
White Light Diffraction Phase Microscopy in Imaging of Breast and Colon Tissues

 , , , ,
, , , ,  ,
,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
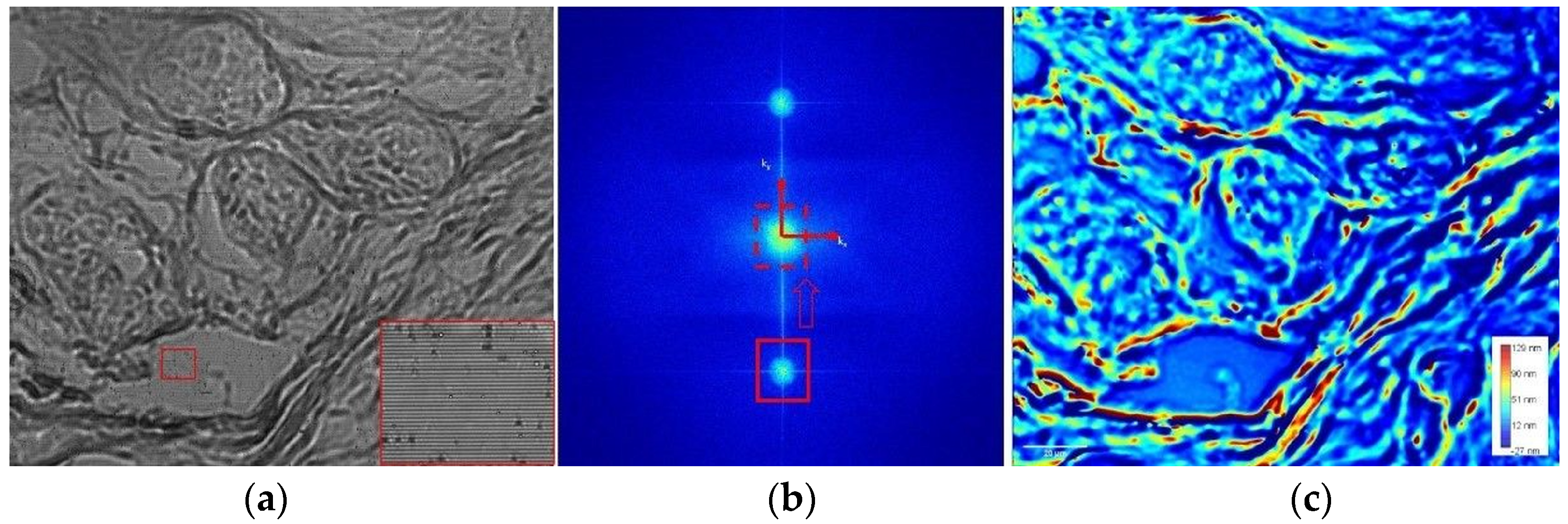
2. Description of wDPM
3. Materials and Methods
4. Results and Discussion
- (a)
- Breast tissue with benign lesions (typical ductal hyperplasia, unstained specimens);
- (b)
- Colon tumor tissue; standard H&E—stained samples.
- (c)
- Normal colon tissue; standard H&E—stained samples.
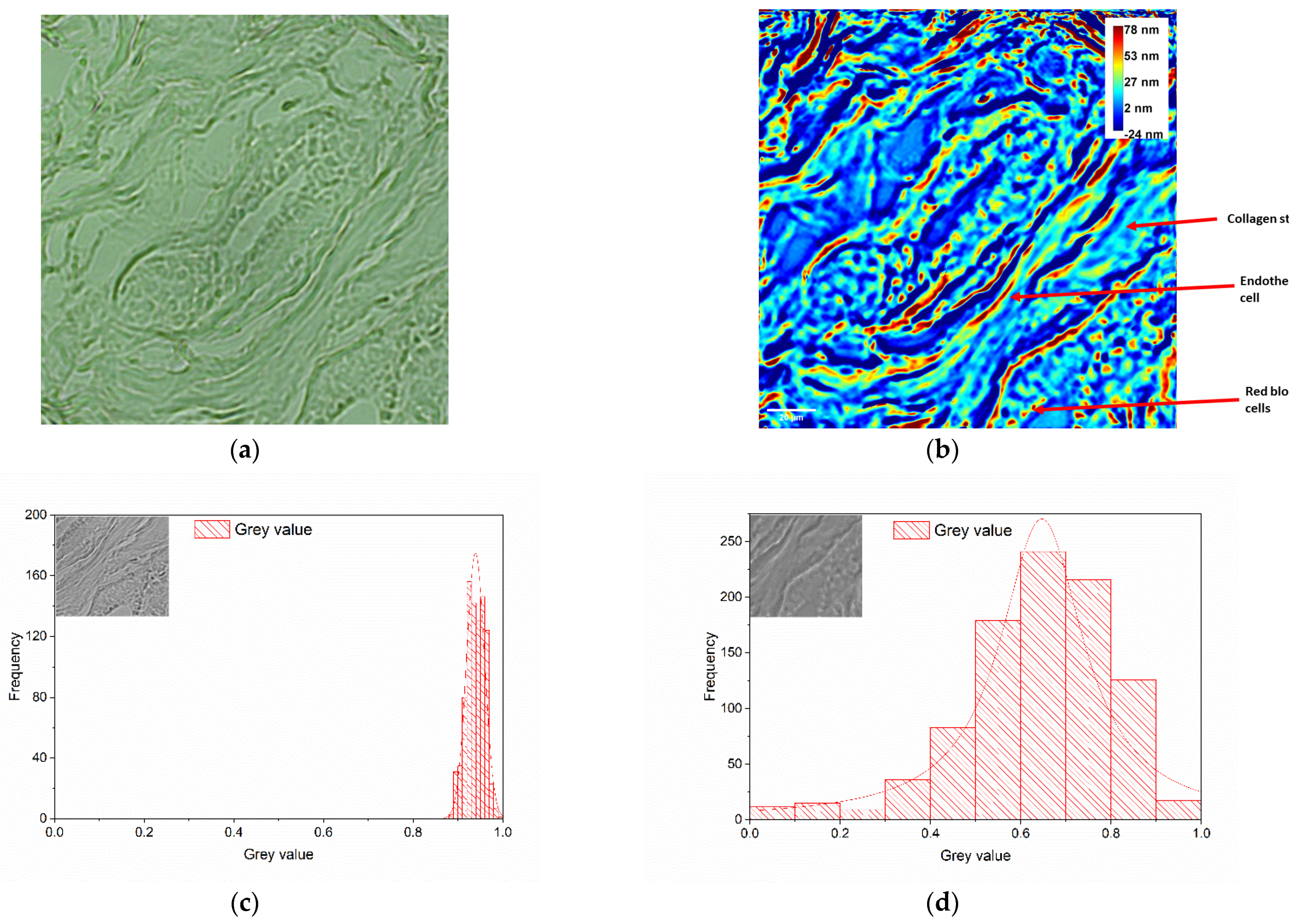
4.1. Breast Tissues Comparative Analysis
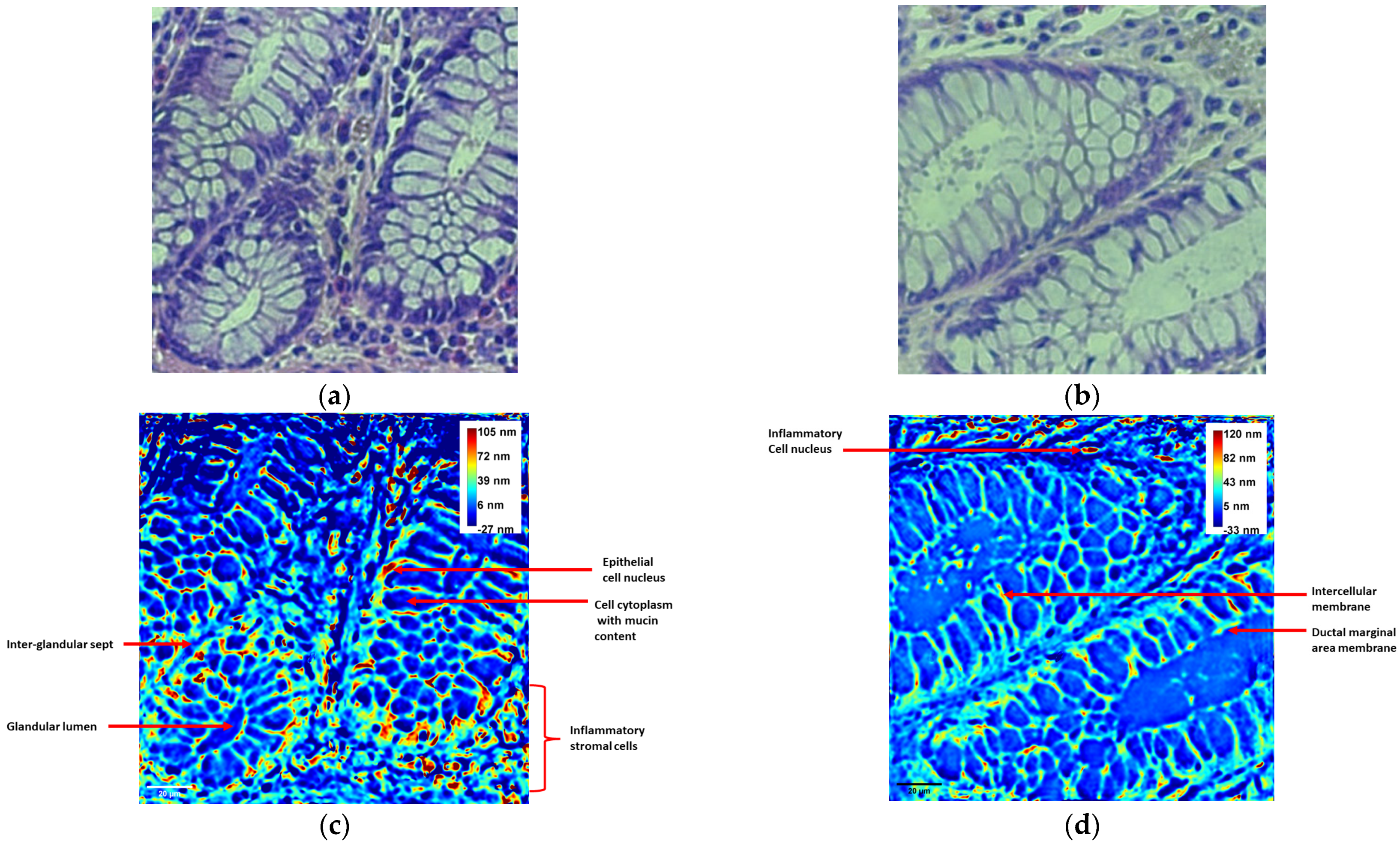
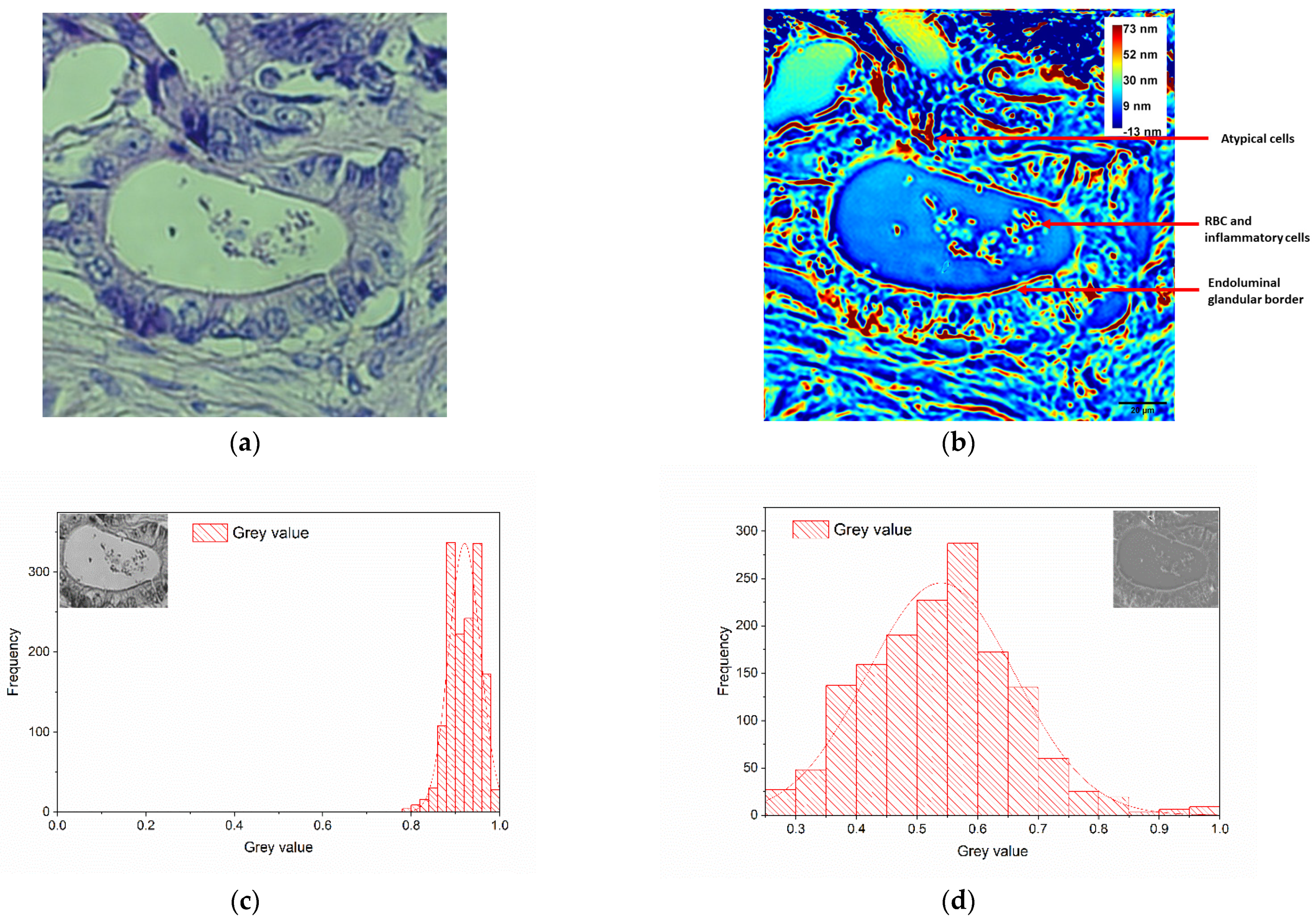
4.2. Colon Tissues Comparative Analysis
5. Conclusions and Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Today. Available online: https://gco.iarc.who.int/today/ (accessed on 23 April 2024).
- Creath, K. V Phase-Measurement Interferometry Techniques. In Progress in Optics; Elsevier: Amsterdam, The Netherlands, 1988; pp. 349–393. [Google Scholar] [CrossRef]
- Ferraro, P.; Miccio, L.; Grilli, S.; Paturzo, M.; De Nicola, S.; Finizio, A.; Osellame, R.; Laporta, P. Quantitative Phase Microscopy of microstructures with extended measurement range and correction of chromatic aberrations by multiwavelength digital holography. Opt. Express 2007, 15, 14591. [Google Scholar] [CrossRef] [PubMed]
- Miccio, L.; Grilli, S.; Paturzo, M.; Finizio, A.; Caprio, G.D.; Coppola, G.; Ferraro, P.; Puglisi, R.; Balduzzi, D.; Galli, A. Quantitative Phase Contrast in Holographic Microscopy Through the Numerical Manipulation of the Retrieved Wavefronts. In Coherent Light Microscopy; Ferraro, P., Wax, A., Zalevsky, Z., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 61–85. [Google Scholar] [CrossRef]
- Bhaduri, B.; Edwards, C.; Pham, H.; Zhou, R.; Nguyen, T.H.; Goddard, L.L.; Popescu, G. Diffraction phase microscopy: Principles and applications in materials and life sciences. Adv. Opt. Photonics 2014, 6, 57–119. [Google Scholar] [CrossRef]
- Karandikar, S.H.; Zhang, C.; Meiyappan, A.; Barman, I.; Finck, C.; Srivastava, P.K.; Pandey, R. Reagent-Free and Rapid Assessment of T Cell Activation State Using Diffraction Phase Microscopy and Deep Learning. Anal. Chem. 2019, 91, 3405–3411. [Google Scholar] [CrossRef] [PubMed]
- Shan, M.; Kandel, M.E.; Majeed, H.; Nastasa, V.; Popescu, G. White-light diffraction phase microscopy at doubled space-bandwidth product. Opt. Express 2016, 24, 29033–29039. [Google Scholar] [CrossRef]
- Bhaduri, B.; Pham, H.; Mir, M.; Popescu, G. Diffraction phase microscopy with white light. Opt. Lett. 2012, 37, 1094–1096. [Google Scholar] [CrossRef]
- Kim, T.; Zhou, R.; Mir, M.; Babacan, S.D.; Carney, P.S.; Goddard, L.L.; Popescu, G. White-light diffraction tomography of unlabelled live cells. Nat. Photonics 2014, 8, 256–263. [Google Scholar] [CrossRef]
- Kocahan, Ö.; Çelebioğlu, N.; Uyanık, M. White light diffraction phase microscopy for imaging of red blood cells for different storage times. Phys. Scr. 2024, 99, 055033. [Google Scholar] [CrossRef]
- Pandiyan, V.P.; John, R. Imaging cell division in E-coli using white light diffraction phase microscopy. In Proceedings of the 2015 Workshop on Recent Advances in Photonics (WRAP), Bangalore, India, 16–17 December 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 1–4. [Google Scholar] [CrossRef]
- Ünal, A.; Kocahan, Ö.; Altunan, B.; Aksoy Gündoğdu, A.; Uyanık, M.; Özder, S. Quantitative phase imaging of erythrocyte in epilepsy patients. Microsc. Res. Tech. 2021, 84, 1172–1180. [Google Scholar] [CrossRef]
- Ikeda, T.; Popescu, G.; Dasari, R.R.; Feld, M.S. Hilbert phase microscopy for investigating fast dynamics in transparent systems. Opt. Lett. 2005, 30, 1165–1167. [Google Scholar] [CrossRef]
- Nastasa, V.; Smarandache, A.; Pirvulescu, R.A.; Andrei, I.R.; Simion, G.; Popescu, G.; Pascu, M.L. Eye Tumor Tissues Imaging with White Llight Diffraction Phase Microscopy. Rom. Rep. Phys. 2022, 74, 604. [Google Scholar]
- Majeed, H.; Kandel, M.E.; Han, K.; Luo, Z.; Macias, V.; Tangella, K.; Balla, A.; Popescu, G. Breast cancer diagnosis using spatial light interference microscopy. J. Biomed. Opt. 2015, 20, 111210. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Tangella, K.; Balla, A.; Popescu, G. Tissue refractive index as marker of disease. J. Biomed. Opt. 2011, 16, 116017. [Google Scholar] [CrossRef] [PubMed]
- Bhaduri, B.; Tangella, K.; Popescu, G. Fourier phase microscopy with white light. Biomed. Opt. Express 2013, 4, 1434–1441. [Google Scholar] [CrossRef]
- Uttam, S.; Pham, H.V.; LaFace, J.; Leibowitz, B.; Yu, J.; Brand, R.E.; Hartman, D.J.; Liu, Y. Early prediction of cancer progression by depth-resolved nanoscale maps of nuclear architecture from unstained tissue specimens. Cancer Res. 2015, 75, 4718–4727. [Google Scholar] [CrossRef] [PubMed]
- Bokemeyer, A.; Tepasse, P.R.; Quill, L.; Lenz, P.; Rijcken, E.; Vieth, M.; Ding, N.; Ketelhut, S.; Rieder, F.; Kemper, B.; et al. Quantitative Phase Imaging Using Digital Holographic Microscopy Reliably Assesses Morphology and Reflects Elastic Properties of Fibrotic Intestinal Tissue. Sci. Rep. 2019, 9, 19388. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.; Cho, H.; Lee, S.Y.; Choi, G.; Kim, G.; Min, H.; Park, Y. Quantitative Phase Imaging and Artificial Intelligence: A Review. IEEE J. Sel. Top. Quantum Electron. 2019, 25, 6800914. [Google Scholar] [CrossRef]
- Allen, D.C.; Cameron, R.I. Histopathology Specimens: Clinical, Pathological and Laboratory Aspects; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Pham, H.; Ding, H.; do, M.; Patel, S.; Popescu, G. Off-axis quantitative phase imaging processing using CUDA: Toward real-time applications. Biomed. Opt. Express 2011, 2, 1781–1793. [Google Scholar] [CrossRef]
- Pham, H.V.; Edwards, C.; Goddard, L.; Popescu, G. Fast phase reconstruction in white light diffraction phase microscopy. Appl. Opt. 2013, 52, A97–A101. [Google Scholar] [CrossRef]
- Masters, B. Superresolution Optical Microscopy: The Quest for Enhanced Resolution and Contrast; Springer International Publishing: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- WMA—The World Medical Association-WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. 2021. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 1 February 2021).
- Hu, C.; Sam, R.; Shan, M.; Nastasa, V.; Wang, M.; Kim, T.; Gillette, M.; Sengupta, P.; Popescu, G. Optical excitation and detection of neuronal activity. J. Biophotonics 2018, 12, e201800269. [Google Scholar] [CrossRef]
- Popescu, G. Quantitative Phase Imaging of Cells and Tissues; McGraw-Hill: New York, NY, USA, 2011. [Google Scholar]
- Bredfeldt, J.S.; Liu, Y.; Conklin, M.W.; Keely, P.J.; Mackie, T.R.; Eliceiri, K.W. Automated quantification of aligned collagen for human breast carcinoma prognosis. J. Pathol. Inform. 2014, 5, 28. [Google Scholar] [CrossRef]
- Hamperl, H. Early Invasive Growth as Seen in Uterine Cancer and the Role of the Basal Membrane. In Mechanisms of Invasion in Cancer; Denoix, P., Ed.; Springer: Berlin/Heidelberg, Germany, 1967; pp. 17–25. [Google Scholar] [CrossRef]
- Li, H.; Bera, K.; Toro, P.; Fu, P.; Zhang, Z.; Lu, C.; Feldman, M.; Ganesan, S.; Goldstein, L.J.; Davidson, N.E.; et al. Collagen fiber orientation disorder from H&E images is prognostic for early stage breast cancer: Clinical trial validation. npj Breast Cancer 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Rahman, F.; Rao, N.N.; Tippu, S.R.; Patil, S.; Agarwal, S.; Srivastava, S. The expression of laminin-5 in severe dysplasia/carcinoma in situ and early invasive squamous cell carcinoma: An immunohistochemical study. Minerva Stomatol. 2013, 62, 139–146. [Google Scholar] [PubMed]
- d’Ardenne, A.J. Use of basement membrane markers in tumour diagnosis. J. Clin. Pathol. 1989, 42, 449–457. [Google Scholar] [CrossRef]
- Wang, Z.; Ding, H.; Popescu, G. Scattering-phase theorem. Opt. Lett. 2011, 36, 1215–1217. [Google Scholar] [CrossRef]
- Park, Y.; Depeursinge, C.; Popescu, G. Quantitative phase imaging in biomedicine. Nat. Photonics 2018, 12, 578–589. [Google Scholar] [CrossRef]
- Born, M.; Wolf, E. Chapter X—Interference and Diffraction with Partially Coherent Light. In Principles of Optics, 6th ed.; Born, M., Wolf, E., Eds.; Elsevier: Pergamon, Turkey, 1980; pp. 491–555. [Google Scholar] [CrossRef]
- Memmolo, P.; Bianco, V.; Carcagnì, P.; Junior, A.G.d.S.; Goncalves, L.M.G.; Merola, F.; Paturzo, M.; Distante, C.; Ferraro, P. Identification and classification of biological micro-organisms by holographic learning. In Proceedings of the Optical Methods for Inspection, Characterization, and Imaging of Biomaterials IV, SPIE 2019, Munich, Germany, 24–27 June 2019; pp. 51–56. [Google Scholar] [CrossRef]
- Jones, V.A.; Patel, P.M.; Gibson, F.T.; Cordova, A.; Amber, K.T. The Role of Collagen XVII in Cancer: Squamous Cell Carcinoma and Beyond. Front. Oncol. 2020, 10, 352. [Google Scholar] [CrossRef]
- Le, C.C.; Bennasroune, A.; Langlois, B.; Salesse, S.; Boulagnon-Rombi, C.; Morjani, H.; Dedieu, S.; Appert-Collin, A. Functional Interplay Between Collagen Network and Cell Behavior Within Tumor Microenvironment in Colorectal Cancer. Front. Oncol. 2020, 10, 527. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Xu, H.; Wang, W.; Li, S.; Li, H.; Li, T.; Zhang, W.; Yu, X.; Liu, L. The role of collagen in cancer: From bench to bedside. J. Transl. Med. 2019, 17, 309. [Google Scholar] [CrossRef] [PubMed]
- Sakakura, M.; Macias, V.; Kajdacsy-Balla, A.; Popescu, G. Label-free imaging of collagen fibers in tissue slices using phase imaging with computational specificity. bioRxiv 2021. [Google Scholar] [CrossRef]
- Konda, P.C.; Konda, P.C.; Loetgering, L.; Loetgering, L.; Loetgering, L.; Zhou, K.C.; Zhou, K.C.; Xu, S.; Harvey, A.R.; Horstmeyer, R. Fourier ptychography: Current applications and future promises. Opt. Express 2020, 28, 9603–9630. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smarandache, A.; Pirvulescu, R.A.; Andrei, I.-R.; Dinache, A.; Romanitan, M.O.; Branisteanu, D.C.; Zemba, M.; Anton, N.; Pascu, M.-L.; Nastasa, V. White Light Diffraction Phase Microscopy in Imaging of Breast and Colon Tissues. Diagnostics 2024, 14, 1966. https://doi.org/10.3390/diagnostics14171966
Smarandache A, Pirvulescu RA, Andrei I-R, Dinache A, Romanitan MO, Branisteanu DC, Zemba M, Anton N, Pascu M-L, Nastasa V. White Light Diffraction Phase Microscopy in Imaging of Breast and Colon Tissues. Diagnostics. 2024; 14(17):1966. https://doi.org/10.3390/diagnostics14171966
Chicago/Turabian StyleSmarandache, Adriana, Ruxandra A. Pirvulescu, Ionut-Relu Andrei, Andra Dinache, Mihaela Oana Romanitan, Daniel Constantin Branisteanu, Mihail Zemba, Nicoleta Anton, Mihail-Lucian Pascu, and Viorel Nastasa. 2024. "White Light Diffraction Phase Microscopy in Imaging of Breast and Colon Tissues" Diagnostics 14, no. 17: 1966. https://doi.org/10.3390/diagnostics14171966
APA StyleSmarandache, A., Pirvulescu, R. A., Andrei, I.-R., Dinache, A., Romanitan, M. O., Branisteanu, D. C., Zemba, M., Anton, N., Pascu, M.-L., & Nastasa, V. (2024). White Light Diffraction Phase Microscopy in Imaging of Breast and Colon Tissues. Diagnostics, 14(17), 1966. https://doi.org/10.3390/diagnostics14171966