
Magnetic Resonance Elastography for Staging Liver Fibrosis in the Oncopig

 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Animal Subjects
2.2. Liver Fibrosis Induction
2.3. MRI/MRE
2.4. Liver Biopsy and Tissue Processing
2.5. Definitions, Outcome Measures, and Statistics
3. Results
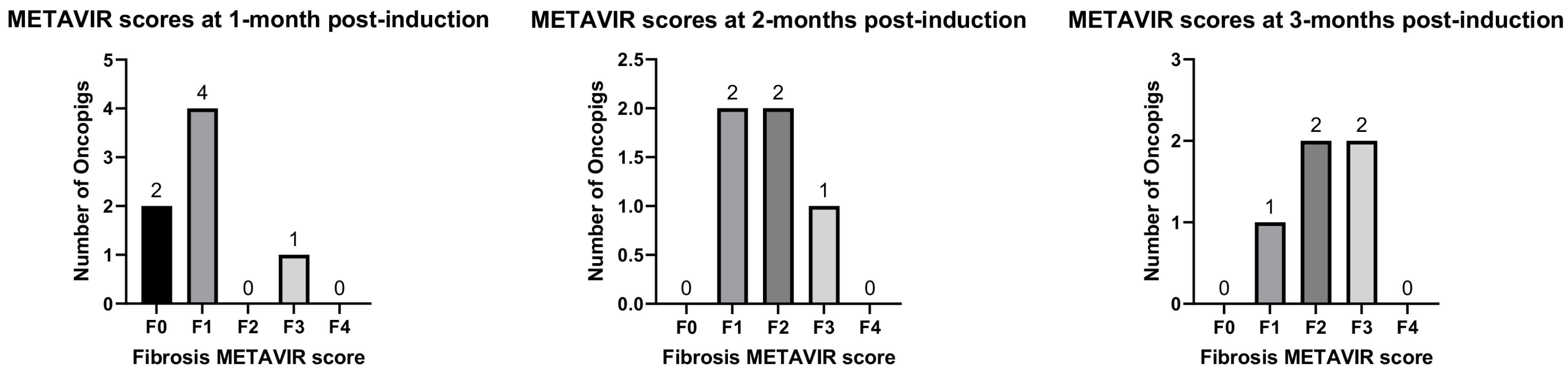
3.1. Induction of Liver Fibrosis in Oncopigs
3.2. Detection of Oncopig Liver Fibrosis Using MRE
3.3. Correlation between Liver Imaging and Histology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of liver diseases in the world. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef] [PubMed]
- Gines, P.; Castera, L.; Lammert, F.; Graupera, I.; Serra-Burriel, M.; Allen, A.M.; Wong, V.W.; Hartmann, P.; Thiele, M.; Caballeria, L.; et al. Population screening for liver fibrosis: Toward early diagnosis and intervention for chronic liver diseases. Hepatology 2022, 75, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Cotter, T.G.; Rinella, M. Nonalcoholic Fatty Liver Disease 2020: The State of the Disease. Gastroenterology 2020, 158, 1851–1864. [Google Scholar] [CrossRef]
- Schachtschneider, K.M.; Schwind, R.M.; Darfour-Oduro, K.A.; De, A.K.; Rund, L.A.; Singh, K.; Principe, D.R.; Guzman, G.; Ray, C.E., Jr.; Ozer, H.; et al. A validated, transitional and translational porcine model of hepatocellular carcinoma. Oncotarget 2017, 8, 63620–63634. [Google Scholar] [CrossRef]
- Gaba, R.C.; Elkhadragy, L.; Boas, F.E.; Chaki, S.; Chen, H.H.; El-Kebir, M.; Garcia, K.D.; Giurini, E.F.; Guzman, G.; LoBianco, F.V.; et al. Development and comprehensive characterization of porcine hepatocellular carcinoma for translational liver cancer investigation. Oncotarget 2020, 11, 2686–2701. [Google Scholar] [CrossRef] [PubMed]
- Nurili, F.; Monette, S.; Michel, A.O.; Bendet, A.; Basturk, O.; Askan, G.; Cheleuitte-Nieves, C.; Yarmohammadi, H.; Maxwell, A.W.P.; Ziv, E.; et al. Transarterial Embolization of Liver Cancer in a Transgenic Pig Model. J. Vasc. Interv. Radiol. 2021, 32, 510–517.e3. [Google Scholar] [CrossRef]
- Gaba, R.C.; Mendoza-Elias, N.; Regan, D.P.; Garcia, K.D.; Lokken, R.P.; Schwind, R.M.; Eichner, M.; Thomas, F.M.; Rund, L.A.; Schook, L.B.; et al. Characterization of an Inducible Alcoholic Liver Fibrosis Model for Hepatocellular Carcinoma Investigation in a Transgenic Porcine Tumorigenic Platform. J. Vasc. Interv. Radiol. 2018, 29, 1194–1202.e1. [Google Scholar] [CrossRef]
- Yasmin, A.; Regan, D.P.; Schook, L.B.; Gaba, R.C.; Schachtschneider, K.M. Transcriptional regulation of alcohol induced liver fibrosis in a translational porcine hepatocellular carcinoma model. Biochimie 2021, 182, 73–84. [Google Scholar] [CrossRef]
- Pirasteh, A.; Periyasamy, S.; Meudt, J.J.; Liu, Y.; Lee, L.M.; Schachtschneider, K.M.; Schook, L.B.; Gaba, R.C.; Mao, L.; Said, A.; et al. Staging Liver Fibrosis by Fibroblast Activation Protein Inhibitor PET in a Human-Sized Swine Model. J. Nucl. Med. 2022, 63, 1956–1961. [Google Scholar] [CrossRef]
- Ganne-Carrie, N.; Nahon, P.; Chaffaut, C.; N’Kontchou, G.; Layese, R.; Audureau, E.; Chevret, S.; CIRRAL group; ANRS CO12 CirVir group. Impact of cirrhosis aetiology on incidence and prognosis of hepatocellular carcinoma diagnosed during surveillance. JHEP Rep. 2021, 3, 100285. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, D.E.; Ripoll, C.; Thiele, M.; Fortune, B.E.; Simonetto, D.A.; Garcia-Tsao, G.; Bosch, J. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology 2024, 79, 1180–1211. [Google Scholar] [CrossRef]
- Dell, R.B.; Holleran, S.; Ramakrishnan, R. Sample size determination. ILAR J. 2002, 43, 207–213. [Google Scholar] [CrossRef]
- Avritscher, R.; Wright, K.C.; Javadi, S.; Uthamanthil, R.; Gupta, S.; Gagea, M.; Bassett, R.L.; Murthy, R.; Wallace, M.J.; Madoff, D.C. Development of a large animal model of cirrhosis and portal hypertension using hepatic transarterial embolization: A study in swine. J. Vasc. Interv. Radiol. 2011, 22, 1329–1334. [Google Scholar] [CrossRef]
- Johnson, C.L.; McGarry, M.D.; Gharibans, A.A.; Weaver, J.B.; Paulsen, K.D.; Wang, H.; Olivero, W.C.; Sutton, B.P.; Georgiadis, J.G. Local mechanical properties of white matter structures in the human brain. Neuroimage 2013, 79, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.L.; Holtrop, J.L.; McGarry, M.D.; Weaver, J.B.; Paulsen, K.D.; Georgiadis, J.G.; Sutton, B.P. 3D multislab, multishot acquisition for fast, whole-brain MR elastography with high signal-to-noise efficiency. Magn. Reson. Med. 2014, 71, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Sinkus, R.; Tanter, M.; Catheline, S.; Lorenzen, J.; Kuhl, C.; Sondermann, E.; Fink, M. Imaging anisotropic and viscous properties of breast tissue by magnetic resonance-elastography. Magn. Reson. Med. 2005, 53, 372–387. [Google Scholar] [CrossRef] [PubMed]
- Sinkus, R.; Tanter, M.; Xydeas, T.; Catheline, S.; Bercoff, J.; Fink, M. Viscoelastic shear properties of in vivo breast lesions measured by MR elastography. Magn. Reson. Imaging 2005, 23, 159–165. [Google Scholar] [CrossRef]
- Manduca, A.; Oliphant, T.E.; Dresner, M.A.; Mahowald, J.L.; Kruse, S.A.; Amromin, E.; Felmlee, J.P.; Greenleaf, J.F.; Ehman, R.L. Magnetic resonance elastography: Non-invasive mapping of tissue elasticity. Med. Image Anal. 2001, 5, 237–254. [Google Scholar] [CrossRef]
- Manduca, A.; Bayly, P.J.; Ehman, R.L.; Kolipaka, A.; Royston, T.J.; Sack, I.; Sinkus, R.; Van Beers, B.E. MR elastography: Principles, guidelines, and terminology. Magn. Reson. Med. 2021, 85, 2377–2390. [Google Scholar] [CrossRef]
- McGarry, M.D.J.; Van Houten, E.E.W. Use of a Rayleigh damping model in elastography. Med. Biol. Eng. Comput. 2008, 46, 759–766. [Google Scholar] [CrossRef]
- Yin, M.; Glaser, K.J.; Manduca, A.; Mounajjed, T.; Malhi, H.; Simonetto, D.A.; Wang, R.; Yang, L.; Mao, S.A.; Glorioso, J.M.; et al. Distinguishing between Hepatic Inflammation and Fibrosis with MR Elastography. Radiology 2017, 284, 694–705. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Yin, M.; Glaser, K.J.; Zhu, X.; Xu, K.; Ehman, R.L.; Chen, J. Static and dynamic liver stiffness: An ex vivo porcine liver study using MR elastography. Magn. Reson. Imaging 2017, 44, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.Y.; Abdelsalam, M.E.; Harmoush, S.; Ensor, J.E.; Chetta, J.A.; Hwang, K.P.; Stafford, R.J.; Madoff, D.C.; Avritscher, R. Evaluation of liver fibrosis and hepatic venous pressure gradient with MR elastography in a novel swine model of cirrhosis. J. Magn. Reson. Imaging 2014, 39, 590–597. [Google Scholar] [CrossRef]
- Duarte-Rojo, A.; Taouli, B.; Leung, D.H.; Levine, D.; Nayfeh, T.; Hasan, B.; Alsawaf, Y.; Saadi, S.; Majzoub, A.M.; Manolopoulos, A.; et al. Imaging-based non-invasive liver disease assessment for staging liver fibrosis in chronic liver disease: A systematic review supporting the AASLD Practice Guideline. Hepatology 2024. [Google Scholar] [CrossRef]
- Pepin, K.M.; Welle, C.L.; Guglielmo, F.F.; Dillman, J.R.; Venkatesh, S.K. Magnetic resonance elastography of the liver: Everything you need to know to get started. Abdom. Radiol. 2022, 47, 94–114. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence | Respiratory Gating | Purpose | Main Parameters |
|---|---|---|---|
| T2 BLADE with fat saturation, transversal | Imaging-based | T2-weighted images | TE/TR 144/2500 ms, 38 cm FOV, 20 slices (5 mm skip 25%), voxel size 1.2 × 1.2 × 5 mm, 15% accept window |
| T2 BLADE without fat saturation, transversal | Imaging-based | T2-weighted images with fat included | TE/TR 156/2500 ms, 38 cm FOV, 20 slices (5 mm skip 25%), voxel size 1.2 × 1.2 × 5 mm, 15% accept window |
| TSE Dixon, transversal | Imaging-based | Fat/water images; highlight fatty tumors | TE/TR 99/4480 ms, 34 cm FOV, 35 slices (5 mm skip 20%), voxel size 0.9 × 0.9 × 5 mm, 15% accept window |
| TurboFLASH in-phase/opposite-phase images, transversal | Imaging-based | In-phase and opposed-phase images for fat/water to show fatty infiltration | TE/TR 2.46/1800 ms, 38 cm FOV, 20 slices (5 mm skip 25%), voxel size 0.7 × 0.7 × 5 mm, 15% accept window |
| T1 TurboFLASH, coronal | Imaging-based | T1-weighted images | TE/TR 2.31/2000 ms, 40 cm FOV, 30 slices (5 mm skip 20%), voxel size 0.8 × 0.8 × 5 mm, 15% accept window |
| Pd + T2 + T2 TSE, transversal | Imaging-based | Multiple contrast from proton density to T2 to TSE T2 | TE1/TE2/TE3/TR 41/107/205/2500 ms, 20 slices (5 mm skip 25%), voxel size 1.5 × 1.5 × 5 mm, 15% accept window |
| EPI diffusion-weighted imaging, transversal | No gating | Diffusion-weighted images for Trace with b-values of 50 and 800 s/mm2 | 4 scan trace, TE/TR 39/4900 ms, 36 slices (4 mm skip 20%), voxel size 1.4 × 1.4 × 4 |
| EPI MRE, transversal | Breath hold | Elastography | TE/TR 35/1200.96 ms, 12 slices (5 mm skip 0%), voxel size 4.9 × 4.9 × 5 mm, 60 Hz, 4 time points, 8.927 μm/rad, duration 34 s |
| T1 VIBE, transversal | Breath hold | DCE venous enhancement characteristics | TE1/TE2/TR 1.29/2.52/3.97 ms, 1 slice 3 mm, voxel size 1.2 × 1.2 × 3 mm, duration 15 s Run at pre injection (x2), then post injection at 20 s, 50 s, 2 min, 5 min, and 7.5 min |
| Grade | Description |
|---|---|
| F0 | Normal porcine liver; no increase in fibrosis. |
| F1 | Mild fibrous expansion of portal areas and/or mild thickening/expansion of few random segments of normal pre-existing fibrous septa. |
| F2 | Mild-to-moderate fibrous expansion of portal tracts and multiple, random, non-contiguous segments of normal fibrous septa surrounding multiple hepatic lobules ± presence of thin bands of fibrosis extending from septa or portal tracts into adjacent lobular parenchyma. |
| F3 | Moderate-to-marked fibrous expansion of contiguous segments of fibrous septa surrounding multiple hepatic lobules; fibrous expansion can involve contiguous segments of septa and partially encircle hepatic lobules, but it typically does not completely circumscribe lobules. Presence of fibrous connective tissue that dissects into lobular parenchyma, surrounding and separating cords of hepatocytes. |
| F4 | Cirrhosis; normal fibrous septa surrounding hepatic lobules are expanded by moderate-to-marked amounts of fibrous connective tissue, with some portal bridging, frequent dissection into adjacent lobular parenchyma, and separation of hepatic cords. Fibrous connective tissue often completely circumscribes multiple hepatic lobules, which appear irregular/shrunken. |
| Pig | 1 Month | 2 Months | 3 Months |
|---|---|---|---|
| A337 | F1 | F1 | F2 |
| A339 | F1 | F2 | F3 |
| A341 | F1 | F1 | F3 |
| A342 | F0 | F2 | F2 |
| A344 | F3 | - | - |
| A345 | F1 | F3 | F1 |
| A347 | F0 | - | - |
| Pig | 1-Month Liver Stiffness (kPA) | 2-Month Liver Stiffness (kPA) | 3-Month Liver Stiffness (kPA) |
|---|---|---|---|
| A337 | 2.51 ± 0.43 | 2.53 * | 2.90 ± 0.52 |
| A339 | 2.41 ± 0.29 | 2.76 ± 0.65 | 2.21 ± 0.15 |
| A341 | 2.80 ± 0.26 | 4.10 ± 0.77 | 3.23 ± 0.36 |
| A342 | 3.07 ± 0.51 | 2.83 ± 0.76 | 2.87 ± 0.71 |
| A344 | 3.30 ± 0.24 | - | - |
| A345 | 3.11 ± 0.11 | 3.36 ± 0.71 | 3.32 ± 0.32 |
| A347 | 3.40 ± 0.18 | 3.94 ± 0.32 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaba, R.C.; Elkhadragy, L.; Pennix, T.; Schachtschneider, K.M.; Bolt, C.R.; Anderson, A.; Majumdar, S.; Weber, D.; Whiteley, H.E.; Regan, D.P.; et al. Magnetic Resonance Elastography for Staging Liver Fibrosis in the Oncopig. Diagnostics 2024, 14, 1880. https://doi.org/10.3390/diagnostics14171880
Gaba RC, Elkhadragy L, Pennix T, Schachtschneider KM, Bolt CR, Anderson A, Majumdar S, Weber D, Whiteley HE, Regan DP, et al. Magnetic Resonance Elastography for Staging Liver Fibrosis in the Oncopig. Diagnostics. 2024; 14(17):1880. https://doi.org/10.3390/diagnostics14171880
Chicago/Turabian StyleGaba, Ron C., Lobna Elkhadragy, Thomas Pennix, Kyle M. Schachtschneider, Courtni R. Bolt, Aaron Anderson, Shreyan Majumdar, Denise Weber, Herbert E. Whiteley, Daniel P. Regan, and et al. 2024. "Magnetic Resonance Elastography for Staging Liver Fibrosis in the Oncopig" Diagnostics 14, no. 17: 1880. https://doi.org/10.3390/diagnostics14171880
APA StyleGaba, R. C., Elkhadragy, L., Pennix, T., Schachtschneider, K. M., Bolt, C. R., Anderson, A., Majumdar, S., Weber, D., Whiteley, H. E., Regan, D. P., Schook, L. B., & Sutton, B. P. (2024). Magnetic Resonance Elastography for Staging Liver Fibrosis in the Oncopig. Diagnostics, 14(17), 1880. https://doi.org/10.3390/diagnostics14171880