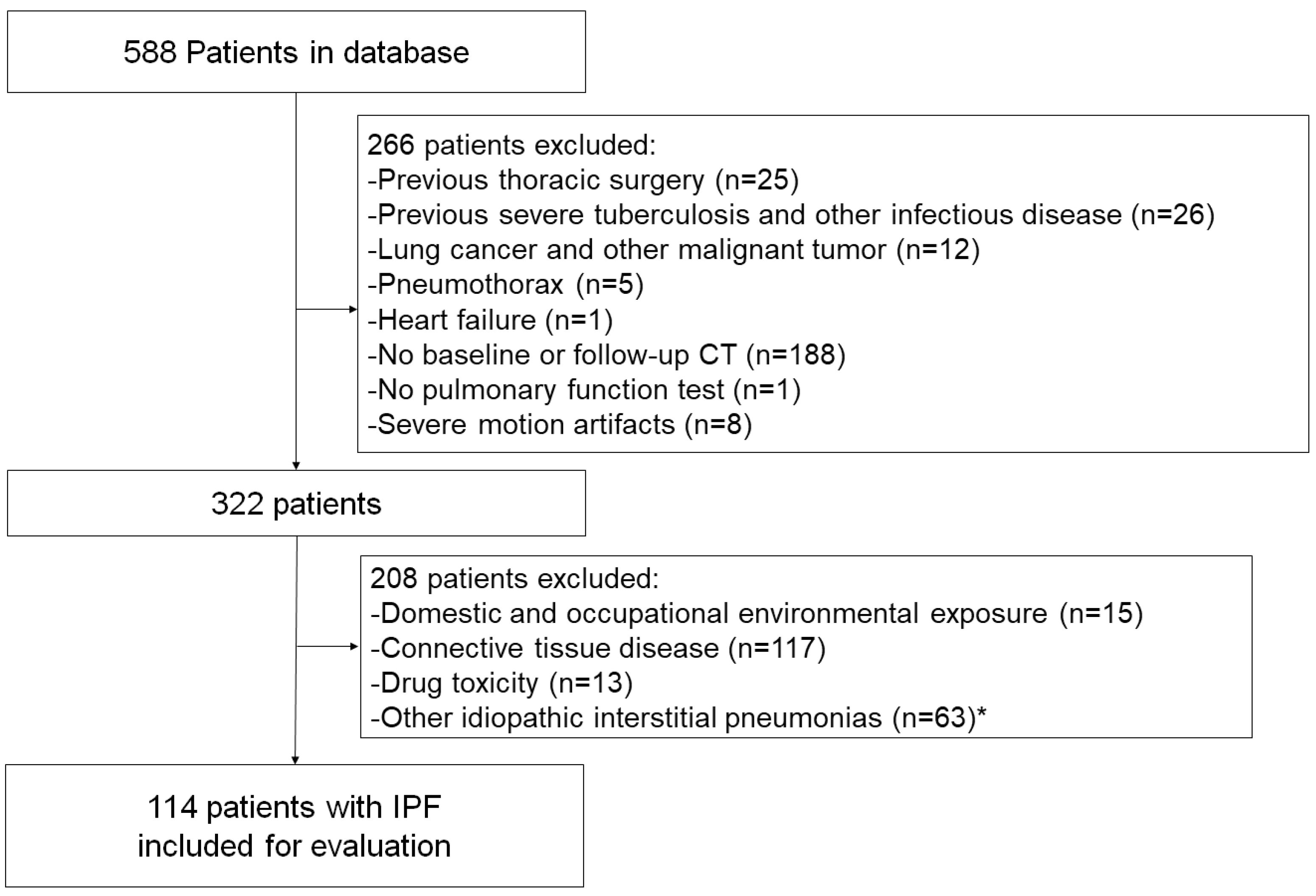
2.1. Study Design and Patient Population
2.2. CT Data Acquisition
2.3. Quantitative Evaluation
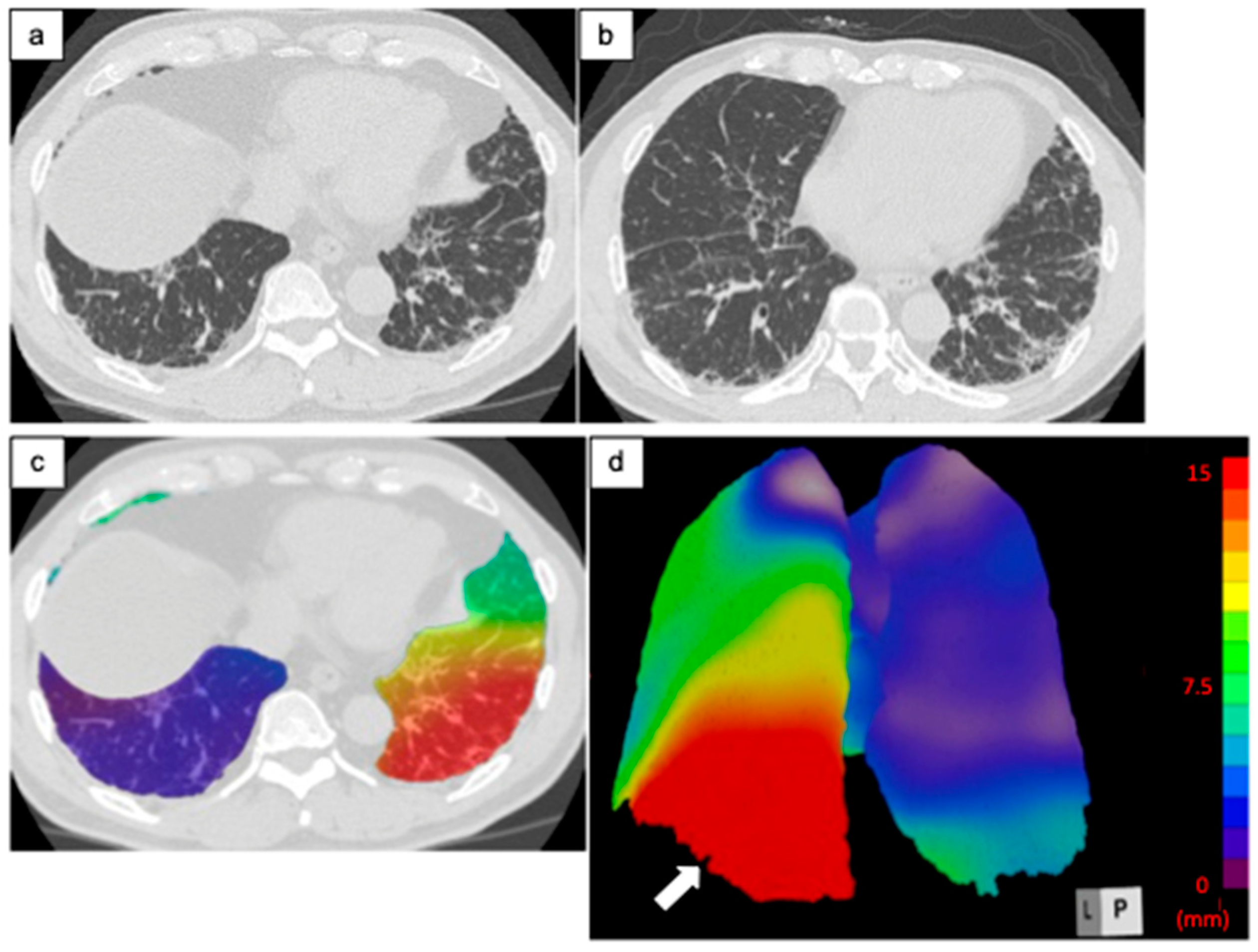
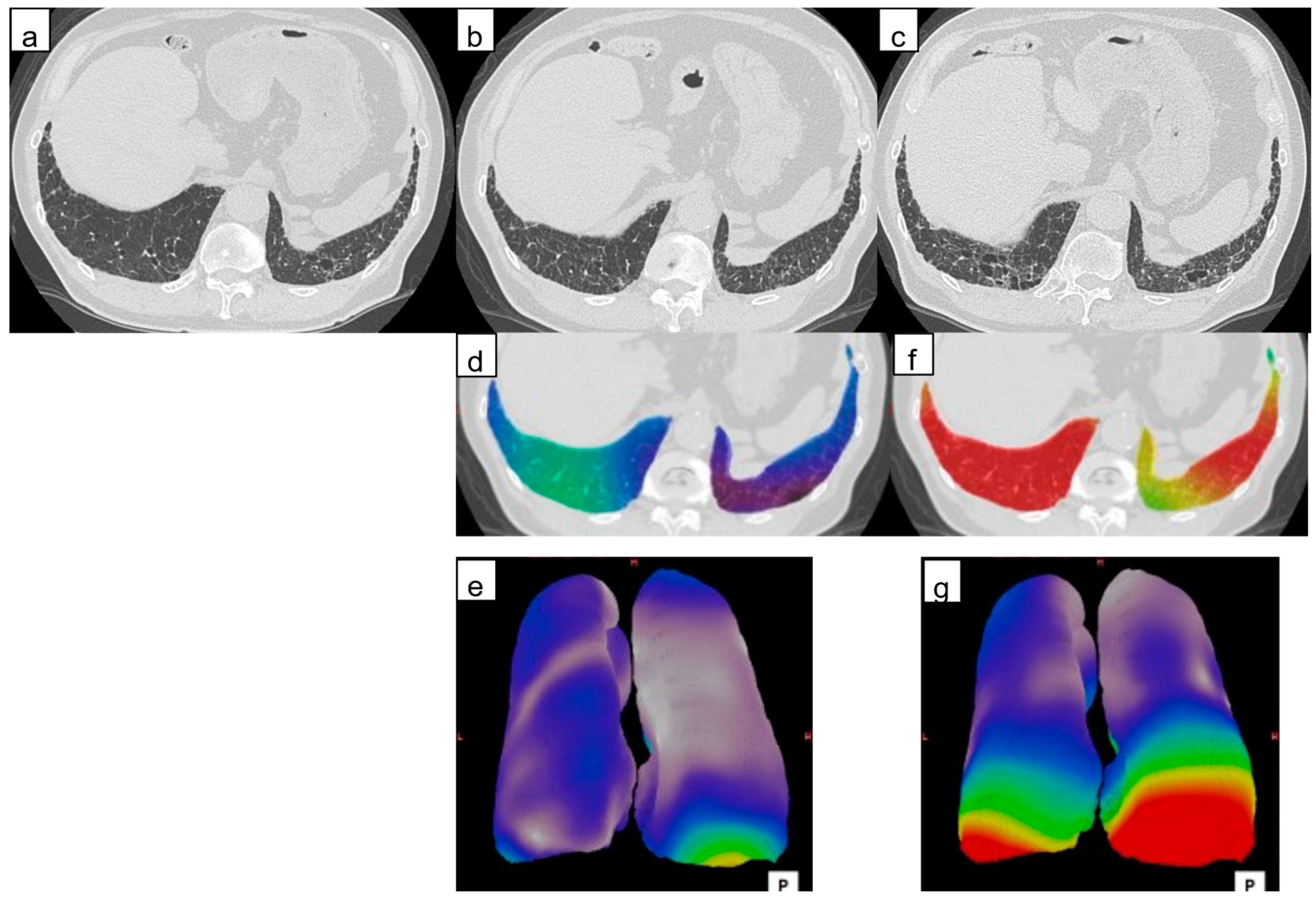
2.3.1. Architectural Distortion Measurement by 3D-AD
2.3.2. ILD Characterization and Lesion Volume
2.4. Relationship of Lung Quantification Results and Prognosis
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Quantitative Evaluation
3.2.1. Architectural Distortion Measurement by 3D-AD
3.2.2. ILD Characterization and Lesion Volume
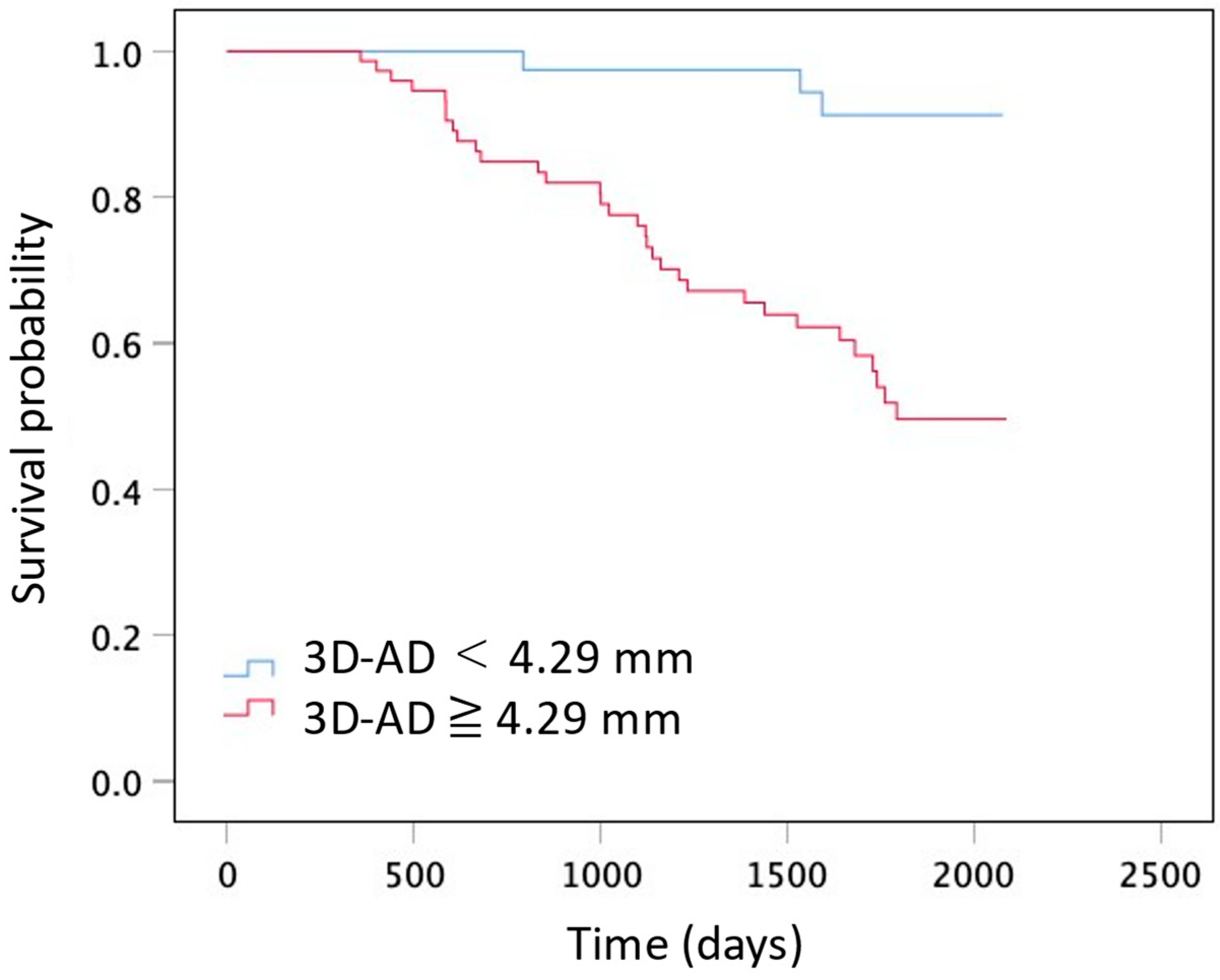
3.3. Relationship of Lung Quantification Results and Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raghu, G.; Remy-Jardin, M.; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: An official ATS/ERS/JRS/ALAT clinical practice guideline. Am. J. Respir. Crit. Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Lee, K.S.; Jeong, Y.J.; Hwang, J.H.; Kim, H.J.; Chung, M.P.; Han, J. High-resolution CT findings in fibrotic idiopathic interstitial pneumonias with little honeycombing: Serial changes and prognostic implications. AJR Am. J. Roentgenol. 2012, 199, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Aksman, L.; Mogulkoc, N.; Procter, A.J.; Gholipour, B.; Cross, G.; Barnett, J.; Brereton, C.J.; Jones, M.G.; van Moorsel, C.H.; et al. Serial CT analysis in idiopathic pulmonary fibrosis: Comparison of visual features that determine patient outcome. Thorax 2020, 75, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; Kokosi, M.; Nair, A.; Karwoski, R.; Raghunath, S.M.; Walsh, S.L.F.; Wells, A.U.; Hansell, D.M. Automated quantitative computed tomography versus visual computed tomography scoring in idiopathic pulmonary fibrosis: Validation against pulmonary function. J. Thorac. Imaging 2016, 31, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, M.L.; Lynch, D.A.; van Beek, E.J.R.; Kazerooni, E.A.; Guo, J.; Xia, M.; Murray, S.; Anstrom, K.J.; Yow, E.; Martinez, F.J.; et al. Idiopathic Pulmonary Fibrosis: The Association between the Adaptive Multiple Features Method and Fibrosis Outcomes. Am. J. Respir. Crit. Care Med. 2017, 195, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Katzenstein, A.L. Katzenstein and Askin’s Surgical Pathology of Non-Neoplastic Lung Disease, 4th ed.; Saunders Elsevier: Philadelphia, PA, USA, 2006; pp. 51–84. [Google Scholar]
- Nakagawa, H.; Nagatani, Y.; Takahashi, M.; Ogawa, E.; Tho, N.V.; Ryujin, Y.; Nagao, T.; Nakano, Y. Quantitative CT analysis of honeycombing area in idiopathic pulmonary fibrosis: Correlations with pulmonary function tests. Eur. J. Radiol. 2016, 85, 125–130. [Google Scholar] [CrossRef]
- Desai, S.R.; Lynch, D.A.; Elicker, B.M.; Devaraj, A.; Sverzellati, N. High-Resolution CT of the Lung, 6th ed.; Wolters Kluwer: Philaderphia, PA, USA, 2021; pp. 636–653. [Google Scholar]
- Lynch, D.A.; Travis, W.D.; Müller, N.L.; Galvin, J.R.; Hansell, D.M.; Grenier, P.A.; King, T.E. Idiopathic interstitial pneumonias: CT features. Radiology 2005, 236, 10–21. [Google Scholar] [CrossRef]
- Hill, D.L.; Batchelor, P.G.; Holden, M.; Hawkes, D.J. Medical image registration. Phys. Med. Biol. 2001, 46, R1–R45. [Google Scholar] [CrossRef]
- Sotiras, A.; Davatzikos, C.; Paragios, N. Deformable medical image registration: A survey. IEEE Trans. Med. Imaging 2013, 32, 1153–1190. [Google Scholar] [CrossRef]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.F.; Flaherty, K.R.; Lasky, J.A.; et al. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Antoniou, K.M.; Brown, K.K.; Cadranel, J.; Corte, T.J.; du Bois, R.M.; Lee, J.S.; Leslie, K.O.; Lynch, D.A.; Matteson, E.L.; et al. An official European Respiratory Society/American Thoracic Society research statement: Interstitial pneumonia with autoimmune features. Eur. Respir. J. 2015, 46, 976–987. [Google Scholar] [CrossRef]
- Valentin, J. International Commission on Radiation Protection. Managing Patient Dose in Multi-Detector Computed Tomography (MDCT); ICRP Publication 102; Elsevier: New York, NY, USA, 2007; Volume 37, pp. 1–79. [Google Scholar] [CrossRef]
- Mattes, D.; Haynor, D.R.; Vesselle, H.; Lewellyn, T.K.; Eubank, W. Nonrigid Multimodality Image Registration; SPIE: Bellingham, WA, USA, 2001; Volume 4322, pp. 1609–1620. [Google Scholar]
- Aoki, R.; Iwasawa, T.; Saka, T.; Yamashiro, T.; Utsunomiya, D.; Misumi, T.; Baba, T.; Ogura, T. Effects of automatic deep-learning-based lung analysis on quantification of interstitial lung disease: Correlation with pulmonary function test results and prognosis. Diagnostics 2022, 12, 3038. [Google Scholar] [CrossRef]
- Reid, L.; Simon, G. The peripheral pattern in the normal bronchogram and its relation to peripheral pulmonary anatomy. Thorax 1958, 13, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Lynch, D.A.; Sverzellati, N.; Travis, W.D.; Brown, K.K.; Colby, T.V.; Galvin, J.R.; Goldin, J.G.; Hansell, D.M.; Inoue, Y.; Johkoh, T.; et al. Diagnostic criteria for idiopathic pulmonary fibrosis: A Fleischner Society White Paper. Lancet Respir. Med. 2018, 6, 138–153. [Google Scholar] [CrossRef] [PubMed]
- Iwasawa, T.; Takemura, T.; Okudera, K.; Gotoh, T.; Iwao, Y.; Kitamura, H.; Baba, T.; Ogura, T.; Oba, M.S. The importance of subpleural fibrosis in the prognosis of patients with idiopathic interstitial pneumonias. Eur. J. Radiol. 2017, 90, 106–113. [Google Scholar] [CrossRef]
- Jacob, J.; Bartholmai, B.J.; Rajagopalan, S.; Kokosi, M.; Nair, A.; Karwoski, R.; Walsh, S.L.F.; Wells, A.U.; Hansell, D.M. Mortality prediction in idiopathic pulmonary fibrosis: Evaluation of computer-based CT analysis with conventional severity measures. Eur. Respir. J. 2017, 49, 1601011. [Google Scholar] [CrossRef] [PubMed]
- Reichmann, W.M.; Yu, Y.F.; Macaulay, D.; Wu, E.Q.; Nathan, S.D. Change in forced vital capacity and associated subsequent outcomes in patients with newly diagnosed idiopathic pulmonary fibrosis. BMC Pulm. Med. 2015, 15, 167. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Seo, J.B.; Oh, S.Y.; Kim, T.H.; Song, J.W.; Lee, S.M.; Kim, N. Prediction of survival by texture-based automated quantitative assessment of regional disease patterns on CT in idiopathic pulmonary fibrosis. Eur. Radiol. 2018, 28, 1293–1300. [Google Scholar] [CrossRef]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of terms for thoracic imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef]
- Chassagnon, G.; Vakalopoulou, M.; Régent, A.; Sahasrabudhe, M.; Marini, R.; Hoang-Thi, T.N.; Dinh-Xuan, A.T.; Dunogué, B.; Mouthon, L.; Paragios, N.; et al. Elastic registration-driven deep learning for longitudinal assessment of systemic sclerosis interstitial lung disease at CT. Radiology 2021, 298, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Yang, X.; Sun, X.; Meng, X.; Kang, H.; Zhang, R.; Zhang, H.; Liu, M.; Dai, H.; Wang, C. Lung shrinking assessment on HRCT with elastic registration technique for monitoring idiopathic pulmonary fibrosis. Eur. Rad. 2023, 33, 2279–2288. [Google Scholar] [CrossRef] [PubMed]
- Wijsenbeek, M.; Cottin, V. Spectrum of fibrotic lung diseases. N. Engl. J. Med. 2020, 383, 958–968. [Google Scholar] [CrossRef] [PubMed]
- Iwasawa, T.; Ogura, T.; Sakai, F.; Kanauchi, T.; Komagata, T.; Baba, T.; Gotoh, T.; Morita, S.; Yazawa, T.; Inoue, T. CT analysis of the effect of pirfenidone in patients with idiopathic pulmonary fibrosis. Eur. J. Radiol. 2014, 83, 32–38. [Google Scholar] [CrossRef]
- Galvin, J.R.; Frazier, A.A.; Franks, T.J. Collaborative radiologic and histopathologic assessment of fibrotic lung disease. Radiology 2010, 255, 692–706. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 114) | Hazard Ratio (95% CI) | p-Value | |
|---|---|---|---|
| Age (y) a | 69 (64–74) | 1.04 (0.99–1.08) | 0.13 |
| Sex (M/F) | 84 (74)/30 (26) | 0.75 (0.37–1.50) | 0.44 |
| History of smoking | 85 (75) | 0.78 (0.38–1.63) | 0.51 |
| Smoking index (no. of pack-years) a | 20 (0–46) | 1.00 (0.99–1.01) | 0.96 |
| Baseline home oxygen therapy (no. of patients) | 10 (8) | 3.31 (1.44–7.61) | 0.005 |
| Baseline pulmonary function test results | |||
| FVC (% predicted) a | 82 (70–97) | 0.96 (0.94–0.97) | <0.001 |
| DLco (% predicted) a,b | 77 (56–94) | 0.97 (0.96–0.98) | <0.001 |
| Bronchoalveolar lavage (no. of patients) | 62 (54) | ||
| Alveolar macrophages (%) a | 71 (60–83) | 0.99 (0.97–1.01) | 0.37 |
| Alveolar lymphocyte (%) a | 17 (8–26) | 0.98 (0.94–1.01) | 0.18 |
| Lesion Patterns b | Whole Lung | Subpleural Region d | Inner Region | p-Value a |
|---|---|---|---|---|
| Emphysema (%) | 0.59 (0.14–1.67) | 0.44 (0.11–1.12) | 0.09 (0.01–0.35) | <0.001 |
| Consolidation + Fibrosis (%) | 1.59 (1.00–2.72) | 1.14 (0.58–1.75) | 0.19 (0.05–0.52) | <0.001 |
| Ground-glass opacity (%) | 5.38 (3.40–8.32) | 3.61 (2.27–4.73) | 1.55 (0.64–2.66) | <0.001 |
| Reticulation (%) | 0.52 (0.24–1.42) | 2.81 (1.50–5.36) | 0.20 (0.06–0.83) | <0.001 |
| Honeycombing + Traction bronchiectasis (%) | 3.48 (1.84–6.44) | 0.31 (0.09–0.91) | 0.18 (0.08–0.44) | <0.001 |
| Normal (%) | 58.1 (40.1–72.4) | 24.7 (16.7–31.8) | 32.4 (23.6–41.2) | <0.001 |
| Fibrotic lesion (%) c | 5.84 (3.06–10.8) | 4.98 (2.73–9.13) | 0.70 (0.22–2.02) | <0.001 |
| Whole Lung | Subpleural Region c | Inner Region | ||||
|---|---|---|---|---|---|---|
| Lesion Patterns a | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value |
| Emphysema (%) | 1.05 (0.96–1.14) | 0.32 | 1.09 (0.93–1.29) | 0.30 | 1.08 (0.90–1.30) | 0.39 |
| Consolidation + Fibrosis (%) | 1.6 (1.40–1.83) | <0.001 | 2.22 (1.75–2.82) | <0.001 | 2.30 (1.65–3.22) | <0.001 |
| Ground-glass opacity (%) | 1.12 (1.06–1.18) | <0.001 | 1.17 (1.04–1.32) | 0.008 | 1.23 (1.12–1.34) | <0.001 |
| Reticulation (%) | 1.17 (1.07–1.27) | 0.001 | 1.22 (1.12–1.32) | <0.001 | 1.55 (1.26–1.90) | <0.001 |
| Honeycombing + Traction bronchiectasis (%) | 1.16 (1.09–1.23) | <0.001 | 1.24 (1.08–1.42) | 0.002 | 1.63 (1.28–2.08) | <0.001 |
| Normal (%) | 0.67 (0.35–1.27) | 0.218 | 0.89 (0.86–0.93) | <0.001 | 0.92 (0.90–0.95) | <0.001 |
| Fibrotic lesion (%) b | 1.10 (1.06–1.14) | <0.001 | 1.17 (1.10–1.23) | <0.001 | 1.26 (1.14–1.38) | <0.001 |
| Whole Lung | Subpleural Region c | Inner Region | p-Value a | |
|---|---|---|---|---|
| Categorical change in CT lesion variables b | ||||
| ΔEmphysema (%) | 0.22 (0.03–0.90) | 0.10 (0.01–0.34) | 0.05 (−0.00–0.47) | 0.40 |
| ΔConsolidation + Fibrosis (%) | 0.25 (0.56–0.71) | 0.15 (0.02–0.38) | 0.06 (0.00–0.31) | 0.01 |
| ΔGround-glass opacity (%) | 0.12 (−1.37–1.43) | −0.06 (−0.75–0.58) | 0.10 (−0.54–0.87) | 0.001 |
| ΔReticulation (%) | 0.52 (−0.07–1.35) | 0.36 (−0.05–0.87) | 0.04 (−0.04–0.45) | 0.003 |
| ΔHoneycombing + Traction bronchiectasis (%) | 0.16 (0.01–0.81) | 0.08 (0.01–0.34) | 0.047 (−0.01–0.26) | <0.001 |
| ΔNormal (%) | 0.00 (−0.01–0.03) | −1.82 (−4.01–−0.06) | −2.54 (−8.47–0.97) | 0.02 |
| ΔFibrotic lesion (%) | 1.08 (0.15–2.69) | 0.70 (0.22–1.60) | 0.21 (0.00–1.12) | <0.001 |
| ΔTotal CT lung volume (cc) | −183 (−469–131) | |||
| 3D-AD (mm) | 5.0 (3.3–6.7) | 5.2 (3.6–7.1) | 4.7 (3.0–6.4) | <0.001 |
| Whole Lung | Subpleural Region b | Inner Region | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Categorical change in CT lesion variables a | ||||||
| ΔEmphysema (%) | 1.12 (0.97–1.30) | 0.134 | 1.78 (1.30–2.45) | <0.001 | 1.02 (0.82–1.26) | 0.86 |
| ΔConsolidation + Fibrosis (%) | 1.41 (0.94–2.11) | 0.093 | 2.33 (1.42–3.81) | 0.001 | 0.80 (0.44–1.43) | 0.45 |
| ΔGround-glass opacity (%) | 0.93 (0.87–1.00) | 0.05 | 0.94 (0.76–1.16) | 0.054 | 0.89 (0.80–0.99) | 0.03 |
| ΔReticulation (%) | 1.20 (1.01–1.42) | 0.035 | 1.64 (1.26–2.13) | <0.001 | 0.95 (0.69–1.30) | 0.73 |
| ΔHoneycombing + Traction bronchiectasis (%) | 1.65 (1.28–2.13) | <0.001 | 2.00 (1.55–2.58) | <0.001 | 0.93 (0.61–1.40) | 0.73 |
| ΔNormal (%) | 1.02 (0.78–1.34) | 0.889 | 0.76 (0.69–0.83) | <0.001 | 1.01 (0.72–1.43) | 0.96 |
| ΔFibrotic lesion (%) | 1.18 (1.07–1.30) | 0.001 | 1.85 (1.55–2.22) | <0.001 | 0.96 (0.83–1.10) | 0.18 |
| 3D-AD (mm) | 1.20 (1.20–1.30) | <0.001 | 1.20 (1.10–1.30) | <0.001 | 1.20 (1.10–1.30) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yasuda, N.; Iwasawa, T.; Baba, T.; Misumi, T.; Cheng, S.; Kato, S.; Utsunomiya, D.; Ogura, T. Evaluation of Progressive Architectural Distortion in Idiopathic Pulmonary Fibrosis Using Deformable Registration of Sequential CT Images. Diagnostics 2024, 14, 1650. https://doi.org/10.3390/diagnostics14151650
Yasuda N, Iwasawa T, Baba T, Misumi T, Cheng S, Kato S, Utsunomiya D, Ogura T. Evaluation of Progressive Architectural Distortion in Idiopathic Pulmonary Fibrosis Using Deformable Registration of Sequential CT Images. Diagnostics. 2024; 14(15):1650. https://doi.org/10.3390/diagnostics14151650
Chicago/Turabian StyleYasuda, Naofumi, Tae Iwasawa, Tomohisa Baba, Toshihiro Misumi, Shihyao Cheng, Shingo Kato, Daisuke Utsunomiya, and Takashi Ogura. 2024. "Evaluation of Progressive Architectural Distortion in Idiopathic Pulmonary Fibrosis Using Deformable Registration of Sequential CT Images" Diagnostics 14, no. 15: 1650. https://doi.org/10.3390/diagnostics14151650