
Association of Sleep Patterns and Respiratory Disturbance Index with Physiological Parameters in Pediatric Patients with Self-Perceived Short Stature

Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Sleep Apnea and Sleep Quality Examination
2.3. Study Variables
2.4. Statistical Methods
3. Results
3.1. Characteristics of Study Participations
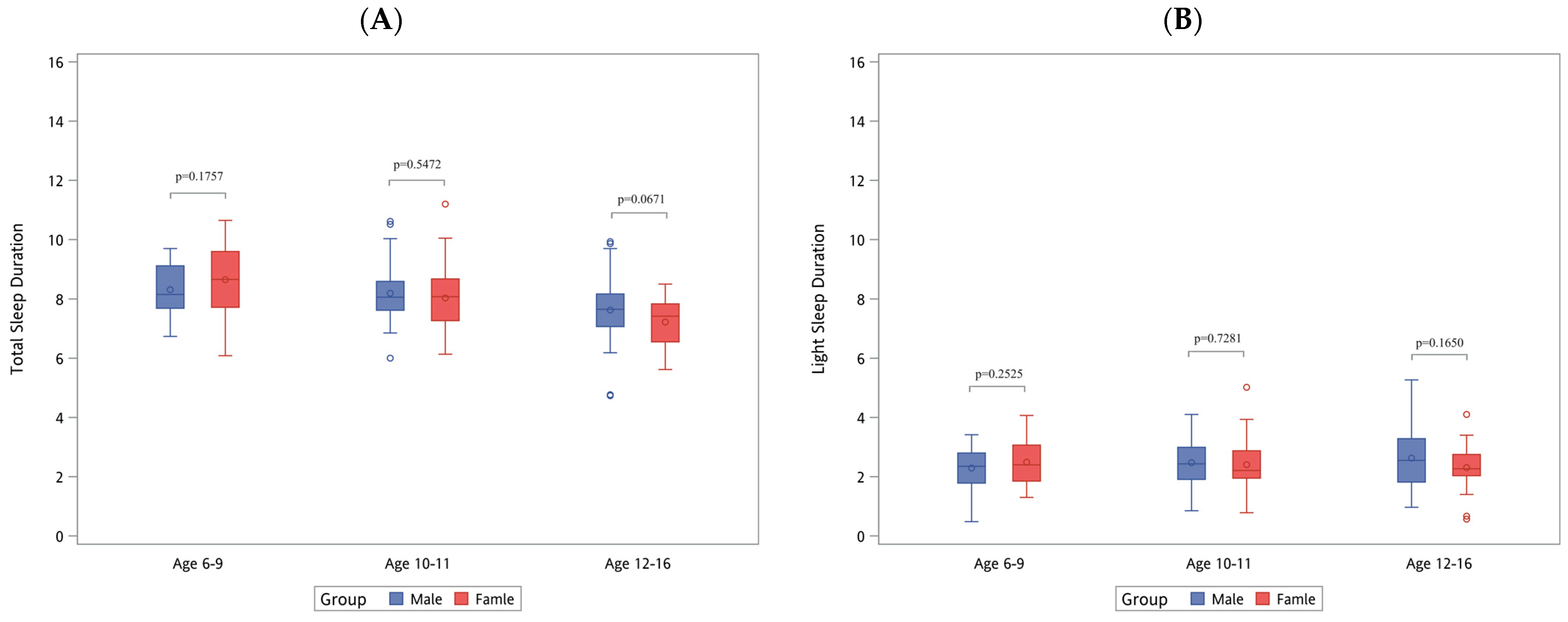
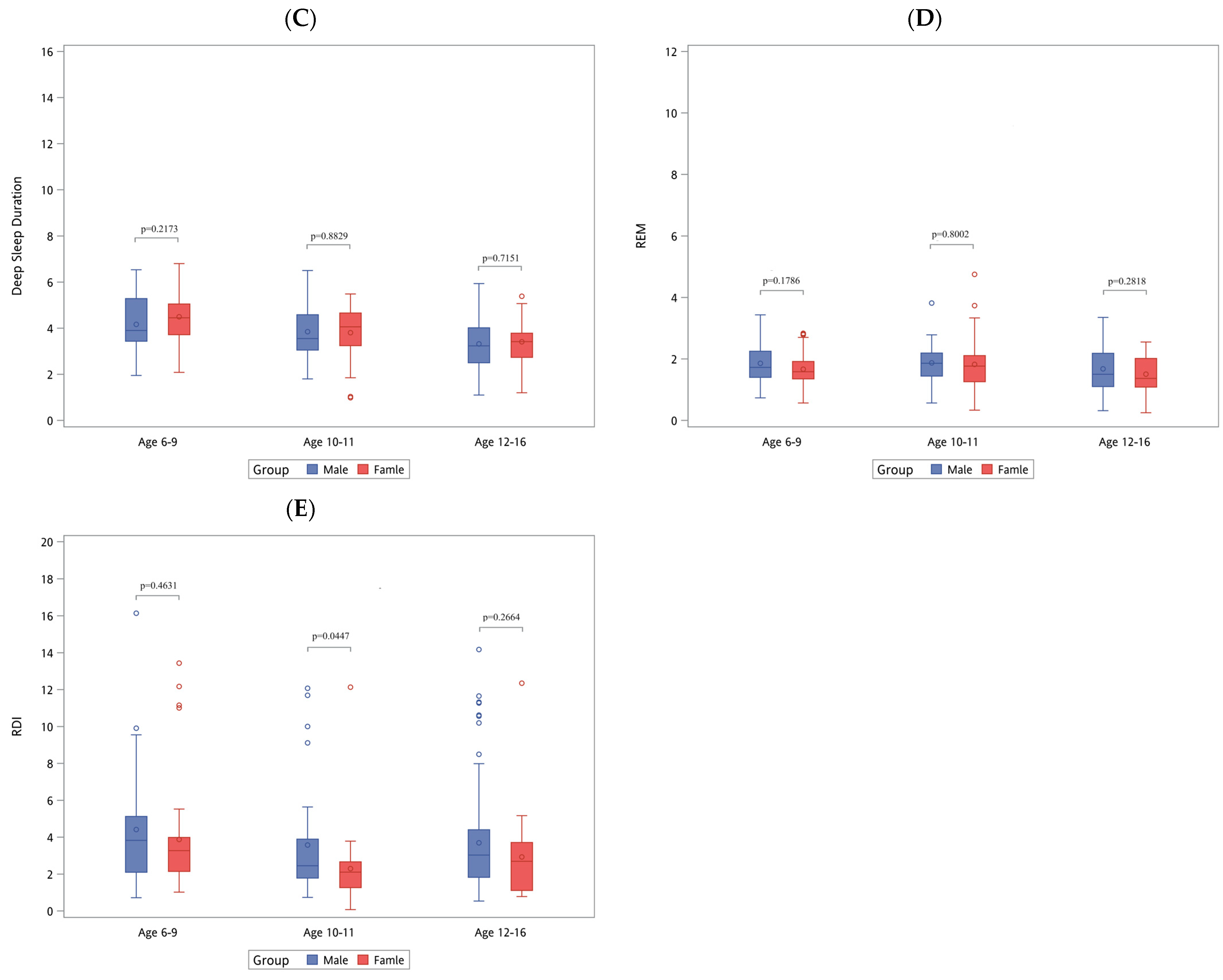
3.2. Differences in States of Sleep among Children
3.3. Subgroup Analysis
3.4. The Association of Sleep Patterns and Sleep Apnea with Body Height and BMI in Children
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine Committee on Sleep M, Research. The National Academies Collection: Reports funded by National Institutes of Health. In Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem; Colten, H.R., Altevogt, B.M., Eds.; National Academy of Sciences: Washington, DC, USA, 2006. [Google Scholar]
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. AASM Scoring Manual Updates for 2017 (Version 2.4). J. Clin. Sleep Med. 2017, 13, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Carskadon, M.A.; Dement, W.C. Normal human sleep: An overview. Princ. Pract. Sleep Med. 2005, 4, 13–23. [Google Scholar]
- Stanley, N. The physiology of sleep and the impact of ageing. Eur. Urol. Suppl. 2005, 3, 17–23. [Google Scholar] [CrossRef]
- Werner, H.; Molinari, L.; Guyer, C.; Jenni, O.G. Agreement rates between actigraphy, diary, and questionnaire for children’s sleep patterns. Arch. Pediatr. Adolesc. Med. 2008, 162, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Rundo, J.V.; Downey, R., 3rd. Polysomnography. Handb. Clin. Neurol. 2019, 160, 381–392. [Google Scholar] [PubMed]
- Molnár, V.; Molnár, A.; Lakner, Z.; Tárnoki, D.L.; Tárnoki, Á.D.; Jokkel, Z.; Szabó, H.; Dienes, A.; Angyal, E.; Németh, F.; et al. Examination of the diaphragm in obstructive sleep apnea using ultrasound imaging. Sleep Breath 2022, 26, 1333–1339. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.M.; Strecker, R.E.; Bianchi, M.T. Recent developments in home sleep-monitoring devices. Int. Sch. Res. Not. 2012, 2012, 768794. [Google Scholar] [CrossRef] [PubMed]
- Park, K.S.; Choi, S.H. Smart technologies toward sleep monitoring at home. Biomed. Eng. Lett. 2019, 9, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Joosten, K.F.; Larramona, H.; Miano, S.; Van Waardenburg, D.; Kaditis, A.G.; Vandenbussche, N.; Ersu, R. How do we recognize the child with OSAS? Pediatr. Pulmonol. 2017, 52, 260–271. [Google Scholar] [CrossRef]
- Paruthi, S.; Brooks, L.J.; D’Ambrosio, C.; Hall, W.A.; Kotagal, S.; Lloyd, R.M.; Malow, B.A.; Maski, K.; Nichols, C.; Quan, S.F.; et al. Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2016, 12, 785–786. [Google Scholar] [CrossRef]
- Gregory, A.M.; Sadeh, A. Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Med. Rev. 2012, 16, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Vriend, J.L.; Davidson, F.D.; Corkum, P.V.; Rusak, B.; Chambers, C.T.; McLaughlin, E.N. Manipulating Sleep Duration Alters Emotional Functioning and Cognitive Performance in Children. J. Pediatr. Psychol. 2013, 38, 1058–1069. [Google Scholar] [CrossRef]
- Shochat, T.; Cohen-Zion, M.; Tzischinsky, O. Functional consequences of inadequate sleep in adolescents: A systematic review. Sleep Med. Rev. 2014, 18, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Koren, D.; Dumin, M.; Gozal, D. Role of sleep quality in the metabolic syndrome. Diabetes Metab. Syndr. Obes. 2016, 9, 281–310. [Google Scholar] [PubMed]
- Kearns, J.C.; Coppersmith, D.D.L.; Santee, A.C.; Insel, C.; Pigeon, W.R.; Glenn, C.R. Sleep problems and suicide risk in youth: A systematic review, developmental framework, and implications for hospital treatment. Gen. Hosp. Psychiatry 2020, 63, 141–151. [Google Scholar] [CrossRef]
- Hysing, M.; Sivertsen, B.; Stormark, K.M.; O’Connor, R.C. Sleep problems and self-harm in adolescence. Br. J. Psychiatry 2015, 207, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Lajoie, A.C.; Privé, A.; Roy-Hallé, A.; Pagé, D.; Simard, S.; Séries, F. Diagnosis and management of sleep apnea by a clinical nurse: A noninferiority randomized clinical trial. J. Clin. Sleep Med. 2022, 18, 89–97. [Google Scholar] [CrossRef]
- Steiger, A. Sleep and endocrine regulation. Front. Biosci. Landmark 2003, 8, 358–376. [Google Scholar] [CrossRef] [PubMed]
- Van Dongen, H.P.; Vitellaro, K.M.; Dinges, D.F. Individual differences in adult human sleep and wakefulness: Leitmotif for a research agenda. Sleep 2005, 28, 479–498. [Google Scholar] [CrossRef]
- Berberoğlu, M. Precocious puberty and normal variant puberty: Definition, etiology, diagnosis and current management. J. Clin. Res. Pediatr. Endocrinol. 2009, 1, 164–174. [Google Scholar] [CrossRef]
- Dékány, L.; Molnár, V.; Molnár, A.; Bikov, A.; Lázár, Z.; Bárdos-Csenteri, O.; Benedek, P. Analysis of possible risk factors for the severity of paediatric obstructive sleep apnoea syndrome. Eur. Arch. Otorhinolaryngol. 2023, 280, 5607–5614. [Google Scholar] [CrossRef] [PubMed]
- Schoch, S.F.; Huber, R.; Kohler, M.; Kurth, S. Which are the Central Aspects of Infant Sleep? The Dynamics of Sleep Composites across Infancy. Sensors 2020, 20, 7188. [Google Scholar] [CrossRef] [PubMed]
- Galland, B.C.; Taylor, B.J.; Elder, D.E.; Herbison, P. Normal sleep patterns in infants and children: A systematic review of observational studies. Sleep Med. Rev. 2012, 16, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Iglowstein, I.; Jenni, O.G.; Molinari, L.; Largo, R.H. Sleep duration from infancy to adolescence: Reference values and generational trends. Pediatrics 2003, 111, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Jenni, O.G.; Carskadon, M.A. Sleep behavior and sleep regulation from infancy through adolescence: Normative aspects. Sleep Med. Clin. 2007, 2, 321–329. [Google Scholar] [CrossRef]
- Carskadon, M.A. Sleep in adolescents: The perfect storm. Pediatr. Clin. N. Am. 2011, 58, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Crowley, S.J.; Wolfson, A.R.; Tarokh, L.; Carskadon, M.A. An update on adolescent sleep: New evidence informing the perfect storm model. J. Adolesc. 2018, 67, 55–65. [Google Scholar] [CrossRef]
- Hagenauer, M.H.; Perryman, J.I.; Lee, T.M.; Carskadon, M.A. Adolescent changes in the homeostatic and circadian regulation of sleep. Dev. Neurosci. 2009, 31, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Gariepy, G.; Danna, S.; Gobiņa, I.; Rasmussen, M.; Gaspar de Matos, M.; Tynjälä, J.; Janssen, I.; Kalman, M.; Villeruša, A.; Husarova, D.; et al. How Are Adolescents Sleeping? Adolescent Sleep Patterns and Sociodemographic Differences in 24 European and North American Countries. J. Adolesc. Health 2020, 66 (Suppl. 6), S81–S88. [Google Scholar] [CrossRef]
- Mong, J.A.; Cusmano, D.M. Sex differences in sleep: Impact of biological sex and sex steroids. Philos. Trans. R. Soc. B 2016, 371, 20150110. [Google Scholar] [CrossRef]
- Segura-Jiménez, V.; Carbonell-Baeza, A.; Keating, X.D.; Ruiz, J.R.; Castro-Piñero, J. Association of sleep patterns with psychological positive health and health complaints in children and adolescents. Qual. Life Res. 2015, 24, 885–895. [Google Scholar] [CrossRef] [PubMed]
- Sadeh, A.; Dahl, R.E.; Shahar, G.; Rosenblat-Stein, S. Sleep and the transition to adolescence: A longitudinal study. Sleep 2009, 32, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Redline, S.; Kirchner, H.L.; Quan, S.F.; Gottlieb, D.J.; Kapur, V.; Newman, A. The effects of age, sex, ethnicity, and sleep-disordered breathing on sleep architecture. Arch. Intern. Med. 2004, 164, 406–418. [Google Scholar] [CrossRef] [PubMed]
- Goel, N.; Kim, H.; Lao, R.P. Gender differences in polysomnographic sleep in young healthy sleepers. Chronobiol. Int. 2005, 22, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.C.; Yűksel, D.; de Zambotti, M. Sex differences in sleep. In Sleep Disorders in Women: A Guide to Practical Management; Springer: Berlin/Heidelberg, Germany, 2020; pp. 55–64. [Google Scholar]
- Ringli, M.; Huber, R. Developmental aspects of sleep slow waves: Linking sleep, brain maturation and behavior. Prog. Brain Res. 2011, 193, 63–82. [Google Scholar] [PubMed]
- Jessen, E.; Vetter, C.; Roenneberg, T.; Liesenkötter, K.P.; Werner, H.; Jenni, O.G.; Lankes, E.; Blankenstein, O.; Neumann, U.; Köhler, B.; et al. Sleep Timing in Patients with Precocious and Delayed Pubertal Development. Clocks Sleep 2019, 1, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Morssinkhof, M.W.L.; van Wylick, D.W.; Priester-Vink, S.; van der Werf, Y.D.; den Heijer, M.; van den Heuvel, O.A.; Broekman, B.F.P. Associations between sex hormones, sleep problems and depression: A systematic review. Neurosci. Biobehav. Rev. 2020, 118, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Sekerovic, Z.; Carrier, J. Sleep regulation and sex hormones exposure in men and women across adulthood. Pathol. Biol. 2014, 62, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.D.; Wit, J.M.; Hochberg, Z.; Sävendahl, L.; van Rijn, R.R.; Fricke, O.; Cameron, N.; Caliebe, J.; Hertel, T.; Kiepe, D.; et al. The use of bone age in clinical practice—Part 1. Horm. Res. Paediatr. 2011, 76, 1–9. [Google Scholar] [CrossRef]
- Manzoor Mughal, A.; Hassan, N.; Ahmed, A. Bone age assessment methods: A critical review. Pak. J. Med. Sci. 2014, 30, 211–215. [Google Scholar]
- Jennum, P.; Ibsen, R.; Kjellberg, J. Morbidity and mortality in children with obstructive sleep apnoea: A controlled national study. Thorax 2013, 68, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Volkov, S.I.; Ginter, O.V.; Covantev, S.; Corlateanu, A. Adenoid Hypertrophy, Craniofacial Growth and Obstructive Sleep Apnea: A Crucial Triad in Children. Curr. Respir. Med. Rev. 2020, 16, 144–155. [Google Scholar] [CrossRef]
- Niedzielski, A.; Chmielik, L.P.; Mielnik-Niedzielska, G.; Kasprzyk, A.; Bogusławska, J. Adenoid hypertrophy in children: A narrative review of pathogenesis and clinical relevance. BMJ Paediatr. Open 2023, 7, e001710. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.P.S. Relationship between adenoid hypertrophy and sleep apnea in children. Braz. Dent. Sci. 2019, 22, 297–304. [Google Scholar]
- Molnár, V.; Lakner, Z.; Molnár, A.; Tárnoki, D.L.; Tárnoki, Á.D.; Kunos, L.; Jokkel, Z.; Tamás, L. The Predictive Role of the Upper-Airway Adipose Tissue in the Pathogenesis of Obstructive Sleep Apnoea. Life 2022, 12, 1543. [Google Scholar] [CrossRef] [PubMed]
- El Halal, C.d.S.; Nunes, M.L. Sleep and weight-height development. J. Pediatr. 2019, 95, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Gulliford, M.C.; Price, C.E.; Rona, R.J.; Chinn, S. Sleep habits and height at ages 5 to 11. Arch. Dis. Child. 1990, 65, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Jenni, O.G.; Molinari, L.; Caflisch, J.A.; Largo, R.H. Sleep duration from ages 1 to 10 years: Variability and stability in comparison with growth. Pediatrics 2007, 120, e769–e776. [Google Scholar] [CrossRef]
- Gassman-Pines, A.; Ananat, E.O.; Fitz-Henley, J.; Leer, J. Effect of daily school and care disruptions during the COVID-19 pandemic on child behavior problems. Dev. Psychol. 2022, 58, 1512–1527. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD/n(%) |
|---|---|
| Total number of participants (N) | 238 (100.0%) |
| Month of measurement | |
| January–March | 23 (9.7%) |
| April–June | 13 (5.5%) |
| July–September | 83 (34.9%) |
| October–December | 119 (50.0%) |
| Day of week | |
| Friday–Saturday (weekend night) | 204 (85.7%) |
| Sunday–Thursday (weeknight) | 34 (14.3%) |
| Sex | |
| Female | 101 (42.4%) |
| Male | 137 (57.6%) |
| Age (Range: 6–16 years) | |
| 6–9 years old | 72 (30.3%) |
| 10–11 years old | 68 (28.6%) |
| 12–16 years old | 98 (41.2%) |
| Average body height (cm) | 140.55 ± 14.59 |
| Body height Z-score | −0.85 ± 1.02 |
| Average BMI (kg/m2) | 35.84 ± 12.53 |
| BMI Z-score | −0.21 ± 1.26 |
| Bone age to chronological age ratio (BA/CA) | 1.00 ± 0.15 |
| Average IGF-1 (ng/mL) | 234.91 ± 108.72 |
| IGF-1 Z-score | 0.00 ± 0.96 |
| Enlarged adenoid tonsil in posterior nasopharynx | |
| Absent | 151 (63.5%) |
| Present | 87 (36.6%) |
| Total sleep duration (hours) | 7.99 ± 1.08 |
| Light sleep duration (hours) | 2.48 ± 0.85 |
| Deep sleep duration (hours) | 3.79 ± 1.18 |
| REM sleep duration (hours) | 1.73 ± 0.68 |
| Respiratory disturbance index (Range: 0.07–16.14) | 3.51 ± 2.87 |
| RDI < 1 | 19 (8.0%) |
| 1 ≤ RDI < 5 | 184 (77.3%) |
| RDI ≥ 5 | 35 (14.7%) |
| Sleep latency | |
| <30 min | 139 (58.4%) |
| ≥30 min | 99 (41.6%) |
| Growth hormone therapy | |
| No | 170 (71.2%) |
| Yes | 68 (28.6%) |
| N | Total Sleep (Hours) | Light Sleep (Hours) | Deep Sleep (Hours) | REM (Hours) | RDI | |
|---|---|---|---|---|---|---|
| Entire sample | 238 | 7.99 ± 1.08 | 2.48 ± 0.85 | 3.79 ± 1.18 | 1.73 ± 0.68 | 3.51 ± 2.87 |
| Month of measurement | ||||||
| APR–SEP (summer) | 96 | 8.10 ± 1.10 | 2.41 ± 0.73 | 3.82 ± 1.18 | 1.87 ± 0.72 | 3.66 ± 3.06 |
| OCT–DEC, JAN–MAR (winter) | 142 | 7.92 ± 1.07 | 2.52 ± 0.92 | 3.76 ± 1.18 | 1.64 ± 0.64 | 3.41 ± 2.74 |
| p-value | 0.2035 | 0.3098 | 0.6882 | 0.0110 * | 0.5095 | |
| Day of week | ||||||
| Friday–Saturday (weekend night) | 204 | 7.94 ± 1.05 | 2.46 ± 0.86 | 3.77 ± 1.18 | 1.71 ± 0.68 | 3.48 ± 2.84 |
| Sunday–Thursday (weeknight) | 34 | 8.28 ± 1.25 | 2.57 ± 0.80 | 3.86 ± 1.21 | 1.86 ± 0.71 | 3.73 ± 3.06 |
| p-value | 0.0947 | 0.5047 | 0.7053 | 0.2440 | 0.6396 | |
| Age | ||||||
| 6–9 years old | 72 | 8.51 ± 1.04 | 2.41 ± 0.72 | 4.36 ± 1.11 | 1.75 ± 0.59 | 4.10 ± 3.04 |
| 10–11 years old | 68 | 8.11 ± 1.07 | 2.44 ± 0.78 | 3.82 ± 1.19 | 1.85 ± 0.78 | 2.90 ± 2.56 |
| 12–16 years old | 98 | 7.53 ± 0.93 | 2.55 ± 0.97 | 3.34 ± 1.03 | 1.64 ± 0.67 | 3.51 ± 2.88 |
| p-value | <0.0001 * | 0.4937 | <0.0001 * | 0.1484 | 0.0457 | |
| Sex | ||||||
| Female | 101 | 8.10 ± 1.20 | 2.42 ± 0.79 | 4.00 ± 1.15 | 1.68 ± 0.69 | 3.10 ± 2.56 |
| Male | 137 | 7.91 ± 0.99 | 2.52 ± 0.89 | 3.63 ± 1.18 | 1.76 ± 0.68 | 3.83 ± 3.06 |
| p-value | 0.1781 | 0.3694 | 0.0153 * | 0.3952 | 0.0530 | |
| Height Z-score | ||||||
| ≤−1 | 116 | 7.99 ± 1.09 | 2.44 ± 0.83 | 3.89 ± 1.26 | 1.67 ± 0.67 | 4.13 ± 3.30 |
| 0 | 110 | 8.04 ± 1.10 | 2.52 ± 0.86 | 3.71 ± 1.11 | 1.81 ± 0.71 | 2.88 ± 2.12 |
| ≥1 | 12 | 7.48 ± 0.78 | 2.41 ± 0.97 | 3.48 ± 0.97 | 1.58 ± 0.39 | 3.46 ± 3.34 |
| p-value | 0.2286 | 0.7574 | 0.3629 | 0.2229 | 0.0041 * | |
| BMI Z-score | ||||||
| ≤−1 | 54 | 7.94 ± 0.84 | 2.30 ± 0.78 | 3.92 ± 1.08 | 1.72 ± 0.63 | 3.71 ± 2.89 |
| 0 | 147 | 8.09 ± 1.17 | 2.55 ± 0.91 | 3.79 ± 1.26 | 1.74 ± 0.68 | 3.54 ± 2.86 |
| ≥1 | 37 | 7.67 ± 1.01 | 2.43 ± 0.65 | 3.56 ± 0.93 | 1.69 ± 0.78 | 3.13 ± 2.93 |
| p-value | 0.1075 | 0.1651 | 0.3470 | 0.8919 | 0.6290 | |
| BA/CA ratios | ||||||
| ≤1.2 | 212 | 7.93 ± 1.04 | 2.47 ± 0.87 | 3.73 ± 1.18 | 1.73 ± 0.69 | 3.60 ± 2.93 |
| >1.2 | 26 | 8.51 ± 1.28 | 2.49 ± 0.69 | 4.26 ± 1.11 | 1.76 ± 0.62 | 2.86 ± 2.27 |
| p-value | 0.0099 * | 0.9127 | 0.0312 * | 0.8197 | 0.2152 | |
| IGF-1 | ||||||
| <0 | 126 | 8.08 ± 1.09 | 2.49 ± 0.88 | 3.82 ± 1.20 | 1.77 ± 0.74 | 3.74 ± 3.06 |
| ≥0 | 112 | 7.89 ± 1.07 | 2.46 ± 0.82 | 3.75 ± 1.16 | 1.68 ± 0.61 | 3.26 ± 2.62 |
| p-value | 0.1900 | 0.8332 | 0.6381 | 0.3103 | 0.1941 | |
| Enlarged adenoid tonsil in posterior nasopharynx | ||||||
| Absent | 151 | 7.98 (±1.04) | 2.49 (±0.75) | 3.72 (±1.14) | 1.77 (±0.63) | 3.67 (±3.06) |
| Present | 87 | 8.01 (±1.16) | 2.45 (±0.99) | 3.90 (±1.24) | 1.66 (±0.76) | 3.25 (±2.50) |
| p-value | 0.8245 | 0.7812 | 0.2691 | 0.2606 | 0.2546 | |
| Growth hormone therapy | ||||||
| No | 170 | 8.01 ± 1.02 | 2.46 ± 0.78 | 3.83 ± 1.13 | 1.73 ± 0.64 | 3.73 ± 3.17 |
| Yes | 68 | 7.93 ± 1.24 | 2.52 ± 1.01 | 3.68 ± 1.30 | 1.74 ± 0.79 | 2.98 ± 1.82 |
| p-value | 0.6317 | 0.6544 | 0.3718 | 0.9353 | 0.0226 * | |
| RDI | ||||||
| RDI < 1 | 19 | 7.24 ± 0.70 | 1.56 ± 0.72 | 4.31 ± 1.31 | 1.36 ± 0.67 | 0.71 ± 0.20 |
| 1 ≤ RDI < 5 | 184 | 8.05 ± 1.09 | 2.44 ± 0.76 | 3.87 ± 1.12 | 1.74 ± 0.67 | 2.71 ± 1.07 |
| 5 ≤ RDI | 35 | 8.09 ± 1.09 | 3.16 ± 0.82 | 3.07 ± 1.14 | 1.85 ± 0.71 | 9.27 ± 3.04 |
| p-value | <0.0001 * | 0.4937 | <0.0001 * | 0.1484 | <0.0001 * |
| Dependent Variable: Body Height | ||||
|---|---|---|---|---|
| Model 1 | Model 2 | |||
| Parameter | Beta coefficients (95% CI) | t value/p-value | Beta coefficients (95% CI) | t value/p-value |
| Sex (male) | −0.35 (−2.27, 1.57) | −0.36/0.7186 | −0.83 (−2.75, 1.08) | −0.86/0.3927 |
| Age (year) | 5.19 (4.80, 5.57) * | 26.44/<0.0001 | 4.89 (4.45, 5.33) * | 21.74/<0.0001 |
| Light sleep duration (hour) | 0.01 (−0.01, 0.03) | 0.84/0.4009 | ||
| Deep sleep duration (hour) | −0.02 (−0.03, 0.00) | −1.82/0.0708 | ||
| REM (hour) | −0.01 (−0.04, 0.01) | −1.00/0.3165 | ||
| RDI | −0.54 (−0.88, −0.20) * | −3.10/0.0022 | ||
| Model Fit | ||||
| R2 | 0.769 | 0.780 | ||
| Dependent Variable: BMI | ||||
|---|---|---|---|---|
| Model 3 | Model 4 | |||
| Parameter | Beta coefficients (95% CI) | t value/p-value | Beta coefficients (95% CI) | t value/p-value |
| Sex (male) | −1.70 (−3.98, 0.58) | −1.47/0.1437 | −2.16 (−4.45, 0.14) | −1.85/0.0661 |
| Age (year) | 3.68 (3.22, 4.14) * | 15.80/<0.0001 | 3.33 (2.80, 3.86) * | 12.34/<0.0001 |
| Light sleep duration (hour) | −0.00 (−0.03, 0.03) | −0.05/0.9629 | ||
| Deep sleep duration (hour) | −0.02 (−0.04, −0.00) * | −2.10/0.0371 | ||
| REM (hour) | −0.03 (−0.06, 0.00) | −1.89/0.0605 | ||
| RDI | −0.40 (−0.81, 0.01) | −1.91/0.0570 | ||
| Model Fit | ||||
| R2 | 0.556 | 0.570 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.-Y.; Liao, P.-L.; Chang, H.-P.; Su, P.-H. Association of Sleep Patterns and Respiratory Disturbance Index with Physiological Parameters in Pediatric Patients with Self-Perceived Short Stature. Diagnostics 2024, 14, 1675. https://doi.org/10.3390/diagnostics14151675
Huang J-Y, Liao P-L, Chang H-P, Su P-H. Association of Sleep Patterns and Respiratory Disturbance Index with Physiological Parameters in Pediatric Patients with Self-Perceived Short Stature. Diagnostics. 2024; 14(15):1675. https://doi.org/10.3390/diagnostics14151675
Chicago/Turabian StyleHuang, Jing-Yang, Pei-Lun Liao, Hua-Pin Chang, and Pen-Hua Su. 2024. "Association of Sleep Patterns and Respiratory Disturbance Index with Physiological Parameters in Pediatric Patients with Self-Perceived Short Stature" Diagnostics 14, no. 15: 1675. https://doi.org/10.3390/diagnostics14151675
APA StyleHuang, J.-Y., Liao, P.-L., Chang, H.-P., & Su, P.-H. (2024). Association of Sleep Patterns and Respiratory Disturbance Index with Physiological Parameters in Pediatric Patients with Self-Perceived Short Stature. Diagnostics, 14(15), 1675. https://doi.org/10.3390/diagnostics14151675