
Array Comparative Genomic Hybridization (aCGH) Results among Patients Referred to Invasive Prenatal Testing after First-Trimester Screening: A Comprehensive Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Genetic Testing
Array Comparative Genomic Hybridization Analysis and Interpretation
2.2. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Nicolaides, K.H.; Azar, G.; Byrne, D.; Mansur, C.; Marks, K. Fetal nuchal translucency: Ultrasound screening for chromosomal defects in first trimester of pregnancy. BMJ 1992, 304, 867–869. [Google Scholar] [CrossRef] [PubMed]
- Snijders, R.J.; Noble, P.; Sebire, N.; Souka, A.; Nicolaides, K.H. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal translucency thickness at 10–14 weeks of gestation. Fetal Medicine Foundation First Trimester Screening Group. Lancet 1998, 352, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Souka, A.P.; Von Kaisenberg, C.S.; Hyett, J.A.; Sonek, J.D.; Nicolaides, K.H. Increased nuchal translucency with normal karyotype. Am. J. Obs. Gynecol. 2005, 192, 1005–1021. [Google Scholar] [CrossRef] [PubMed]
- Hellmuth, S.G.; Pedersen, L.H.; Miltoft, C.B.; Petersen, O.B.; Kjaergaard, S.; Ekelund, C.; Tabor, A. Increased nuchal translucency thickness and risk of neurodevelopmental disorders. Ultrasound Obs. Gynecol. 2017, 49, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.J.; Norton, M.E.; Shaw, G.M.; Flessel, M.C.; Goldman, S.; Currier, R.J.; Jelliffe-Pawlowski, L.L. Risk of selected structural abnormalities in infants after increased nuchal translucency measurement. Am. J. Obstet. Gynecol. 2014, 211, 675.e1–675.e19. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.; Kagan, K.O.; Molina, F.S.; Gazzoni, A.; Nicolaides, K.H. A mixture model of nuchal translucency thickness in screening for chromosomal defects. Ultrasound Obs. Gynecol. 2008, 31, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Kagan, K.O.; Wright, D.; Valencia, C.; Maiz, N.; Nicolaides, K.H. Screening for trisomies 21, 18 and 13 by maternal age, fetal nuchal translucency, fetal heart rate, free beta-hCG and pregnancy-associated plasma protein-A. Hum. Reprod. 2008, 23, 1968–1975. [Google Scholar] [CrossRef]
- Nicolaides, K.H. Screening for fetal aneuploidies at 11 to 13 weeks. Prenat. Diagn. 2011, 31, 7–15. [Google Scholar] [CrossRef]
- Grande, M.; Jansen, F.A.R.; Blumenfeld, Y.J.; Fisher, A.; Odibo, A.O.; Haak, M.C.; Borrell, A. Genomic microarray in fetuses with increased nuchal translucency and normal karyotype: A systematic review and meta-analysis. Ultrasound Obs. Gynecol. 2015, 46, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Polish Gynaecological Society guideline on prenatal diagnosis. Ginekol. Pol. 2009, 80, 390–393.
- Maya, I.; Yacobson, S.; Kahana, S.; Yeshaya, J.; Tenne, T.; Agmon-Fishman, I.; Cohen-Vig, L.; Shohat, M.; Basel-Vanagaite, L.; Sharony, R. Cut-off value of nuchal translucency as indication for chromosomal microarray analysis. Ultrasound Obs. Gynecol. 2017, 50, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Kagan, K.O.; Sonek, J.; Wagner, P.; Hoopmann, M. Principles of first trimester screening in the age of non-invasive prenatal diagnosis: Screening for chromosomal abnormalities. Arch. Gynecol. Obs. 2017, 296, 645–651. [Google Scholar] [CrossRef]
- van der Meij, K.R.M.; Sistermans, E.A.; Macville, M.V.E.; Stevens, S.J.C.; Bax, C.J.; Bekker, M.N.; Bilardo, C.M.; Boon, E.M.J.; Boter, M.; Diderich, K.E.M.; et al. TRIDENT-2: National implementation of genome-wide non-invasive prenatal testing as a first-tier screening test in the Netherlands. Am. J. Hum. Genet. 2019, 105, 1091–1101. [Google Scholar] [CrossRef]
- Srebniak, M.I.; de Wit, M.C.; Diderich, K.E.; Govaerts, L.C.; Joosten, M.; Knapen, M.F.; Bos, M.J.; Looye-Bruinsma, G.A.; Koningen, M.; Go, A.T.; et al. Enlarged NT (≥3.5 mm) in the first trimester—Not all chromosome aberrations can be detected by NIPT. Mol. Cytogenet. 2016, 9, 69. [Google Scholar] [CrossRef]
- Huang, J.; Poon, L.C.; Akolekar, R.; Choy, K.W.; Leung, T.Y.; Nicolaides, K.H. Is high fetal nuchal translucency associated with submicroscopic chromosomal abnormalities on array CGH? Ultrasound Obs. Gynecol. 2014, 43, 620–624. [Google Scholar] [CrossRef]
- Wapner, R.J.; Martin, C.L.; Levy, B.; Ballif, B.C.; Eng, C.M.; Zachary, J.M.; Savage, M.; Platt, L.D.; Saltzman, D.; Grobman, W.A.; et al. Chromosomal microarray versus karyotyping for prenatal diagnosis. N. Engl. J. Med. 2012, 367, 2175–2184. [Google Scholar] [CrossRef]
- Committee on Genetics and the Society for Maternal-Fetal Medicine. Committee Opinion No.682: Microarrays and Next-Generation Sequencing Technology: The Use of Advanced Genetic Diagnostic Tools in Obstetrics and Gynecology. Obs. Gynecol. 2016, 128, e262–e268. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.; de Leeuw, N.; Mann, K.; Schuring-Blom, H.; Morgan, S.; Giardino, D.; Rack, K.; Hastings, R. European guidelines for constitutional cytogenomic analysis. Eur. J. Hum. Genet. 2019, 27, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Polish Gynecological Society—Ultrasound Section Guidelines on ultrasound screening in uncomplicated pregnancy (2 December 2011). Ginekol. Pol. 2012, 83, 309–315.
- Salomon, L.J.; Alfirevic, Z.; Bilardo, C.M.; Chalouhi, G.E.; Ghi, T.; Kagan, K.O.; Lau, T.K.; Papageorghiou, A.T.; Raine-Fenning, N.J.; Stirnemann, J.; et al. ISUOG practice guidelines: Performance of first-trimester fetal ultrasound scan. Ultrasound Obstet. Gynecol. 2013, 41, 102–113. [Google Scholar]
- Kowalczyk, K.; Bartnik-Głaska, M.; Smyk, M.; Plaskota, I.; Bernaciak, J.; Kędzior, M.; Wiśniowiecka-Kowalnik, B.; Jakubów-Durska, K.; Braun-Walicka, N.; Barczyk, A.; et al. Prenatal Diagnosis by Array Comparative Genomic Hybridization in Fetuses with Cardiac Abnormalities. Genes 2021, 12, 2021. [Google Scholar] [CrossRef]
- Wójtowicz, A.; Madetko-Talowska, A.; Wójtowicz, W.; Szewczyk, K.; Huras, H.; Bik-Multanowski, M. Cardiovascular Anomalies among 1005 Fetuses Referred to Invasive Prenatal Testing-A Comprehensive Cohort Study of Associated Chromosomal Aberrations. Int. J. Environ. Res. Public Health 2022, 19, 10019. [Google Scholar] [CrossRef]
- Claustres, M.; Kožich, V.; Dequeker, E.; Fowler, B.; Hehir-Kwa, J.; Miller, K.; Oosterwijk, C.; Peterlin, B.; van Ravenswaaij-Arts, C.; Zimmermann, U.; et al. Recommendations for reporting results of diagnostic genetic testing (biochemical, cytogenetic and molecular genetic). Eur. J. Hum. Gen. 2013, 22, 160–170. [Google Scholar] [CrossRef]
- Nowakowska, B. Clinical interpretation of copy number variants in the human genome. J. Appl. Gen. 2017, 58, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Chan, K.; Leung, K.; Au, P.; Tam, W.; Li, S.; Luk, H.; Kan, A.; Chung, B.; Lo, I.; et al. Experience of chromosomal microarray applied in prenatal and postnatal settings in Hong Kong. Am. J. Med. Gen. Part. C Semin. Med. Genet. 2019, 181, 196–207. [Google Scholar] [CrossRef]
- Johnson, K.; Kelley, J.; Saxton, V.; Walker, S.P.; Hui, L. Declining invasive prenatal diagnostic procedures: A comparison of tertiary hospital and national data from 2012 to 2015. Aust. N. Z. J. Obs. Gynaecol. 2017, 57, 152–156. [Google Scholar] [CrossRef]
- Bardi, F.; Bosschieter, P.; Verheij, J.; Go, A.; Haak, M.; Bekker, M.; Sikkel, E.; Coumans, A.; Pajkrt, E.; Bilardo, C. Is there still a role for nuchal translucency measurement in the changing paradigm of first trimester screening? Prenat. Diagn. 2020, 40, 197–205. [Google Scholar] [CrossRef]
- Shaffer, L.G.; Rosenfeld, J.A.; Dabell, M.P.; Coppinger, J.; Bandholz, A.M.; Ellison, J.W.; Ravnan, J.B.; Torchia, B.S.; Ballif, B.C.; Fisher, A.J. Detection rates of clinically significant genomic alterations by microarray analysis for specific anomalies detected by ultrasound. Prenat. Diagn. 2012, 32, 986–995. [Google Scholar] [CrossRef]
- Scott, F.; Murphy, K.; Carey, L.; Greville, W.; Mansfield, N.; Barahona, P.; Robertson, R.; McLennan, A. Prenatal diagnosis using combined quantitative fluorescent polymerase chain reaction and array comparative genomic hybridization analysis as a first-line test: Results from over 1000 consecutive cases. Ultrasound Obs. Gynecol 2013, 41, 500–507. [Google Scholar] [CrossRef]
- Hillman, S.C.; McMullan, D.J.; Hall, G.; Togneri, F.S.; James, N.; Maher, E.J.; Meller, C.H.; Williams, D.; Wapner, R.J.; Maher, E.R.; et al. Use of prenatal chromosomal microarray: Prospective cohort study and systematic review and meta-analysis. Ultrasound Obs. Gynecol. 2013, 41, 610–620. [Google Scholar] [CrossRef]
- Tanner, L.M.; Alitalo, T.; Stefanovic, V. Prenatal array comparative genomic hybridization in a well-defined cohort of high-risk pregnancies. A 3-year implementation results in a public tertiary academic referral hospital. Prenat. Diagn. 2021, 41, 422–433. [Google Scholar] [CrossRef]
- Coello-Cahuao, E.; Sánchez-Durán, M.Á.; Calero, I.; Higueras, M.T.; García, M.A.; Rodó, C.; Maiz, N.; Plaja Rustein, A.; Castells-Sarret, N.; Mediano-Vizuete, C.; et al. Array study in fetuses with nuchal translucency above the 95th percentile: A 4-year observational single-centre study. Arch. Gynecol. Obs. 2023, 307, 285–292. [Google Scholar] [CrossRef]
- Egloff, M.; Hervé, B.; Quibel, T.; Jaillard, S.; Le Bouar, G.; Uguen, K.; Saliou, A.H.; Valduga, M.; Perdriolle, E.; Coutton, C.; et al. Diagnostic yield of chromosomal microarray analysis in fetuses with isolated increased nuchal translucency: A French multicenter study. Ultrasound Obs. Gynecol. 2018, 52, 715–721. [Google Scholar] [CrossRef]
- Petersen, O.B.; Smith, E.; Van Opstal, D.; Polak, M.; Knapen, M.F.C.M.; Diderich, K.E.M.; Bilardo, C.M.; Arends, L.R.; Vogel, I.; Srebniak, M.I. Nuchal translucency of 3.0–3.4 mm an indication for NIPT or microarray? Cohort analysis and literature review. Acta Obs. Gynecol. Scand. 2020, 99, 765–774. [Google Scholar] [CrossRef]
- Hui, L.; Pynaker, C.; Bonacquisto, L.; Lindquist, A.; Poulton, A.; Kluckow, E.; Hutchinson, B.; Norris, F.; Pertile, M.D.; Gugasyan, L.; et al. Reexamining the optimal nuchal translucency cutoff for diagnostic testing in the cell-free DNA and microarray era: Results from the Victorian Perinatal Record Linkage study. Am. J. Obs. Gynecol. 2021, 225, 527.e1–527.e12. [Google Scholar] [CrossRef]
- Sagi-Dain, L.; Singer, A.; Ben Shachar, S.; Josefsberg Ben Yehoshua, S.; Feingold-Zadok, M.; Greenbaum, L.; Maya, I. Risk of Clinically Significant Chromosomal Microarray Analysis Findings in Fetuses with Nuchal Translucency From 3.0 mm through 3.4 mm. Obs. Gynecol. 2021, 137, 126–131. [Google Scholar] [CrossRef]
- Su, L.; Huang, H.; An, G.; Cai, M.; Wu, X.; Li, Y.; Xie, X.; Lin, Y.; Wang, M.; Xu, L. Clinical application of chromosomal microarray analysis in fetuses with increased nuchal translucency and normal karyotype. Mol. Genet. Genom. Med. 2019, 7, e811. [Google Scholar] [CrossRef]
- Xue, S.; Yan, H.; Chen, J.; Li, N.; Wang, J.; Liu, Y.; Zhang, H.; Li, S.; Zhang, W.; Chen, D.; et al. Genetic examination for fetuses with increased fetal nuchal translucency by genomic technology. Cytogenet. Genome Res. 2020, 160, 57–62. [Google Scholar] [CrossRef]
- Srebniak, M.I.; Joosten, M.; Knapen, M.F.C.M.; Arends, L.R.; Polak, M.; van Veen, S.; Go, A.T.J.I.; Van Opstal, D. Frequency of submicroscopic chromosomal aberrations in pregnancies without increased risk for structural chromosomal aberrations: Systematic review and meta-analysis. Ultrasound Obs. Gynecol. 2018, 51, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Spataro, E.; Cordisco, A.; Luchi, C.; Filardi, G.R.; Masini, G.; Pasquini, L. Increased nuchal translucency with normal karyotype and genomic microarray analysis: A multicenter observational study. Int. J. Gynaecol. Obs. 2023, 161, 1040–1045. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| NT < p95 n = 754 | NT ≥ p95 n = 992 | OR (95% CI) | p | |
|---|---|---|---|---|
| Maternal age, years | ||||
| mean ± SD | 34.98 ± 5.1614 | 35.5 ± 5.5 | - | 0.326 |
| Min–max | 17–46 | 18–47 | ||
| median | 35 | 36 | ||
| All pathogenic chromosomal aberrations, n (%) | 67 (8.8) | 354 (35.7) | 5.7 (7.54–4.28) | 0.0000 |
| Numerical chromosomal aberrations (total), n (%) | N = 45 (5.9%) | N = 289 (29.1%) | 6.48 (4.66–9.02) | 0.0000 |
| T21, n (%) | 17 (2.3) | 157 (15.8) | 8.15 (4.89–13.57) | 0.0000 |
| T18, n (%) | 7 (0.9) | 48 (4.8) | 5.4 (2.44–12.06) | 0.0000 |
| T13, n (%) | 5 (0.6) | 19 (1.9) | 2.925 (1.08–7.87) | 0.026 |
| 45, X0, n (%) | 3 (0.4) | 57 (5.7) | 15.26 (4.76–48.92) | 0.0000 |
| 47, XXX; 47, XXY, n (%) | 5 (0.6) | 5 (0.5) | 0.75 (0.21–2.63) | 0.66 |
| Triploidy, n (%) | 8 (1.0) | 3 (0.3) | 0.34 (0.11–1.11) | 0.06 |
| CNV, n (%) | 22 (2.9) | 65 (6.5) | 2.33 (1.42–3.81) | 0.0005 |
| Associated structural anomalies | ||||
| -none, n (%) | 454 (60.2) | 684 (68.9) | 1.46 (1.20–1.78) | 0.0001 |
| -one or more anomalies, n (%) | 300 (39.8) | 308 (31.1) | 0.68 (0.83–0.56) | 0.0001 |
| Structural anomalies | ||||
| -CNS, n (%) | 55 (7.3) | 14 (1.4) | 0.18 (0.1–0.32) | 0.0000 |
| -cardiovascular anomalies, n (%) | 102 (13.5) | 108 (10.8) | 0.78 (0.58–1.04) | 0.092 |
| -genitourinary tract, n (%) | 20 (2.6) | 16 (1.6) | 0.60 (0.30–1,16) | 0.1300 |
| -gastro-abdominal, n (%) | 40 (5.2) | 13 (1.3) | 0,23 (0.12–0.44) | 0,0000 |
| -skeletal, n (%) | 62 (8.2) | 33 (3.3) | 0.38 (0.24–0.59) | 0,0000 |
| -face/neck, n (%) | 35 (4.6) | 36 (3.6) | 0.77 (0.48–1.24) | 0.2885 |
| -pulmonary/thoracic, n (%) | 11 (1.4) | 6 (0.6) | 0.41 (0.15–1.11) | 0.07 |
| -oedema, n (%) | 4 (0.5) | 81 (8.1) | 16.6 (6.08–45.70) | 0.0000 |
| -FGR, n (%) | 39 (5.1) | 6 (0.6) | 0.11 (0.04–0.26) | 0.0000 |
| -amniotic fluid anomaly, n (%) | 17 (2.2) | 3 (0.3) | 0.13 (0.03–0.45) | 0.0001 |
| First-trimester markers: | ||||
| -TR, n (%) | 39 (5.1) | 52 (5.2) | 1.01 (0.66–1.55) | 0.94 |
| -DV abnormal, n (%) | 33 (4.4) | 34 (3.4) | 0.77 (0.47–1.26) | 0.30 |
| -NB hypoplasia, n (%) | 88 (11.7) | 89 (8.9) | 0.74 (0.54–1.01) | 0.064 |
| Fetuses without associated anomalies, n (%) | N = 454 (60.2) | N = 684 (68.9) | 1.46 (1.20–1.78) | 0.0001 |
| All pathogenic chromosomal aberrations, n (%) | 24 (5.3) | 224 (32.7) | 8.72 (5.61–13.56) | 0.0000 |
| Numerical chromosomal aberrations (total), n (%) | 15 (3.3) | 184 (26.9) | 10.77 (6.26–18.51) | 0.0000 |
| T21, n (%) | 9 (1.9) | 123 (18.0) | 10.84 (5.44–21.57) | 0.0000 |
| T18, n (%) | 0 (0.0) | 20 (2.9) | - | 0.0002 |
| T13, n (%) | 0 (0.0) | 5 (0.7) | - | 0.0679 |
| 45, X0 n (%) | 2 (0.4) | 32 (4.7) | 0.03 (0.01–0.16) | 0.0000 |
| 47,XXX; 47,XXY, n (%) | 4 (0.8) | 4 (0.6) | 0.66 (0.16–2.65) | 0.5580 |
| Triploidy, n (%) | 0 (0.0) | 0 (0.0) | - | - |
| CNV, n (%) | 9 (1.9) | 40 (5.8) | 3.07 (1.47–6.39) | 0.0017 |
| No | ISCN 2020 arr[GRCh37] | Size and Type | CNV Interpretation | Detailed Clinical Indications |
|---|---|---|---|---|
| 1. | 6q27(168157088_170041859)x1 | 1.88 Mbp deletion | Female karyotype, 6q microdeletion syndrome reported in UNIQUE database: https://www.rarechromo.org/media/information/Chromosome%20%206/6q%20deletions%20from%206q26%20and%206q27%20FTNP.pdf (accessed on 29 April 2024) | NT = 2 mm First-trimester abnormal biochemistry, high risk of Down syndrome |
| 2. | 10q22.3q23.2(81641918_88847443)x1 | 7.2 Mbp deletion | Male karyotype, genome imbalance was found in the form of a deletion of the long arm of chromosome 10 in the 10q22.3q23.2 region | NT = 3 mm High risk of Down syndrome Agenesis of one kidney |
| 3. | 22q11.21(18894820_21457610)x1 | 2.56 Mbp deletion | Female karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 22 in the 22q11.21 region. The deletion covers the 22q11.2 deletion syndrome region (OMIM 188400)1 (ORPHA:567)2, including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, thymic aplasia/hypoplasia and immunodeficiency | NT = 3 mm High risk of Down syndrome, RAA |
| 4. | Xq22.3(105159857_105621192)x2 | 460 kb duplication | Male karyotype, genome imbalance was found in the form of a duplication of the long arm of the X chromosome in the Xq22.3 band with a size of ~460 kb. The duplication includes the SERPINA7 gene (OMIM 314200) and exons 16–29 of the NRK gene (OMIM 300791). Amplification of the SERPINA7 gene has been described in patients with excess thyroxine-binding globulin (TBG). | NT = 4 mm High risk of Down syndrome |
| 5. | 5p15.33p11(22149_46115173)x3 dn | 46.09 Mbp duplication | Female karyotype, in which genome imbalance was found in the form of the short arm of chromosome 5 duplication in the 5p15.33p11 region with a size of ~46.09 Mbp, which corresponds to trisomy of the short arm of chromosome 5. The aberration affects many genes and is a pathogenic change. Chromosome analysis after cell culture (DM700/19) showed the presence of two cell lines: mos46,XX[11]/47,XX,del(5)(p11),+i(5)(p11)[3]. In 3 out of 14 cells analyzed, a deletion of the short arm of chromosome 5 and the presence of an additional isochromosome 5p were found, and in the remaining 11 cells analyzed, a normal female karyotype was found. The presence of a normal female cell line may indicate the growth of cells of maternal origin in the resulting culture. | NT = 4 mm High risk of Down syndrome |
| 6. | 3q24q29(147103808_197837069)x2~3, 4q34.1q35.2(174521042_190791091)x1~2 | 50.73 Mbp duplication 16.27 Mbp deletion | Male karyotype, genome imbalance was found in the form of a mosaic duplication of the long arm of chromosome 3 in the 3q24q29 region of ~50.73 Mbp and a mosaic deletion of the long arm of chromosome 4 in the 4q34.1q35.2 region of ~16.27 Mbp. Aberrations involve many genes and may be responsible for abnormalities detected in the fetus during ultrasound examination. | NT = 4 mm High risk of Down syndrome |
| 7. | 6p21.33(31946615_32009011)x1 | 60 kb deletion | Male karyotype, genome imbalance was found in the form of a deletion of the short arm of chromosome 6 in the 6p21.33 region of ~60 kb. The deletion includes the following genes: C4A (OMIM 120810)1, C4B (OMIM 120820)1, CYP21A2 (OMIM 613815)1 and exons 4–8 of the STK19 gene (OMIM 604977)1. Due to the family history of congenital adrenal hyperplasia, it is advisable to exclude the presence of mutations in the second allele of the CYP21A2 gene. | NT = 4 mm High risk of Down syndrome, positive family history of congenital adrenal hyperplasia in daughter from a previous pregnancy. |
| 8. | 22q11.21(18894820_21457610)x1 | 2.56 Mb deletion | Male karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The deletion covers the 22q11.2 deletion syndrome region (OMIM 188400)1 (ORPHA:567)2, including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, aplasia/hypoplasia of the thymus and immunodeficiency. | NT = 4 mm High risk of Down syndrome, CHD (TOF) |
| 9. | 22q11.21(18894820_21457610)x1 | 2.56 Mb deletion | Male karyotype, genome imbalance was found in the form of deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The deletion is located in the region of the known 22q11 microdeletion syndrome (OMIM: 188400). | NT = 5 mm omphalocele,HLHS, NB hypoplasia High risk of Down syndrome |
| 10. | 22q11.21(18894820_21457610)x1 | 2.56 Mb deletion | Female karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The deletion covers the 22q11.2 deletion syndrome region (OMIM 188400)1 (ORPHA:567)2, including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, aplasia/hypoplasia of the thymus and immunodeficiency. | NT = 5 mm High risk of Down syndrome, Abnormal profile |
| 11. | 22q11.21(18894820_21457610)x1 | 2.56 Mb deletion | Male karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The deletion covers the 22q11.2 deletion syndrome region (OMIM 188400)1 (ORPHA:567)2, including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, aplasia/hypoplasia of the thymus and immunodeficiency. | NT = 5 mm High risk of Down syndrome HLHS |
| 12. | 13q14.2q34(49772419_115093115)x3 | 65.3 Mbp duplication | Male karyotype, genome imbalance was found in the form of a duplication of the long arm of chromosome 13 in the 13q14.2q34 region with a size of ~65.3 Mbp. | NT = 6 mm High risk of Down syndrome micrognatia, polidactyly |
| 13. | 14q11.2(21859914_21913304)x1 | 53 kb deletion | Male karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 14 in the 14q11.2 region with a size of ~53 kb. The deletion covers exons 1–35 of the dose-sensitive CHD8 gene (OMIM 610528)1 and is located in the region of the 14q11-q22 deletion syndrome (OMIM 613457)1 (ORPHA:261120)3, described in patients among others, with, delayed psychomotor development, hypotonia, facial dysmorphic features. Additionally, mutations and deletions of the CHD8 gene have been described in patients, among others, with autism. | NT = 7 mm High risk of Down syndrome |
| 14. | 1p21.3p12(95352587_118623859)x1 | 23.3 Mbp deletion | Male karyotype, genome imbalance was found in the form of an interstitial deletion of the short arm of chromosome 1 in the 1p21.3p12 region with a size of ~23.3 Mbp. The deletion in the 1p21.3p12 region covers 157 protein-coding genes, including the following genes: DPYD (OMIM 612779)1, DBT (OMIM 248610)1, dose-sensitive COL11A1 (OMIM 120280)1, GPSM2 (OMIM 609245)1, dose-sensitive TAF13 (OMIM 600774)1, AP4B1 (OMIM 607245)1, NRAS (OMIM 164790)1 and CASQ2 (OMIM 114251)1. The aberration covers the region of the 1p21.3 microdeletion syndrome (ORPHA:293948)2 described in patients including those with speech development delay, intellectual disability, autism, facial dysmorphic features and obesity. Deletions in the 1p13.1p21.1 region have been described in patients, among others, with intellectual disability, short stature, dysmorphic features, and eye defects. | NT = 7 mm High risk of Down syndrome |
| 15. | 5q35.2q35.3(175116131_180696832)x1 | 5.58 Mbp deletion | Female karyotype, genome imbalance was found in the form of a terminal deletion of the long arm of chromosome 5 in the 5q35.2q35.3 region with a size of ~5.58 Mbp. The deletion covers 87 protein-coding genes, including the NSD1 gene (OMIM 606681) and is located in the region of 5q35 deletion syndrome (ORPHA:1627)2, characterized by: lymphedema with widening of the nuchal translucency In the prenatal period, as well as early infantile hypotonia, short stature, facial dysmorphic features and heart defects. The 5q35 deletion regionIdes the region of Sotos syndrome 1 (SOTOS1, OMIM 117550), described in patients with facial dysmorphic features, high birth weight and excessive growth in early life, macrocephaly, intellectual disability, as well as heart defects such as atrial septal defect (ASD), ventricular septal defect (VSD). | NT = 7 mm High risk of Down syndrome CHD (ASD) |
| 16. | 22q11.21(18894820_21457610)x1 | 2.56 Mbp deletion | Male karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The deletion covers the 22q11.2 deletion syndrome region (OMIM 188400) (ORPHA:567), including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, aplasia/hypoplasia of the thymus, and immunodeficiency. | NT = 8 mm High risk of Down syndrome |
| 17. | Xp21.1(31837550_32165393)x1,(21)x3 | 328 kb deletion | Female karyotype, genome imbalance was found in the form of trisomy of chromosome 21 and deletion of the short arm of the X chromosome in the Xp21.1 region of ~328 kb. Trisomy of chromosome 21 corresponds to the diagnosis of Down syndrome. The deletion in the Xp21.1 region covers exons 45–78 of the dose-sensitive DMD gene (OMIM 300377). Mutations and deletions of this gene have been described in patients with Duchenne muscular dystrophy (OMIM 310200), Becker muscular dystrophy (OMIM 300376) and dilated cardiomyopathy (OMIM 302045). The aberration is a pathogenic change and may be inherited from carrier mothers who do not show clinical symptoms. | NT = 9 mm High risk of Down syndrome |
| 18. | 3q26.32q26.33(177804563_180939724)x3 | 3.1 Mbp duplication | Male karyotype, 3q duplication syndrome reported in the UNIQUE database, phenotype depending on the size and location of the aberration https://www.rarechromo.org/media/information/Chromosome%20%203/3q%20duplications%20FTNP.pdf (accessed on 29 April 2024) | NT = 10 mm High risk of Down syndrome NB hypoplasia, flat profile, club foot |
| 19. | 18p11.32p11.21(149089_11050847)x1, 18p11.21q23(11162185_77794890)x3 | 11 Mbp deletion 66.7 Mbp duplication | Female karyotype, genome imbalance was found in the form of a deletion of the short arm of chromosome 18 in the 18p11.31p11.21 region of ~11 Mbp and a duplication in the 18p11.21q23 region of ~66.7 Mbp | NT= 10 mm, Multiple structural anomalies High risk of Down syndrome |
| 20. | 13q33.1q34(103658425_115092648)x1, 21q22.2q22.3(39764621_48090317)x3 | 11.4 Mbp deletion | Male karyotype, common phenotype after both changes: del13 CHROMOSOME 13q33-q34 DELETION SYNDROME (OMIM#619148) and dup21 genes which are essential in producing the main Down syndrome hen CP, Chen CY, Chern SR, et al. Detection of a familial 21q22.3 microduplication in a fetus associated with congenital heart defects. Taiwan J. Obstet. Gynecol. 2019, 58, 869–871 features cluster in chromosomal bands 21q22.2q22.3 Schnabel F, Smogavec M, Funke R, Pauli S, Burfeind P, Bartels I. Down syndrome phenotype in a boy with a mosaic microduplication of chromosome 21q22. Mol. Cytogenet. 2018, 11, 62. | NT = 11 mm High risk of Down syndrome |
| 21. | 22q11.21(18661724_21440514)x1 | 2.77 Mbp deletion | Male karyotype,the deletion covers the 22q11.2 deletion syndrome region (OMIM 188400) (ORPHA:567), including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, aplasia/hypoplasia of the thymus, and immunodeficiency. | NT = 1.2 mm HRHS,NB hypoplasia |
| 22. | 17p11.2(19143173_2021946 | 1.1 Mbp deletion | Female karyotype, Smith–Magenis syndrome (OMIM#182290) bez mutacji w RAI1. Vieira GH, Rodriguez JD, Carmona-Mora P, et al. Detection of classical 17p11.2 deletions, an atypical deletion and RAI1 alterations in patients with features suggestive of Smith–Magenis syndrome. Eur. J. Hum. Genet. 2012, 20, 148–154. doi:10.1038/ejhg.2011.167 | NT = 1.3 mm Family history of mental retardation, Abnormal appearance of the eyelids after delivery |
| 23. | 16p11.2(29673954_30190568)x3 | 0.5 Mbp duplication | Female karyotype, chromosome 16p11.2 duplication syndrome (# 614671) | NT = 2.2 mm Intermediate risk of Down synfrome, parental request, FGR in third trimester+ hyperechogenic bowels |
| 24. | 1q43q44(242398564_249212668)x1 | 6.8 Mbp deletion | Male karyotype, chromosome 1q43-q44 deletion syndrome: mental retardation, autosomal dominant 22 (# 612337) | NT = 1.5 mm High risk of Down syndrome |
| 25. | 6q26q27(163373677_170921089)x1 | 7.56 Mbp deletion | Female karytype, 6q26 deletion syndrome | NT = 1.5 mm Amniocentesis due to Toxoplasma gondii infection |
| 26. | 22q11.21(18904835_21505400)x1 | 2.6 Mbp deletion | Male karyotype, the deletion covers the 22q11.2 deletion syndrome region (OMIM 188400) (ORPHA:567), including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, aplasia/hypoplasia of the thymus, and immunodeficiency. | NT = 1.6 mm IAA + VSD |
| 27. | 16p13.12p13.11(14762239_16194578)x1 | 1.4 Mbp deletion | Female karyotype, 16p13.11 microdeletion syndrome reported in UNIQUE database, https://www.rarechromo.org/media/information/Chromosome%2016/16p13.11%20microdeletions%20FTNW.pdf (accessed on 29 April 2024) | NT = 1.6 mm maternal request, AMA |
| 28. | 5p15.33p15.2(22149_10044258)x1 | 10 Mbp deletion | Female karyotype, CRI-DU-CHAT SYNDROME (# 123450) | NT = 1.7 mm DORV TOF type |
| 29. | Xq28(149116213_155232907)x1 | 6.1 Mbp deletion | Male karyotype, Xq28 deletion syndrome in male (OMIM:# 300475) | NT = 1.7 mm RAA, thymus hypoplasia |
| 30. | 3q29(194969955_197317103)x1 | 2.35 Mbp deletion | Male karyotype, 3q29 DELETION SYNDROME (# 609425) | NT = 1.8 mm pulomoray valve dysplasia |
| 31. | 7p22.3p21.1(2634026_16758426)x3 | 14.1 Mbp duplcation | Male karyotype, 14.1 Mbp | NT = 4.7 mm Small kidneys, Oligohydramnion/amnioinfusion High risk of Down syndrome |
| 32. | 16p11.2(29673954_30190568)x1 | 0.5 Mbp deletion | Female karyotype, chromosome 16p11.2 deletion syndrome (# 611913) | NT = 4.8 mm carrier status in mother High risk of Down syndrome |
| 33. | 7q31.2q32.2(116255056_129694097)x3, 7q32.2q36.3(129853288_159085681)x1 | 13.4 Mbp duplication 29.2 Mbp deletion | Male karyotype; posssibly structural aberration in chromosome 7; duplication in UNIQUE database reported dup7q: https://www.rarechromo.org/media/information/Chromosome%20%207/7q%20Duplications%20FTNW.pdf (accessed on 29 April 2024) deletion: https://www.rarechromo.org/media/information/Chromosome%20%207/7q32q34%20deletions%20FTNW.pdf (accessed on 29 April 2024) | NT = 1.9 mm cleft palate, CHD, CCA |
| 34. | 18p11.32p11.21(148963_14081887)x1 | 13.9 Mbp deletion | Female karyotype, 18p deletions described at UniQue | NT = 1.9 mm holoprosencephaly |
| 35. | 1q21.1q21.2(145415190_147824207)x1 | 2.4 Mbp deletion | Female karyotype, chromosome 1q21.1 deletion syndrome (# 612474) | NT = 2 mm CHROMOSOME 1q21.1 DELETION SYNDROME in the mother and first son |
| 36. | 22q11.21(18894835_21505417)x1 | 2.6 Mbp deletion | Male karyotype, DiGeorge syndrome (OMIM#188400) | NT = 2.1 mm TOF + LSVC |
| 37. | 22q11.21q11.22(21808950_22905x1 | 1.1 Mbp deletion | Male karyotype, DiGeorge syndrome (OMIM#188400) | NT = 2.1 mm cleft lip and palate |
| 38. | 17p12p11.2(15801346_20464365)x1 | 4.66 Mbp deletion | Male karyotype, Smith–Magenis syndrome (OMIM#182290) | NT = 2.3 mm High risk od Down syndrome |
| 39. | 2p21(43391586_45394811)x1 | 2 Mbp deletion | Female karyotype, recurrent microdeletion 2q21.1: Report on a new patient with neurological disorders | NT = 2.3 mm semilobar holoprsonecephaly, cleft palate |
| 40. | 22q11.21q11.22(18894835_21505417)x1 | 2.6 Mbp deletion | Female karyotype, DiGeorge syndrome (OMIM#188400) | NT = 2.4 mm TOF + LSVC,thymus agenesis |
| 41. | 1q21.1q21.2(145415190_149275124)x3 | 3.86 Mbp duplication | Female, chromosome 1q21.1 duplication syndrome | NT = 2.4 mm High risk of Down syndrome, mental retardation in the mother |
| 42. | 2p16.3(51137071_51382872)x1 | 0.24 Mbp deletion | Male karyotype, chromosome 2p16.3 deletion syndrome (OMIM#614332) | NT = 2.4 mm DILV + PS |
| 43. | 22q11.1q11.21(17397498_20311763)x1 | 2.9 Mbp deletion | Male karyotype, DiGeorge syndrome (OMIM#188400) in corelation with translocation visible in GTG binding | NT = 2.5 mm Right isomerism |
| 44. | 5p15.33p15.1(22149_17479238)x1, 5p15.1p14.3(17745048_23253135)x4, 5p14.2p12(23503596_44506716)x3 | 17.46 Mbp deletion 5.51 Mbp duplication 21 Mbp duplication | Male karyotype, genome imbalance was found in the form of a deletion of the short arm of chromosome 5 in the 5p15.33p15.1 region with a size of ~17.46 Mbp, a triplication of the short arm of chromosome 5 in the 5p15.1p14.3 region with a size of ~5.51 Mbp and a duplication of the short arm of chromoIome 5 in the 5p14.2p12 region of ~21 Mbp. The 5p15.33p15.1 deletion covers the critical region of the 5p microdeletion syndrome (Cri Du Chat syndrome; OMIM: 123450). | NT = 2.7 mm AMA High risk of Down syndrome, AVSD |
| 45. | 1p36.33(779727_2063244)x1, 1p36.33p36.32(2162136_3444846)x3 | 1.28 Mbp deletion 1.28 Mbp duplication | Female karyotype, 1p36 microdeletion syndrome (OMIM# 607872; ORPHA:1606), 1p36 microduplication syndrome (ORPHA:96069) | NT = 4.7 mm early FGR High risk of Down syndrome |
| 46. | 6q25.2q27(153306440_170921089)x1, 20p13p12.3(60747_6317313)x3 | 17.6 Mbp deletion 6.26 Mpb duplication | Female karyotype, UNIQUE: 6q25.2q25.3 microdeletion syndrome (ORPHA:251056) and 6.26Mb duplication (UNIQUE: 20p duplication phenotype affected) | NT = 4.7 mm High risk of Down syndrome |
| 47. | 12p13.33p11.1(230421_34756209)x3 | 34.5 Mbp duplication | Female karyotype, Pallister–Killian syndrome (OMIM#601803) | NT = 2.8 mm CDH,flat profile, cleft palate, shortened bones, NB hypoplasia, FGR |
| 48. | 1q21.1q21.2(146155929_147824212)x1 | 1.67 Mbp deletion | Male karyotype, genome imbalance was found in the form of deletion of the long arm of chromosome 1 in the 1q21.1q21.2 region with a size of ~1.67 Mbp. The deletion covers the region of the known microdeletion syndrome 1q21.1 (OMIM: 612474)1 and belongs to pathogenic changes. | NT = 2.8 mm High risk of Down syndrome |
| 49. | 9p24.3p13.1(204090_38815471)x4 | 39 Mbp duplication | Male karyotype. Genomic imbalance was found in the form of tetrasomy of the short arm of chromosome 9 in the 9p24.3p13.1 region of ~39 Mbp. Chromosome analysis after cell culture (DM402/18) showed the presence of an additional isodicentric chromosome 9 in all 12 cells analyzed. | NT = 2.8 mm Age 36 years, hypoplastic nasal bone, posterior cranial fossa cyst, bilateral cleft lip, micrognathia, CHD. |
| 50. | 4p16.3p14(45889_38064734)x1 | 38 Mbp deletion | Female karyotype, genome imbalance was found in the form of deletion of the short arm of chromosome 4 in the 4p16.3p14 region with a size of ~38 Mbp. | NT = 4.8 mm Dysmorphic profile, CoA, club foot, abnormal first-trimester biochemistry High risk of Down syndrome |
| 51. | 11q24.1q25(123624201_134868407)x1 | 11.24 Mbp deletion | Female karyotype, Jacobsen syndrome (Deletion syndrome 11q, OMIM:# 147791 | NT = 4.6 mm CHD High risk of Down syndrome |
| 52. | 22q11.22q11.23(22843461_25066484)x3dn | 2.22 Mbp duplication | Male karyotype, genome imbalance was found in the form of a duplication of the long arm of chromosome 22 in the 22q11.22q11.23 region with a size of ~2.22 Mbp. The test result was confirmed by FISH (F2897). The duplIcation involves multiple genes, including the dose-sensitive SMARCB1 (OMIM: 6016071 and SNRPD3 (OMIM: 601062) genes. | NT = 3.1 mm history of fetal death, TR, VSD, NB hypoplasia |
| 53. | 7p14.3p14.1(32209242_41224388)x1 | 9 Mbp deletion | Male karyotype, genome imbalance was found in the form of a deletion of the short arm of chromosome 7 in the 7p14.3p14.1 region with a size of ~9 Mbp. The obtained test result confirms the 7p14 deletion found in the fetal karyotype test (study no. P 644/2017, Kraków) | NT = 3.2 mm High risk of Down syndrome |
| 54. | 9q21.13(77992580_78478835)x1 | 0.49 Mpb deletion | 0,49Mb/possibly microdeletion 9q21.13 syndrome (ORPHA:531151) | NT = 3.3 mm High risk of Down syndrome |
| 55. | 22q11.23(23720181_25066484)x3, | 1.35 Mbp duplication | Male karyotype, genome imbalance was found in the form of a duplication of the long arm of chromosome 22 in the 22q11.23 region with a size of ~1.35 Mbp. The dupIication involves multiple genes, including the dose-sensitive SMARCB1 (OMIM: 601607) and SNRPD3 (OMIM: 601062) genes. Duplications of this region may present with a wide range of clinical symptoms and may be inherited from parents who do not show clinical symptoms. | NT= 3.3 mm High risk of Down syndrome |
| 56. | 5p15.33p15.31(22149_7449397)x1, 5p15.31p12(7506131_44341490)x3 | 7.4 Mbp deletion duplication | Feamale karyotype, DELETION 5p15.3 is critical for Cri du Chat (OMIM#123450); DUPLICATION in UNIQUE reported trisomy 5p syndrome, phenotype depending on the size and location of the aberration https://www.crarechromo.Irg/media/information/Chromosome%20%205/Trisomy%205p%20Duplications%20of%205p15%20FTNW.pdf (accessed on 29 April 2024) | NT = 3.4 mm PA + VSD, FGR, NB hypoplasia |
| 57. | 2q13(110862477_111368891)x1, 12p13.33p13.32(23.421_3358023)x1 | 0.5 Mb deletion 3.1 Mbp deletion | 0.5Mb (2q13 benign variant), 3.1Mb (12p deletion pathogenic-12p13.33 deletion syndrome (ORPHA:280325) | NT = 3.4 mm hemivertebra, cerebellum hypoplasia, kidney dysplasia, club foot |
| 58. | 20p12.3(7246510_8558204)x1 | 1.31 Mbp deletion | Female karyotype, genome imbalance was found in the form of a deletion of the short arm of chromosome 20 in the 20p12.3 region with a size of ~1.31 Mbp. Examination of the parents using aCGH method showed that the deletion detected in the fetus was of paternal origin. The deletion includes the following genes: HAO1 (OMIM 605023)1, TMX4 (OMIM 616766)1, and exons 1–3 of the dose-sensitive gene PLCB1 (OMIM 607120)1. | NT = 3.5 mm High risk of Down syndrome |
| 59. | 22q11.21(18894820_21457610)x1 | 2.56 Mbp deletion | Female karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The deletion covers the 22q11.2 deletion syndrome region (OMIM 188400)1 (ORPHA:567)2, including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, thymic aplasia/hypoplasia, and immunodeficiency. Aberration is a pathogenic change. | NT = 3.5 mm High risk of Down syndrome |
| 60. | 16p13.11(15048732_16194575)x1,(21)x3 | 1.15 Mbp deletion | Male karyotype, additionally, an interstitial deletion of the short arm of chromosome 16 was found in the 16p13.11 region with a size of ~1.15 Mbp. The aberration involves the 16p13.11 microdeletion syndrome region (ORPHA:261236)1, including 11 protein-coding genes. 16p13.11 deletions have been described in patients mainly with neurodevelopmental disorders (psychomotor development delay, epilepsy, behavioral disorders), microcephaly, short stature, and less frequently with dysmorphic features and congenital defects. The aberration is a potentially pathogenic lesion, characterized by variable expression and incomplete penetrance (13.1%)3 and may be inherited from parents who do not show clinical symptoms. Despite the low penetrance, the aberration was included in the test result due to the presence of trisomy of chromosome 21 of the pair. | NT = 3.6 mm AMA High risk of Down syndrome |
| 61. | 17p12(14111772_15442066)x1 | 1.33 Mbp deletion | Female karyotype, neuropathy, hereditary, with liability to pressure palsies; HNPP(OMIM#162500) | NT = 3.7 mm High risk of Down syndrome |
| 62. | 22q11.21(18894820_21457610)x3 | 2.56 Mbp duplication | Female karyotype, genome imbalance was found in the form of a duplication of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The duplication covers the region of the known microduplication complex 22q11.2 (OMIM: 608363)1. | NT = 3.9 mm AMA, High risk of Down syndrome, |
| 63. | 5p15.33p14.1(22149_27788732)x1, 13q31.2q34(89267673_115093115)x3 | 28 Mbp deletion 26 Mbp duplication | Male karyotype, genome imbalance was found in the form of a deletion of the short arm of chromosome 5 in the 5p15.33p14.1 region of ~28 Mbp and a duplication of the long arm of chromosome 13 in the 13q31.2q34 region of ~26 Mbp. The detected aberrations belong to pathogenic changes. The 5p15.33p14.1 deletion affects 67 protein-coding genes and the 5p deletion syndrome region (OMIM 123450). Patients with this syndrome have been described, among others, with IUGR, characteristic crying, hypotonia, microcephaly, dysmorphic facial features, delay in psychomotor development and intellectual disability. The 13q31.2q34 duplication covers 87 protein-coding genes. Clinical features found in people with distal duplication of chromosome 13q (ORPHA 96105) include: developmental delay, intellectual disability, behavioral disorders, facial dysmorphia, and congenital defects of the nervous, cardiovascular and urogenital systems. | NT = 3.9 mm High risk of Down syndrome |
| 64. | 22q11.21(18765102_20311733)x3,mat | 1.55 Mbp duplication | Female karyotype, genome imbalance was found in the form of a duplication of the long arm of chromosome 22 in the 22q11.21 region with a size of ~1.55 Mbp. The aberration partially involves the region of the known microduplication complex 22q11.2 (OMIM: 608363). | NT = 4.1 mm High risk of Down syndrome |
| 65. | 20p11.23p11.21(19852522_22840889)x1 | 2.99 Mbp deletion | Male karyotype, proximal deletion 20p | NT = 5.2 mm left isomerism,bradycardia |
| 66. | 5p15.33p13.1(22149_40841558)x3, 9p24.3p24.2(204090_2267859)x1 | 41 Mbp duplication 2 Mbp deletion | Female karyotype, genome imbalance was found in the form of a duplication of the short arm of chromosome 5 in the 5p15.33p13.1 region of ~41 Mbp and a deletion of the short arm of the chromosome 9 in the 9p24.3p24.2 region of ~2 Mb. | NT = 4.2 mm High risk of Down syndrome |
| 67. | 3p26.3p26.1(127472_5179975)x3, 6p25.3p25.1(164360_5733668)x1 | 5.05 Mbp duplication 5.57 Mbp deletion | Female karyotype, genome imbalance was found in the form of a duplication of the short arm of chromosome 3 in the 3p26.3p26.1 region of ~5.05 Mbp and a deletion of the short arm of chromosome 6 in the 6p25.3p25.1 region of ~5.57 Mbp. The test result was confirmed by FISH (study no. F2937). | NT = 4.2 mm AMA, HLHS High risk of Down syndrome |
| 68. | 20q13.33(62103563_62908679)x1~2 | 0.805 Mbp deletion | Male karyotype, genome imbalance was found in the form of a mosaic deletion of the long arm of chromosome 20 in the 20q13.33 region with a size of ~805 kb. The deletion covers 33 protein-coding genes, including exon 1 of the dose-sensitive KCNQ2 gene (OMIM 602235)1 and the following genes: EEF1A2 (OMIM 602959)1, RTEL1 (OMIM 608833)1, DNAJC5 (OMIM 611203)1, PRPF6 (OMIM 613979) 1, and SOX18 (OMIM 601618)1. Aberration is a potentially pathogenic change. | NT = 4.3 mm AMA High risk of Down syndrome |
| 69. | 8q11.1q11.21(47456485_51757184)x3 | 4.3 Mbp duplication | Female karyotype, in UNIQUE database reported 8q duplication syndrome: https://www.rarechromo.org/media/information/Chromosome%20%208/8q%20duplications%20FTNW.pdf (accessed on 29 April 2024) | NT = 4.4 mm High risk of Down syndrome |
| 70. | Xp21.1(32006239_32383121)x0 | 377 kb deletion | Male karyotype, genome imbalance was found in the form of a deletion of the long arm of the X chromosome in the Xp21.1 region of ~377 kb. The deletion covers exons 36–44 of the DMD gene (OMIM 300377)1. Mutations and deletions of this gene have been described in patients with Duchenne Muscular Dystrophy (OMIM: 310200)1 and Becker Muscular Dystrophy (OMIM: 300376)1 and may be inherited from mothers, carriers who do not show clinical symptoms | NT = 4.4 mm High risk of Down syndrome |
| 71. | 22q11.21(18894820_21457610)x3 | 2.56 Mbp duplication | Male karyotype, genome imbalance was found in the form of a duplication of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The duplication covers the region of the known microduplication complex 22q11.2 (OMIM: 608363)1. Duplications of this region may present with a wide range of clinical features and may be inherited from asymptomatic parents. | NT = 4.4 mm High risk of Down syndrome |
| 72. | Xp22.31(7145359_7159518)x0 | 0.01 Mb deletion | Male karyotype, Ichthyosis, X-linked (OMIM#308100) | NT = 4.5 mm High risk of Down syndrome |
| 73. | 1p33p32.3(48016425_52280457)x1 | 4.26 Mb deletion | Female karyotype, genome imbalance was found in the form of deletion of the short arm of chromosome 1 in the 1p33p32.3 region with a size of ~4.26 Mbp The deletion covers 15 protein-coding genes, including dose-sensitive genes: AGBL4 (OMIM 616476)1, ELAVL4 (OMIM 168360)1, FAF1 (OMIM 604460)1, CDKN2C (OMIM 603369)1, RNF11 (OMIM 612598)1, EPS15 (OMIM 600051). | NT = 4.5 mm High risk of Down syndrome |
| 74. | 5p15.33p15.32(22149_4768822)x1, 5p15.2(10212960_12513658)x1, 11p15.5p14.1(113082_27880946)x3 | 4.75 Mbp deletion 2.3 Mbp deletion 27.77 Mbp duplication | Male karyotype, genome imbalance was found in the form of a terminal deletion of the short arm of chromosome 5 in the region 5p15.33p15.32 with a size of ~4.75 Mbp and an interstitial deletion of the short arm of chromosome 5 in the region 5p15.2 with a size of ~2.3 Mbp and terminal duplication of the short arm of chromosome 11 in the 11p15.5p14.1 region with a size of ~27.77 Mbp. The 5p15.33p15.32 deletion covers 29 protein-coding genes, including the following genes: SDHA (OMIM 600857)1, SLC9A3 (OMIM 182307)1, TRIP13 (OMIM 604507)1, SLC6A19 (OMIM 608893)1, TERT (OMIM 187270)1, SLC6A3 (OMIM 126455)1, and NDUFS6 (OMIM 603848)1. The 5p15.2 deletion covers 8 protein-coding genes, including CCT5 (OMIM 610150)1 and MARCH6 (OMIM 613297)1. The detected deletions are located in the region of Cri du Chat syndrome (OMIM 123450)1, described in patients including those with microcephaly, growth retardation, characteristic crying in the neonatal/infantile period, dysmorphic facial features, and significant delay in psychomotor development. The duplication in the 11p15.5p14.1 region covers 314 protein-coding genes, as well as the region of Beckwith–Wiedemann syndrome (OMIM 130650)1, described in patients including those with excessive growth, predisposition to cancer and congenital defects, and the region of Silver–Russell syndrome (OMIM 180860)1 described in patients, among others, with short stature, limb asymmetry, and facial dysmorphic features. The detected aberrations belong to pathogenic changes. | NT = 4.65 mm, Hig risk of Down syndrome |
| 75. | 14q32.12q32.33(93833237_107287708)x1 | 13.45 Mbp deletion | Female karyotype, genome imbalance was found in the form of a terminal deletion of the long arm of chromosome 14 in the 14q32.12q32.33 region with a size of ~13.45 Mbp. The aberration affects 201 protein-coding genes, including dose-sensitive genes: DICER1 (OMIM 606241)1, PAPOLA (OMIM 605553)1, YY1 (OMIM 600013)1, HSP90AA1 (OMIM 140571)1, WDR20 (OMIM 617741)1, EIF5 (OMIM 601710)1, and AKT1 (OMIM 164730)1. The deletion covers the region of 14q32 deletion syndrome (IDDHDF, OMIM 618147)1, described in patients including those with developmental delay, hypertelorism, and facial dysmorphic features. Terminal deletions in the 14q32 region have been described in patients with, among others, growth retardation, hypotonia, dysmorphic features, intellectual disability, developmental delay, and heart defects. Aberration is a pathogenic change. | NT = 4.7 mm CHD(VSD), DV PI = 1.4, High risk of Down syndrome |
| 76. | 22q11.21(18628147_21661435)x1 | 3.03 Mbp deletion | Female karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~3.03 Mbp. The deletion covers the 22q11.2 deletion syndrome region (OMIM 188400)1 (ORPHA:567)2, including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, thymic aplasia/hypoplasia, and immunodeficiency1,2.Aberration is a pathogenic change. | NT = 4.7 mm High risk of Down syndrome |
| 77. | 22q11.21(18894820_21457610)x1 | 2.56 Mbp deletion | Female karyotype, genome imbalance was found in the form of an interstitial deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~2.56 Mbp. The deletion covers the 22q11.2 deletion syndrome region (OMIM 188400)1 (ORPHA:567)2, including 52 protein-coding genes. Deletions of this region have been described in patients, among others, with heart defects, anatomical abnormalities of the palate, facial dysmorphic features, developmental delay, thymic aplasia/hypoplasia, and immunodeficiency.Aberration is a pathogenic change. | NT = 4.7 mm TOF High risk of Down syndrome |
| 78. | 22q11.21(18628147_21759580)x1dn | 3.13 Mbp deletion | Female karyotype, genome imbalance was found in the form of a deletion of the long arm of chromosome 22 in the 22q11.21 region with a size of ~ 3.13 Mbp. The deletion covers the region of the known microdeletion syndrome 22q11.2 (OMIM: 188400)1 and is responsible for for abnormalities detected in the fetus during ultrasound examination. | NT = 4.8 mm TOF High risk of Down syndrome |
| 79. | 2p21(44507916_44618832)x1, 12p13.33p13.1(244335_13244974)x3 | 110 kb deletion 13 Mbp duplication | Female karyotype, genome imbalance was found in the form of a deletion of the short arm of chromosome 2 in the 2p21 region of ~110 kb and a duplication of the short arm of chromosome 12 in the 12p13.33p13.1 region of ~13 Mb. The obtained test result indicates that the additional material on chromosome 12 found in the karyotype study comes from the short arm of chromosome 12 (region 12p13.33p13.1). Since karyotypes of the parents were previously performed (outside IMiD), a familial origin of the 12p13.33p13.1 duplication can be ruled out with high probability. However, the 2p21 deletion covers the dose-sensitive PREPL gene (OMIM: 609557)1, exons 2–10 of the SLC3A1 gene (OMIM: 104614)1 and exons 1–3 of the CAMKMT gene (OMIM: 609559)1 and is located in the region of the known 2p21 microdeletion syndrome (OMIM: 606407). | NT = 4.8 mm High risk of Down syndrome |
| 80. | Xp22.31(7226972_7679167)x0 | 0.45 Mbp deletion | Male karyotype, Ichthyosis, X-linked (OMIM#308100) | NT = 5.5 mm megacystis, NB hypoplasia High risk of Down syndrome |
| 81. | 2q13(111646676_113065741)x1mat | 1.42 Mbp deletion | Female karyotype, genome imbalance was found in the form of deletion of the long arm of chromosome 2 in the 2q13 region with a size of ~1.42 Mbp The 2q13 deletion includes the following genes: BCL2L11 (OMIM 603827)1, ANAPC1 (OMIM 608473)1, MERTK (OMIM 604705)1, FBLN7 (OMIM 611551)1, and exons 1–3 of the dose-sensitive ZC3H62. Deletions of this region have been described in patients with heart defects, dysmorphic features, abnormal head circumference, hypotonia, and in some cases also with intellectual disability and autism spectrum disorders. These deletions may be inherited from parents who do not show clinical symptoms. Deletion is a potentially pathogenic change. | NT = 5.7 mm Small head, TR, VSD, abnormal profile High risk of Down syndrome |
| 82. | 3q23q29(141143997_197837049)x3 | 56.7 Mbp duplication | Male karyotype | NT = 5.9 mm DORV High risk of Down syndrome |
| 83. | 10q26.13q26.3(123902691_135404550)x1, 11q23.3q25(120610827_134868420)x3, Xp22.12(19363761_20185740)x2 | 11.5 Mbp deletion 14.26 Mbp duplication 822 kp duplication | Male karyotype, genome imbalance in the form of deletion of the long arm of chromosome 10 in the 10q26.13q26.3 region of ~11.5 Mbp, and duplication of the long arm of the chromosome 11 in the 11q23.3q25 region with a size of ~14.26 Mbp. Additionally, the study found a duplication of the short arm of the X chromosome in the Xp22.12 region With a size of ~822 kb. This duplication includes the following genes: PDHA1 (OMIM: 300502)1, MAP3K16 (OMIM: 300820)1, SH3KBP1 (OMIM: 300374)1, MAP7D22, and exons 17–22 of the dose-sensitive RPS6KA3 gene (OMIM: 300075)1. Duplications in the RPS6KA3 gene have been described in patients with Coffin–Lowry syndrome (OMIM: 303600)1. | NT = 6.6 mm cystic hygroma, abnormal profile, AMA High risk of Down syndrome |
| 84. | 1p36.32p35.3(2558854_29403494)x3 | 26.8 Mbp duplication | Chromosome 1p36.33 duplication syndrome, ATAD3 gene cluster (OMIM#618815) | NT = 7.5 mm hygroma colli |
| 85. | 2p25.3p24.3(21191_13382780)x3, 4p16.3p15.31(45889_20673992)x1 | 13.36 Mbp duplication 20.63 Mbp deletion | Male karyotype, genome imbalance was found in the form of a duplication of the short arm of chromosome 2 in the 2p25.3p24.3 region of ~13.36 Mbp and a deletion of the short arm of chromosome 4 in the 4p16.3p15.31 region of ~20.63 Mbp. | NT = 7.7 mm High risk of Down syndrome |
| 86. | Xq25q28(126504430_152689544)x3, Xq28(152788476_155246643)x1 | 26.19 Mbp duplication 2.46 Mbp deletion | Female karyotype, genome imbalance was found in the form of a duplication of the long arm of the X chromosome in the Xq25q28 region with a size of ~26.19 Mbp and a deletion of the long arm of the X chromosome in the Xq28 region with a size of ~2.46 Mbp. | NT = 8.4 mm Hygroma colli High risk of Down syndrome |
| 87. | 1q43q44(238724105_249203359)x3 dn, 18q22.3q23(70759329_78005754)x1 dn | 10.48 Mbp duplication 7.25 Mbp deletion | Female karyotype, genome imbalance was found in the form of a duplication of the long arm of chromosome 1 in the 1q43q44 region of ~10.48 Mbp and a deletion of the long arm of chromosome 18 in the 18q22.3q23 region of ~7.25 Mbp. | NT = 8.8 mm High risk of Down syndrome |
| NT < p95 n = 754 | NT p95-2.9 mm n = 142 | NT 3.0–3.4 mm n = 229 | NT 3.5–3.9 mm n = 139 | NT 4.0–4.5 mm n = 115 | NT > 4.5 mm n = 367 | |
|---|---|---|---|---|---|---|
| Numerical chromosomal aberrations, n (%) | 45 (5.9) | 24 (16.9) | 43 (18.7) | 32 (23.0) | 34 (29.5) | 159 (43.3) |
| CNVs, n (%) | 22 (3.0) | 4 (2.8) | 8 (3.5) | 6 (4.3) | 14 (12.2) | 33 (9.0) |
| CNVs in fetuses with normal karyotype, (%) | 3.1% | 3.3% | 4.3% | 5.6% | 17.2% | 15.8% |
| With Associated Anomalies | NT < p95 N = 300 | NT p95-2.9 mm N = 68 | NT 3.0–3.4 mm N = 42 | NT 3.5–3.9 mm N = 22 | NT 4.0–4.5 mm N = 27 | NT > 4.5 mm N = 175 |
|---|---|---|---|---|---|---|
| All pathogenic chromosomal aberrations, n (%) | 43 (14.3) | 16 (23.5) | 14 (33.3) | 8 (36.3) | 11 (40.7) | 103 (58.8) |
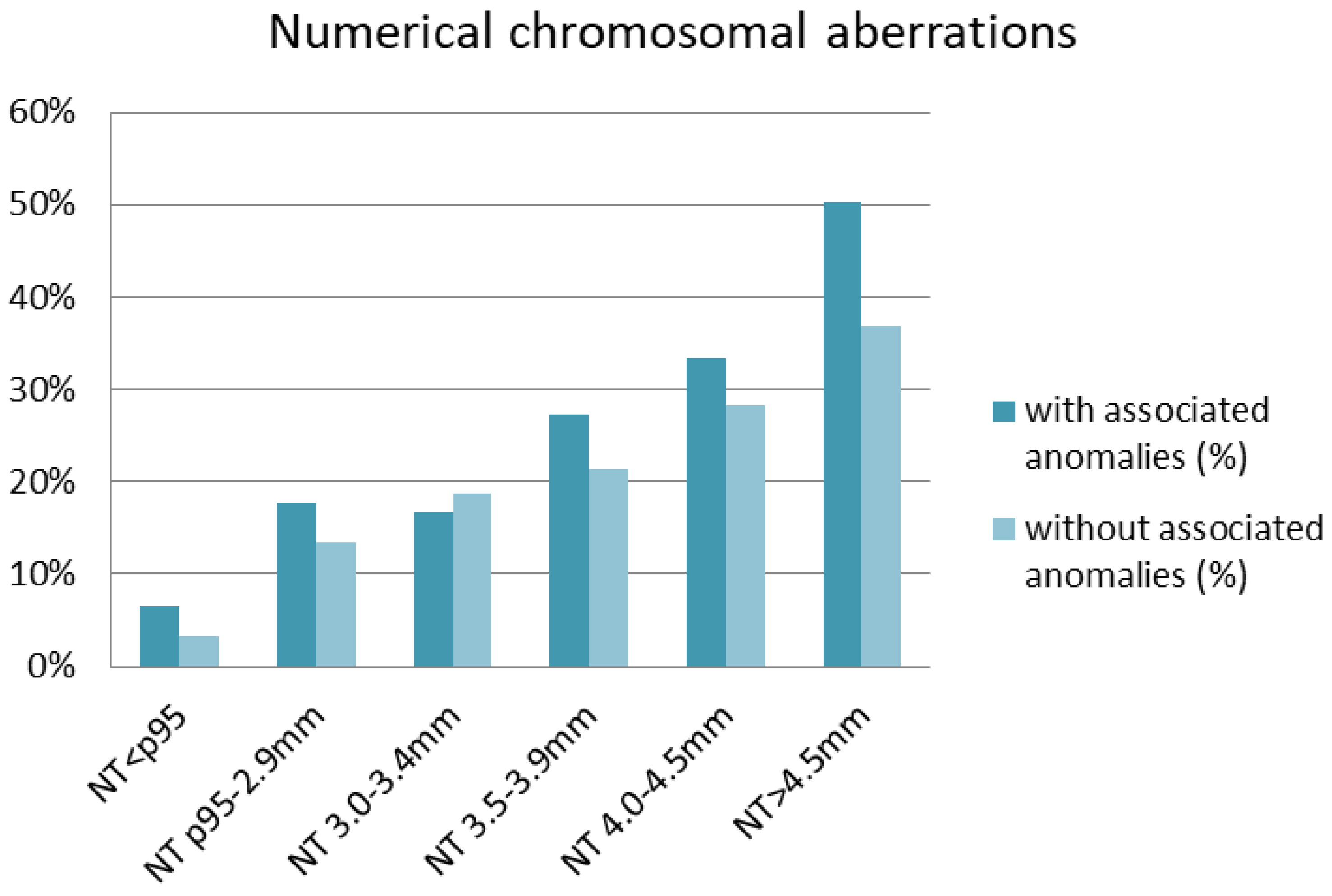
| Numerical chromosomal aberrations, n (%) | 30 (10.0) | 13 (19.1) | 8 (19.0) | 7 (31.8) | 9 (33.3) | 88 (50.2) |
| T21, n (%) | 8 (2.6) | 9 (13.2) | 0 (0.0) | 2 (9.0) | 8 (29.6) | 27 (15.4) |
| T18, n (%) | 7 (2.3) | 1 (1.4) | 4 (9.5) | 3 (13.6) | 1 (3.7) | 23 (13.1) |
| T13, n (%) | 5 (1.6) | 0 (0.0) | 2 (4.7) | 1 (4.5) | 0 (0.0) | 11 (6.3) |
| 45XO, n (%) | 1 (0.3) | 1 (1.4) | 1 (2.4) | 0 (0.0) | 0 (0.0) | 27 (15.4) |
| 47,XXX; 47,XXY, n (%) | 1 (0.3) | 1 (1.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Triploidy, n (%) | 8 (2.6) | 1 (1.4) | 1 (1.4) | 1 (1.4) | 0 (0.0) | 0 (0.0) |
| CNVs, n (%) | 13 (4.3) | 3 (4.4) | 6 (14.3) | 1 (4.5) | 2 (7.4) | 15 (8.6) |
| CNVs in fetuses with normal karyotype, (%) | 4.8 | 5.4 | 17.6 | 6.6 | 11.1 | 17.2 |
| Without associated anomalies, n | NT < p95 N = 454 | NT p95-2.9 mm N = 74 | NT 3.0–3.4 mm N = 187 | NT 3.5–3.9 mm N = 117 | NT 4.0–4.5 mm N = 88 | NT > 4.5 mm N = 192 |
| All pathogenic chromosomal aberrations, n (%) | 24 (5.3) | 12 (16.2) | 37 (19.8) | 30 (25.6) | 37 (42.0) | 89 (46.3) |
| Numerical chromosomal aberrations, n (%) | 15 (3.3) | 11 (14.8) | 35 (18.7) | 25 (21.3) | 25 (28.4) | 71 (36.9) |
| T21, n (%) | 9 (2.0) | 7 (9.4) | 31 (16.6) | 19 (16.2) | 20 (22.7) | 35 (18.2) |
| T18, n (%) | 0 (0.0) | 0 (0.0) | 1 (0.5) | 3 (2.5) | 1 (1.1) | 13 (6.7) |
| T13, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (2.2) | 3 (1.5) |
| 45X0, n (%) | 2 (0.4) | 0 (0.0) | 3 (1.5) | 3 (2.5) | 2 (2.2) | 19 (9.9) |
| 47,XXX; 47,XXY, n (%) | 4 (0.8) | 3 (4.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.5) |
| Triploidy, n (%) | 0 (0.0) | 0 | 0 | 0 | 0 | 0 |
| CNVs, n (%) | 9 (2.0) | 1 (1.3) | 2 (1.0) | 5 (4.3) | 12 (13.6) | 18 (9.3) |
| CNVs in fetuses with normal karyotype, (%) | 2.0 | 1.5 | 1.3 | 5.4 | 19.0 | 14.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wójtowicz, A.; Kowalczyk, K.; Szewczyk, K.; Madetko-Talowska, A.; Wójtowicz, W.; Huras, H.; Bik-Multanowski, M.; Beata, N. Array Comparative Genomic Hybridization (aCGH) Results among Patients Referred to Invasive Prenatal Testing after First-Trimester Screening: A Comprehensive Cohort Study. Diagnostics 2024, 14, 2186. https://doi.org/10.3390/diagnostics14192186
Wójtowicz A, Kowalczyk K, Szewczyk K, Madetko-Talowska A, Wójtowicz W, Huras H, Bik-Multanowski M, Beata N. Array Comparative Genomic Hybridization (aCGH) Results among Patients Referred to Invasive Prenatal Testing after First-Trimester Screening: A Comprehensive Cohort Study. Diagnostics. 2024; 14(19):2186. https://doi.org/10.3390/diagnostics14192186
Chicago/Turabian StyleWójtowicz, Anna, Katarzyna Kowalczyk, Katarzyna Szewczyk, Anna Madetko-Talowska, Wojciech Wójtowicz, Hubert Huras, Mirosław Bik-Multanowski, and Nowakowska Beata. 2024. "Array Comparative Genomic Hybridization (aCGH) Results among Patients Referred to Invasive Prenatal Testing after First-Trimester Screening: A Comprehensive Cohort Study" Diagnostics 14, no. 19: 2186. https://doi.org/10.3390/diagnostics14192186