
Oral Health-Related Quality of Life in Temporomandibular Disorder Patients and Healthy Subjects—A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy
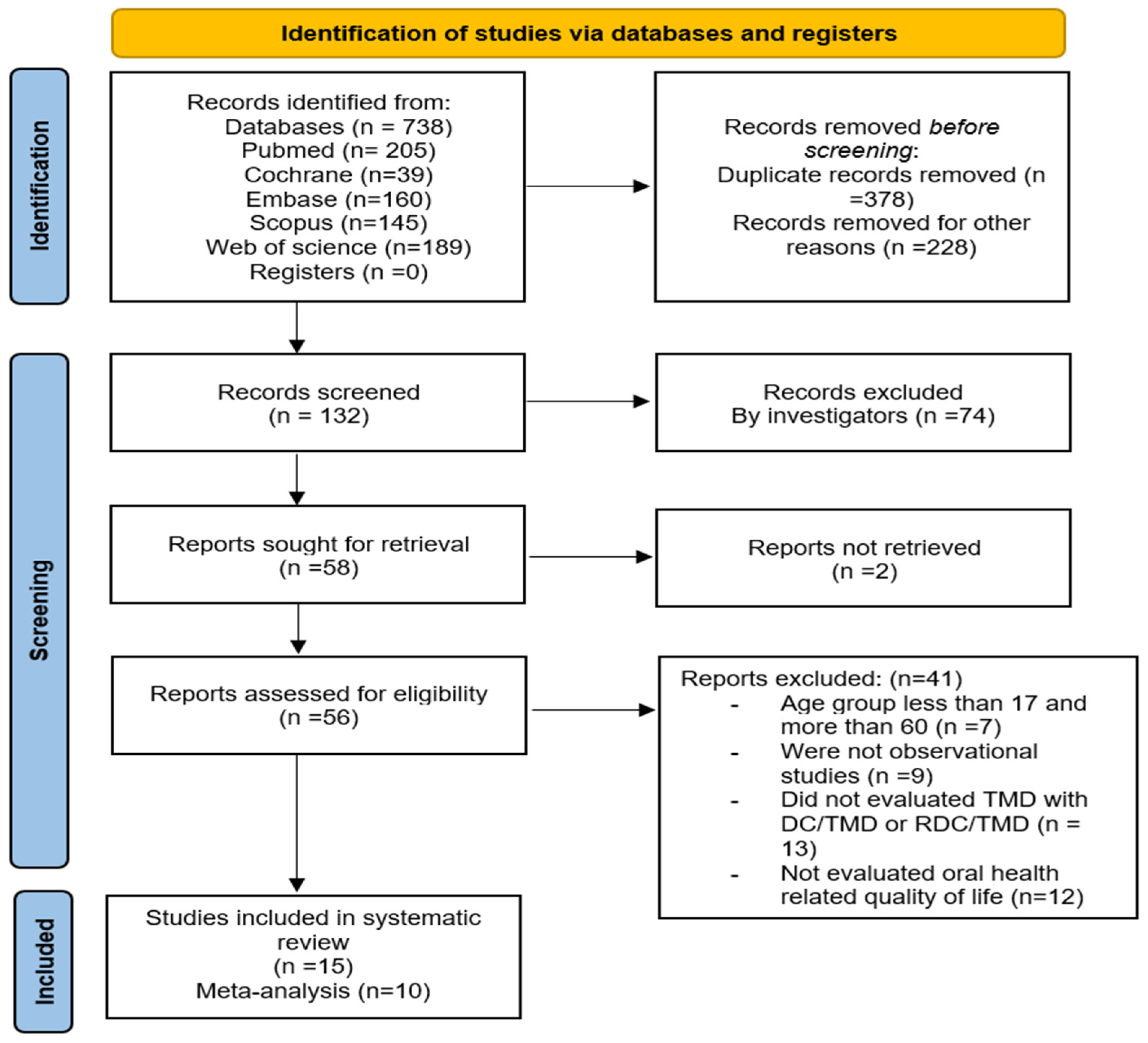
2.4. Data Extraction and Study Selection
2.5. Risk of Bias and Data Analysis
2.6. Certainty of Evidence (GRADE Analysis)
3. Results
3.1. Characteristics of Included Studies
3.2. Oral Health-Related Quality of Life
3.3. Result from Meta-Analysis
3.4. Quality of Included Studies
3.5. GRADE Certainty of Evidence
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Leeuw, R.; Klasser, G. Orofacial pain: Guidelines for assessment, diagnosis, and management. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 171. [Google Scholar] [CrossRef]
- Blanco-Aguilera, A.; Blanco-Hungría, A.; Biedma-Velázquez, L.; Serrano-Del-Rosal, R.; González-López, L.; Blanco-Aguilera, E.; Segura-Saint-Gerons, R. Application of an oral health-related quality of life questionnaire in primary care patients with orofacial pain and temporomandibular disorders. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e127–e135. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Yap, A.U.; Lei, J.; Zhang, M.J.; Fu, K.Y. Oral health-related quality of life of patients with acute and chronic temporomandibular disorder diagnostic subtypes. J. Am. Dent. Assoc. 2022, 153, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Hanna, K.; Nair, R.; Amarasena, N.; Armfield, J.M.; Brennan, D.S. Temporomandibular dysfunction experience is associated with oral health-related quality of life: An Australian national study. BMC Oral Health 2021, 21, 432. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Shearer, D.M.; MacLeod, R.J.; Thomson, W.M. Oral-health-related quality of life: An overview for the general dental practitioner. N. Z. Dent. J. 2007, 103, 82–87. [Google Scholar] [PubMed]
- McGrath, C.; Bedi, R. An evaluation of a new measure of oral health related quality of life--OHQoL-UK(W). Community Dent. Health 2001, 18, 138–143. [Google Scholar] [PubMed]
- Namvar, M.A.; Moslemkhani, C.; Mansoori, K.; Dadashi, M. The Relationship between Depression and Anxiety with Temporomandibular Disorder Symptoms in Dental Students. Maedica J. Clin. Med. 2021, 16, 590. [Google Scholar] [CrossRef]
- Almoznino, G.; Zini, A.; Zakuto, A.; Sharav, Y.; Haviv, Y.; Avraham, H.; Chweidan, H.; Noam, Y.; Benoliel, R. Oral Health-Related Quality of Life in Patients with Temporomandibular Disorders. J. Oral Facial Pain. Headache 2015, 29, 231–241. [Google Scholar] [CrossRef]
- Dahlström, L.; Carlsson, G.E. Temporomandibular disorders and oral health-related quality of life. A systematic review. Acta Odontol. Scand. 2010, 68, 80–85. [Google Scholar] [CrossRef]
- Karaman, A.; Sapan, Z. Evaluation of temporomandibular disorders, quality of life, and oral habits among dentistry students. Cranio 2023, 41, 316–322. [Google Scholar] [CrossRef]
- Oberoi, S.S.; Hiremath, S.S.; Yashoda, R.; Marya, C.; Rekhi, A. Prevalence of Various Orofacial Pain Symptoms and Their Overall Impact on Quality of Life in a Tertiary Care Hospital in India. J. Maxillofac. Oral Surg. 2014, 13, 533–538. [Google Scholar] [CrossRef]
- Potewiratnanond, P.; Limpuangthip, N.; Karunanon, V.; Buritep, A.; Thawai, A. Factors associated with the oral health-related quality of life of patients with temporomandibular disorder at the final follow-up visit: A cross-sectional study. BDJ Open 2022, 8, 30. [Google Scholar] [CrossRef]
- Turcio, K.H.; Neto, C.M.; Pirovani, B.O.; Dos Santos, D.M.; Guiotti, A.M.; Bertoz, A.M.; Brandini, D.A. Relationship of bruxism with oral health-related quality of life and facial muscle pain in dentate individuals. J. Clin. Exp. Dent. 2022, 14, e385–e389. [Google Scholar] [CrossRef]
- Qamar, Z.; Alghamdi, A.M.S.; Haydarah, N.K.B.; Balateef, A.A.; Alamoudi, A.A.; Abumismar, M.A.; Shivakumar, S.; Cicciu, M.; Minervini, G. Impact of temporomandibular disorders on oral health-related quality of life: A systematic review and meta-analysis. J. Oral Rehabil. 2023, 50, 706–714. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Groupdagger. J. Oral Facial Pain. Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 2019, ED000142. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Margulis, A.V.; Pladevall, M.; Riera-Guardia, N.; Varas-Lorenzo, C.; Hazell, L.; Berkman, N.D.; Viswanathan, M.; Perez-Gutthann, S. Quality assessment of observational studies in a drug-safety systematic review, comparison of two tools: The Newcastle–Ottawa scale and the RTI item bank. Clin. Epidemiol. 2014, 6, 359–368. [Google Scholar] [CrossRef]
- Cook, D.A.; Reed, D.A. Appraising the quality of medical education research methods: The medical education research study quality instrument and the Newcastle–Ottawa scale-education. Acad. Med. 2015, 90, 1067–1076. [Google Scholar] [CrossRef] [PubMed]
- Huguet, A.; Hayden, J.A.; Stinson, J.; McGrath, P.J.; Chambers, C.T.; Tougas, M.E.; Wozney, L. Judging the quality of evidence in reviews of prognostic factor research: Adapting the GRADE framework. Syst. Rev. 2013, 2, 71. [Google Scholar] [CrossRef]
- Bayat, M.; Abbasi, A.J.; Noorbala, A.A.; Mohebbi, S.Z.; Moharrami, M.; Yekaninejad, M.S. Oral health-related quality of life in patients with temporomandibular disorders: A case-control study considering psychological aspects. Int. J. Dent. Hyg. 2018, 16, 165–170. [Google Scholar] [CrossRef]
- Celik, O.; Secgin, C.K.; Gulashi, A.; Yuzugullu, B. Oral Health-Related Quality of Life in Patients with Temporomandibular Disorders and Effect of Anxiety: A Retrospective Case-Control Study. Int. J. Prosthodont. 2023, 36, 148–154. [Google Scholar] [CrossRef]
- Filho, J.C.; Vedovello, S.A.S.; Venezian, G.C.; Vedovello Filho, M.; Degan, V.V. Women’s oral health-related quality of life as a risk factor for TMD symptoms. A case-control study. Cranio 2023, 41, 139–143. [Google Scholar] [CrossRef]
- Rener-Sitar, K.; Celebic, A.; Mehulic, K.; Petricevic, N. Factors Related to Oral Health Related Quality of Life in TMD Patients. Coll. Antropol. 2013, 37, 407–413. [Google Scholar]
- Yap, A.U.; Cao, Y.; Zhang, M.J.; Lei, J.; Fu, K.Y. Comparison of emotional disturbance, sleep, and life quality in adult patients with painful temporomandibular disorders of different origins. Clin. Oral Investig. 2021, 25, 4097–4105. [Google Scholar] [CrossRef]
- Yap, A.U.; Tan, S.H.X.; Marpaung, C. Temporomandibular disorder symptoms in young adults: Three-dimensional impact on oral health-related quality of life. J. Oral Rehabil. 2022, 49, 769–777. [Google Scholar] [CrossRef]
- Yildirim, G.; Erol, F.; Guven, M.C.; Sakar, O. Evaluation of the effects of bruxism on oral health-related quality of life in adults. Cranio 2023, 41, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Balik, A.; Peker, K.; Ozdemir-Karatas, M. Comparisons of measures that evaluate oral and general health quality of life in patients with temporomandibular disorder and chronic pain. Cranio 2021, 39, 310–320. [Google Scholar] [CrossRef]
- Gui, M.S.; Pimentel, M.J.; Gama, M.C.d.S.; Ambrosano, G.M.B.; Barbosa, C.M.R. Quality of life in temporomandibular disorder patients with localized and widespread pain. Braz. J. Oral Sci. 2014, 13, 193–197. [Google Scholar] [CrossRef]
- Lemos, G.A.; Paulino, M.R.; Forte, F.D.S.; Beltrão, R.T.S.; Batista, A.U.D. Influence of temporomandibular disorder presence and severity on oral health-related quality of life. Rev. D’or 2015, 16, 10–14. [Google Scholar] [CrossRef]
- Pawar, P.; Puranik, M.; Shanbhag, N. Relationship between Oral Health Status and Oral Health-Related Quality of Life among Patients with Temporomandibular Disorders in Bengaluru City: A Cross-Sectional Comparative Study. J. Indian Assoc. Public Health Dent. 2022, 20, 287–292. [Google Scholar] [CrossRef]
- Resende CMBMd Alves, A.C.d.M.; Coelho, L.T.; Alchieri, J.C.; Roncalli, Â.G.; Barbosa, G.A.S. Quality of life and general health in patients with temporomandibular disorders. Braz. Oral Res. 2013, 27, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Su, N.; Liu, Y.; Yang, X.; Shen, J.; Wang, H. Correlation between oral health-related quality of life and clinical dysfunction index in patients with temporomandibular joint osteoarthritis. J. Oral Sci. 2016, 58, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.; Cao, Y.; Zhang, M.J.; Lei, J.; Fu, K.Y. Number and type of temporomandibular disorder symptoms: Their associations with psychological distress and oral health-related quality of life. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, 288–296. [Google Scholar] [CrossRef]
- Yap, A.U.; Cao, Y.; Zhang, M.J.; Lei, J.; Fu, K.Y. Age-related differences in diagnostic categories, psychological states and oral health-related quality of life of adult temporomandibular disorder patients. J. Oral Rehabil. 2021, 48, 361–368. [Google Scholar]
- Kroese, J.M.; Volgenant, C.M.C.; van Schaardenburg, D.; van Boheemen, L.; van Selms, M.K.A.; Visscher, C.M.; Crielaard, W.; Loos, B.G.; Lobbezoo, F. Oral health-related quality of life in patients with early rheumatoid arthritis is associated with periodontal inflammation and painful temporomandibular disorders: A cross-sectional study. Clin. Oral Investig. 2022, 26, 555–563. [Google Scholar] [CrossRef]
- Aranha, R.L.d.B.; Martins, R.d.C.; de Aguilar, D.R.; Moreno-Drada, J.A.; Sohn, W.; Martins, C.d.C.; de Abreu, M.H.N.G. Association between Stress at Work and Temporomandibular Disorders: A Systematic Review. BioMed Res. Int. 2021, 2021, 2055513. [Google Scholar] [CrossRef] [PubMed]
- Bieganska-Banas, J.M.; Gierowski, J.K.; Pihut, M.; Ferendiuk, E. Oral health-related quality of life and cognitive functioning in myofascial temporomandibular disorders pain. Arch. Psychiatry Psychother. 2019, 21, 45–58. [Google Scholar] [CrossRef]
- Rahimi, H.; Twilt, M.; Herlin, T.; Spiegel, L.; Pedersen, T.K.; Küseler, A.; Stoustrup, P. Orofacial symptoms and oral health-related quality of life in juvenile idiopathic arthritis: A two-year prospective observational study. Pediatr. Rheumatol. Online J. 2018, 16, 47. [Google Scholar] [CrossRef] [PubMed]
- Su, N.; Wang, H.; van Wijk, A.J.; Visscher, C.M.; Lobbezoo, F.; Shi, Z.; van der Heijden, G. Prediction Models for Oral Health-Related Quality of Life in Patients with Temporomandibular Joint Osteoarthritis 1 and 6 Months After Arthrocentesis with Hyaluronic Acid Injections. J. Oral Facial Pain. Headache 2019, 33, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Oghli, I.; List, T.; Su, N.; Häggman-Henrikson, B. The impact of oro-facial pain conditions on oral health-related quality of life: A systematic review. J. Oral Rehabil. 2020, 47, 1052–1064. [Google Scholar] [CrossRef]
- Tanner, J.; Teerijoki-Oksa, T.; Kautiainen, H.; Vartiainen, P.; Kalso, E.; Forssell, H. Health-related quality of life in patients with chronic orofacial pain compared with other chronic pain patients. Clin. Exp. Dent. Res. 2022, 8, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.L.; Yap, A.U. Outcomes of therapeutic TMD interventions on oral health related quality of life: A qualitative systematic review. Quintessence Int. 2018, 49, 487–496. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Databases Searched | MesH Terms | Articles Found |
|---|---|---|
| PubMed | “Temporomandibular disorders [MeSH Terms] OR Temporomandibular Joint Disorders OR TMD” [MesH Terms] OR “temporomandibular joint disorder” [All Fields] OR “temporomandibular joint disease” [All Fields] OR “temporomandibular joint diseases” [All Fields] OR “temporomandibular joint dysfunction syndrome” [MeSH Terms] OR “temporomandibular joint dysfunction syndrome” [All Fields] OR “temporomandibular joint syndromes” [All Fields] OR “tmj disease” [All Fields] OR “tmd” [All Fields] OR “tmj” [All Fields] OR “tmjd” [All Fields] OR “tmj disorders” [All Fields] OR “tmj disorder” [All Fields] OR “tmj diseases” [All Fields] AND “orofacial pain” [Mesh term] OR “craniofacial pain [MesH term]” AND “Oral health [MeSH Terms] OR Oral Health OR Oral Health-Related Quality of Life [All Fields] OR OHRQoL [All Fields] OR Oral Health-Related Quality of Life [Mesh Terms] OR OHRQoL [MesH terms] | Initial search 205 Abstract and Title 26 |
| Scopus | TITLE-ABS-KEY (temporomandibular disorders OR temporomandibular joint disorders OR TMD) AND (oral health-related quality of life OR oral health OR OHRQoL) AND (orofacial pain OR craniofacial pain) | Initial search 145 |
| Web of science | (TS = (“temporomandibular joint disorder” OR “temporomandibular joint disorders” OR “temporomandibular dysfunctions” OR “temporomandibular joint syndrome” OR “tmj disease” OR tmjd OR “tmj disorders” OR “tmj disorder” OR “tmj diseases” OR “temporomandibular joint dysfunction syndrome”) AND TI = (“oral health related quality of life” OR “OHRQoL”)) AND TI = (“orofacial pain” OR “craniofacial pain”) AND DOCUMENT TYPES: (Article) | Initial search 189 |
| EMBASE | #1 = (‘temporomandibular joint disorders’:ta,ab OR ‘tmj disorder’:ta,ab OR ‘temporomandibular joint disease’:ta,ab ‘temporomandibular joint dysfunction syndrome’:ta,ab) #2 = (‘oral health related quality of life’:ta,ab OR ‘OHRQoL’:ta,ab) #3 = (‘orofacial Pain’ OR craniaofacial pain’) AND #4 = ([article]/lim) #5 = #1 AND #2 AND #3 AND #4 | Total articles: 160 |
| Cochrane | (TS = (“temporomandibular joint disorder” OR “temporomandibular joint disorders” OR “temporomandibular dysfunctions” OR “temporomandibular joint syndrome” OR “tmj disease” OR tmjd OR “tmj disorders” OR “tmj disorder” OR “tmj diseases” OR “temporomandibular joint dysfunction syndrome”) AND TI = (“oral health related quality of life” OR “OHRQoL”)) AND TI = (“orofacial pain” OR “craniofacial pain”) AND DOCUMENT TYPES: (Article) | Total articles:39 Abstract and title: 2 |
| Study No. | Author/Year/Country | Study Design | Number of Participants (Cases and Control) | Age (AR) and Gender | Case Selection Method | Control Selection Method | Diagnostic Criteria for TMD | Measurement of Oral Heath-Related Quality of Life | Method for Data Collection | Results/Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Celik et al., 2022 [24] Turkey | Case-Control Study | n = 200 (Case = 150; Control = 50) | AR = 18–60 years (F = 121; M = 79) | Patient seeking treatment for TMD | Not specified | DC/TMD for all cases | OHIP-14 | Questionnaire | OHIP score was higher in patients with disc displacement and TMD-related pain compared to healthy controls |
| 2 | Pawar et al., 2022 [33] India | Cross-sectional comparitive study | n = 320 (Cases = 160; Control = 160) | AR = 18–60 years (F = 168; M = 152) | Patient seeking treatment for TMD (divided in three groups; G1 = myofacial pain, G2 = disc displacement, G3 = osteoarthritis | Patient seeking dental treatment for other reasons | RDC/TMD axis I and II for all the cases | OHIP-14 | Questionnaire | Poor OHRQoL was reported in TMD patients compared to healthy controls |
| 3 | Ujin Yap et al., 2021 [28] China | Case-Control Study | n = 961 (Cases = 816; Control = 147) | AR = 18–40 years (F = 761; M = 200) | Not specified | Not specified | DC/TMD-SQ axis I for all the cases | OHIP-14 | Questionnaire | OHRQoL is affected by different types of TMD symptoms. Individuals having more and pain-related TMD symptoms with/without intra-articular features generally had greater OHRQoL impairments. |
| 4 | Ujin Yap et al., 2021 [36] China | Case-Control Study | n = 961 (Cases = 845; Control = 116) | AR = 18–40 years (F = 761; M = 200) | Patient visted oral and maxillofacial clinics | Patients visited in prosthetic dental clinics | DC/TMD axis II for all the cases | OHIP-14 | Questionnaire | Correlations between TMD severity OHRQoL were moderately strong to strong (rs = 0.42–0. 72) |
| 5 | Filho et al., 2020 [25] Brazil | Case-Control Study | n = 765 (Cases = 153; Control = 612 | AR = 18–25 years (F = 765) | Not specified | Not specified | RDC/TMD axis II for all the cases | OHIP-14 | Questionnaire | Women with negative OHRQoL reports symptoms of TMD |
| 6 | Yıldırım et al., 2020 [29] Turkey | Case-Control Study | n = 315 (Cases = 172; Controls = 143) | AR = 18–60 years(F = 192; M = 123) | Not specified | Not specified | RDC/TMD axis I and II for all the cases | OHIP-14 questionnaire | Questionnaire | Bruxers with TMD had poorer OHRQoL than those without TMD |
| 7 | Bayat et al., 2017 [23] Iran | Case-Control Study | n = 150 (Cases = 75;control = 75) | AR = 30–50 years (F = 119; M = 31) | Patient seeking treatment at clinic | Patients coming for follow-up of any dental treatment | RDC/TMD axis I and II for all the cases | OHIP-14 | Interview | The TMD group had a worse quality of life than controls. The prevalence and severity of OHIP was 6 and 2 times higher, respectively, in the TMD group. |
| 8 | Balik et al., 2017 [30] Turkey | Cross-sectional study | n = 104 (Case and Control = not specified) | AR = 32–59 years(F = 64; M = 40) | Not specified | Not specified | RDC/TMD axis I and II for all the cases | OHIP-14 | Questionnaire | OHIP score was higher in patients with disc displacement and TMD-related pain |
| 9 | Su et al., 2016 [35] China | Cross-sectional | n = 541 (Case and Control = not specified) | AR = 25–48 years (M = 134; F = 407) | Patient seeking treatment at clinic | Not specified | RDC/TMD axis I for all the cases | OHIP-14 | Interview | OHIP score was worst in patients with muscular pain. |
| 10 | Almoznino et al. 2015, [9] Israel | Case-Control Study | n = 387 (Cases = 187 and Controls = 200 | AR = 20–30 years (F = 111; M = 76) | Patient seeking treatment at clinic | Patient seeking treatment at clinic | DC/TMD and RDC/ TMDaxis I in cases | OHIP-14 | Interview | TMD group showed statistical differences for the OHIP as compared to controls. |
| 11 | Lemos et al., 2015 [32] Brazil | Cross-sectional | n = 135 (Case and Control = not specified) | AR = 18–25 years (F = 77; M = 58) | Dental students | Not specified | RDC/TMD axes I | OHIP-14 | Questionnaire | Severity of TMD impaired the oral health-related quality of life |
| 12 | Blanco-Aguilera et al. 2014, [2] Spain | Cross-sectional | n = 407 (Case and Control = not specified) | AR = 18–60 years (F = 365; M = 42) | Sample of the population of the Public Health System | Not specified | RDC/TMD (did not report axis) | OHIP-14 | Interview | OHIP showed a significant and positive association in patients with painful TMD |
| 13 | Gui et al., 2014 [31] Brazil | Cross-sectional | n = 116 (Case = 76 and control = 40) | AR = 25–50 years (F = 116) | Sample from hospital records | Sample from hospital records | RDC/TMD for all the cases | OHIP-14 | Questionnaire | Quality of life is significantly impared by widespread TMD pain compared to healthy control |
| 14 | Rener-Sitar et al. 2014, [26] Slovenia | Case-Control Study | n = 481 (Cases = 81 and Control = 400) | AR = 18–60 years (F = 365; M = 115) | Patients seeking treatment at the dental clinic | Random patients without TMD taking treatment at hospital | RDC/TMD axis I in all the cases | OHIP-49 | Interview | TMD patients are highly associated with a lower OHRQoL. |
| 15 | Resende et al. 2013, [34] Brazil | Cross-Sectional | n = 43 (Cases = 43 divided in 3 groups G1 = 30; G2 = 9; G3 = 4) | AR = 30–45 years (F = 32; M = 11) | Patients seeking treatment at the dental clinic | Patients seeking treatment at the dental clinic | RDC-TMD axis I for cases | WHOQOL-BREF | Interview | Impiared oral health-related quality of life is recorded in patient with myofacial pain associated with TMD. |
| Studies | Celik et al., 2022 [24] Turkey | Ujin Yap et al., 2021 [28] China | Ujin Yap et al., 2021 [36] China | Filho et al., 2020 [25] Brazil | Yıldırım et al., 2020 [29] Turkey | Bayat et al., 2017 [23] Iran | Almoznino et al., 2015 [9] Israel | Rener-Sitar et al., 2014 [26] Slovenia | |
|---|---|---|---|---|---|---|---|---|---|
| Selection | Case definition adequate | * | * | * | * | * | * | * | * |
| Representativeness of cases | * | * | * | * | * | * | * | * | |
| Selection of controls | * | * | * | * | * | * | * | * | |
| Definition of controls | * | _ | * | _ | * | * | _ | * | |
| Comparability | ** | ** | ** | * | ** | ** | ** | ** | |
| Exposure | Ascertainment of exposure | _ | * | * | _ | * | _ | _ | * |
| Same method of ascertainment for case and control | _ | _ | _ | _ | _ | _ | _ | _ | |
| Nonresponse rate | _ | * | * | * | _ | _ | * | * | |
| Quality | Moderate | Good | Good | Poor | Good | Moderate | Moderate | Good |
| Studies | Pawar et al., 2022 [33] India | Balik et al., 2017 [30] Turkey | Su et al., 2016 [35] China | Lemos et al., 2015 [32] Brazil | Blanco-Aguilera et al., 2014 [2] Spain | Gui et al., 2014 [31] Brazil | Resende et al., 2013 [34] Brazil | |
|---|---|---|---|---|---|---|---|---|
| Selection | Representativeness of sample | * | * | * | * | * | * | * |
| Sample size | * | * | * | * | * | * | * | |
| Nonrespondent | _ | _ | * | * | * | * | * | |
| Uncertainty of exposure | _ | _ | _ | _ | _ | * | * | |
| Comparability | ** | _ | * | _ | _ | ** | ** | |
| Outcome | Assessment of outcome | * | * | * | * | * | * | * |
| Statistical tests | * | * | * | * | * | * | * | |
| Quality | Moderate | Poor | Good | Moderate | Poor | Good | Good |
| Outcomes | № of Participants (Studies) Follow-Up | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Anticipated Absolute Effects | |
|---|---|---|---|---|---|
| Risk with Healthy Control | Risk Difference with Temporomandibular Disorder Patients | ||||
| TMD and Myofascial pain and oral health-related quality of life (TMD) assessed with: Relative risk timing of exposure: mean 6 months | 3945 cases 1943 controls (7 observational studies) | Low a,b | RR 3.18 (1.90 to 4.46) | Low | |
| 520 per 1000 | 1134 more per 1000 (468 more to 1799 more) | ||||
| TMD and Myofascial pain and oral health-related quality of life assessed with odds ratio follow-up: mean 6 months | 304 cases 727 controls/exposed 304/991 unexposed (3 observational studies) | Low | OR 8.21 (2.39 to 28.25) | Study population | |
| 307 per 1000 | 477 more per 1000 (358 more to 619 more) | ||||
| Low | |||||
| 307 per 1000 | 477 more per 1000 (358 more to 619 more) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlSahman, L.; AlBagieh, H.; AlSahman, R. Oral Health-Related Quality of Life in Temporomandibular Disorder Patients and Healthy Subjects—A Systematic Review and Meta-Analysis. Diagnostics 2024, 14, 2183. https://doi.org/10.3390/diagnostics14192183
AlSahman L, AlBagieh H, AlSahman R. Oral Health-Related Quality of Life in Temporomandibular Disorder Patients and Healthy Subjects—A Systematic Review and Meta-Analysis. Diagnostics. 2024; 14(19):2183. https://doi.org/10.3390/diagnostics14192183
Chicago/Turabian StyleAlSahman, Lujain, Hamad AlBagieh, and Roba AlSahman. 2024. "Oral Health-Related Quality of Life in Temporomandibular Disorder Patients and Healthy Subjects—A Systematic Review and Meta-Analysis" Diagnostics 14, no. 19: 2183. https://doi.org/10.3390/diagnostics14192183