
Revolutionizing Bladder Health: Artificial-Intelligence-Powered Automatic Measurement of Bladder Volume Using Two-Dimensional Ultrasound
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Endpoint
2.3. Study Protocol
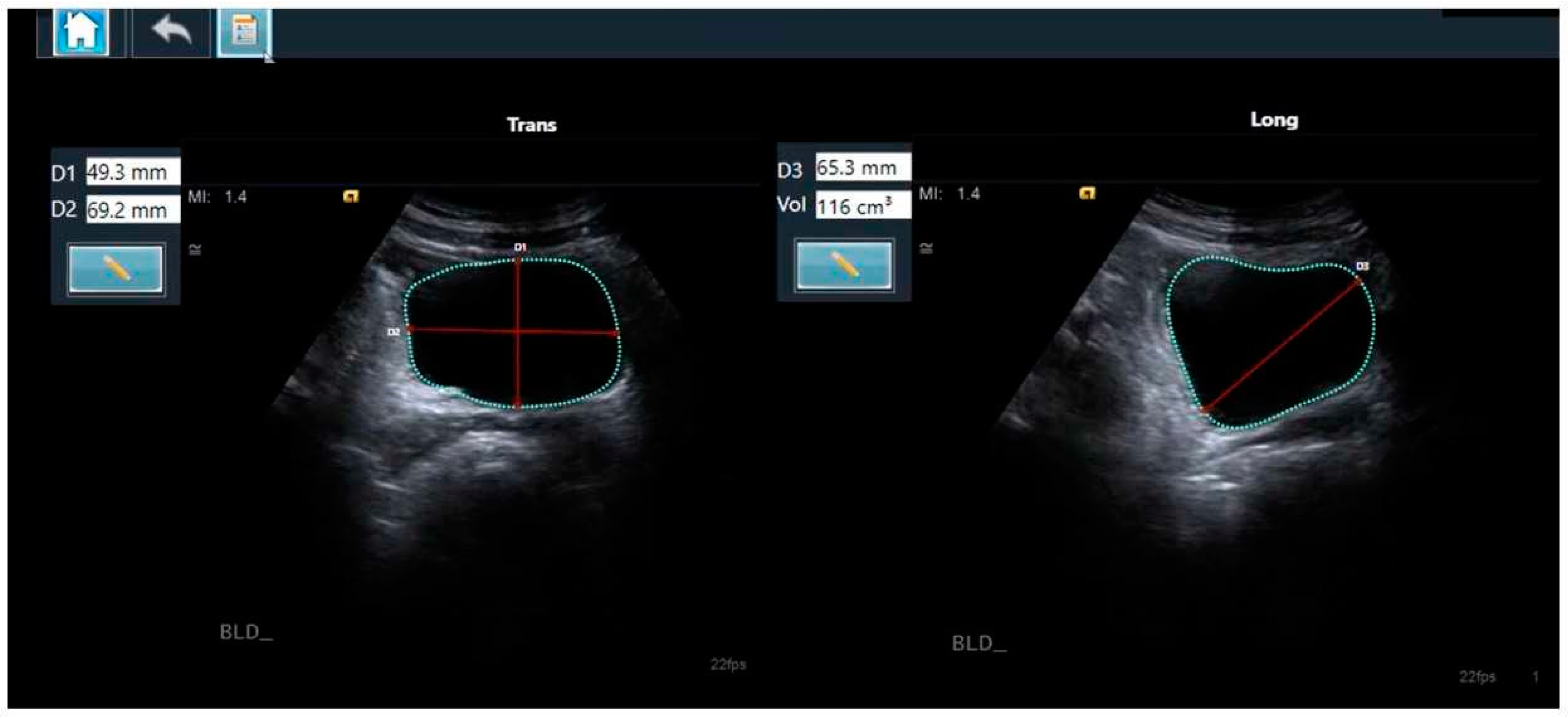
2.4. The Two-Dimensional Ultrasound-Based Bladder Volume Calculation Method
2.5. The AI-Based Module
2.6. Sample Size Calculation
2.7. The Statistical Analyses
3. Results
3.1. A Bladder Volume Assessment Comparison: The AI-Based Module vs. the Gold Standard
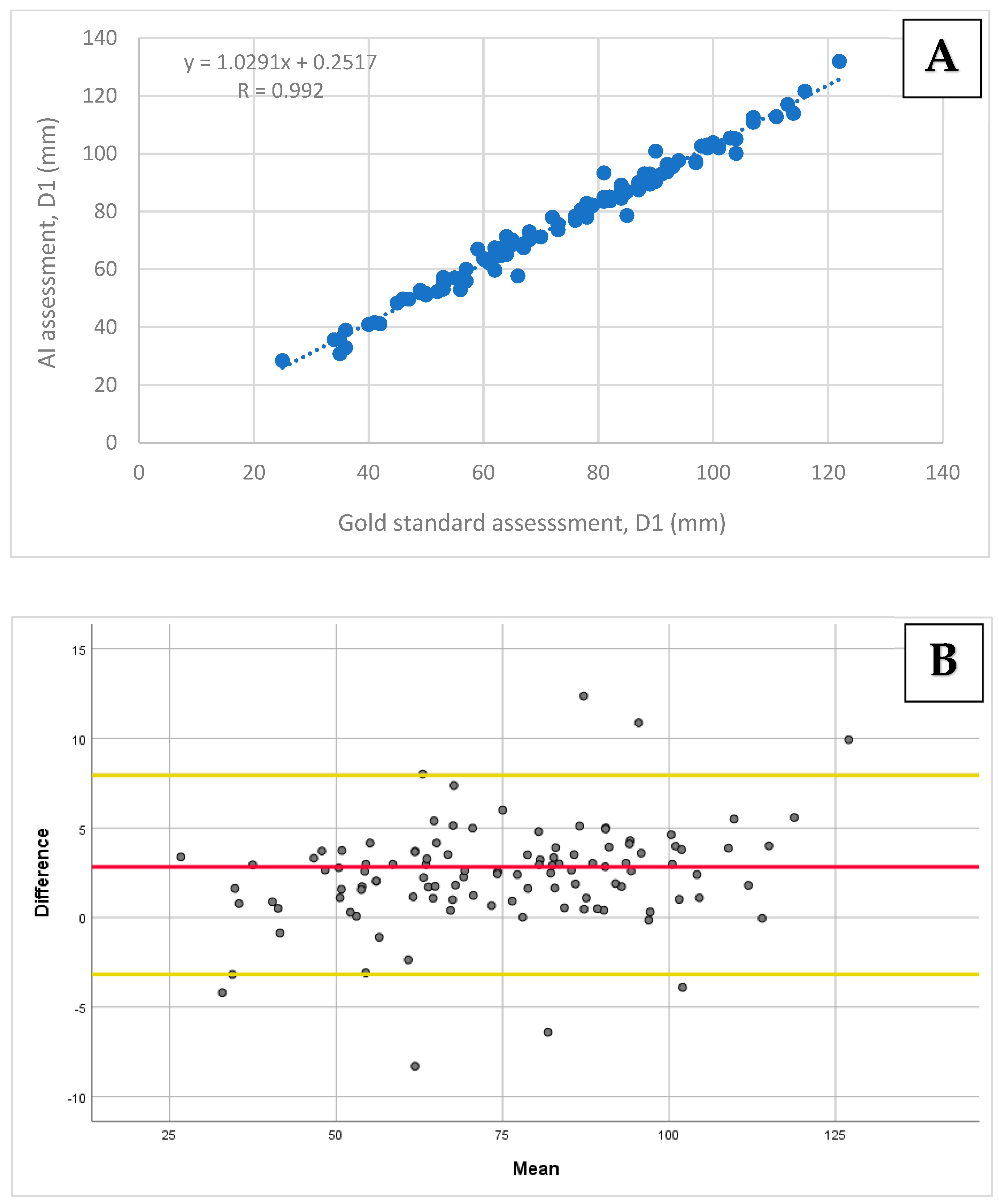
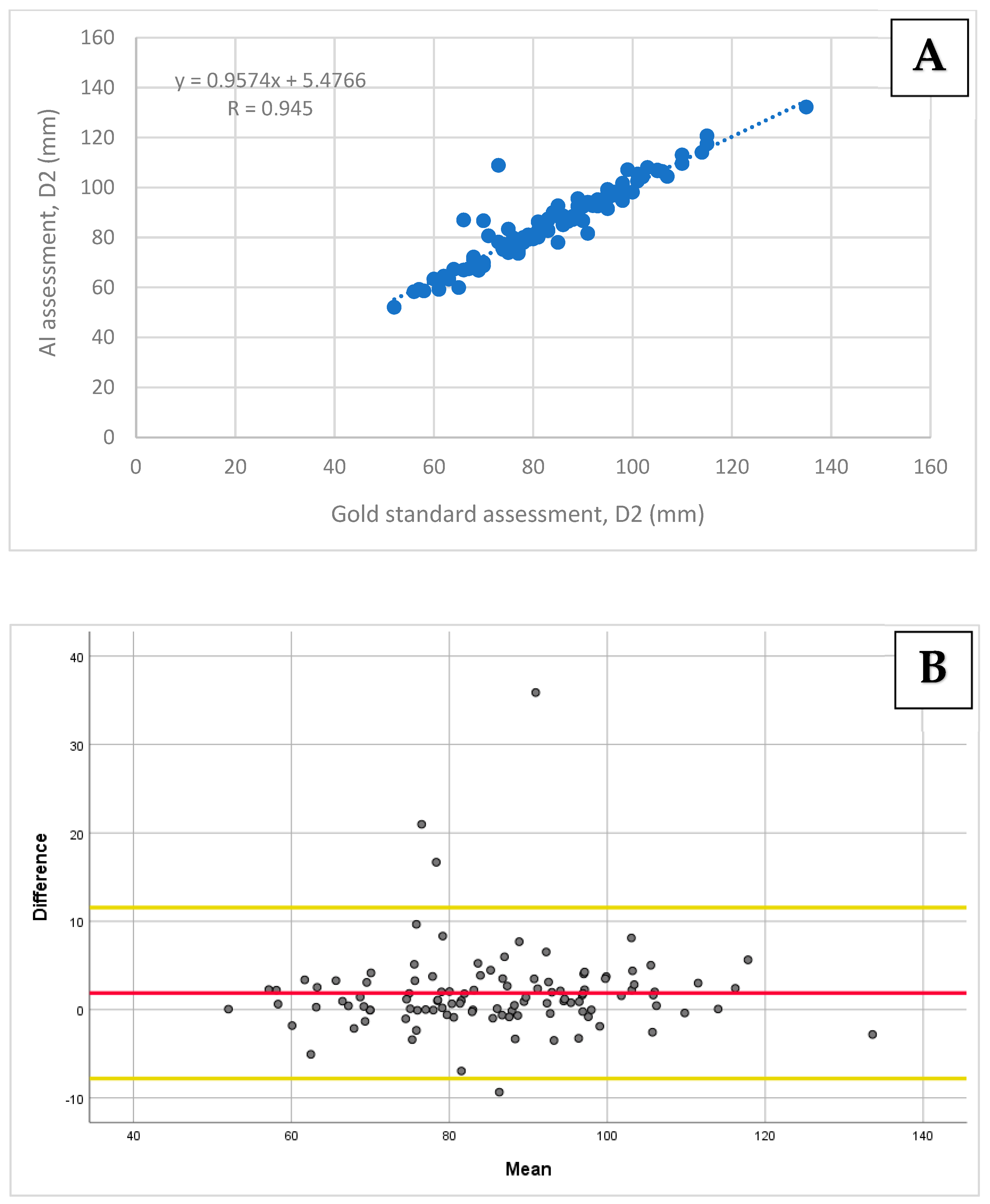
3.2. A Bladder Diameter (D1, D2, and D3) Measurement Comparison: The AI-Based Module vs. the Gold Standard
3.3. The Sensitivity and Specificity Analyses
3.4. The Inter- and Intra-Observer Variabilities
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spampinato, M.D.; Luppi, F.; Cristofaro, E.; Benedetto, M.; Cianci, A.; Bachechi, T.; Ghirardi, C.; Perna, B.; Guarino, M.; Passaro, A.; et al. Diagnostic accuracy of Point of Care UltraSound (POCUS) in clinical practice: A retrospective, emergency department based study. J. Clin. Ultrasound 2024, 52, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Ultrasound Guidelines: Emergency, Point-of-Care, and Clinical Ultrasound Guidelines in Medicine. Ann. Emerg. Med. 2023, 82, e115–e155. [CrossRef] [PubMed]
- Hartman, N.; Wittler, M.; Askew, K.; Hiestand, B.; Manthey, D. Validation of a performance checklist for ultrasound-guided internal jugular central lines for use in procedural instruction and assessment. Postgrad. Med. J. 2017, 93, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Farrow, R.A., 2nd; Shalaby, M.; Newberry, M.A.; Montes De Oca, R.; Kinas, D.; Farcy, D.A.; Zitek, T. Implementation of an Ultrasound-Guided Regional Anesthesia Program in the Emergency Department of a Community Teaching Hospital. Ann. Emerg. Med. 2024, 83, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Jeffers, K.L.; Cohen, J.; Chin, E.; Thompson, N.; Tekmal, S.; Lombardo, R.; Barlow, J.; Billstrom, A.; Aden, J.; Myers, M. Point of Care Ultrasounds Obtained by Novice Physician Assistant Residents (POCUS ON PAR). Mil. Med. 2024, usae219. [Google Scholar] [CrossRef]
- Stuckey, C.; Curtis, M.P. Development of a nurse-led ultrasound-guided peripheral intravenous program. J. Vasc. Nurs. 2019, 37, 246–249. [Google Scholar] [CrossRef]
- Bahl, A.; Pandurangadu, A.V.; Tucker, J.; Bagan, M. A randomized controlled trial assessing the use of ultrasound for nurse-performed IV placement in difficult access ED patients. Am. J. Emerg. Med. 2016, 34, 1950–1954. [Google Scholar] [CrossRef]
- Gundersen, G.H.; Norekval, T.M.; Haug, H.H.; Skjetne, K.; Kleinau, J.O.; Graven, T.; Dalen, H. Adding point of care ultrasound to assess volume status in heart failure patients in a nurse-led outpatient clinic. A randomised study. Heart 2016, 102, 29–34. [Google Scholar] [CrossRef]
- Farrington, E.A.; Maskell, G.; Hussaini, H.S. Feasibility and experience of nurse-led ultrasound-guided percutaneous liver biopsy. Frontline Gastroenterol. 2012, 3, 187–190. [Google Scholar] [CrossRef]
- Chenevert, L.; Coneybeare, D.; Weingart, G.; Truong, J. The effect of a point-of-care ultrasound curriculum on PAs in emergency medicine. JAAPA 2023, 36, 43–46. [Google Scholar] [CrossRef]
- Yamada, T.; Ehara, J.; Funakoshi, H.; Endo, K.; Kitano, Y. Effectiveness of point of care ultrasound (POCUS) simulation course and skills retention for Japanese nurse practitioners. BMC Nurs. 2023, 22, 21. [Google Scholar] [CrossRef] [PubMed]
- Gorick, H. How to triage patients in the emergency department. Emerg. Nurse 2023, 32, 18–21. [Google Scholar] [CrossRef]
- Dellimore, K.H.; Helyer, A.R.; Franklin, S.E. A scoping review of important urinary catheter induced complications. J. Mater. Sci. Mater. Med. 2013, 24, 1825–1835. [Google Scholar] [CrossRef]
- Duque-Sanchez, L.; Qu, Y.; Voelcker, N.H.; Thissen, H. Tackling catheter-associated urinary tract infections with next-generation antimicrobial technologies. J. Biomed. Mater. Res. A 2024, 112, 312–335. [Google Scholar] [CrossRef]
- Niederhauser, A.; Züllig, S.; Marschall, J.; Schwappach, D.L. Nurses’ and Physicians’ Perceptions of Indwelling Urinary Catheter Practices and Culture in Their Institutions. J. Patient Saf. 2020, 16, e82–e89. [Google Scholar] [CrossRef] [PubMed]
- Bent, A.E.; Nahhas, D.E.; McLennan, M.T. Portable ultrasound determination of urinary residual volume. Int. Urogynecol J. Pelvic Floor. Dysfunct. 1997, 8, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Coombes, G.M.; Millard, R.J. The accuracy of portable ultrasound scanning in the measurement of residual urine volume. J. Urol. 1994, 152 Pt 1, 2083–2085. [Google Scholar] [CrossRef] [PubMed]
- Dmochowski, R.R. Bladder outlet obstruction: Etiology and evaluation. Rev. Urol. 2005, 7 (Suppl. S6), S3–S13. [Google Scholar]
- Selius, B.A.; Subedi, R. Urinary retention in adults: Diagnosis and initial management. Am. Fam. Physician 2008, 77, 643–650. [Google Scholar]
- Stevens, E. Bladder ultrasound: Avoiding unnecessary catheterizations. Medsurg. Nurs. 2005, 14, 249–253. [Google Scholar]
- Negro, C.L.; Muir, G.H. Chronic urinary retention in men: How we define it, and how does it affect treatment outcome. BJU Int. 2012, 110, 1590–1594. [Google Scholar] [CrossRef] [PubMed]
- Katzouraki, G.; Zubairi, A.J.; Hershkovich, O.; Grevitt, M.P. A prospective study of the role of bladder scanning and post-void residual volume measurement in improving diagnostic accuracy of cauda equina syndrome. Bone Joint J. 2020, 102-B, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Schallom, M.; Prentice, D.; Sona, C.; Vyers, K.; Arroyo, C.; Wessman, B.; Ablordeppey, E. Accuracy of Measuring Bladder Volumes with Ultrasound and Bladder Scanning. Am. J. Crit. Care 2020, 29, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Annangi, P.; Frigstad, S.; Subin, S.B.; Torp, A.; Ramasubramaniam, S.; Varna, S. An automated bladder volume measurement algorithm by pixel classification using random forests. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2016, 2016, 4121–4124. [Google Scholar] [CrossRef] [PubMed]
- Hvarness, H.; Skjoldbye, B.; Jakobsen, H. Urinary bladder volume measurements: Comparison of three ultrasound calculation methods. Scand. J. Urol. Nephrol. 2002, 36, 177–181. [Google Scholar] [CrossRef]
- Dicuio, M.; Pomara, G.; Menchini Fabris, F.; Ales, V.; Dahlstrand, C.; Morelli, G. Measurements of urinary bladder volume: Comparison of five ultrasound calculation methods in volunteers. Arch. Ital. Urol. Androl. 2005, 77, 60–62. [Google Scholar]
- Rageth, J.C.; Langer, K. Ultrasonic assessment of residual urine volume. Urol. Res. 1982, 10, 57–60. [Google Scholar] [CrossRef]
- Chen, L.L. Standardized adult-gerontology acute care nurse practitioner point-of-care ultrasound training: A new perspective in the age of a pandemic. J. Am. Assoc. Nurse Pract. 2020, 32, 416–418. [Google Scholar] [CrossRef]
- Dornhofer, K.; Farhat, A.; Guan, K.; Parker, E.; Kong, C.; Kim, D.; Nguyen, T.; Mogi, J.; Lahham, S.; Fox, J.C. Evaluation of a point-of-care ultrasound curriculum taught by medical students for physicians, nurses, and midwives in rural Indonesia. J. Clin. Ultrasound 2020, 48, 145–151. [Google Scholar] [CrossRef]
- Matsumoto, M.; Tamai, N.; Miura, Y.; Okawa, Y.; Yoshida, M.; Igawa, Y.; Nakagami, G.; Sanada, H. Evaluation of a Point-of-Care Ultrasound Educational Program for Nurse Educators. J. Contin. Educ. Nurs. 2021, 52, 375–381. [Google Scholar] [CrossRef]
- Snelling, P.J.; Jones, P.; Keijzers, G.; Bade, D.; Herd, D.W.; Ware, R.S. Nurse practitioner administered point-of-care ultrasound compared with X-ray for children with clinically non-angulated distal forearm fractures in the ED: A diagnostic study. Emerg. Med. J. 2021, 38, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, P.; Bowra, J.; Lambert, M.; Lamprecht, H.; Noble, V.; Jarman, B. International Federation for Emergency Medicine point of care ultrasound curriculum. Can. J. Emerg. Med. 2015, 17, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Dadon, Z.; Orlev, A.; Butnaru, A.; Rosenmann, D.; Glikson, M.; Gottlieb, S.; Alpert, E.A. Empowering Medical Students: Harnessing Artificial Intelligence for Precision Point-of-Care Echocardiography Assessment of Left Ventricular Ejection Fraction. Int. J. Clin. Pract. 2023, 2023, 5225872. [Google Scholar] [CrossRef]
- Dadon, Z.; Rav Acha, M.; Orlev, A.; Carasso, S.; Glikson, M.; Gottlieb, S.; Alpert, E.A. Artificial Intelligence-Based Left Ventricular Ejection Fraction by Medical Students for Mortality and Readmission Prediction. Diagnostics 2024, 14, 767. [Google Scholar] [CrossRef]
- Kagiyama, N.; Abe, Y.; Kusunose, K.; Kato, N.; Kaneko, T.; Murata, A.; Ota, M.; Shibayama, K.; Izumo, M.; Watanabe, H. Multicenter validation study for automated left ventricular ejection fraction assessment using a handheld ultrasound with artificial intelligence. Sci. Rep. 2024, 14, 15359. [Google Scholar] [CrossRef]
- Shaikh, F.; Kenny, J.E.; Awan, O.; Markovic, D.; Friedman, O.; He, T.; Singh, S.; Yan, P.; Qadir, N.; Barjaktarevic, I. Measuring the accuracy of cardiac output using POCUS: The introduction of artificial intelligence into routine care. Ultrasound J. 2022, 14, 47. [Google Scholar] [CrossRef]
- Oikonomou, E.K.; Vaid, A.; Holste, G.; Coppi, A.; McNamara, R.L.; Baloescu, C.; Krumholz, H.M.; Wang, Z.; Apakama, D.J.; Nadkarni, G.N.; et al. Artificial intelligence-guided detection of under-recognized cardiomyopathies on point-of-care cardiac ultrasound: A multi-center study. medRxiv 2024. [Google Scholar] [CrossRef]
- Schneider, E.; Maimon, N.; Hasidim, A.; Shnaider, A.; Migliozzi, G.; Haviv, Y.S.; Halpern, D.; Abu Ganem, B.; Fuchs, L. Can Dialysis Patients Identify and Diagnose Pulmonary Congestion Using Self-Lung Ultrasound? J. Clin. Med. 2023, 12, 3829. [Google Scholar] [CrossRef]
- Marks, L.S.; Dorey, F.J.; Macairan, M.L.; Park, C.; deKernion, J.B. Three-dimensional ultrasound device for rapid determination of bladder volume. Urology 1997, 50, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Choe, J.H.; Lee, J.Y.; Lee, K.S. Accuracy and precision of a new portable ultrasound scanner, the BME-150A, in residual urine volume measurement: A comparison with the BladderScan BVI 3000. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2007, 18, 641–644. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Chambers, S.K.; Rutherford, T.J.; Foster, H.E., Jr. Cystic pelvic pathology presenting as falsely elevated post-void residual urine measured by portable ultrasound bladder scanning: Report of 3 cases and review of the literature. Urology 2000, 55, 590. [Google Scholar] [CrossRef] [PubMed]
- Yucel, S.; Kocak, H.; Sanli, A.; Tosun, O.; Tuncer, M.; Ersoy, F.; Baykara, M. How accurate is measuring postvoid residual volume by portable abdominal ultrasound equipment in peritoneal dialysis patient? Neurourol. Urodyn. 2005, 24, 358–361. [Google Scholar] [CrossRef]
- Barrington, J.W.; Jones, A.; Robinson, J.; Stephenson, T.P. Estimation of bladder volume using portable ultrasound in clam enterocystoplasty patients. J. Urol. 1996, 155, 82–83. [Google Scholar] [CrossRef] [PubMed]
- Barrington, J.W.; Arunkalaivanan, A.S.; Abdel Fattah, M. The accuracy of Bladderscan in intrapartum care. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2003, 14, 214–215; discussion 215. [Google Scholar] [CrossRef] [PubMed]
- Dudley, N.J.; Kirkland, M.; Lovett, J.; Watson, A.R. Clinical agreement between automated and calculated ultrasound measurements of bladder volume. Br. J. Radiol. 2003, 76, 832–834. [Google Scholar] [CrossRef]
- Prentice, D.M.; Sona, C.; Wessman, B.T.; Ablordeppey, E.A.; Isakow, W.; Arroyo, C.; Schallom, M. Discrepancies in measuring bladder volumes with bedside ultrasound and bladder scanning in the intensive care unit: A pilot study. J. Intensive Care Soc. 2018, 19, 122–126. [Google Scholar] [CrossRef]
- Moore, C.L.; Copel, J.A. Point-of-care ultrasonography. N. Engl. J. Med. 2011, 364, 749–757. [Google Scholar] [CrossRef]
- Smallwood, N.; Dachsel, M. Point-of-care ultrasound (POCUS): Unnecessary gadgetry or evidence-based medicine? Clin. Med. 2018, 18, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Dadon, Z.; Carasso, S.; Gottlieb, S. The Role of Hand-Held Cardiac Ultrasound in Patients with COVID-19. Biomedicines 2023, 11, 239. [Google Scholar] [CrossRef]
- Savino, K.; Ambrosio, G. Handheld Ultrasound and Focused Cardiovascular Echography: Use and Information. Medicina 2019, 55, 423. [Google Scholar] [CrossRef]
- Austin, D.R.; Chang, M.G.; Bittner, E.A. Use of handheld point-of-care ultrasound in emergency airway management. Chest 2021, 159, 1155–1165. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.N.; Rowland, J.; Haber, B.D.; Thom, S.; Jackson, B.; Volk, B.; Ehrman, R.R. The Use of Handheld Ultrasound Devices in Emergency Medicine. Curr. Emerg. Hosp. Med. Rep. 2021, 9, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Mancusi, C.; Carlino, M.V.; Sforza, A. Point-of-care ultrasound with pocket-size devices in emergency department. Echocardiography 2019, 36, 1755–1764. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.; Gardner, E.; Morley, T. Cauda equina syndrome: A review of the current clinical and medico-legal position. Eur. Spine J. 2011, 20, 690–697. [Google Scholar] [CrossRef]
- Long, B.; Koyfman, A.; Gottlieb, M. Evaluation and management of cauda equina syndrome in the emergency department. Am. J. Emerg. Med. 2020, 38, 143–148. [Google Scholar] [CrossRef]
- Fairbank, J.; Hashimoto, R.; Dailey, A.; Patel, A.A.; Dettori, J.R. Does patient history and physical examination predict MRI proven cauda equina syndrome? Evid. Based Spine Care J. 2011, 2, 27–33. [Google Scholar] [CrossRef]
- Sylvester, P.A.; McLoughlin, J.; Sibley, G.N.; Dorman, P.J.; Kabala, J.; Ormerod, I.E. Neuropathic urinary retention in the absence of neurological signs. Postgrad. Med. J. 1995, 71, 747–748. [Google Scholar] [CrossRef]
- Cooper, M.C.; Jones, J.; Pascual, M.; Field, S.; Rendon, J.M.; Kulstad, C.; Dixon, B.; Pham Tu, K.; Narayan, A.; Pyle, H.; et al. Can Medical Students Learn and Perform POCUS in the Pediatric Emergency Department? Implementation of a Short Curriculum. POCUS J. 2022, 7, 171–178. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alpert, E.A.; Gold, D.D.; Kobliner-Friedman, D.; Wagner, M.; Dadon, Z. Revolutionizing Bladder Health: Artificial-Intelligence-Powered Automatic Measurement of Bladder Volume Using Two-Dimensional Ultrasound. Diagnostics 2024, 14, 1829. https://doi.org/10.3390/diagnostics14161829
Alpert EA, Gold DD, Kobliner-Friedman D, Wagner M, Dadon Z. Revolutionizing Bladder Health: Artificial-Intelligence-Powered Automatic Measurement of Bladder Volume Using Two-Dimensional Ultrasound. Diagnostics. 2024; 14(16):1829. https://doi.org/10.3390/diagnostics14161829
Chicago/Turabian StyleAlpert, Evan Avraham, Daniel David Gold, Deganit Kobliner-Friedman, Michael Wagner, and Ziv Dadon. 2024. "Revolutionizing Bladder Health: Artificial-Intelligence-Powered Automatic Measurement of Bladder Volume Using Two-Dimensional Ultrasound" Diagnostics 14, no. 16: 1829. https://doi.org/10.3390/diagnostics14161829