
Validation of Fixed Ultrasonography for Achilles Tendon Assessment: A Reliability Study

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Population
2.3. Procedure
2.4. Protocol Scanning
2.5. Statistical Analysis
3. Results
3.1. Sample Description
3.2. Ultrasound Data
3.3. Reliability
3.4. Inter-Rater Reliability
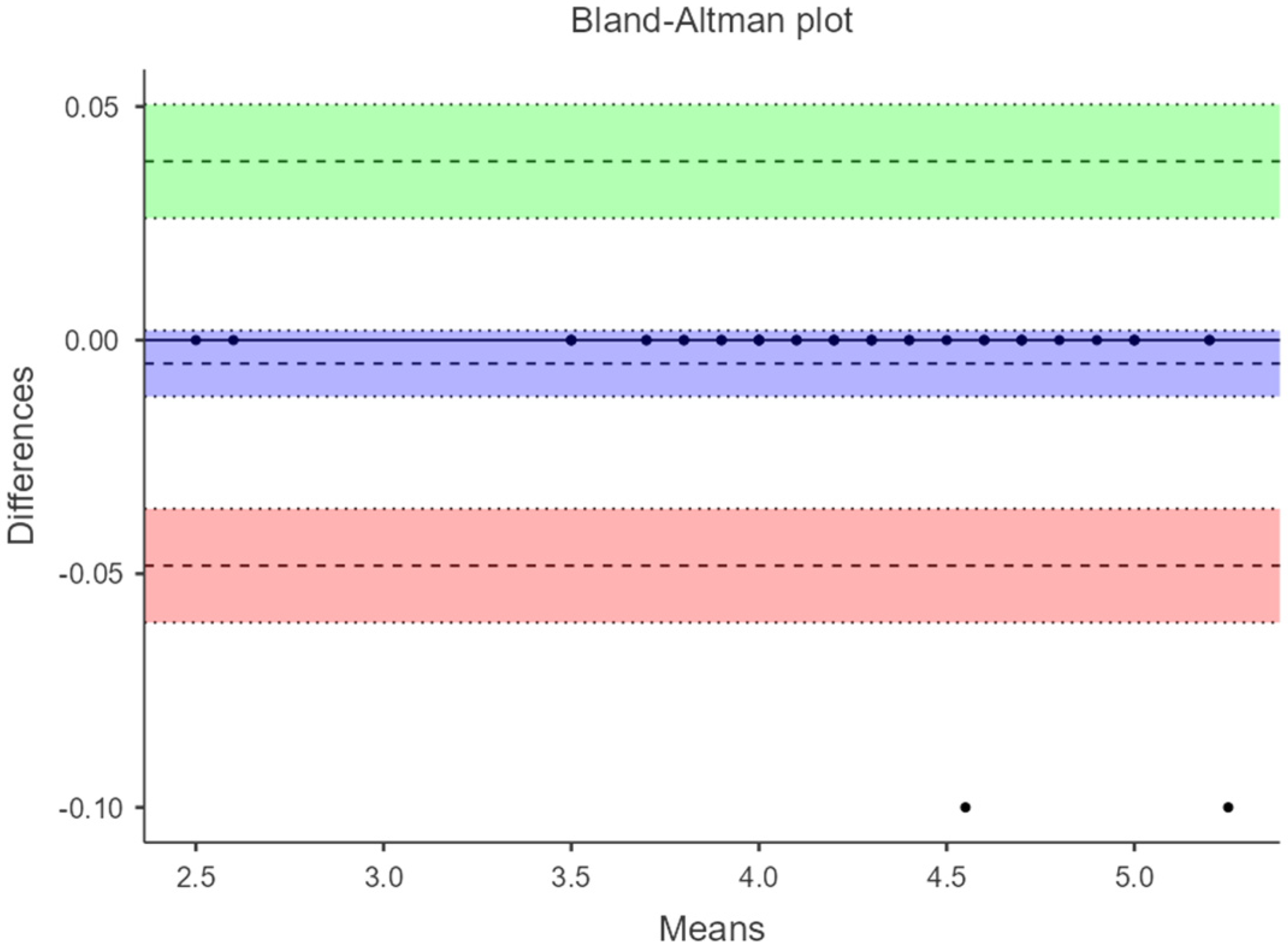
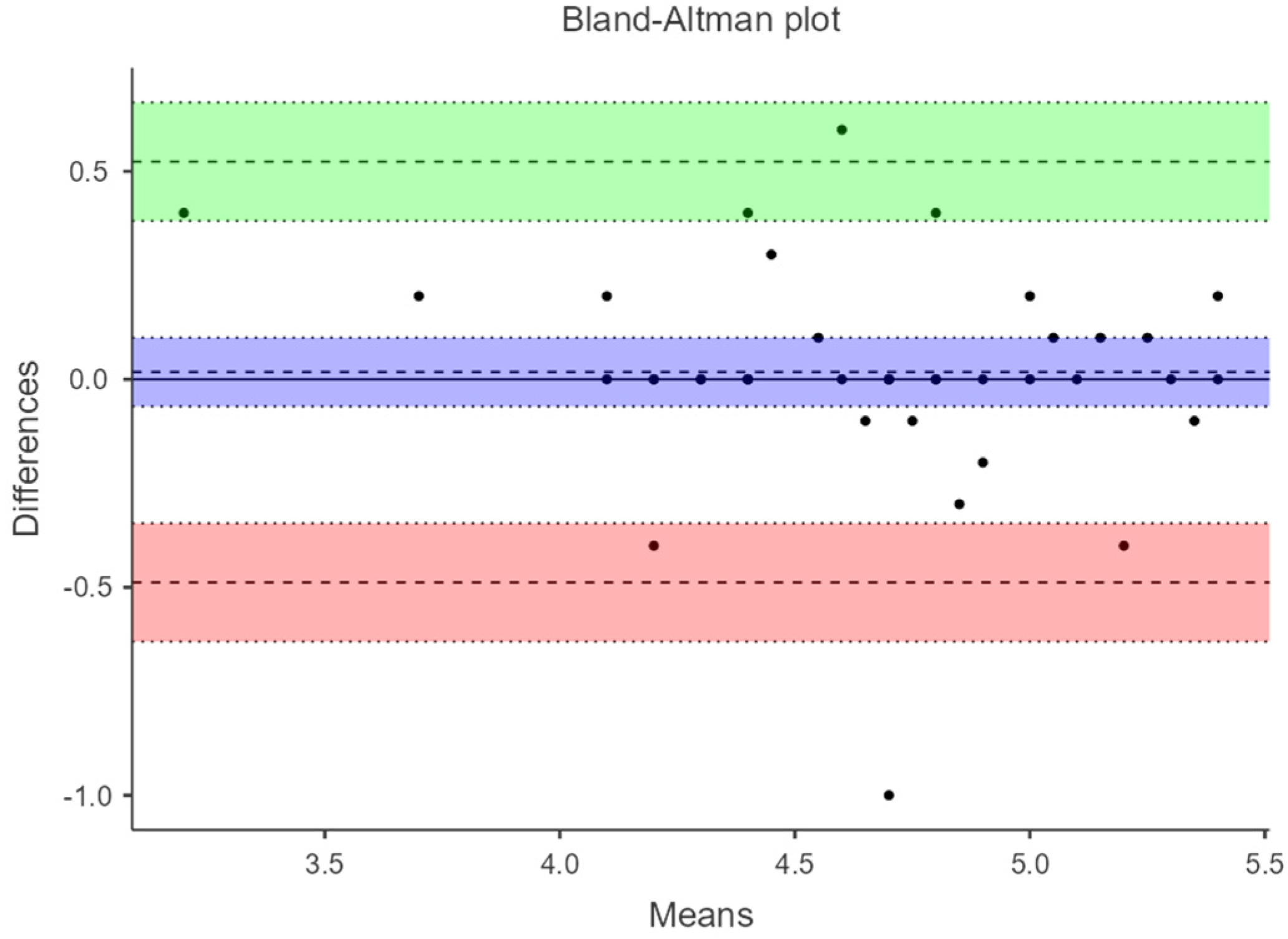
3.5. Bland–Altman Plots
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- French, C.N.; Walker, E.A.; Phillips, S.F.; Loeffert, J.R. Ultrasound in Sports Injuries. Clin. Sports Med. 2021, 40, 801–819. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N. Overuse tendon conditions: Time to change a confusing terminology. Arthrosc. J. Arthrosc. Relat. Surg. 1998, 14, 840–843. [Google Scholar] [CrossRef] [PubMed]
- Uquillas, C.A.; Guss, M.S.; Ryan, D.J.; Jazrawi, L.M.; Strauss, E.J. Everything Achilles: Knowledge Update and Current Concepts in Management. J. Bone Jt. Surg. 2015, 97, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Hagoort, I.; Hortobágyi, T.; Vuillerme, N.; Lamoth, C.J.C.; Murgia, A. Age- and muscle-specific reliability of muscle architecture measurements assessed by two-dimensional panoramic ultrasound. Biomed. Eng. Online 2022, 21, 15. [Google Scholar] [CrossRef] [PubMed]
- Heres, H.M.; Sjoerdsma, M.; Schoots, T.; Rutten, M.C.M.; van de Vosse, F.N.; Lopata, R.G.P. Image acquisition stability of fixated musculoskeletal sonography in an exercise setting: A quantitative analysis and comparison with freehand acquisition. J. Med Ultrason. 2020, 47, 47–56. [Google Scholar] [CrossRef]
- Gao, J.; Rosander, A.; Rubin, J.M. Quantitative Assessment of Tendon Backscatter Anisotropy in B-Mode Ultrasound. Ultrasound Med. Biol. 2023, 49, 1408–1414. [Google Scholar] [CrossRef]
- Van Schie, H.T.; de Vos, R.J.; de Jonge, S.; Bakker, E.M.; Heijboer, M.P.; Verhaar, J.A.; Tol, J.L.; Weinans, H. Ultrasonographic tissue characterisation of human Achilles tendons: Quantification of tendon structure through a novel non-invasive approach. Br. J. Sports Med. 2010, 44, 1153–1159. [Google Scholar] [CrossRef]
- Daftary, A.; Adler, R.S. Sonographic Evaluation and Ultrasound-Guided Therapy of the Achilles Tendon. Ultrasound Q. 2009, 25, 103–110. [Google Scholar] [CrossRef]
- Alabau-Dasi, R.; Dominguez-Maldonado, G.; Gijon-Nogueron, G.; Ortega-Avila, A.B.; Delacroix, S. How susceptible are our Achilles Tendons? Sonoanatomical assessment. A cross-sectional study. J. Tissue Viability 2023, 32, 572–576. [Google Scholar] [CrossRef]
- Fukunaga, T.; Ichinose, Y.; Ito, M.; Kawakami, Y.; Fukashiro, S. Determination of fascicle length and pennation in a contracting human muscle in vivo. J. Appl. Physiol. 1997, 82, 354–358. [Google Scholar] [CrossRef]
- Färnqvist, K.; Pearson, S.; Malliaras, P. Adaptation of Tendon Structure and Function in Tendinopathy With Exercise and Its Relationship to Clinical Outcome. J. Sport Rehabil. 2020, 29, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Rabusin, C.L.; Menz, H.B.; McClelland, J.A.; Evans, A.M.; Malliaras, P.; Docking, S.I.; Landorf, K.B.; Gerrard, J.M.; E. Munteanu, S. Efficacy of heel lifts versus calf muscle eccentric exercise for mid-portion Achilles tendinopathy (HEALTHY): A randomised trial. Br. J. Sports Med. 2021, 55, 486–492. [Google Scholar] [CrossRef]
- Shivapatham, G.; Richards, S.; Bamber, J.; Screen, H.; Morrissey, D. Ultrasound Measurement of Local Deformation in the Human Free Achilles Tendon Produced by Dynamic Muscle-Induced Loading: A Systematic Review. Ultrasound Med. Biol. 2023, 49, 1499–1509. [Google Scholar] [CrossRef]
- Fredberg, U.; Bolvig, L.; Andersen, N.T.; Stengaard-Pedersen, K. Ultrasonography in Evaluation of Achilles and Patella Tendon Thickness. Ultraschall Der Med.-Eur. J. Ultrasound 2007, 29, 60–65. [Google Scholar] [CrossRef]
- Hutchison, A.-M.; Evans, R.; Bodger, O.; Pallister, I.; Topliss, C.; Williams, P.; Vannet, N.; Morris, V.; Beard, D. What is the best clinical test for Achilles tendinopathy? Foot Ankle Surg. 2013, 19, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Reiman, M.; Burgi, C.; Strube, E.; Prue, K.; Ray, K.; Elliott, A.; Goode, A. The Utility of Clinical Measures for the Diagnosis of Achilles Tendon Injuries: A Systematic Review With Meta-Analysis. J. Athl. Train. 2014, 49, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Bohm, S.; Mersmann, F.; Schroll, A.; Mäkitalo, N.; Arampatzis, A. Insufficient accuracy of the ultrasound-based determination of Achilles tendon cross-sectional area. J. Biomech. 2016, 49, 2932–2937. [Google Scholar] [CrossRef]
- Nadeau, M.; Desrochers, A.; Lamontagne, M.; Larivière, C.; Gagnon, D.H. Quantitative ultrasound imaging of Achilles tendon integrity in symptomatic and asymptomatic individuals: Reliability and minimal detectable change. J. Foot Ankle Res. 2016, 9, 30. [Google Scholar] [CrossRef]
- Bennell, K.; Talbot, R.; Wajswelner, H.; Techovanich, W.; Kelly, D.; Hall, A. Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsiflexion. Aust. J. Physiother. 1998, 44, 175–180. [Google Scholar] [CrossRef]
- Ríos-Díaz, J.; Martínez-Payá, J.J.; del Baño-Aledo, M.E.; de Groot-Ferrando, A.; Botía-Castillo, P.; Fernández-Rodríguez, D. Sonoelastography of Plantar Fascia: Reproducibility and Pattern Description in Healthy Subjects and Symptomatic Subjects. Ultrasound Med. Biol. 2015, 41, 2605–2613. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zhang, Y.-Z.; Gao, Y.; Luo, T.-Y. Assessment the reliability of ultrasonography in the imaging of the plantar fascia: A comparative study. BMC Med. Imaging 2019, 19, 62. [Google Scholar] [CrossRef] [PubMed]
- Barfod, K.W.; Riecke, A.F.; Anders, B.; Hansen, P.; Maier, J.F.; Døssing, S.; Troelsen, A. Validity and reliability of an ultrasound measurement of the free length of the Achilles tendon. Dan Med. J. 2018, 65, A5453. [Google Scholar]
- Alabau-Dasi, R.; Nieto-Gil, P.; Ortega-Avila, A.B.; Gijon-Nogueron, G. Variations in the Thickness of the Plantar Fascia After Training Based in Training Race. A Pilot Study. J. Foot Ankle Surg. 2022, 61, 1230–1234. [Google Scholar] [CrossRef]
- Ying, M.; Yeung, E.; Li, B.; Li, W.; Lui, M.; Tsoi, C.-W. Sonographic evaluation of the size of achilles tendon: The effect of exercise and dominance of the ankle. Ultrasound Med. Biol. 2003, 29, 637–642. [Google Scholar] [CrossRef]
- O’connor, P.J.; Grainger, A.J.; Morgan, S.R.; Smith, K.L.; Waterton, J.C.; Nash, A.F.P. Ultrasound assessment of tendons in asymptomatic volunteers: A study of reproducibility. Eur. Radiol. 2004, 14, 1968–1973. [Google Scholar] [CrossRef]
- Pang, B.S.F.; Ying, M. Sonographic Measurement of Achilles Tendons in Asymptomatic Subjects. J. Ultrasound Med. 2006, 25, 1291–1296. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Del Bano-Aledo, M.E.; Martinez-Paya, J.J.; Rios-Diaz, J.; Mejias-Suarez, S.; Serrano-Carmona, S.; de Groot-Ferrando, A. Ultrasound measures of tendon thickness: Intra-rater, Inter-rater and Inter-machine reliability. Muscle Ligaments Tendons J. 2017, 7, 192–199. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Zhou, H.-H.; Nie, Z.; Cui, S. Prevalence of Achilles tendinopathy in physical exercise: A systematic review and meta-analysis. Sports Med. Health Sci. 2022, 4, 152–159. [Google Scholar] [CrossRef]
- Lewis, R.; Álvarez, C.B.G.; Rayman, M.; Lanham-New, S.; Woolf, A.; Mobasheri, A. Strategies for optimising musculoskeletal health in the 21st century. BMC Musculoskelet. Disord. 2019, 20, 164. [Google Scholar] [CrossRef] [PubMed]
- Nuri, L.; Obst, S.J.; Newsham-West, R.; Barrett, R.S. Three-dimensional morphology and volume of the free Achilles tendon at rest and under load in people with unilateral mid-portion Achilles tendinopathy. Exp. Physiol. 2018, 103, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Bruno, F.; Arrigoni, F.; Palumbo, P.; Natella, R.; Splendiani, A.; Di Cesare, E.; Guglielmi, G.; Masciocchi, C.; Barile, A. Weight-bearing MR Imaging of Knee, Ankle and Foot. Semin. Musculoskelet. Radiol. 2019, 23, 594–602. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender (n) | Age (y) (Mean/SD) | Weight (k) (Mean/SD) | Height (cm) (Mean/SD) | BMI (Mean/SD) |
|---|---|---|---|---|
| Male (6) | 22.5 ± 3.12 | 79.8 ± 13.91 | 167 ±6.79 | 25.1 ± 2.99 |
| Female (14) | 22.6 ± 1.95 | 63.8 ± 6.94 | 178 ± 6.16 | 23 ± 2.77 |
| Total (20) | 22.55 ± 2.32 | 68.6 ± 12.51 | 170 ± 8.07 | 23.61 ± 2.97 |
| Intra-Rater | Inter-Rater | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | US Acquisition | Examiner 1 | Examiner 2 | Mean (SD) 95% CI | α Cronbach | * Mean Difference 95% LOA | ||
| Mean (SD) 95% CI | Mean (SD) 95% CI | ICC(1-1) (95% CI) | p-Value | |||||
| 4 cm At rest | manual acquisition | 4.50 (0.54) | 4.49 (0.60) | 0.91 (0.86–0.95) | <0.001 | 4.51 (0.528) | 0.998 | 0.005 (−0.104 to 0.094) |
| 6 cm At rest | manual acquisition | 4.63 (0.455) | 4.66 (0.611) | 0.895 (0.861–0.945) | <0.001 | 4.63 (0.450) | 0.996 | 0.02 (−0.0905 to 0.13) |
| 4 cm At rest | fixed ultrasonography | 4.58 (0.556) | 4.66 (0.579) | 0.926 (0.882–0.957) | <0.001 | 4.58 (0.543) | 0.997 | 0.000 (−0.109 to 0.109) |
| 6 cm At rest | fixed ultrasonography | 4.67 (0.461) | 4.66 (0.510) | 0.909 (0.861–0.945) | <0.001 | 4.67 (0.460) | 0.997 | 0.01 (−0.0872 to 0.1072) |
| 4 cm At load/DF | fixed ultrasonography | 4.24 (0.624) | 4.36 (0.614) | 0.894 (0.826–0.94) | <0.001 | 4.24 (0.626) | 1.000 | −0.005 (−0.0483 to 0.0383) |
| 6 cm At load/DF | fixed ultrasonography | 4.39 (0.531) | 4.36 (0.631) | 0.876 (0.802–0.928) | <0.001 | 4.39 (0.533) | 0.999 | −0.0025 (−0.0725 to 0.0675) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alabau-Dasi, R.; Dominguez-Maldonado, G.; Ortega-Avila, A.B.; Gordillo-Fernandez, L.M.; Ortiz-Romero, M.; Melchor-Rodriguez, J.M.; Gijon-Nogueron, G. Validation of Fixed Ultrasonography for Achilles Tendon Assessment: A Reliability Study. Diagnostics 2024, 14, 2221. https://doi.org/10.3390/diagnostics14192221
Alabau-Dasi R, Dominguez-Maldonado G, Ortega-Avila AB, Gordillo-Fernandez LM, Ortiz-Romero M, Melchor-Rodriguez JM, Gijon-Nogueron G. Validation of Fixed Ultrasonography for Achilles Tendon Assessment: A Reliability Study. Diagnostics. 2024; 14(19):2221. https://doi.org/10.3390/diagnostics14192221
Chicago/Turabian StyleAlabau-Dasi, Raquel, Gabriel Dominguez-Maldonado, Ana Belen Ortega-Avila, Luis M. Gordillo-Fernandez, Mercedes Ortiz-Romero, Juan Manuel Melchor-Rodriguez, and Gabriel Gijon-Nogueron. 2024. "Validation of Fixed Ultrasonography for Achilles Tendon Assessment: A Reliability Study" Diagnostics 14, no. 19: 2221. https://doi.org/10.3390/diagnostics14192221