
Reliability of Kaiser Score in Assessing Additional Breast Lesions Identified on Staging MRI in Patients with Breast Cancer
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. MRI Protocol
2.3. Data Collection
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 26 June 2024).
- Chen, H.; Zhou, J.; Chen, Q.; Deng, Y. Comparison of the Sensitivity of Mammography, Ultrasound, Magnetic Resonance Imaging and Combinations of These Imaging Modalities for the Detection of Small (≤2 Cm) Breast Cancer. Medicine 2021, 100, e26531. [Google Scholar] [CrossRef] [PubMed]
- Iacconi, C.; Galman, L.; Zheng, J.; Sacchini, V.; Sutton, E.J.; Dershaw, D.; Morris, E.A. Multicentric Cancer Detected at Breast MR Imaging and Not at Mammography: Important or Not? Radiology 2016, 279, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Nassar, L.; Nakad, S.; Abou Zeid, F.; Farah, Z.; Saheb, G.; Mroueh, N.; Debs, P.; Berjawi, G. Additional Occult Cancers Identified on Staging Breast MRI: Imaging Appearances and Pathologic Characteristics. J. Med. Radiat. Sci. 2023, 70, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.L.; Lotfalla, M.; Cimino-Mathews, A.; Habibi, M.; Ambinder, E.B. Radiologic-Pathologic Correlation of Nonmass Enhancement Contiguous with Malignant Index Breast Cancer Masses at Preoperative Breast MRI. Radiol. Imaging Cancer 2024, 6, e230060. [Google Scholar] [CrossRef] [PubMed]
- Newell, M.S. It’s Complicated: Managing Nonmass Enhancement Found at Breast MRI in Patients with Newly Diagnosed Cancer. Radiol. Imaging Cancer 2024, 6, e240003. [Google Scholar] [CrossRef] [PubMed]
- Mota, B.S.; Reis, Y.N.; de Barros, N.; Cardoso, N.P.; Mota, R.M.S.; Shimizu, C.; de Mello Tucunduva, T.C.; de Siqueira Ferreira, V.C.C.; Goncalves, R.; Doria, M.T.; et al. Effects of Preoperative Magnetic Resonance Image on Survival Rates and Surgical Planning in Breast Cancer Conservative Surgery: Randomized Controlled Trial (BREAST-MRI Trial). Breast Cancer Res. Treat. 2023, 198, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Houssami, N.; Turner, R.M.; Morrow, M. Meta-Analysis of Pre-Operative Magnetic Resonance Imaging (MRI) and Surgical Treatment for Breast Cancer. Breast Cancer Res. Treat. 2017, 165, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Sardanelli, F.; Trimboli, R.M.; Houssami, N.; Gilbert, F.J.; Helbich, T.H.; Álvarez Benito, M.; Balleyguier, C.; Bazzocchi, M.; Bult, P.; Calabrese, M.; et al. Magnetic Resonance Imaging before Breast Cancer Surgery: Results of an Observational Multicenter International Prospective Analysis (MIPA). Eur. Radiol. 2022, 32, 1611–1623. [Google Scholar] [CrossRef] [PubMed]
- (PDF) American College of Radiology Breast Imaging Reporting and Data System Ultrasound: An Overview of the Second Edition. Available online: https://www.researchgate.net/publication/281365755_American_College_of_Radiology_Breast_Imaging_Reporting_and_Data_System_Ultrasound_An_Overview_of_the_Second_Edition (accessed on 26 June 2024).
- Magny, S.J.; Shikhman, R.; Keppke, A.L. Breast Imaging Reporting and Data System. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- BI-RADS® Fifth Edition: A Summary of Changes—University of Texas Southwestern Medical Center. Available online: https://utsouthwestern.elsevierpure.com/en/publications/bi-radssupsup-fifth-edition-a-summary-of-changes (accessed on 26 June 2024).
- Nguyen, D.L.; Myers, K.S.; Oluyemi, E.; Mullen, L.A.; Panigrahi, B.; Rossi, J.; Ambinder, E.B. BI-RADS 3 Assessment on MRI: A Lesion-Based Review for Breast Radiologists. J. Breast Imaging 2022, 4, 460–473. [Google Scholar] [CrossRef]
- Choi, J.S. Breast Imaging Reporting and Data System (BI-RADS): Advantages and Limitations. J. Korean Soc. Radiol. 2023, 84, 3–14. [Google Scholar] [CrossRef]
- Brennan, M.E.; Houssami, N.; Lord, S.; Macaskill, P.; Irwig, L.; Dixon, J.M.; Warren, R.M.L.; Ciatto, S. Magnetic Resonance Imaging Screening of the Contralateral Breast in Women with Newly Diagnosed Breast Cancer: Systematic Review and Meta-Analysis of Incremental Cancer Detection and Impact on Surgical Management. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 5640–5649. [Google Scholar] [CrossRef] [PubMed]
- Baltzer, P.A.T.; Dietzel, M.; Kaiser, W.A. A Simple and Robust Classification Tree for Differentiation between Benign and Malignant Lesions in MR-Mammography. Eur. Radiol. 2013, 23, 2051–2060. [Google Scholar] [CrossRef] [PubMed]
- Marino, M.A.; Clauser, P.; Woitek, R.; Wengert, G.J.; Kapetas, P.; Bernathova, M.; Pinker-Domenig, K.; Helbich, T.H.; Preidler, K.; Baltzer, P.A.T. A Simple Scoring System for Breast MRI Interpretation: Does It Compensate for Reader Experience? Eur. Radiol. 2016, 26, 2529–2537. [Google Scholar] [CrossRef] [PubMed]
- Woitek, R.; Spick, C.; Schernthaner, M.; Rudas, M.; Kapetas, P.; Bernathova, M.; Furtner, J.; Pinker, K.; Helbich, T.H.; Baltzer, P.A.T. A Simple Classification System (the Tree Flowchart) for Breast MRI Can Reduce the Number of Unnecessary Biopsies in MRI-Only Lesions. Eur. Radiol. 2017, 27, 3799–3809. [Google Scholar] [CrossRef] [PubMed]
- Clauser, P.; Mann, R.; Athanasiou, A.; Prosch, H.; Pinker, K.; Dietzel, M.; Helbich, T.H.; Fuchsjäger, M.; Camps-Herrero, J.; Sardanelli, F.; et al. A Survey by the European Society of Breast Imaging on the Utilisation of Breast MRI in Clinical Practice. Eur. Radiol. 2018, 28, 1909–1918. [Google Scholar] [CrossRef] [PubMed]
- Jajodia, A.; Sindhwani, G.; Pasricha, S.; Prosch, H.; Puri, S.; Dewan, A.; Batra, U.; Doval, D.C.; Mehta, A.; Chaturvedi, A.K. Application of the Kaiser Score to Increase Diagnostic Accuracy in Equivocal Lesions on Diagnostic Mammograms Referred for MR Mammography. Eur. J. Radiol. 2021, 134, 109413. [Google Scholar] [CrossRef] [PubMed]
- Wengert, G.J.; Pipan, F.; Almohanna, J.; Bickel, H.; Polanec, S.; Kapetas, P.; Clauser, P.; Pinker, K.; Helbich, T.H.; Baltzer, P.A.T. Impact of the Kaiser Score on Clinical Decision-Making in BI-RADS 4 Mammographic Calcifications Examined with Breast MRI. Eur. Radiol. 2020, 30, 1451–1459. [Google Scholar] [CrossRef] [PubMed]
- Aslan, O.; Oktay, A. Diagnostic Accuracy of the Breast MRI Kaiser Score in Suspected Architectural Distortions and Its Comparison with Mammography. Sci. Rep. 2024, 14, 447. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Li, Z.; Yang, G.; Xue, J.; Zhang, L.; Rong, X. Diagnostic performance of the Kaiser score in the evaluation of breast lesions on contrast-enhanced mammography|Elsevier Enhanced Reader. Eur. J. Radiol. 2022, 156, 110524. [Google Scholar] [CrossRef]
- Milos, R.I.; Pipan, F.; Kalovidouri, A.; Clauser, P.; Kapetas, P.; Bernathova, M.; Helbich, T.H.; Baltzer, P.A.T. The Kaiser Score Reliably Excludes Malignancy in Benign Contrast-Enhancing Lesions Classified as BI-RADS 4 on Breast MRI High-Risk Screening Exams. Eur. Radiol. 2020, 30, 6052–6061. [Google Scholar] [CrossRef]
- Zhang, B.; Feng, L.; Wang, L.; Chen, X.; Li, X.; Yang, Q. Kaiser score for diagnosis of breast lesions presenting as non-mass enhancement on MRI. Nan Fang Yi Ke Da Xue Xue Bao 2020, 40, 562–566. [Google Scholar] [CrossRef]
- Istomin, A.; Masarwah, A.; Vanninen, R.; Okuma, H.; Sudah, M. Diagnostic Performance of the Kaiser Score for Characterizing Lesions on Breast MRI with Comparison to a Multiparametric Classification System. Eur. J. Radiol. 2021, 138, 109659. [Google Scholar] [CrossRef] [PubMed]
- Pötsch, N.; Clauser, P.; Kapetas, P.; Baykara Ulusan, M.; Helbich, T.; Baltzer, P. Enhancing the Kaiser Score for Lesion Characterization in Unenhanced Breast MRI. Eur. J. Radiol. 2024, 176, 111520. [Google Scholar] [CrossRef]
- Dietzel, M.; Bernathova, M.; Clauser, P.; Kapetas, P.; Uder, M.; Baltzer, P.A.T. Added Value of Clinical Decision Rules for the Management of Enhancing Breast MRI Lesions: A Systematic Comparison of the Kaiser Score and the Göttingen Score. Eur. J. Radiol. 2023, 169, 111185. [Google Scholar] [CrossRef] [PubMed]
- Dietzel, M.; Baltzer, P.A.T. How to Use the Kaiser Score as a Clinical Decision Rule for Diagnosis in Multiparametric Breast MRI: A Pictorial Essay. Insights Imaging 2018, 9, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Baltzer, P.A.T.; Kaiser, W.A.; Dietzel, M. Lesion Type and Reader Experience Affect the Diagnostic Accuracy of Breast MRI: A Multiple Reader ROC Study. Eur. J. Radiol. 2015, 84, 86–91. [Google Scholar] [CrossRef]
- Baltzer, P.A.T.; Krug, K.B.; Dietzel, M. Evidence-Based and Structured Diagnosis in Breast MRI Using the Kaiser Score. ROFO. Fortschr. Geb. Rontgenstr. Nuklearmed. 2022, 194, 1216–1228. [Google Scholar] [CrossRef]
- Pötsch, N.; Vatteroni, G.; Clauser, P.; Rainer, E.; Kapetas, P.; Milos, R.; Helbich, T.H.; Baltzer, P. Using the Kaiser Score as a Clinical Decision Rule for Breast Lesion Classification: Does Computer-Assisted Curve Type Analysis Improve Diagnosis? Eur. J. Radiol. 2024, 170, 111271. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Additional Lesion | |||
|---|---|---|---|
| Kaiser Score | Benign | Cancer | Total |
| 1 | 9 | 1 | 10 |
| 2 | 5 | 0 | 5 |
| 3 | 12 | 1 | 13 |
| 4 | 8 | 0 | 8 |
| 5 | 8 | 1 | 9 |
| 6 | 17 | 4 | 21 |
| 7 | 6 | 6 | 12 |
| 8 | 4 | 2 | 6 |
| 9 | 4 | 4 | 8 |
| 10 | 0 | 0 | 0 |
| 11 | 0 | 0 | 0 |
| Total | 73 | 19 | 92 |
| Lesion 1 | Lesion 2 | |
|---|---|---|
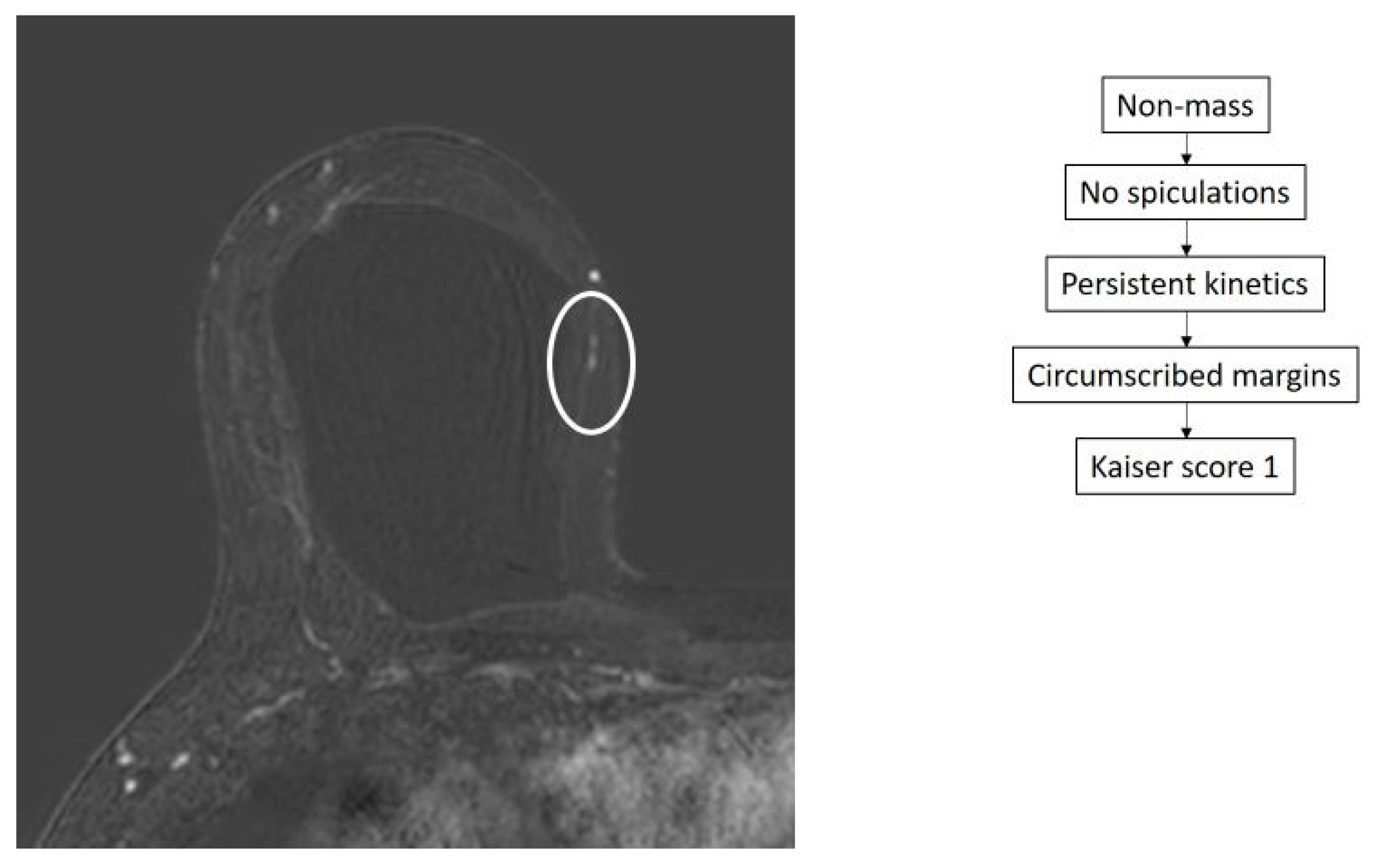
| Kaiser score | 1 | 3 |
| Pathology | DCIS | Invasive Tubular Carcinoma and DCIS |
| MRI type | Non-mass | Non-mass |
| MR shape | Linear | Clumped |
| Location with respect to the index cancer | Ipsilateral different quadrant | Ipsilateral different quadrant |
| Main suspicious feature | Additional unique enhancing lesion | Faint but asymmetrical enhancement compared to the contralateral side |
| Benign Lesion n (Percentage) | Cancer n (Percentage) | p Value * | OR | 95% C.I. for EXP(B) | |
|---|---|---|---|---|---|
| Kaiser score 1–4 | 34 (94.4%) | 2 (5.6%) | 0.004 | 7.410 | 1.5963–34.415 |
| Kaiser score 5 and above | 39 (69.6%) | 17 (30.4%) |
| Kaiser Score | |||
|---|---|---|---|
| Score 1–4 | Score 5 and above | p Value | |
| Index cancer | |||
| Pathology | 0.221 | ||
| DCIS | 13 (52%) | 12 (48%) | |
| IDC | 16 (34%) | 31 (66%) | |
| ILC | 1 (20%) | 4 (80%) | |
| Additional lesion | |||
| Size (mean in mm) | 12.6 | 16.8 | 0.167 |
| Location | |||
| Ipsilateral same quadrant | 0.957 | ||
| no | 31 (39.2%) | 48 (60.8%) | |
| yes | 5 (38.5%) | 8 (61.5%) | |
| Ipsilateral different quadrant | 0.081 | ||
| no | 27 (45.8%) | 32 (54.2%) | |
| yes | 9 (27.3%) | 24 (72.7%) | |
| Contralateral | 0.087 | ||
| no | 14 (30.4%) | 32 (69.6%) | |
| yes | 22 (47.8%) | 24 (52.2%) | |
| Imaging appearance | |||
| Type | 0.764 | ||
| NME | 24 (38.1%) | 39 (61.9%) | |
| Mass | 12 (41.4%) | 17 (58.6%) | |
| Enhancement type | 0.207 | ||
| clumped | 18 (42.9%) | 24 (57.1%) | |
| heterogeneous | 0 (0%) | 4 (100%) | |
| homogeneous | 11 (50%) | 11 (50%) | |
| rim | 0 (0%) | 1 (100%) | |
| linear | 5 (25%) | 15 (75%) | |
| Initial enhancement | 0.877 | ||
| Slow | 9 (36%) | 16 (64%) | |
| Medium | 4 (36.4%) | 7 (63.6%) | |
| Rapid | 22 (41.5%) | 31 (58.5%) | |
| Delayed enhancement | 0.601 | ||
| Persistent | 18 (45%) | 22 (55%) | |
| Plateau | 8 (33.3%) | 16 (66.7%) | |
| Washout | 9 (36%) | 16 (64%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hijazi, M.; Chahine, R.; Berjawi, G.; Jabbour, Y.; El Annan, T.; Ibrahim, R.; Nassar, L. Reliability of Kaiser Score in Assessing Additional Breast Lesions Identified on Staging MRI in Patients with Breast Cancer. Diagnostics 2024, 14, 1726. https://doi.org/10.3390/diagnostics14161726
Hijazi M, Chahine R, Berjawi G, Jabbour Y, El Annan T, Ibrahim R, Nassar L. Reliability of Kaiser Score in Assessing Additional Breast Lesions Identified on Staging MRI in Patients with Breast Cancer. Diagnostics. 2024; 14(16):1726. https://doi.org/10.3390/diagnostics14161726
Chicago/Turabian StyleHijazi, Madiha, Reve Chahine, Ghina Berjawi, Yara Jabbour, Tamara El Annan, Roy Ibrahim, and Lara Nassar. 2024. "Reliability of Kaiser Score in Assessing Additional Breast Lesions Identified on Staging MRI in Patients with Breast Cancer" Diagnostics 14, no. 16: 1726. https://doi.org/10.3390/diagnostics14161726