

Long-Term Survival in BRCA1 Mutant Advanced Ovarian Cancer: Unveiling the Impact of Olaparib

 , , and
, , and
Abstract
1. Introduction
2. Case Presentations
2.1. First Case Presentation
2.1.1. Main Characteristics and Admission to Hospital
2.1.2. History, Comorbidities, and Interventions
2.1.3. Examinations and Investigations
2.1.4. Diagnosis
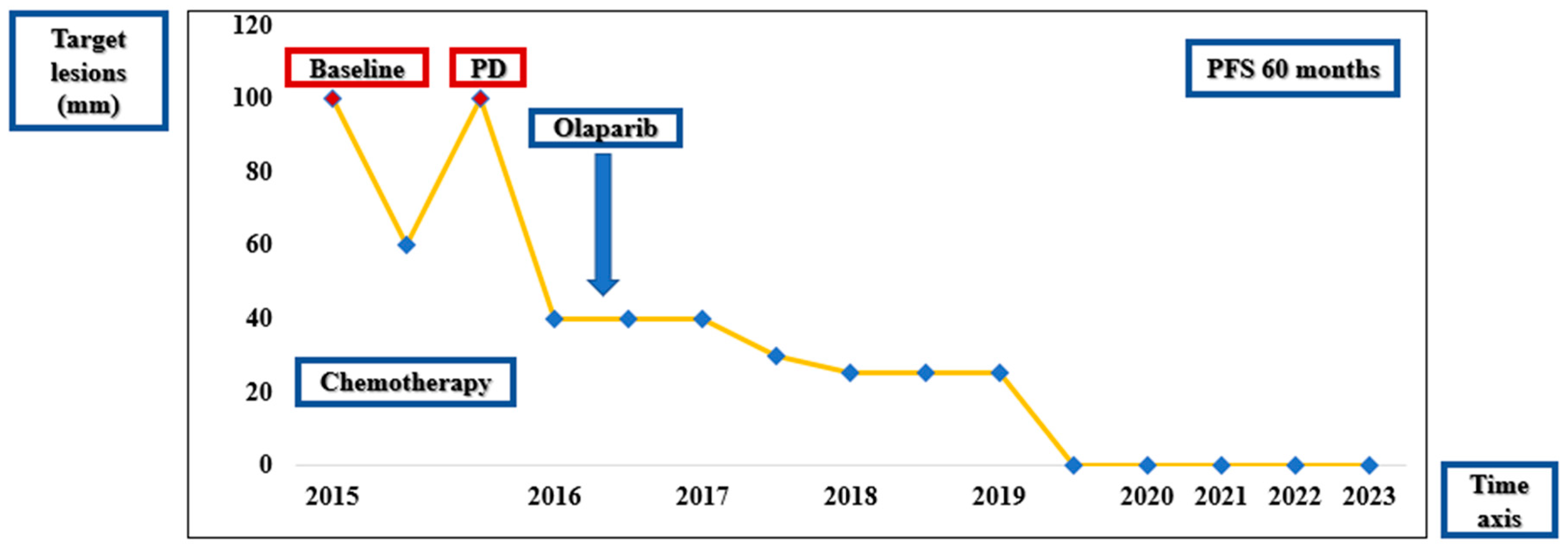
2.1.5. Treatment and Outcomes
2.1.6. Follow-Up
2.1.7. Compliance
2.2. Second Case Presentation
2.2.1. Main Characteristics and Admission to Hospital
2.2.2. History, Comorbidities, and Interventions
2.2.3. Examinations and Investigations
2.2.4. Diagnosis
2.2.5. Treatment and Outcomes
2.2.6. Follow-Up
2.2.7. Compliance
3. Discussion
3.1. Case Discussions
3.2. Romanian Landscape of BRCA Mutations
3.3. Biomarkers in Ovarian Cancer–BRCA and ER
3.4. Limitations of the Study
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cortez, A.J.; Tudrej, P.; Kujawa, K.A.; Lisowska, K.M. Advances in ovarian cancer therapy. Cancer Chemother. Pharmacol. 2018, 81, 17–38. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Guarneri, V.; Peccatori, F.A.; Ronzino, G.; Scandurra, G.; Zamagni, C.; Zola, P.; Salutari, V. Current strategies for the targeted treatment of high-grade serous epithelial ovarian cancer and relevance of BRCA mutational status. J. Ovarian Res. 2019, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Alexa, T.; Luca, A.; Dondas, A.; Bohotin, C.R. Preconditioning with cobalt chloride modifies pain perception in mice. Exp. Ther. Med. 2015, 9, 1465–1469. [Google Scholar] [CrossRef]
- Franzese, E.; Centonze, S.; Diana, A.; Carlino, F.; Guerrera, L.P.; Di Napoli, M.; De Vita, F.; Pignata, S.; Ciardiello, F.; Orditura, M. PARP inhibitors in ovarian cancer. Cancer Treat. Rev. 2019, 73, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Evans, T.; Matulonis, U. PARP inhibitors in ovarian cancer: Evidence, experience and clinical potential. Ther. Adv. Med. Oncol. 2017, 9, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Pommier, Y.; O’connor, M.J.; de Bono, J. Laying a trap to kill cancer cells: PARP inhibitors and their mechanisms of action. Sci. Transl. Med. 2016, 8, 362ps17. [Google Scholar] [CrossRef]
- Neagu, A.N.; Whitham, D.; Buonanno, E.; Jenkins, A.; Alexa-Stratulat, T.; Tamba, B.I.; Darie, C.C. Proteomics and its applications in breast cancer. Am. J. Cancer Res. 2021, 11, 4006–4049. [Google Scholar] [PubMed] [PubMed Central]
- Vos, J.R.; E Fakkert, I.; A de Hullu, J.; van Altena, A.M.; Sie, A.S.; Ouchene, H.; Willems, R.W.; Nagtegaal, I.D.; Jongmans, M.C.J.; Mensenkamp, A.R.; et al. Universal tumor DNA BRCA 1/2 testing of ovarian cancer: Prescreening PARPI treatment and genetic predisposition. J. Natl. Cancer Inst. 2020, 112, 161–169. [Google Scholar] [CrossRef]
- Tan, D.S.; Kaye, S.B. Chemotherapy for patients with BRCA1 and BRCA2-mutated ovarian cancer: Same or different? Am. Soc. Clin. Oncol. Educ. Book 2015, 35, 114–121. [Google Scholar] [CrossRef]
- Zhang, S.; Royer, R.; Li, S.; McLaughlin, J.R.; Rosen, B.; Risch, H.A.; Fan, I.; Bradley, L.; Shaw, P.A.; Narod, S.A. Frequencies of BRCA1 and BRCA2 mutations among 1,342 unselected patients with invasive ovarian cancer. Gynecol. Oncol. 2011, 121, 353–357. [Google Scholar] [CrossRef]
- National Library of Medicine. Available online: https://www.ncbi.nlm.nih.gov/clinvar/variation/17662/ (accessed on 6 February 2021).
- Online Mendelian Inheritance. Available online: https://omim.org/entry/113705#0003 (accessed on 6 February 2021).
- Struewing, J.P.; Abeliovich, D.; Peretz, T.; Avishai, N.; Kaback, M.M.; Collins, F.S.; Brody, L.C. The carrier frequency of the BRCA1 185delAG mutation is approximately 1 percent in Ashkenazi Jewish individuals. Nat. Genet. 1995, 11, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Abeliovich, D.; Kaduri, L.; Lerer, I.; Weinberg, N.; Amir, G.; Sagi, M.; Zlotogora, J.; Heching, N.; Peretz, T. The founder mutations 185delAG and 5382insC in BRCA1 and 6174delT in BRCA2 appear in 60% of ovarian cancer and 30% of early-onset breast cancer patients among Ashkenazi women. Am. J. Hum. Genet. 1997, 60, 505–514. [Google Scholar]
- Qin, Z.; Li, J.; Tam, B.; Sinha, S.; Zhao, B.; Bhaskaran, S.P.; Huang, T.; Wu, X.; Chian, J.S.; Guo, M.; et al. Ethnic-specificity, evolution origin and deleteriousness of Asian BRCA variation revealed by over 7500 BRCA variants derived from Asian population. Int. J. Cancer 2023, 152, 1159–1173. [Google Scholar] [CrossRef]
- Negura, L.; Uhrhammer, N.; Negura, A.; Artenie, V.; Carasevici, E.; Bignon, Y.-J. Complete BRCA mutation screening in breast and ovarian cancer predisposition families from a North-Eastern Romanian population. Fam. Cancer 2010, 9, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Goidescu, I.G.; Caracostea, G.; Eniu, D.T.; Stamatian, F.V. Prevalence of deleterious mutations among patients with breast cancer referred for multigene panel testing in a Romanian population. Clujul Med. 2018, 91, 157. [Google Scholar] [CrossRef]
- Janavičius, R. Founder BRCA1/2 mutations in the Europe: Implications for hereditary breast-ovarian cancer prevention and control. EPMA J. 2010, 1, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Negură, L.; Carasevici, E.; Negură, A.; Uhrhammer, N.; Bignon, Y.J. Identification of a recurrent BRCA1 mutation in two breast/ovarian cancer predisposition families with distinct phenotypes, by using allele-specific multiplex-PCR. Rev. Română Med. Lab. 2010, 18, 53–61. [Google Scholar]
- Negură, L.; Duşa, C.P.; Balmuş, M.I.; Azoicăi, D.; Negură, A.M.; Marinca, M.V.; Miron, L. BRCA1 5382insC founder mutation has not a significative recurrent presence in Northeastern Romanian cancer patients. Rom. J. Morphol. Embryol. 2015, 56, 379–385. [Google Scholar]
- Stanculeanu, D.; Median, D.M.; Cebotaru, C.L.; Teodorescu, G.; Voinea, C. EP987 Prevalence and spectrum of BRCA mutations in patients with platinum-sensitive ovarian cancer from Romania—Results of an observational study. Int. J. Gynecol. Cancer 2019, 29, A52. [Google Scholar]
- Eniu, A.; Pop, L.; Stoian, A.; Dronca, E.; Matei, R.; Ligtenberg, M.; Ouchene, H.; Onisim, A.; Rotaru, O.; Eniu, R.; et al. Understanding BRCA1 and BRCA2 mutated breast cancer cases in Romania: First report on founder mutations in Romanians. Ann. Oncol. 2017, 28 (Suppl. 5), v43–v67. [Google Scholar] [CrossRef]
- Vidra, R.; Ciuleanu, T.E.; Nemeș, A.; Pascu, O.; Heroiu, A.M.; Antone, N.; Vidrean, A.I.; Oprean, C.M.; Pop, L.A.; Berindan-Neagoe, I.; et al. Spectrum of BRCA1/2 Mutations in Romanian Breast and Ovarian Cancer Patients. Int. J. Environ. Res. Public Health 2022, 19, 4314. [Google Scholar] [CrossRef]
- Karami, F.; Mehdipour, P. A comprehensive focus on global spectrum of BRCA1 and BRCA2 mutations in breast cancer. Biomed. Res. Int. 2013, 2013, 928562. [Google Scholar] [CrossRef]
- Cătană, A.; Trifa, A.P.; Achimas-Cadariu, P.A.; Bolba-Morar, G.; Lisencu, C.; Kutasi, E.; Chelaru, V.F.; Muntean, M.; Martin, D.L.; Antone, N.Z.; et al. Hereditary Breast Cancer in Romania—Molecular Particularities and Genetic Counseling Challenges in an Eastern European Country. Biomedicines 2023, 11, 1386. [Google Scholar] [CrossRef]
- Bolton, K.L.; Chenevix-Trench, G.; Goh, C.; Sadetzki, S.; Ramus, S.J.; Karlan, B.Y.; Lambrechts, D.; Despierre, E.; Barrowdale, D.; McGuffog, L.; et al. Association between BRCA 1 and BRCA 2 mutations and survival in women with invasive epithelial ovarian cancer. JAMA 2012, 307, 382–390. [Google Scholar] [CrossRef]
- Friedlander, M.; Matulonis, U.; Gourley, C.; du Bois, A.; Vergote, I.; Rustin, G.; Scott, C.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Long-term efficacy, tolerability and overall survival in patients with platinum-sensitive, recurrent high-grade serous ovarian cancer treated with maintenance olaparib capsules following response to chemotherapy. Br. J. Cancer 2018, 119, 1075–1085. [Google Scholar] [CrossRef]
- Poveda, A.; Floquet, A.; A Ledermann, J.; Asher, R.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Pignata, S.; Friedlander, M.; et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): A final analysis of a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2021, 22, 620–631. [Google Scholar] [CrossRef]
- Lheureux, S.; Lai, Z.; Dougherty, B.A.; Runswick, S.; Hodgson, D.R.; Timms, K.M.; Lanchbury, J.S.; Kaye, S.; Gourley, C.; Bowtell, D.; et al. Long-Term Responders on Olaparib Maintenance in High-Grade Serous Ovarian Cancer: Clinical and Molecular Characterization. Clin. Cancer Res. 2017, 23, 4086–4094. [Google Scholar] [CrossRef]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.L.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: A preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol. 2014, 15, 852–861. [Google Scholar] [CrossRef]
- Swisher, E.M.; Kristeleit, R.S.; Oza, A.M.; Tinker, A.V.; Ray-Coquard, I.; Oaknin, A.; Coleman, R.L.; Burris, H.A.; Aghajanian, C.; O’Malley, D.M.; et al. Characterization of patients with long-term responses to rucaparib treatment in recurrent ovarian cancer. Gynecol. Oncol. 2021, 163, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D. What predicts the clinical benefits of PARP inhibitors in platinum-sensitive recurrent ovarian cancer: A real-world single-center retrospective cohort study from China. Front. Oncol. 2022, 12, 955124. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Moore, K.N.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; et al. Maintenance olaparib for patients with newly diagnosed advanced ovarian cancer and a BRCA mutation (SOLO1/GOG 3004): 5-year follow-up of a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2021, 22, 1721–1731. [Google Scholar] [CrossRef]
- A Study of Long-Term Responders on Olaparib (OLALA), ClinicalTrials.gov ID NCT02489058. Available online: https://clinicaltrials.gov/ct2/show/NCT02489058 (accessed on 9 July 2024).
- Giudice, E.; Gentile, M.; Salutari, V.; Ricci, C.; Musacchio, L.; Carbone, M.V.; Ghizzoni, V.; Camarda, F.; Tronconi, F.; Nero, C.; et al. PARP inhibitors resistance: Mechanisms and perspectives. Cancers 2022, 14, 1420. [Google Scholar] [CrossRef]
- Ng, C.W.; Wong, K.K. Impact of estrogen receptor expression on prognosis of ovarian cancer according to antibody clone used for immunohistochemistry: A meta-analysis. J. Ovarian Res. 2022, 15, 63. [Google Scholar] [CrossRef]
- Paleari, L.; Gandini, S.; Provinciali, N.; Puntoni, M.; Colombo, N.; DeCensi, A. Clinical benefit and risk of death with endocrine therapy in ovarian cancer: A comprehensive review and meta-analysis. Gynecol. Oncol. 2017, 146, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Perez-Gracia, J.L.; Carrasco, E.M. Tamoxifen therapy for ovarian cancer in the adjuvant and advanced settings: Systematic review of the literature and implications for future research. Gynecol. Oncol. 2002, 84, 201–209. [Google Scholar] [CrossRef]
- Stanley, B.; Hollis, R.L.; Nunes, H.; Towler, J.D.; Yan, X.; Rye, T.; Dawson, C.; Mackean, M.J.; Nussey, F.; Churchman, M.; et al. Endocrine treatment of high grade serous ovarian carcinoma; quantification of efficacy and identification of response predictors. Gynecol. Oncol. 2019, 152, 278–285. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Point | Hemoglobin (g/dL) | Thrombocytes (mm3) | CA-125 (IU/L) |
|---|---|---|---|
| July 2015 (diagnosis) | 10.4 | 883,000 | 520.00 |
| December 2015 (3 × Carboplatin/Paclitaxel; 1 × Carboplatin) | 6.4 | 238,000 | 10.00 |
| April 2016 (progression) | 11.9 | 190,000 | 354.00 |
| November 2017 (Olaparib start) | 10.6 | 125,000 | 12.00 |
| April 2018–January 2020 (stable disease under Olaparib therapy) | 13.1 | 317,000 | 8.00 |
| February 2020–February 2021 (complete response under Olaparib therapy) | 13.8 | 293,000 | 7.80 |
| March 2021–March 2022 | 12.4 | 212,000 | 7.20 |
| March 2022–December 2023 | 13.4 | 233,000 | 7.60 |
| Time Point | Hemoglobin (g/dL) | Thrombocytes (mm3) | CA-125 (IU/L) |
|---|---|---|---|
| September 2015 (diagnosis) | 10.0 | 552,000 | 1852.00 |
| February 2016 (after 6 × Carboplatin/Paclitaxel) | 11.5 | 296,000 | 9.04 |
| May 2016 (after interval debulking surgery) | 11.5 | 233,000 | 7.04 |
| September 2016 (after 5 × Carboplatin/Paclitaxel) | 8.0 | 96,000 | - |
| October 2016 (start Olaparib maintenance) | 7.9 | 121,000 | 5.79 |
| October 2016–August 2018 (partial response under Olaparib therapy) | 9.5 * | 256,000 * | 7.80 * |
| August 2018–December 2021 (complete response under Olaparib therapy) | 9.7 * | 330,000 * | 12.70 * |
| January 2022 (progression) | 11.3 | 278,000 | 145.20 |
| June 2022 (after secondary cytoreductive surgery) | 10.1 | 488,000 | 18.65 |
| November 2022 (start Tamoxifen treatment) | 11.7 | 229,000 | 8.66 |
| November 2022–December 2023 | 12.7 * | 190,000 * | 16.37 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afrăsânie, V.-A.; Rusu, A.; Gheorghe, A.S.; Froicu, E.M.; Dumitrescu, E.A.; Gafton, B.; Alexa-Stratulat, T.; Miron, L.; Stănculeanu, D.L.; Marinca, M.V. Long-Term Survival in BRCA1 Mutant Advanced Ovarian Cancer: Unveiling the Impact of Olaparib. Diagnostics 2024, 14, 1898. https://doi.org/10.3390/diagnostics14171898
Afrăsânie V-A, Rusu A, Gheorghe AS, Froicu EM, Dumitrescu EA, Gafton B, Alexa-Stratulat T, Miron L, Stănculeanu DL, Marinca MV. Long-Term Survival in BRCA1 Mutant Advanced Ovarian Cancer: Unveiling the Impact of Olaparib. Diagnostics. 2024; 14(17):1898. https://doi.org/10.3390/diagnostics14171898
Chicago/Turabian StyleAfrăsânie, Vlad-Adrian, Alexandra Rusu, Adelina Silvana Gheorghe, Eliza Maria Froicu, Elena Adriana Dumitrescu, Bogdan Gafton, Teodora Alexa-Stratulat, Lucian Miron, Dana Lucia Stănculeanu, and Mihai Vasile Marinca. 2024. "Long-Term Survival in BRCA1 Mutant Advanced Ovarian Cancer: Unveiling the Impact of Olaparib" Diagnostics 14, no. 17: 1898. https://doi.org/10.3390/diagnostics14171898
APA StyleAfrăsânie, V.-A., Rusu, A., Gheorghe, A. S., Froicu, E. M., Dumitrescu, E. A., Gafton, B., Alexa-Stratulat, T., Miron, L., Stănculeanu, D. L., & Marinca, M. V. (2024). Long-Term Survival in BRCA1 Mutant Advanced Ovarian Cancer: Unveiling the Impact of Olaparib. Diagnostics, 14(17), 1898. https://doi.org/10.3390/diagnostics14171898