
Classification of Hydroxychloroquine Retinopathy: A Literature Review and Proposal for Revision

Abstract
:1. Introduction
2. Classification Systems of Hydroxychloroquine Retinopathy in the Literature
2.1. Modalities Used for Classification: Advances in Retinal Imaging
2.2. Classiciation According to Topographical Distribution
2.3. Severity Staging
3. Clinical Significance of Classifications for Hydroxychloroquine Retinopathy
3.1. Racial Variations in Presentation (Retinopathy Pattern) and Screening Recommendations
3.2. Management Decisions Based on Retinopathy Pattern and Stage
4. Limitations of the Suggested Classifications of Hydroxychloroquine Retinopathy
5. Proposed Disease Classification System
5.1. Classification in Terms of Topographic Distribution
5.2. Classification According to Disease Severity
6. Conclusions and Future Directions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levy, G.D.; Munz, S.J.; Paschal, J.; Cohen, H.B.; Pince, K.J.; Peterson, T. Incidence of hydroxychloroquine retinopathy in 1,207 patients in a large multicenter outpatient practice. Arthritis Rheum. 1997, 40, 1482–1486. [Google Scholar] [CrossRef] [PubMed]
- Marmor, M.F.; Kellner, U.; Lai, T.Y.; Melles, R.B.; Mieler, W.F.; American Academy of Ophthalmology. Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy (2016 Revision). Ophthalmology 2016, 123, 1386–1394. [Google Scholar] [CrossRef]
- Alarcon, G.S.; McGwin, G.; Bertoli, A.M.; Fessler, B.J.; Calvo-Alen, J.; Bastian, H.M.; Vila, L.M.; Reveille, J.D. Effect of hydroxychloroquine on the survival of patients with systemic lupus erythematosus: Data from LUMINA, a multiethnic US cohort (LUMINA L). Ann. Rheum. Dis. 2007, 66, 1168–1172. [Google Scholar] [CrossRef]
- Bernstein, H.N. Ocular safety of hydroxychloroquine. Ann. Ophthalmol. 1991, 23, 292–296. [Google Scholar]
- Bourke, B.; Jones, S.; Rajammal, A.; Silman, A.; Smith, R. Hydroxychloroquine and Ocular Toxicity Recommendations on Screening; The Royal College of Ophthalmologists: London, UK, 2009. [Google Scholar]
- Rempenault, C.; Combe, B.; Barnetche, T.; Gaujoux-Viala, C.; Lukas, C.; Morel, J.; Hua, C. Clinical and Structural Efficacy of Hydroxychloroquine in Rheumatoid Arthritis: A Systematic Review. Arthritis Care Res. 2019, 72, 36–40. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef]
- Gaujoux-Viala, C.; Smolen, J.S.; Landewe, R.; Dougados, M.; Kvien, T.K.; Mola, E.M.; Scholte-Voshaar, M.; van Riel, P.; Gossec, L. Current evidence for the management of rheumatoid arthritis with synthetic disease-modifying antirheumatic drugs: A systematic literature review informing the EULAR recommendations for the management of rheumatoid arthritis. Ann. Rheum. Dis. 2010, 69, 1004–1009. [Google Scholar] [CrossRef]
- Browning, D.J. Hydroxychloroquine and Chloroquine Retinopathy; Springer: New York, NY, USA, 2014. [Google Scholar]
- Browning, D.J.; Lee, C. Somatotype, the risk of hydroxychloroquine retinopathy, and safe daily dosing guidelines. Clin. Ophthalmol. 2018, 12, 811–818. [Google Scholar] [CrossRef]
- Marmor, M.F. The Demise of the Bull’s Eye (Screening for Hydroxychloroquine Retinopathy). Retina 2016, 36, 1803–1805. [Google Scholar] [CrossRef] [PubMed]
- Maturi, R.K.; Folk, J.C.; Nichols, B.; Oetting, T.T.; Kardon, R.H. Hydroxychloroquine retinopathy. Arch. Ophthalmol. 1999, 117, 1262–1263. [Google Scholar] [CrossRef] [PubMed]
- Allahdina, A.M.; Chen, K.G.; Alvarez, J.A.; Wong, W.T.; Chew, E.Y.; Cukras, C.A. Longitudinal changes in eyes with hydroxychloroquine retinal toxicity. Retina 2019, 39, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Brown, D.M.; Benz, M.S.; Fish, R.H.; Wong, T.P.; Kim, R.Y.; Major, J.C. Spectral domain optical coherence tomography as an effective screening test for hydroxychloroquine retinopathy (the “flying saucer” sign). Clin. Ophthalmol. 2010, 4, 1151–1158. [Google Scholar] [CrossRef]
- Anderson, C.; Blaha, G.R.; Marx, J.L. Humphrey visual field findings in hydroxychloroquine toxicity. Eye 2011, 25, 1535–1545. [Google Scholar] [CrossRef]
- Ahn, S.J.; Ryu, S.J.; Lim, H.W.; Lee, B.R. Toxic effects of hydroxychloroquine on the choroid: Evidence From Multimodal Imaging. Retina 2019, 39, 1016–1026. [Google Scholar] [CrossRef]
- Ahn, S.J.; Seo, E.J.; Kim, K.E.; Kim, Y.J.; Lee, B.R.; Kim, J.G.; Yoon, Y.H.; Lee, J.Y. Long-Term Progression of Pericentral Hydroxychloroquine Retinopathy. Ophthalmology 2021, 128, 889–898. [Google Scholar] [CrossRef] [PubMed]
- de Sisternes, L.; Hu, J.; Rubin, D.L.; Marmor, M.F. Localization of damage in progressive hydroxychloroquine retinopathy on and off the drug: Inner versus outer retina, parafovea versus peripheral fovea. Investig. Ophthalmol. Vis. Sci. 2015, 56, 3415–3426. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.J.; Joung, J.; Lee, B.R. Evaluation of Hydroxychloroquine Retinopathy Using Ultra-Widefield Fundus Autofluorescence: Peripheral Findings in the Retinopathy. Am. J. Ophthalmol. 2020, 209, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.E.; Ahn, S.J.; Woo, S.J.; Park, K.H.; Lee, B.R.; Lee, Y.K.; Sung, Y.K. Use of Optical Coherence Tomography Retinal Thickness Deviation Map for Hydroxychloroquine Retinopathy Screening. Ophthalmology 2021, 128, 110–119. [Google Scholar] [CrossRef]
- Lally, D.R.; Heier, J.S.; Baumal, C.; Witkin, A.J.; Maler, S.; Shah, C.P.; Reichel, E.; Waheed, N.K.; Bussel, I.; Rogers, A.; et al. Expanded spectral domain-OCT findings in the early detection of hydroxychloroquine retinopathy and changes following drug cessation. Int. J. Retin. Vitr. 2016, 2, 18. [Google Scholar] [CrossRef]
- Marmor, M.F. Comparison of screening procedures in hydroxychloroquine toxicity. Arch. Ophthalmol. 2012, 130, 461–469. [Google Scholar] [CrossRef]
- Marmor, M.F.; Chien, F.Y.; Johnson, M.W. Value of red targets and pattern deviation plots in visual field screening for hydroxychloroquine retinopathy. JAMA Ophthalmol 2013, 131, 476–480. [Google Scholar] [CrossRef]
- Rynes, R.I.; Krohel, G.; Falbo, A.; Reinecke, R.D.; Wolfe, B.; Bartholomew, L.E. Ophthalmologic safety of long-term hydroxychloroquine treatment. Arthritis Rheum. 1979, 22, 832–836. [Google Scholar] [CrossRef]
- Easterbrook, M. The ocular safety of hydroxychloroquine. Semin. Arthritis Rheum. 1993, 23, 62–67. [Google Scholar] [CrossRef]
- Easterbrook, M. Detection and prevention of maculopathy associated with antimalarial agents. Int. Ophthalmol. Clin. 1999, 39, 49–57. [Google Scholar] [CrossRef]
- Garrity, S.T.; Jung, J.Y.; Zambrowski, O.; Pichi, F.; Su, D.; Arya, M.; Waheed, N.K.; Duker, J.S.; Chetrit, Y.; Miserocchi, E.; et al. Early hydroxychloroquine retinopathy: Optical coherence tomography abnormalities preceding Humphrey visual field defects. Br. J. Ophthalmol. 2019, 103, 1600–1604. [Google Scholar] [CrossRef]
- Gobbett, A.; Kotagiri, A.; Bracewell, C.; Smith, J. Two years’ experience of screening for hydroxychloroquine retinopathy. Eye 2020, 35, 1171–1177. [Google Scholar] [CrossRef]
- Marmor, M.F.; Melles, R.B. Disparity between visual fields and optical coherence tomography in hydroxychloroquine retinopathy. Ophthalmology 2014, 121, 1257–1262. [Google Scholar] [CrossRef]
- Ahn, S.J.; Joung, J.; Lim, H.W.; Lee, B.R. Optical Coherence Tomography Protocols for Screening of Hydroxychloroquine Retinopathy in Asian Patients. Am. J. Ophthalmol. 2017, 184, 11–18. [Google Scholar] [CrossRef]
- Marmor, M.F. Fundus autofluorescence is not the best early screen for hydroxychloroquine toxicity. JAMA Ophthalmol 2013, 131, 1487–1488. [Google Scholar] [CrossRef]
- Marmor, M.F.; Kellner, U.; Lai, T.Y.; Lyons, J.S.; Mieler, W.F.; American Academy of Ophthalmology. Revised recommendations on screening for chloroquine and hydroxychloroquine retinopathy. Ophthalmology 2011, 118, 415–422. [Google Scholar] [CrossRef]
- Cheong, K.X.; Ong, C.J.T.; Chandrasekaran, P.R.; Zhao, J.; Teo, K.Y.C.; Mathur, R. Review of Retinal Imaging Modalities for Hydroxychloroquine Retinopathy. Diagnostics 2023, 13, 1752. [Google Scholar] [CrossRef]
- Lai, T.Y.; Chan, W.M.; Li, H.; Lai, R.Y.; Lam, D.S. Multifocal electroretinographic changes in patients receiving hydroxychloroquine therapy. Am. J. Ophthalmol. 2005, 140, 794–807. [Google Scholar] [CrossRef]
- Lai, T.Y.; Ngai, J.W.; Chan, W.M.; Lam, D.S. Visual field and multifocal electroretinography and their correlations in patients on hydroxychloroquine therapy. Doc. Ophthalmol. Adv. Ophthalmol. 2006, 112, 177–187. [Google Scholar] [CrossRef]
- Maturi, R.K.; Yu, M.; Weleber, R.G. Multifocal electroretinographic evaluation of long-term hydroxychloroquine users. Arch. Ophthalmol. 2004, 122, 973–981. [Google Scholar] [CrossRef]
- Browning, D.J.; Lee, C. Scotoma analysis of 10-2 visual field testing with a white target in screening for hydroxychloroquine retinopathy. Clin. Ophthalmol. 2015, 9, 943–952. [Google Scholar] [CrossRef]
- Kim, K.E.; Kim, Y.H.; Kim, J.; Ahn, S.J. Macular Ganglion Cell Complex and Peripapillary Retinal Nerve Fiber Layer Thicknesses in Hydroxychloroquine Retinopathy. Am. J. Ophthalmol. 2023, 245, 70–80. [Google Scholar] [CrossRef]
- Melles, R.B.; Marmor, M.F. Pericentral retinopathy and racial differences in hydroxychloroquine toxicity. Ophthalmology 2015, 122, 110–116. [Google Scholar] [CrossRef]
- Lee, D.H.; Melles, R.B.; Joe, S.G.; Lee, J.Y.; Kim, J.G.; Lee, C.K.; Yoo, B.; Koo, B.S.; Kim, J.T.; Marmor, M.F.; et al. Pericentral hydroxychloroquine retinopathy in Korean patients. Ophthalmology 2015, 122, 1252–1256. [Google Scholar] [CrossRef]
- Pham, B.H.; Marmor, M.F. Sequential changes in hydroxychloroquine retinopathy up to 20 years after stopping the drug: Implications for mild versus severe toxicity. Retina 2019, 39, 492–501. [Google Scholar] [CrossRef]
- Babeau, F.; Busetto, T.; Hamel, C.; Villain, M.; Daien, V. Adaptive optics: A tool for screening hydroxychloroquine-induced maculopathy? Acta Ophthalmol. 2017, 95, e424–e425. [Google Scholar] [CrossRef]
- Stepien, K.E.; Han, D.P.; Schell, J.; Godara, P.; Rha, J.; Carroll, J. Spectral-domain optical coherence tomography and adaptive optics may detect hydroxychloroquine retinal toxicity before symptomatic vision loss. Trans. Am. Ophthalmol. Soc. 2009, 107, 28–33. [Google Scholar]
- Marmor, M.F.; Durbin, M.; de Sisternes, L.; Pham, B.H. Sequential Retinal Thickness Analysis Shows Hydroxychloroquine Damage before Other Screening Techniques. Retin. Cases Brief Rep. 2021, 15, 185–196. [Google Scholar] [CrossRef]
- Melles, R.B.; Marmor, M.F. Rapid Macular Thinning Is an Early Indicator of Hydroxychloroquine Retinal Toxicity. Ophthalmology 2022, 129, 1004–1013. [Google Scholar] [CrossRef]
- Ahn, S.J.; Joung, J.; Lee, B.R. En Face Optical Coherence Tomography Imaging of the Photoreceptor Layers in Hydroxychloroquine Retinopathy. Am. J. Ophthalmol. 2019, 199, 71–81. [Google Scholar] [CrossRef]
- Rosenbaum, J.T.; Costenbader, K.H.; Desmarais, J.; Ginzler, E.M.; Fett, N.; Goodman, S.M.; O’Dell, J.R.; Schmajuk, G.; Werth, V.P.; Melles, R.B.; et al. American College of Rheumatology, American Academy of Dermatology, Rheumatologic Dermatology Society, and American Academy of Ophthalmology 2020 Joint Statement on Hydroxychloroquine Use With Respect to Retinal Toxicity. Arthritis Rheumatol. 2021, 73, 908–911. [Google Scholar] [CrossRef]
- Daich Varela, M.; Sen, S.; De Guimaraes, T.A.C.; Kabiri, N.; Pontikos, N.; Balaskas, K.; Michaelides, M. Artificial intelligence in retinal disease: Clinical application, challenges, and future directions. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 3283–3297. [Google Scholar] [CrossRef]
- Fan, W.S.; Nguyen, H.T.; Wang, C.Y.; Liang, S.W.; Tsao, Y.M.; Lin, F.C.; Wang, H.C. Detection of Hydroxychloroquine Retinopathy via Hyperspectral and Deep Learning through Ophthalmoscope Images. Diagnostics 2023, 13, 2373. [Google Scholar] [CrossRef]
- Kalra, G.; Talcott, K.E.; Kaiser, S.; Ugwuegbu, O.; Hu, M.; Srivastava, S.K.; Ehlers, J.P. Machine Learning-Based Automated Detection of Hydroxychloroquine Toxicity and Prediction of Future Toxicity Using Higher-Order OCT Biomarkers. Ophthalmol Retin. 2022, 6, 1241–1252. [Google Scholar] [CrossRef]
- Batioglu, F.; Yanik, O.; Demirel, S.; Ozmert, E. Clinical Use of Optical Coherence Tomography Angiography in Retinal Diseases. Diagnostics 2023, 13, 1820. [Google Scholar] [CrossRef]
- Chang, A.; Mieler, W.F.; Ohno-Matsui, K.; Lai, C.C. Retina Update: Entering an Era of Personalized Medicine in Ophthalmology. Asia-Pac. J. Ophthalmol. 2023, 12, 111–112. [Google Scholar] [CrossRef]
- Jorge, A.M.; Melles, R.B.; Marmor, M.F.; Zhou, B.; Zhang, Y.; Choi, H.K. Risk Factors for Hydroxychloroquine Retinopathy and Its Subtypes. JAMA Netw. Open 2024, 7, e2410677. [Google Scholar] [CrossRef]
- Melles, R.B.; Jorge, A.M.; Marmor, M.F.; Zhou, B.; Conell, C.; Niu, J.; McCormick, N.; Zhang, Y.; Choi, H.K. Hydroxychloroquine Dose and Risk for Incident Retinopathy: A Cohort Study. Ann. Intern. Med. 2023, 176, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Melles, R.B.; Marmor, M.F. The risk of toxic retinopathy in patients on long-term hydroxychloroquine therapy. JAMA Ophthalmol. 2014, 132, 1453–1460. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Classification | Definitions | References |
|---|---|---|
| Parafoveal retinopathy | 2°–6° from the fovea | [39] |
| 2°–8° from the fovea | [37,38] | |
| Pericentral retinopathy | Predominantly extramacular pattern of damage near the major retinal vascular arcades (beyond 8° from the fovea) | [37,38,39] |
| Mixed retinopathy | Both parafoveal and pericentral patterns | [38,39] |
| Author | Year | Classifications | References |
|---|---|---|---|
| Marmor | 2012 | 0. Normal on fields, SD-OCT, FAF, mfERG, full-field ERG 1. Patchy damage on fields, SD-OCT, and FAF and parafoveal weakness on mfERG 2. Bull’s eye damage on fields, SD-OCT, and FAF and central subnormal and parafoveal weakness on mfERG 3. Bull’s eye damage + fovea or RPE on fields, SD-OCT, and FAF and amplitudes 25–75% on full-field ERG 4. Diffuse posterior pole damage on fields, SD-OCT, and FAF and amplitudes < 25% on full-field ERG | [22] |
| De Sisternes et al. | 2015 | Early as patchy ellipsoid zone damage in the parafoveal region (i.e., areas of damage with parafoveal localization, but not coalesced into a clear ring) Moderate as a clear ring (50% to 100% complete) of damage, but still without RPE involvement observed by SD-OCT, funduscopy, and/or autofluorescence Severe as having RPE damage (by any of the assessment techniques) in the parafoveal bull’s-eye region | [18] |
| Lally et al. | 2016 | Early, no disruption of parafoveal or foveal EZ Obvious, disruption of parafoveal EZ with intact foveal EZ Severe, disruption of both foveal and parafoveal EZ | [21] |
| Allahdina et al. | 2019 | 1. Subtle changes confined to the parafoveal region 2. Definite localized changes in the parafovea 3. Extensive parafoveal changes; and 4, foveal involvement on OCT | [13] |
| Criterion | Modalities Used | Classifications | Definitions |
|---|---|---|---|
| Pattern | Optical coherence tomography (OCT) | Parafoveal | 2°–6° from the fovea (approximately 500–1500 μm from the foveal center) |
| Pericentral | Beyond 8° from the fovea | ||
| Combined parafoveal and pericentral * | Retinal damage involving, but confined to, both parafoveal and pericentral areas | ||
| Posterior polar with or without foveal involvement * | Retinal damage involving wide areas of the posterior pole (extending to the margin of the 30° or 9-mm OCT B-scan), with or without the fovea | ||
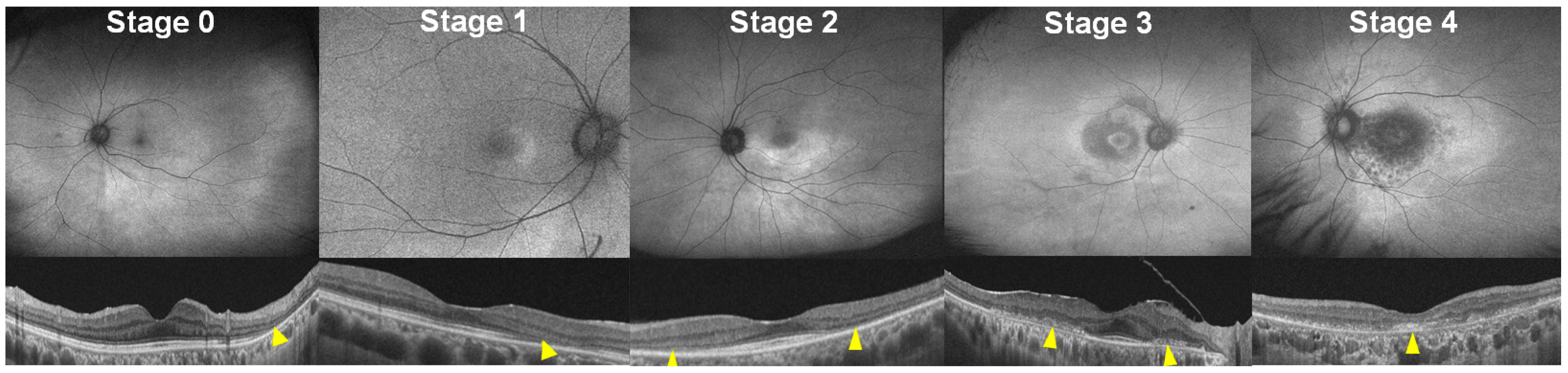
| Severity | Fundus autofluorescence (FAF) | Stage 0 | No abnormal finding, hyper- or hypoautofluorescence on FAF |
| Stage 1 | Localized hyperautofluorescence on FAF | ||
| Stage 2 | Hyperautofluorescence extending over 180° on FAF | ||
| Stage 3 | Combined RPE damage, hypo-autofluorescence on FAF, without foveal abnormality | ||
| Stage 4 | Hypoautofluorescence with foveal involvement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, S.J. Classification of Hydroxychloroquine Retinopathy: A Literature Review and Proposal for Revision. Diagnostics 2024, 14, 1803. https://doi.org/10.3390/diagnostics14161803
Ahn SJ. Classification of Hydroxychloroquine Retinopathy: A Literature Review and Proposal for Revision. Diagnostics. 2024; 14(16):1803. https://doi.org/10.3390/diagnostics14161803
Chicago/Turabian StyleAhn, Seong Joon. 2024. "Classification of Hydroxychloroquine Retinopathy: A Literature Review and Proposal for Revision" Diagnostics 14, no. 16: 1803. https://doi.org/10.3390/diagnostics14161803