
Eyes as Windows: Unveiling Neuroinflammation in Multiple Sclerosis via Optic Neuritis and Uhthoff’s Phenomenon

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical and Demographic Characteristics
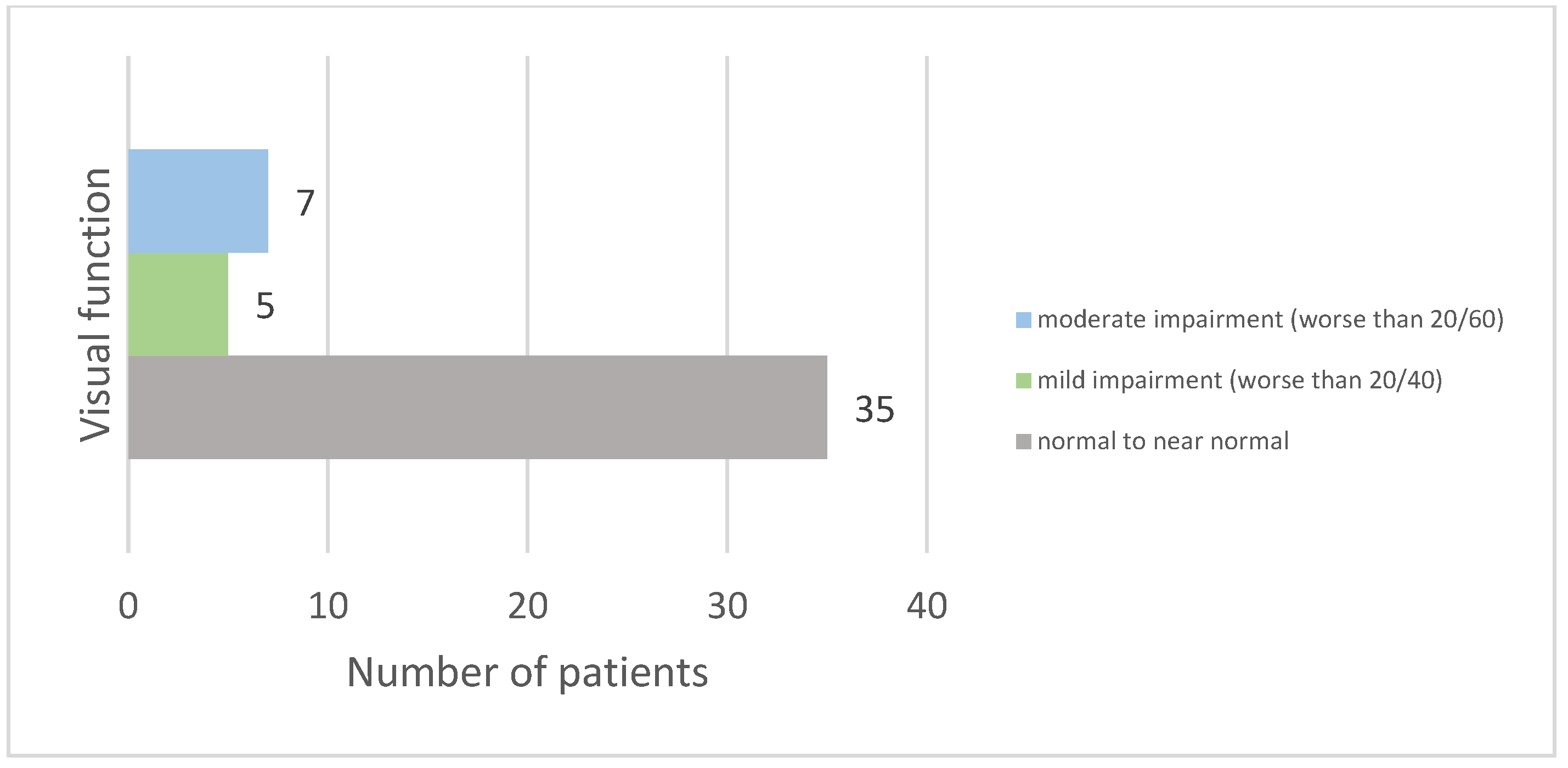
3.2. Optic Neuritis Characteristics
3.3. Uhthoff Phenomenon and Lhermitte’s Sign
4. Discussion
4.1. Optic Neuritis in Multiple Sclerosis
4.2. Uhthoff’s Phenomenon and Lhermitte Sign
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sormani, M.P.; Naismith, R.T. Measuring disability in multiple sclerosis: Walking plus much more. Neurology 2019, 93, 919–920. [Google Scholar] [CrossRef] [PubMed]
- MS International Federation. Atlas of MS 2020—Epidemiology Report. Available online: https://www.msif.org/resource/atlas-of-ms-2020/ (accessed on 10 November 2022).
- Ford, H. Clinical presentation and diagnosis of multiple sclerosis. Clin. Med. 2020, 20, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Brass, S.D.; Zivadinov, R.; Bakshi, R. Acute demyelinating optic neuritis: A review. Front. Biosci. 2008, 13, 2376–2390. [Google Scholar] [CrossRef] [PubMed]
- Sîrbu, C.A.; Drăgoi, C.M.; Nicolae, A.C.; Plesa, F.C. History of interferon treatments in multiple sclerosis–60 years of progress. Farmacia 2017, 65, 14–18. [Google Scholar]
- Costa Novo, J.; Felgueiras, H. Neuro-ophthalmologic manifestations of multiple sclerosis other than acute optic neuritis. Mult. Scler. Relat. Disord. 2021, 48, 102730. [Google Scholar] [CrossRef]
- Nerrant, E.; Tilikete, C. Ocular motor manifestations of multiple sclerosis. J. Neuro-Ophthalmol. 2017, 37, 332–340. [Google Scholar] [CrossRef]
- Liu, J.; O’Connor, P. Optic Neuritis: Pathophysiology, Clinical Features, and Diagnosis. In UpToDate; O’Connor, P., Ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2024. [Google Scholar]
- Ghelmez, D.; Moraru, A.; Antonescu, F.; Chelmambet, A.; Bucur, A.; Sorin, T. Double seropositive neuromyelitis optica associated with COVID-19: A case report. Front. Neurol. 2022, 13, 1004132. [Google Scholar] [CrossRef]
- Sguigna, P.V.; Meltzer, E. The Evolution of Myelin Oligodendrocyte Glycoprotein Antibody–Associated Disease. Pract. Neurol. Mult. Scler. Expand. Field Beyond Manag. 2023, 3, 38–51. [Google Scholar]
- Leavitt, V.M.; Cirnigliaro, C.; Cohen, A.; Amato, M.P. Uhthoff’s Phenomenon in Multiple Sclerosis: Clinical Features and Pathophysiology. Mult. Scler. J. Exp. Transl. Clin. 2020, 6, 2055217320915704. [Google Scholar]
- Panginikkod, S. Uhthoff Phenomenon. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470244/ (accessed on 24 October 2022).
- Teoli, D.; Rocha Cabrero, F.; Smith, T.; Ghassemzadeh, S. Lhermitte Sign. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK493237/ (accessed on 12 March 2024).
- Etemadifar, M.; Mehrbod, N.; Dehghani, L.; Golabbakhsh, A.; Fereidan-Esfahani, M.; Akbari, M.; Nasr, Z. Prevalence of Lhermitte’s sign in multiple sclerosis versus neuromyelitis optica. Iran. J. Neurol. 2014, 13, 50–51. [Google Scholar]
- Foley, P.; Vesterinen, H.M.; Laird, B.J.; Sena, E.S.; Colvin, L.A.; Chandran, S.; MacLeod, M.R.; Fallon, M.T. Prevalence and natural history of pain in adults with multiple sclerosis: Systematic review and meta-analysis. Pain 2013, 154, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Klineova, S.; Lublin, F.D. Clinical Course of Multiple Sclerosis. Cold Spring Harb. Perspect. Med. 2018, 8, a028928. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.L.; Cree, B.A.C. Treatment of Multiple Sclerosis: A Review. Am. J. Med. 2020, 133, 1380–1390.e2. [Google Scholar] [CrossRef]
- Füvesi, J. The Expanded Disability Status Scale scoring in patients with multiple sclerosis. Ideggyogy. Sz. 2019, 72, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Yanoff, M.; Duker, J.S. Ophthalmology; Elsevier: Amsterdam, The Netherlands, 2023. [Google Scholar]
- Ciapă, M.A.; Șalaru, D.L.; Stătescu, C.; Sascău, R.A.; Bogdănici, C.M. Optic neuritis in multiple sclerosis—A review of molecular mechanisms involved in the degenerative process. Curr. Issues Mol. Biol. 2022, 44, 3959–3979. [Google Scholar] [CrossRef] [PubMed]
- Baecher-Allan, C.; Kaskow, B.J.; Weiner, H.L. Multiple Sclerosis: Mechanisms and Immunotherapy. Neuron 2018, 97, 742–768. [Google Scholar] [CrossRef]
- Dulamea, A.O. The contribution of oligodendrocytes and oligodendrocyte progenitor cells to central nervous system repair in multiple sclerosis: Perspectives for remyelination therapeutic strategies. Neural Regen. Res. 2017, 12, 1939–1944. [Google Scholar] [CrossRef]
- Franklin, R.J.M.; Goldman, S.A. Glia Disease and Repair-Remyelination. Cold Spring Harb. Perspect. Biol. 2015, 7, a020594. [Google Scholar] [CrossRef]
- Guier, C.P.; Stokkermans, T.J. Optic Neuritis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557853/ (accessed on 3 January 2024).
- Kale, N. Optic neuritis as an early sign of multiple sclerosis. Eye Brain 2016, 8, 195–202. [Google Scholar] [CrossRef]
- Toosy, A.T.; Mason, D.F.; Miller, D.H. Optic neuritis. Lancet Neurol. 2014, 13, 83–99. [Google Scholar] [CrossRef]
- Optic Neuritis Study Group. Multiple sclerosis risk after optic neuritis: Final optic neuritis treatment trial follow-up. Arch. Neurol. 2008, 65, 727–732. [Google Scholar]
- Sørensen, T.L.; Frederiksen, J.L.; Brønnum-Hansen, H.; Petersen, H.C. Optic neuritis as onset manifestation of multiple sclerosis: A nationwide, long-term survey. Neurology 1999, 53, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.W.; Cleary, P.A.; Nerve, S.M.; Foroozan, R. Visual function more than 10 years after optic neuritis: Experience of the optic neuritis treatment trial. Am. J. Ophthalmol. 2004, 137, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Shaygannejad, V.; Abtahi, S.; Nikseresht, M.; Khodadadi, M. Color blindness among multiple sclerosis patients in Isfahan. J. Res. Med. Sci. 2012, 17, 254–257. [Google Scholar] [PubMed]
- Robertson, D.; Moreo, N. Disease-Modifying Therapies in Multiple Sclerosis: Overview and Treatment Considerations. Fed. Pract. 2016, 33, 28–34. [Google Scholar] [PubMed]
- Shah, P. Symptomatic management in multiple sclerosis. Ann. Indian. Acad. Neurol. 2015, 18 (Suppl. 1), S35–S42. [Google Scholar] [CrossRef]
- Sîrbu, C.A.; Tăbăran, F.A.; Păcurar, R.; Mihăilescu, R.; Ardelean, S. Cannabis and cannabinoids in multiple sclerosis: From experimental models to clinical practice—A review. Am. J. Ther. 2023, 30, e220–e231. [Google Scholar] [CrossRef]
- Weld-Blundell, I.V.; Lazzarini, S.; Jeyakumar, M.; White, A.C.; Baker, J.F. Lifestyle and complementary therapies in multiple sclerosis guidelines: Systematic review. Acta Neurol. Scand. 2022, 145, 379–392. [Google Scholar] [CrossRef]
- Alberti, T.B.; Barbosa, W.L.R.; Vieira, J.L.F.; Raposo, N.R.B.; Dutra, R.C. (−)-β-Caryophyllene, a CB2 Receptor-Selective Phytocannabinoid, Suppresses Motor Paralysis and Neuroinflammation in a Murine Model of Multiple Sclerosis. Int. J. Mol. Sci. 2017, 18, 691. [Google Scholar] [CrossRef]
- Sîrbu, C.A.; Plesa, F.C.; Rusu, D.S.; Ardelean, S.; Stefan, C. Neurorehabilitation in multiple sclerosis—A review of present approaches and future considerations. J. Clin. Med. 2022, 11, 7003. [Google Scholar] [CrossRef]
- Amatya, B.; Khan, F.; Galea, M. Rehabilitation for people with multiple sclerosis: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 1, CD012732. [Google Scholar] [CrossRef] [PubMed]
- Frohman, E.M.; Davis, S.L.; Beh, S.C.; Greenberg, B.M.; Remington, G.; Frohman, T.C. Uhthoff’s phenomena in MS—Clinical features and pathophysiology. Nat. Rev. Neurol. 2013, 9, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Howells, J.; Czesnik, D.; Trevillion, L.; Burke, D. Excitability and the safety margin in human axons during hyperthermia. J. Physiol. 2013, 591, 3063–3080. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Smith, M.T. Multiple sclerosis-induced neuropathic pain: Pharmacological management and pathophysiological insights from rodent EAE models. Inflammopharmacology 2014, 22, 1–22. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demyelinating | Infections | Inflammatory | Others |
|---|---|---|---|
|
|
|
|
| ON Features | MS | NMOSD | MOGAD |
|---|---|---|---|
| Bilateral presentation | rare | common | common |
| Visual acuity impairment | mild to moderate | moderate to severe | moderate to severe |
| Ocular pain | common | rare | common |
| Optic nerve involvement | segmental (<50% of optic nerve) | extensive (>50% of optic nerve) | extensive (>50% of optic nerve) |
| Optic chiasm involvement | infrequent | common | uncommon |
 |  |  | |
| Perineuritis | absent or mild | less common | common |
| RNFL measured via OCT | typically normal in acute phase | typically normal in acute phase | acutely thickening |
| Relapse recovery | intermediate | generally poor | usually good |
| Category | Specific Causes |
|---|---|
| Demyelinating Diseases | MS, NMOSD |
| Autoimmune Disorders | Antiphospholipid antibody syndrome, Behçet’s disease, CNS lupus, CNS vasculitis, Sjogren’s syndrome |
| Infectious Diseases | HIV, HTLV, Lyme disease |
| Hematologic Conditions | CNS lymphoma |
| Nutritional Deficiencies | Copper deficiency |
| Genetic Disorders | Leukodystrophies |
| Vascular Disorders | Small vessel disease |
| Other Conditions | Sarcoidosis, osmotic demyelination syndrome |
| Category | Specific Causes |
|---|---|
| Demyelinating Diseases | MS |
| Autoimmune Disorders | Transverse myelitis, CNS lupus, Behçet’s disease |
| Infectious Diseases | Herpes zoster toxicity, parasitic invasion of the cord |
| Nutritional Deficiencies | Vitamin B12 deficiency |
| Toxic/Drug-related | Radiation myelopathy, high dose chemoradiation (cisplatin), nitric oxide toxicity |
| Mechanical/Structural | Tumor, radiculopathy, cervical spondylitis, Arnold–Chiari malformation, syringomyelia, trauma, arachnoiditis, post-dural puncture headache |
| Parameter | Group 1—Patients with ON N = 47 | Group 2—Patients without ON N = 80 | p Value | |
|---|---|---|---|---|
| Age | Mean age ± SD | 41.87 ± 11.958 years | 44.44 ± 10.918 years | 0.223 (NS) |
| Gender N, % | Male | 12 (26%) | 25 (31%) | 0.557 (NS) |
| Female | 35 (74%) | 55 (69%) | ||
| Residency | Urban | 37 (79%) | 69 (86%) | 0.273 (NS) |
| Rural | 10 (21%) | 11 (14%) | ||
| MS age of onset | Mean age of onset ± SD | 31.60 ± 9.380 years | 35.76 ± 10.511 years | 0.039 (S) |
| Type of MS | Recurrent remissive | 45 (96%) | 65 (81%) | 0.132 (NS) |
| Primary progressive | 0 (0%) | 8 (10%) | ||
| Secondary progressive | 2 (4%) | 6 (9%) | ||
| EDSS score | Mean EDSS ± SD | 2.20 ± 1.51 | 2.35 ± 1.801 | 0.639 (NS) |
| Treatment | Beta-interferon | 18 (38%) | 18 (23%) | - |
| Ocrelizumab | 7 (15%) | 18 (23%) | ||
| Teriflunomide | 5 (11%) | 13 (16%) | ||
| Natalizumab | 5 (11%) | 6 (8%) | ||
| Glatiramer acetate | 4 (9%) | 3 (4%) | ||
| Cladribine | 4 (9%) | 6 (8%) | ||
| Dimethyl fumarate | 2 (4%) | 7 (9%) | ||
| Fingolimod | 1 (2%) | 5 (6%) | ||
| Siponimod | 1 (2%) | 4 (5%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pleșa, A.; Antochi, F.A.; Macovei, M.L.; Vîrlan, A.-G.; Georgescu, R.; Beuran, D.-I.; Bucurica, S.N.; Sîrbu, C.A.; Axelerad, A.; Pleșa, F.C. Eyes as Windows: Unveiling Neuroinflammation in Multiple Sclerosis via Optic Neuritis and Uhthoff’s Phenomenon. Diagnostics 2024, 14, 2198. https://doi.org/10.3390/diagnostics14192198
Pleșa A, Antochi FA, Macovei ML, Vîrlan A-G, Georgescu R, Beuran D-I, Bucurica SN, Sîrbu CA, Axelerad A, Pleșa FC. Eyes as Windows: Unveiling Neuroinflammation in Multiple Sclerosis via Optic Neuritis and Uhthoff’s Phenomenon. Diagnostics. 2024; 14(19):2198. https://doi.org/10.3390/diagnostics14192198
Chicago/Turabian StylePleșa, Andreea, Florina Anca Antochi, Mioara Laura Macovei, Alexandra-Georgiana Vîrlan, Ruxandra Georgescu, David-Ionuț Beuran, Săndica Nicoleta Bucurica, Carmen Adella Sîrbu, Any Axelerad, and Florentina Cristina Pleșa. 2024. "Eyes as Windows: Unveiling Neuroinflammation in Multiple Sclerosis via Optic Neuritis and Uhthoff’s Phenomenon" Diagnostics 14, no. 19: 2198. https://doi.org/10.3390/diagnostics14192198
APA StylePleșa, A., Antochi, F. A., Macovei, M. L., Vîrlan, A.-G., Georgescu, R., Beuran, D.-I., Bucurica, S. N., Sîrbu, C. A., Axelerad, A., & Pleșa, F. C. (2024). Eyes as Windows: Unveiling Neuroinflammation in Multiple Sclerosis via Optic Neuritis and Uhthoff’s Phenomenon. Diagnostics, 14(19), 2198. https://doi.org/10.3390/diagnostics14192198