
Parathyroid Adenoma Detected in 68Ga-PSMA PET/CT but Not in the Dedicated Imaging Modalities
 , , , , and
, , , , and {kind=link}
{kind=link}
Abstract
1. Introduction
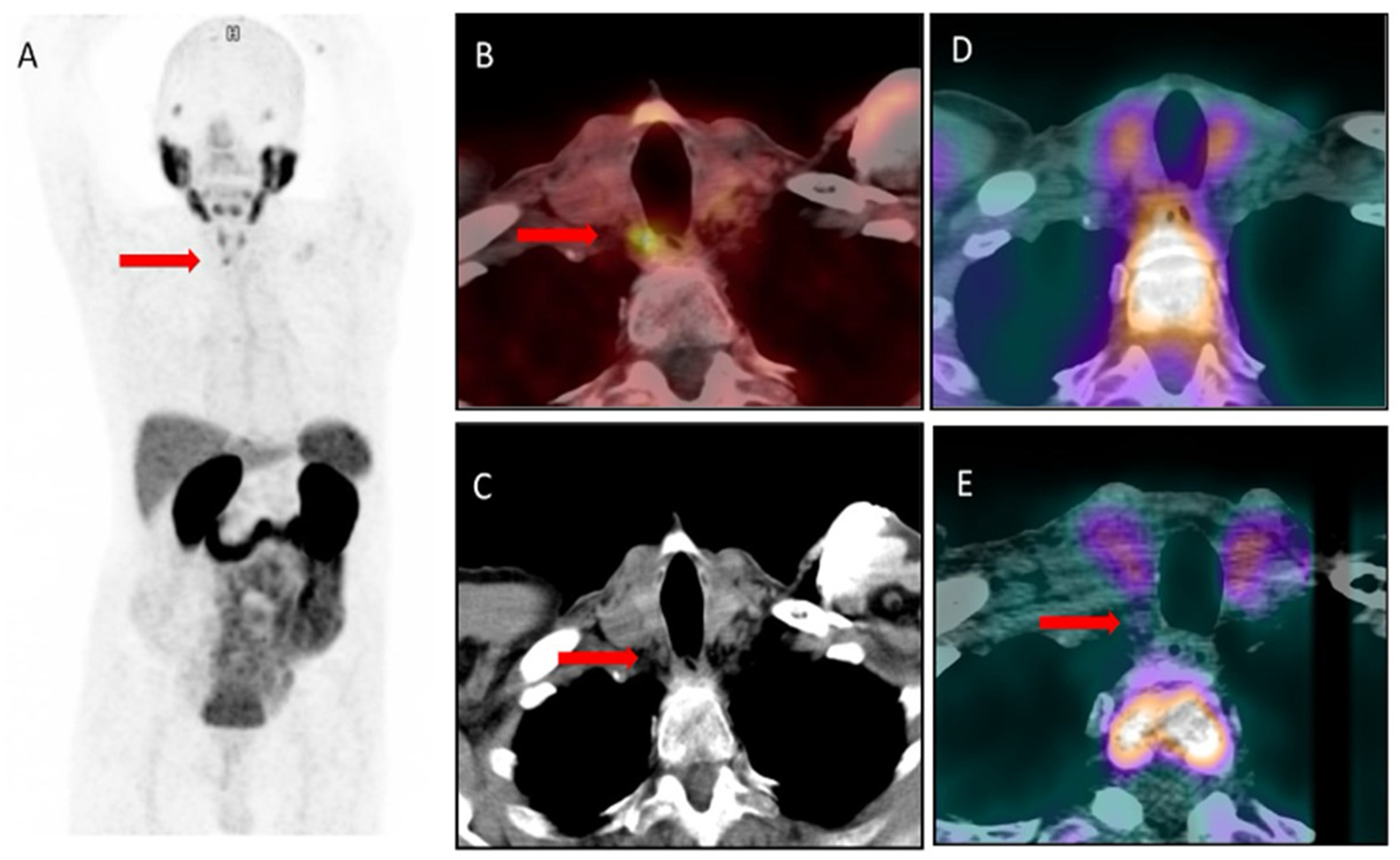
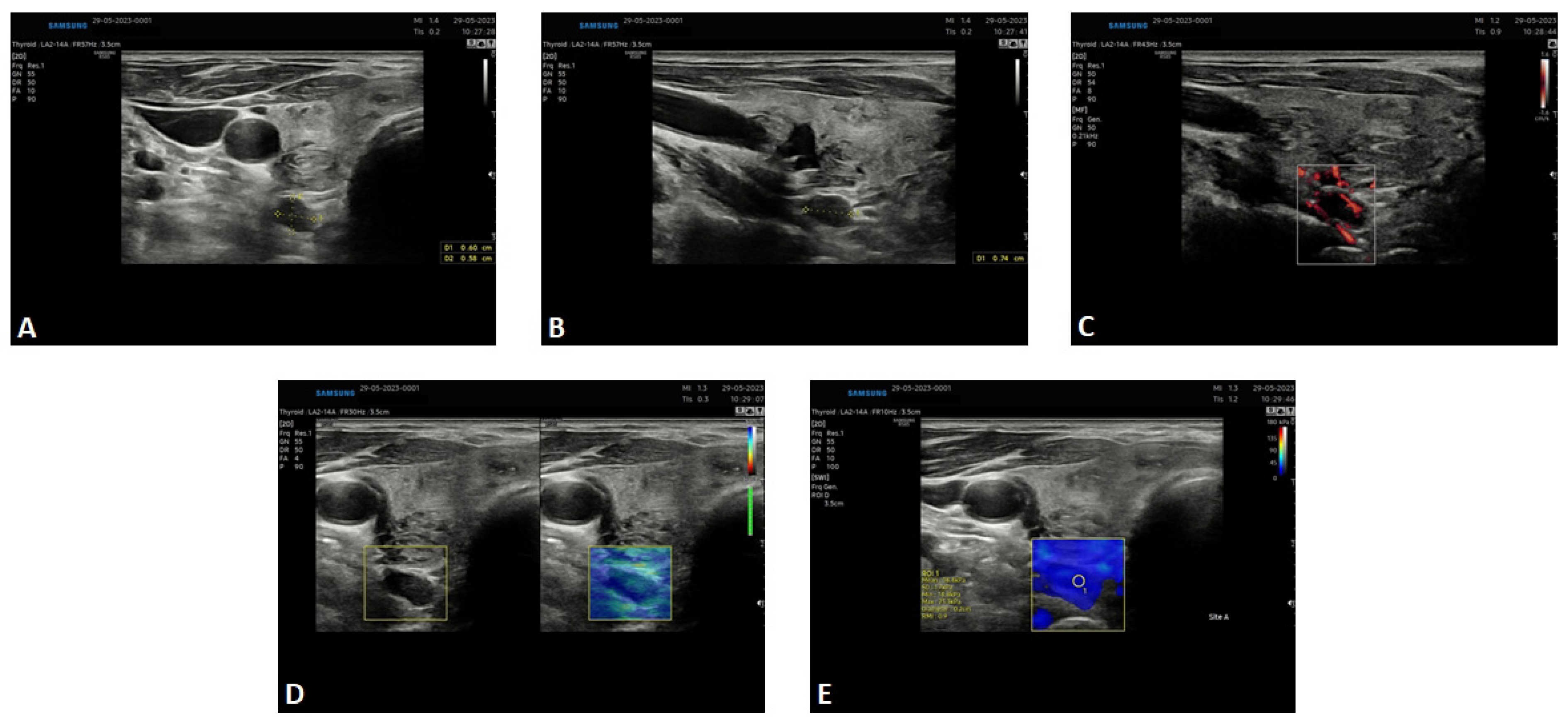
2. Results—Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walker, M.D.; Silverberg, S.J. Primary hyperparathyroidism. Nat. Rev. Endocrinol. 2017, 14, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Bromińska, B.; Milewska, E.; Szczepanek-Parulska, E.; Czepczyński, R.; Ruchała, M. Diagnostic workup of a patient with severe hypercalcemia and a history of malignancy. Pol. Arch. Intern. Med. 2021, 131, 727–729. [Google Scholar] [CrossRef] [PubMed]
- Petranović Ovčariček, P.; Giovanella, L.; Carrió Gasset, I.; Hindié, E.; Huellner, M.W.; Luster, M.; Piccardo, A.; Weber, T.; Talbot, J.N.; Verburg, F.A. The EANM practice guidelines for parathyroid imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2801–2822. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mazurek, A.; Dziuk, M.; Witkowska-Patena, E.; Chudzinski, W.; Piszczek, S.; Gizewska, A.; Saracyn, M. The utility of 18F-fluorocholine PET/CT in the imaging of parathyroid adenomas. Endokrynol. Pol. 2022, 73, 43–48. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, D.S.; Su, S.L.; Bacich, D.J.; Horiguchi, Y.; Luo, Y.; Powell, C.T.; Zandvliet, D.; Russell, P.J.; Molloy, P.L.; Nowak, N.J.; et al. Mapping, genomic organization and promoter analysis of the human prostate-specific membrane antigen gene. Biochim. Biophys. Acta 1998, 1443, 113–127. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, D.S.; Bacich, D.J.; Huang, S.S.; Heston, W.D.W. A Perspective on the Evolving Story of PSMA Biology, PSMA-Based Imaging, and Endoradiotherapeutic Strategies. J. Nucl. Med. 2018, 59, 1007–1013. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ceci, F.; Oprea-Lager, D.E.; Emmett, L.; Adam, J.A.; Bomanji, J.; Czernin, J.; Eiber, M.; Haberkorn, U.; Hofman, M.S.; Hope, T.A.; et al. E-PSMA: The EANM standardized reporting guidelines v1.0 for PSMA-PET. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1626–1638. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chang, S.S.; Reuter, V.E.; Heston, W.D.; Bander, N.H.; Grauer, L.S.; Gaudin, P.B. Five different anti-prostate-specific membrane antigen (PSMA) antibodies confirm PSMA expression in tumor-associated neovasculature. Cancer Res. 1999, 59, 3192–3198. [Google Scholar] [PubMed]
- Grant, C.L.; Caromile, L.A.; Ho, V.; Durrani, K.; Rahman, M.M.; Claffey, K.P.; Fong, G.H.; Shapiro, L.H. Prostate specific membrane antigen (PSMA) regulates angiogenesis independently of VEGF during ocular neovascularization. PLoS ONE 2012, 7, e41285, Erratum in PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Galiza Barbosa, F.; Queiroz, M.A.; Nunes, R.F.; Costa, L.B.; Zaniboni, E.C.; Marin, J.F.G.; Cerri, G.G.; Buchpiguel, C.A. Nonprostatic diseases on PSMA PET imaging: A spectrum of benign and malignant findings. Cancer Imaging 2020, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Kunikowska, J.; Czepczyński, R.; Pawlak, D.; Koziara, H.; Pełka, K.; Królicki, L. Expression of glutamate carboxypeptidase II in the glial tumor recurrence evaluated in vivo using radionuclide imaging. Sci. Rep. 2022, 12, 652. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.E.; Rojas, C.; Alt, J.; Nováková, Z.; Richardson, S.M.; Rodrick, T.C.; Fuentes, J.L.; Richardson, N.H.; Attalla, J.; Stewart, S.; et al. Prostate-specific membrane antigen (PSMA)-mediated laminin proteolysis generates a pro-angiogenic peptide. Angiogenesis 2016, 19, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Dassie, J.P.; Liu, X.Y.; Thomas, G.S.; Whitaker, R.M.; Thiel, K.W.; Stockdale, K.R.; Meyerholz, D.K.; McCaffrey, A.P.; McNamara, J.O., II; Giangrande, P.H. Systemic administration of optimized aptamer-siRNA chimeras promotes regression of PSMA-expressing tumors. Nat. Biotechnol. 2009, 27, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Andryszak, N.; Świniuch, D.; Wójcik, E.; Ramlau, R.; Ruchała, M.; Czepczyński, R. Head-to-Head Comparison of [18F]PSMA-1007 and [18F]FDG PET/CT in Patients with Triple-Negative Breast Cancer. Cancers 2024, 16, 667. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Broos, W.A.; van der Zant, F.M.; Knol, R.J. Incidental Detection of Parathyroid Adenoma on 18F-PSMA PET/CT. Clin. Nucl. Med. 2023, 48, 1082–1083. [Google Scholar] [CrossRef] [PubMed]
- Piek, M.W.; de Vries, L.H.; Donswijk, M.L.; de Keizer, B.; de Boer, J.P.; Lodewijk, L.; van Leeuwaarde, R.S.; Vriens, M.R.; Hartemink, K.J.; van der Ploeg, I.M.C. Retrospective analysis of PSMA PET/CT thyroid incidental uptake in adults: Incidence, diagnosis, and treatment/outcome in a tertiary cancer referral center and University Medical Center. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2392–2400. [Google Scholar] [CrossRef] [PubMed]
- Pfob, C.H.; Karimov, I.; Jesinghaus, M.; Novotny, A.; Weber, W.A.; Eiber, M.; Feuerecker, B. Pitfalls in Ga-68-PSMA-PET/CT: Incidental finding of parathyroid adenoma. Eur. J. Nucl. Med. Mol. Imaging 2018, 46, 1041. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, Y.; Kuratsukuri, K.; Landas, S.; Imaida, K.; Rovito, P.M.; Wang, C.Y.; Haas, G.P. Expression of prostate-specific membrane antigen in normal and malignant human tissues. World J. Surg. 2006, 30, 628–636. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cieślewicz, M.; Andryszak, N.; Pełka, K.; Szczepanek-Parulska, E.; Ruchała, M.; Kunikowska, J.; Czepczyński, R. Parathyroid Adenoma Detected in 68Ga-PSMA PET/CT but Not in the Dedicated Imaging Modalities. Diagnostics 2024, 14, 1690. https://doi.org/10.3390/diagnostics14151690
Cieślewicz M, Andryszak N, Pełka K, Szczepanek-Parulska E, Ruchała M, Kunikowska J, Czepczyński R. Parathyroid Adenoma Detected in 68Ga-PSMA PET/CT but Not in the Dedicated Imaging Modalities. Diagnostics. 2024; 14(15):1690. https://doi.org/10.3390/diagnostics14151690
Chicago/Turabian StyleCieślewicz, Maja, Natalia Andryszak, Kacper Pełka, Ewelina Szczepanek-Parulska, Marek Ruchała, Jolanta Kunikowska, and Rafał Czepczyński. 2024. "Parathyroid Adenoma Detected in 68Ga-PSMA PET/CT but Not in the Dedicated Imaging Modalities" Diagnostics 14, no. 15: 1690. https://doi.org/10.3390/diagnostics14151690
APA StyleCieślewicz, M., Andryszak, N., Pełka, K., Szczepanek-Parulska, E., Ruchała, M., Kunikowska, J., & Czepczyński, R. (2024). Parathyroid Adenoma Detected in 68Ga-PSMA PET/CT but Not in the Dedicated Imaging Modalities. Diagnostics, 14(15), 1690. https://doi.org/10.3390/diagnostics14151690