
The Usage of Different Hyaluronic-Acid-Containing Artificial Tears and the Treatment Outcome of Intense Pulsed Light Therapy for Dry Eye Disease: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Selection
2.2. Intense Pulsed Light Therapy
2.3. Dry Eye Evaluation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clayton, J.A. Dry Eye. N. Engl. J. Med. 2018, 378, 2212–2223. [Google Scholar] [CrossRef]
- Cai, Y.; Wei, J.; Zhou, J.; Zou, W. Prevalence and Incidence of Dry Eye Disease in Asia: A Systematic Review and Meta-Analysis. Ophthalmic Res. 2022, 65, 647–658. [Google Scholar] [CrossRef]
- Sheppard, J.; Shen Lee, B.; Periman, L.M. Dry eye disease: Identification and therapeutic strategies for primary care clinicians and clinical specialists. Ann. Med. 2023, 55, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Szczotka-Flynn, L.B.; Maguire, M.G.; Ying, G.S.; Lin, M.C.; Bunya, V.Y.; Dana, R.; Asbell, P.A. Impact of Dry Eye on Visual Acuity and Contrast Sensitivity: Dry Eye Assessment and Management Study. Optom. Vis. Sci. 2019, 96, 387–396. [Google Scholar] [CrossRef]
- Pflugfelder, S.C.; Stern, M.E. The cornea in keratoconjunctivitis sicca. Exp. Eye Res. 2020, 201, 108295. [Google Scholar] [CrossRef]
- Messmer, E.M. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch. Arztebl. Int. 2015, 112, 71–81, quiz 82. [Google Scholar] [CrossRef] [PubMed]
- Fogagnolo, P.; Giannaccare, G.; Mencucci, R.; Villani, E.; Orfeo, V.; Aragona, P. Effectiveness of a New Active Tear Substitute Containing 0.2% Hyaluronic Acid and 0.001% Hydrocortisone on Signs and Symptoms of Dry Eye Disease by Means of Low- and High-Tech Assessments. Ophthalmol. Ther. 2024, 13, 251–266. [Google Scholar] [CrossRef]
- Fogagnolo, P.; Romano, D.; De Ruvo, V.; Sabella, P.; Rossetti, L. Clinical Efficacy of an Eyedrop Containing Hyaluronic Acid and Ginkgo Biloba in the Management of Dry Eye Disease Induced by Cataract Surgery. J. Ocul. Pharmacol. Ther. 2022, 38, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Rolando, M.; Villella, E.; Loreggian, L.; Marini, S.; Loretelli, C.; Fiorina, P.; Barabino, S. Long-Term Activity and Safety of a Low-Dose Hydrocortisone Tear Substitute in Patients with Dry Eye Disease. Curr. Eye Res. 2023, 48, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.M.S.; Tighe, S.; Sheha, H.; Tseng, S.C.G. Adjunctive role of self-retained cryopreserved amniotic membrane in treating immune-related dry eye disease. Int. Ophthalmol. 2018, 38, 2219–2222. [Google Scholar] [CrossRef]
- Srinivasan, S.; Garofalo, R.; Williams, R. Safe and Effective Management of Dry Eye Symptoms with Hydroxypropyl Guar and Hyaluronic Acid Dual-Polymer Lubricating Eye Drops: A Review of Preclinical and Clinical Studies. Clin. Ophthalmol. 2023, 17, 3883–3898. [Google Scholar] [CrossRef] [PubMed]
- Yusufoğlu, E.; Keser, S. The effect of sodium hyaluronate on dry eye and corneal epithelial thickness following cataract surgery. Int. Ophthalmol. 2024, 44, 211. [Google Scholar] [CrossRef] [PubMed]
- Kojima, T.; Nagata, T.; Kudo, H.; Müller-Lierheim, W.G.K.; van Setten, G.B.; Dogru, M.; Tsubota, K. The Effects of High Molecular Weight Hyaluronic Acid Eye Drop Application in Environmental Dry Eye Stress Model Mice. Int. J. Mol. Sci. 2020, 21, 3516. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Patel, S.; Galor, A. Alternative therapies for dry eye disease. Curr. Opin. Ophthalmol. 2021, 32, 348–361. [Google Scholar] [CrossRef] [PubMed]
- Dell, S.J. Intense pulsed light for evaporative dry eye disease. Clin. Ophthalmol. 2017, 11, 1167–1173. [Google Scholar] [CrossRef]
- Toyos, R.; Desai, N.R.; Toyos, M.; Dell, S.J. Intense pulsed light improves signs and symptoms of dry eye disease due to meibomian gland dysfunction: A randomized controlled study. PLoS ONE 2022, 17, e0270268. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Pazo, E.E.; Zhang, Q.; Wu, Y.; Song, Y.; Qin, G.; Zhang, H.; Li, J.; Xu, L.; He, W. Treatment of contact lens related dry eye with intense pulsed light. Cont. Lens Anterior Eye 2022, 45, 101449. [Google Scholar] [CrossRef]
- Martínez-Hergueta, M.C.; Cantó-Cerdán, M.; Amesty, M.A.; García-Corral, M.J.; Casanova-Blanquer, L.; Plaza-Puche, A.B.; Alió, J.L.; Alió Del Barrio, J.L. Perioperative intense pulsed light to prevent and improve symptoms of post-laser corneal refractive surgery dry eye. A randomized clinical trial. Asia-Pac. J. Ophthalmol. 2024, 13, 100029. [Google Scholar] [CrossRef]
- Pazo, E.E.; Huang, H.; Fan, Q.; Zhang, C.; Yue, Y.; Yang, L.; Xu, L.; Moore, J.E.; He, W. Intense Pulse Light for Treating Post-LASIK Refractory Dry Eye. Photobiomodul. Photomed. Laser Surg. 2021, 39, 155–163. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, L.; Song, Y.; Zhang, Q.; Qin, G.; Yang, L.; Ma, J.; Palme, C.; Moore, J.E.; Pazo, E.E.; et al. Management of Post-LASIK Dry Eye with Intense Pulsed Light in Combination with 0.1% Sodium Hyaluronate and Heated Eye Mask. Ophthalmol. Ther. 2022, 11, 161–176. [Google Scholar] [CrossRef]
- Bron, A.J.; de Paiva, C.S.; Chauhan, S.K.; Bonini, S.; Gabison, E.E.; Jain, S.; Knop, E.; Markoulli, M.; Ogawa, Y.; Perez, V.; et al. TFOS DEWS II pathophysiology report. Ocul. Surf. 2017, 15, 438–510. [Google Scholar] [CrossRef] [PubMed]
- Rolando, M.; Zierhut, M. The ocular surface and tear film and their dysfunction in dry eye disease. Surv. Ophthalmol. 2001, 45 (Suppl. S2), S203–S210. [Google Scholar] [CrossRef] [PubMed]
- Roda, M.; Corazza, I.; Bacchi Reggiani, M.L.; Pellegrini, M.; Taroni, L.; Giannaccare, G.; Versura, P. Dry Eye Disease and Tear Cytokine Levels-A Meta-Analysis. Int. J. Mol. Sci. 2020, 21, 3111. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.R.; Praveen, M.; Narasimhan, R.; Khamar, P.; D’Souza, S.; Sinha-Roy, A.; Sethu, S.; Shetty, R.; Ghosh, A. Tear biomarkers in dry eye disease: Progress in the last decade. Indian. J. Ophthalmol. 2023, 71, 1190–1202. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, C.; Aragona, P.; Messmer, E.M.; Tomlinson, A.; Calonge, M.; Boboridis, K.G.; Akova, Y.A.; Geerling, G.; Labetoulle, M.; Rolando, M. Role of hyperosmolarity in the pathogenesis and management of dry eye disease: Proceedings of the OCEAN group meeting. Ocul. Surf. 2013, 11, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Seen, S.; Tong, L. Dry eye disease and oxidative stress. Acta Ophthalmol. 2018, 96, e412–e420. [Google Scholar] [CrossRef] [PubMed]
- Bu, J.; Liu, Y.; Zhang, R.; Lin, S.; Zhuang, J.; Sun, L.; Zhang, L.; He, H.; Zong, R.; Wu, Y.; et al. Potential New Target for Dry Eye Disease-Oxidative Stress. Antioxidants 2024, 13, 422. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.C.; Yang, S.F.; Lee, C.Y.; Hsueh, Y.J.; Huang, J.Y.; Chang, C.K. Differences in change of post-operative antioxidant levels between laser-assisted lenticule extraction and femtosecond laser in situ keratomileusis. J. Cell Mol. Med. 2024, 28, e18069. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.L.; Hung, Y.J.; Chen, Z.Y.; Fang, H.W.; Chen, K.H. Synergistic Effect of Artificial Tears Containing Epigallocatechin Gallate and Hyaluronic Acid for the Treatment of Rabbits with Dry Eye Syndrome. PLoS ONE 2016, 11, e0157982. [Google Scholar] [CrossRef] [PubMed]
- Macri, A.; Scanarotti, C.; Bassi, A.M.; Giuffrida, S.; Sangalli, G.; Traverso, C.E.; Iester, M. Evaluation of oxidative stress levels in the conjunctival epithelium of patients with or without dry eye, and dry eye patients treated with preservative-free hyaluronic acid 0.15% and vitamin B12 eye drops. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 425–430. [Google Scholar] [CrossRef]
- Hynnekleiv, L.; Magno, M.; Moschowits, E.; Tønseth, K.A.; Vehof, J.; Utheim, T.P. A comparison between hyaluronic acid and other single ingredient eye drops for dry eye, a review. Acta Ophthalmol. 2024, 102, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, D.F.; Millar, T.J.; Raju, S.R. Tear film stability: A review. Exp. Eye Res. 2013, 117, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Nomura, S.; Sato, Y.; Takagi, K.; Ishii, T.; Honma, Y.; Watanabe, K.; Mizukami, Y.; Muto, J. Anti-inflammatory effects of differential molecular weight Hyaluronic acids on UVB-induced calprotectin-mediated keratinocyte inflammation. J. Dermatol. Sci. 2022, 107, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Cho, P.; Yap, M. Schirmer test. I. A review. Optom. Vis. Sci. 1993, 70, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, A.; Martínez-Plaza, E.; Fernández, I.; Sobas, E.M.; González-García, M.J.; Enríquez-de-Salamanca, A.; Ortega, E.; López-Miguel, A.; Calonge, M. Phenotypic characterization of patients developing chronic dry eye and pain after refractive surgery: A cross-sectional study. Ocul. Surf. 2022, 26, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Mejía, L.F.; Gil, J.C.; Jaramillo, M. Intense pulsed light therapy: A promising complementary treatment for dry eye disease. Arch. Soc. Esp. Oftalmol. 2019, 94, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Yurttaser Ocak, S.; Karakus, S.; Ocak, O.B.; Cakir, A.; Bolukbasi, S.; Erden, B.; Bas, E.; Elcioglu, M. Intense pulse light therapy treatment for refractory dry eye disease due to meibomian gland dysfunction. Int. Ophthalmol. 2020, 40, 1135–1141. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Feature | 0.1% HA Group (N: 42) | 0.15% HA Group (N: 40) | p |
|---|---|---|---|
| Age (years, mean ± SD) | 46.23 ± 11.72 | 45.96 ± 12.51 | 0.905 |
| Sex (male: female) | 16:26 | 17:23 | 0.822 |
| Ocular disease | 0.526 | ||
| Retinal disorder | 2 | 1 | |
| Glaucoma | 0 | 0 | |
| Other | 1 | 0 | |
| Ocular surgery | 0.999 | ||
| Retinal surgery | 1 | 0 | |
| UDVA (LogMAR) | 0.38 ± 0.12 | 0.35 ± 0.13 | 0.260 |
| Cycloplegia SE (D) | −2.91 ± 1.36 | −2.65 ± 1.27 | 0.342 |
| IOP | 12.68 ± 2.74 | 12.89 ± 3.05 | 0.713 |
| NITBUT | 8.72 ± 3.35 | 8.84 ± 3.60 | 0.826 |
| Eyelid closure rate | 94.02 ± 5.69 | 93.78 ± 5.32 | 0.831 |
| Lipid thickness | 0.269 | ||
| Grade A–C | 25 | 18 | |
| Grade D–E | 17 | 22 | |
| TMH | 0.29 ± 0.10 | 0.28 ± 0.11 | 0.673 |
| Meibomian gland loss rate | 28.59 ± 6.68 | 29.27 ± 6.31 | 0.624 |
| Schirmer II test | 10.07 ± 4.63 | 9.84 ± 5.14 | 0.788 |
| Ocular surface stain | 0.651 | ||
| Grade 0–3 | 27 | 23 | |
| Grade 4–6 | 15 | 17 | |
| DED-related syndrome | 0.729 | ||
| 1 | 16 | 18 | |
| 2 | 16 | 15 | |
| ≥3 | 10 | 7 |
| Outcome | 0.1% HA Group (N: 42) | 0.15% HA Group (N: 40) | p |
|---|---|---|---|
| UDVA | 0.37 ± 0.14 | 0.35 ± 0.12 | 0.468 |
| SE | −2.90 ± 1.38 | −2.62 ± 1.28 | 0.313 |
| IOP | 13.16 ± 2.48 | 12.57 ± 3.38 | 0.334 |
| Schirmer II test | 11.74 ± 4.20 | 12.97 ± 3.46 | 0.101 |
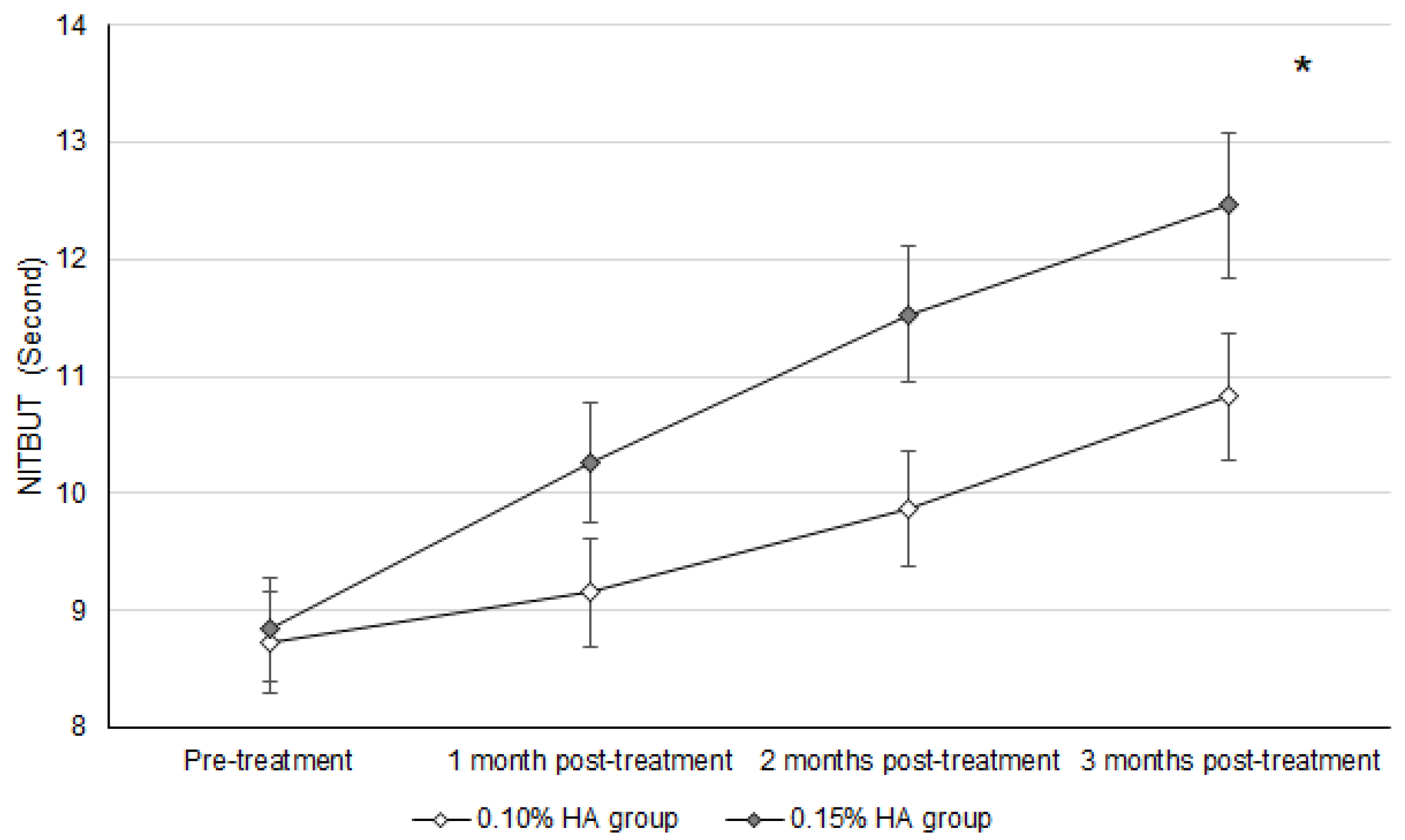
| NITBUT | 10.83 ± 3.14 | 12.46 ± 3.29 | 0.023 * |
| Ocular surface stain | 0.788 | ||
| Grade 0–3 | 34 | 31 | |
| Grade 4–6 | 8 | 9 | |
| DED-related syndrome | 0.508 | ||
| 1 | 24 | 25 | |
| 2 | 10 | 11 | |
| ≥3 | 8 | 4 |
| Outcome (Reference: 0.10% HA Group) | aOR | 95% CI | p | |
|---|---|---|---|---|
| Lower | Upper | |||
| Schirmer II test | 1.140 | 0.997 | 1.257 | 0.054 |
| NITBUT | 1.238 | 1.014 | 1.377 | 0.039 * |
| Ocular surface stain | 0.975 | 0.930 | 1.099 | 0.729 |
| DED-related syndromes | 1.005 | 0.942 | 1.183 | 0.636 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-Y.; Yang, S.-F.; Chen, Y.-C.; Chang, C.-K. The Usage of Different Hyaluronic-Acid-Containing Artificial Tears and the Treatment Outcome of Intense Pulsed Light Therapy for Dry Eye Disease: A Retrospective Cohort Study. Diagnostics 2024, 14, 1796. https://doi.org/10.3390/diagnostics14161796
Lee C-Y, Yang S-F, Chen Y-C, Chang C-K. The Usage of Different Hyaluronic-Acid-Containing Artificial Tears and the Treatment Outcome of Intense Pulsed Light Therapy for Dry Eye Disease: A Retrospective Cohort Study. Diagnostics. 2024; 14(16):1796. https://doi.org/10.3390/diagnostics14161796
Chicago/Turabian StyleLee, Chia-Yi, Shun-Fa Yang, Yun-Chen Chen, and Chao-Kai Chang. 2024. "The Usage of Different Hyaluronic-Acid-Containing Artificial Tears and the Treatment Outcome of Intense Pulsed Light Therapy for Dry Eye Disease: A Retrospective Cohort Study" Diagnostics 14, no. 16: 1796. https://doi.org/10.3390/diagnostics14161796