
Feasibility of Double-Deployment Small-Diameter Covered Metallic Stent for Malignant Distal Biliary Obstruction (with Video)
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Procedure
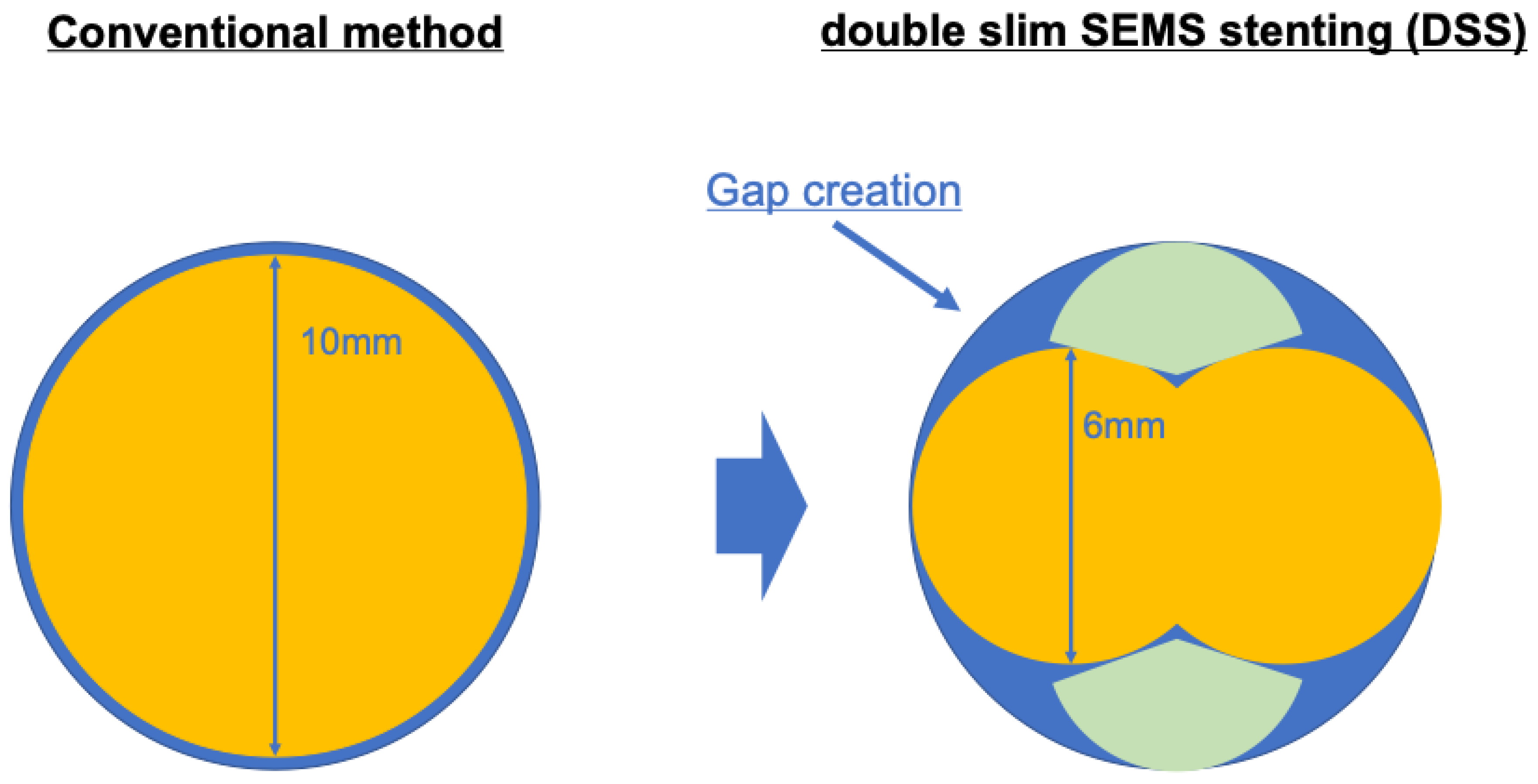
2.3. Procedure for DSS
2.4. Outcome Measurements
2.5. Statistics Analysis
3. Results
3.1. Patient Characteristics
3.2. Procedure Details
3.3. Clinical Outcome
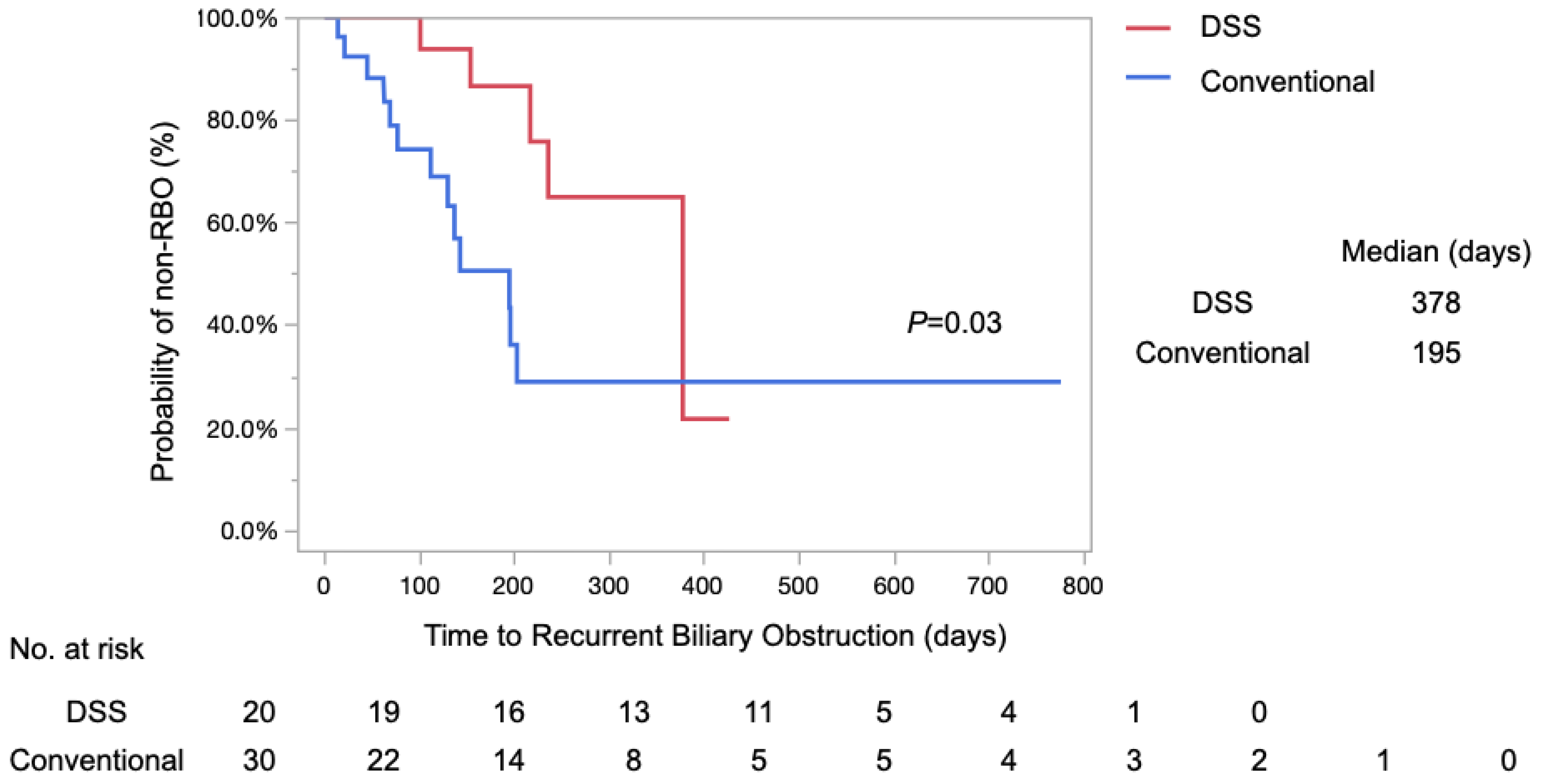
3.4. TRBO
3.5. Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moses, P.L.; AlNaamani, K.M.; Barkun, A.N.; Gordon, S.R.; Mitty, R.D.; Branch, M.S.; Kowalski, T.E.; Martel, M.; Adam, V. Randomized trial in malignant biliary obstruction: Plastic vs partially covered metal stents. World J. Gastroenterol. 2013, 19, 8638–8646. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Itonaga, M.; Ashida, R.; Yamashita, Y.; Hatamaru, K.; Kawaji, Y.; Emori, T.; Kitahata, Y.; Miyazawa, M.; Hirono, S.; et al. Covered self-expandable metal stents versus plastic stents for preoperative biliary drainage in patient receiving neo-adjuvant chemotherapy for borderline resectable pancreatic cancer: Prospective randomized study. Dig. Endosc. 2021, 33, 1170–1178. [Google Scholar] [CrossRef]
- Tol, J.A.M.G.; van Hooft, J.E.; Timmer, R.; Kubben, F.J.G.M.; van der Harst, E.; de Hingh, I.H.J.T.; Vleggaar, F.P.; Molenaar, I.Q.; Keulemans, Y.C.A.; Boerma, D.; et al. Metal or plastic stents for preoperative biliary drainage in resectable pancreatic cancer. Gut 2016, 65, 1981–1987. [Google Scholar] [CrossRef]
- Isayama, H.; Yasuda, I.; Ryozawa, S.; Maguchi, H.; Igarashi, Y.; Matsuyama, Y.; Katanuma, A.; Hasebe, O.; Irisawa, A.; Itoi, T.; et al. Results of a Japanese multicenter, randomized trial of endoscopic stenting for non-resectable pancreatic head cancer (JM-test): Covered Wallstent versus DoubleLayer stent. Dig. Endosc. 2011, 23, 310–315. [Google Scholar] [CrossRef]
- Tringali, A.; Hassan, C.; Rota, M.; Rossi, M.; Mutignani, M.; Aabakken, L. Covered vs. uncovered self-expandable metal stents for malignant distal biliary strictures: A systematic review and meta-analysis. Endoscopy 2018, 50, 631–641. [Google Scholar]
- Isayama, H.; Komatsu, Y.; Tsujino, T.; Sasahira, N.; Hirano, K.; Toda, N.; Nakai, Y.; Yamamoto, N.; Tada, M.; Yoshida, H.; et al. A prospective randomised study of “covered” versus “uncovered” diamond stents for the management of distal malignant biliary obstruction. Gut 2004, 53, 729–734. [Google Scholar] [CrossRef]
- Decker, C.; Christein, J.D.; Phadnis, M.A.; Wilcox, C.M.; Varadarajulu, S. Biliary metal stents are superior to plastic stents for preoperative biliary decompression in pancreatic cancer. Surg. Endosc. 2011, 25, 2364–2367. [Google Scholar] [CrossRef]
- Saleem, A.; Leggett, C.L.; Murad, M.H.; Baron, T.H. Meta-analysis of randomized trials comparing the patency of covered and uncovered self-expandable metal stents for palliation of distal malignant bile duct obstruction. Gastrointest. Endosc. 2011, 74, 321–327.e3. [Google Scholar] [CrossRef]
- Sakai, Y.; Sugiyama, H.; Kawaguchi, Y.; Kawashima, Y.; Hirata, N.; Nakaji, S.; Natsui, M.; Shioji, K.; Nakahara, K.; Tsuyuguchi, T.; et al. Uncovered versus covered metallic stents for the management of unresectable malignant distal biliary obstruction: A randomized multicenter trial. Scand. J. Gastroenterol. 2021, 56, 1229–1235. [Google Scholar] [CrossRef]
- Yoshida, T.; Hara, K.; Imaoka, H.; Hijioka, S.; Mizuno, N.; Ishihara, M.; Tanaka, T.; Tajika, M.; Niwa, Y.; Yamao, K. Benefits of side-by-side deployment of 6-mm covered self-expandable metal stents for hilar malignant biliary obstructions. J. Hepatobiliary Pancreat. Sci. 2016, 23, 548–555. [Google Scholar] [CrossRef]
- Inoue, T.; Okumura, F.; Naitoh, I.; Fukusada, S.; Kachi, K.; Ozeki, T.; Anbe, K.; Iwasaki, H.; Mizushima, T.; Kobayashi, Y.; et al. Feasibility of the placement of a novel 6-mm diameter threaded fully covered self-expandable metal stent for malignant hilar biliary obstructions (with videos). Gastrointest. Endosc. 2016, 84, 352–357. [Google Scholar] [CrossRef]
- Miyazaki, M.; Ohtsuka, M.; Miyakawa, S.; Nagino, M.; Yamamoto, M.; Kokudo, N.; Sano, K.; Endo, I.; Unno, M.; Chijiiwa, K.; et al. Classification of biliary tract cancers established by the Japanese Society of Hepato-Biliary-Pancreatic Surgery: 3(rd) English edition. J. Hepatobiliary Pancreat. Sci. 2015, 22, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Cotton, P.; Lehman, G.; Vennes, J.; Geenen, J.; Russell, R.; Meyers, W.; Liguory, C.; Nickl, N. Endoscopic sphincterotomy complications and their management: An attempt at consensus. Gastrointest. Endosc. 1991, 37, 383–393. [Google Scholar] [CrossRef]
- Yokoe, M.; Hata, J.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Wakabayashi, G.; Kozaka, K.; Endo, I.; Deziel, D.J.; Miura, F.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018, 25, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, M.; Takatori, H.; Okafuji, H.; Hayashi, T.; Toyama, T.; Yamada, S.; Kitamura, K.; Arai, K.; Sakai, Y.; Yamashita, T.; et al. Efficacy of a novel self-expandable metal stent with dumbbell-shaped flare ends for distal biliary obstruction due to unresectable pancreatic cancer. Sci. Rep. 2022, 12, 21100. [Google Scholar] [CrossRef] [PubMed]
- Huscher, C.G.S.; Lazzarin, G. Coronary artery stent for securing pancreatico-jejunal anastomosis after PD: The “Huscher technique”. Pancreatology 2022, 22, 1057–1058. [Google Scholar] [CrossRef] [PubMed]
- Kullman, E.; Frozanpor, F.; Söderlund, C.; Linder, S.; Sandström, P.; Lindhoff-Larsson, A.; Toth, E.; Lindell, G.; Jonas, E.; Freedman, J.; et al. Covered versus uncovered self-expandable nitinol stents in the palliative treatment of malignant distal biliary obstruction: Results from a randomized, multicenter study. Gastrointest. Endosc. 2010, 72, 915–923. [Google Scholar] [CrossRef]
- Krokidis, M.; Fanelli, F.; Orgera, G.; Tsetis, D.; Mouzas, I.; Bezzi, M.; Kouroumalis, E.; Pasariello, R.; Hatzidakis, A. Percutaneous palliation of pancreatic head cancer: Randomized comparison of ePTFE/FEP-covered versus uncovered nitinol biliary stents. Cardiovasc. Intervent. Radiol. 2011, 34, 352–361. [Google Scholar] [CrossRef]
- Kitano, M.; Yamashita, Y.; Tanaka, K.; Konishi, H.; Yazumi, S.; Nakai, Y.; Nishiyama, O.; Uehara, H.; Mitoro, A.; Sanuki, T.; et al. Covered self-expandable metal stents with an anti-migration system improve patency duration without increased complications compared with uncovered stents for distal biliary obstruction caused by pancreatic carcinoma: A randomized multicenter trial. Am. J. Gastroenterol. 2013, 108, 1713–1722. [Google Scholar] [CrossRef]
- Li, J.; Li, T.; Sun, P.; Yu, Q.; Wang, K.; Chang, W.; Song, Z.; Zheng, Q. Covered versus Uncovered Self-Expandable Metal Stents for Managing Malignant Distal Biliary Obstruction: A Meta-Analysis. PLoS ONE 2016, 11, e0149066. [Google Scholar] [CrossRef]
- Almadi, M.A.; Barkun, A.N.; Martel, M. No benefit of covered vs uncovered self-expandable metal stents in patients with malignant distal biliary obstruction: A meta-analysis. Clin. Gastroenterol. Hepatol. 2013, 11, 27–37.e1. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-Y.; Lin, J.-W.; Zhu, H.-P.; Zhang, B.; Jiang, G.-Y.; Yan, P.-J.; Cai, X.-J. Covered Stents versus Uncovered Stents for Unresectable Malignant Biliary Strictures: A Meta-Analysis. BioMed Res. Int. 2016, 2016, 6408067. [Google Scholar] [CrossRef] [PubMed]
- Ota, S.; Shiomi, H.; Nakano, R.; Nishimura, T.; Enomoto, H.; Iijima, H. A case of delayed pancreatic fistula after covered self-expandable metallic stent deployment for pancreatic head cancer. Clin. J. Gastroenterol. 2023, 16, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Sofuni, A.; Maguchi, H.; Mukai, T.; Kawakami, H.; Irisawa, A.; Kubota, K.; Okaniwa, S.; Kikuyama, M.; Kutsumi, H.; Hanada, K.; et al. Endoscopic pancreatic duct stents reduce the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis in high-risk patients. Clin. Gastroenterol. Hepatol. 2011, 9, 851–858. [Google Scholar] [CrossRef]
- Kahaleh, M.; Tokar, J.; Conaway, M.R.; Brock, A.; Le, T.; Adams, R.B.; Yeaton, P. Efficacy and complications of covered Wallstents in malignant distal biliary obstruction. Gastrointest. Endosc. 2005, 61, 528–533. [Google Scholar] [CrossRef]
- Suk, K.T.; Kim, H.S.; Kim, J.W.; Baik, S.K.; Kwon, S.O.; Kim, H.G.; Lee, D.H.; Yoo, B.M.; Kim, J.H.; Moon, Y.S.; et al. Risk factors for cholecystitis after metal stent placement in malignant biliary obstruction. Gastrointest. Endosc. 2006, 64, 522–529. [Google Scholar] [CrossRef]
- Fumex, F.; Coumaros, D.; Napoleon, B.; Barthet, M.; Laugier, R.; Yzet, T.; Sidaner, A.; Desurmont, P.; Lamouliatte, H.; Letard, J.-C.; et al. Similar performance but higher cholecystitis rate with covered biliary stents: Results from a prospective multicenter evaluation. Endoscopy 2006, 38, 787–792. [Google Scholar] [CrossRef]
- Isayama, H.; Kawabe, T.; Nakai, Y.; Tsujino, T.; Sasahira, N.; Yamamoto, N.; Arizumi, T.; Togawa, O.; Matsubara, S.; Ito, Y. Cholecystitis after metallic stent placement in patients with malignant distal biliary obstruction. Clin. Gastroenterol. Hepatol. 2006, 4, 1148–1153. [Google Scholar] [CrossRef]
- Motoi, F.; Kosuge, T.; Ueno, H.; Yamaue, H.; Satoi, S.; Sho, M.; Honda, G.; Matsumoto, I.; Wada, K.; Furuse, J.; et al. Randomized phase II/III trial of neoadjuvant chemotherapy with gemcitabine and S-1 versus upfront surgery for resectable pancreatic cancer (Prep-02/JSAP05). Jpn. J. Clin. Oncol. 2019, 49, 190–194. [Google Scholar] [CrossRef]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.-J.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- Kobayashi, K.; Kobara, H.; Kamada, H.; Kohno, T.; Namima, D.; Fujita, N.; Yamana, H.; Fujihara, S.; Okano, K.; Masaki, T. Comparison of plastic stent versus metal stent in preoperative biliary drainage for pancreatic head cancer with neoadjuvant chemoradiotherapy. J. Hepatobiliary Pancreat. Sci. 2021, 28, 856–863. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 50) | DSS (n = 20) | Conventional (n = 30) | p Value | |
|---|---|---|---|---|
| Age (years), median ±SD | 72 ± 8.9 | 72 ± 7.4 | 71.5 ± 9.4 | 0.71 |
| Gender (male/female) | 28/22 | 9/11 | 19/11 | 0.20 |
| BMI * (kg/m2), mean ± SD | 20.2 ± 3.1 | 20.2 ± 3.5 | 19.9 ± 3.1 | 0.76 |
| Cause of biliary obstruction | 0.55 | |||
| Pancreatic cancer | 46 | 19 | 27 | |
| Cholangiocarcinoma | 3 | 1 | 2 | |
| Lymph node metastasis | 1 | 0 | 1 | |
| Cystic duct invasion (yes/no) | 8/42 | 4/16 | 4/26 | 0.52 |
| MPD * dilation (yes/no) | 35/15 | 12/8 | 23/7 | 0.20 |
| Duodenum invasion (yes/no) | 13/37 | 7/13 | 6/24 | 0.23 |
| Length of stenosis (cm), mean ± SD | 2.1 ± 0.7 | 1.9 ± 0.6 | 2.3 ± 0.7 | 0.15 |
| Initial drainage (yes/no) | 34/16 | 12/8 | 22/8 | 0.32 |
| Prior Cholangitis (yes/no) | 17/33 | 10/10 | 7/23 | 0.09 |
| Total bilirubin (mg/dL), mean ± SD | 4.0 ± 4.2 | 4.3 ± 3.3 | 3.7 ± 4.5 | 0.51 |
| CRP (mg/dL), median ± SD | 3.7 ± 4.0 | 4.4 ± 5.1 | 3.2 ± 3.5 | 0.31 |
| Total (n = 50) | DSS (n = 20) | Conventional (n = 30) | p Value | |
|---|---|---|---|---|
| Technical success, (yes, %) | 50 (100%) | 20 (100%) | 30 (100%) | 1 |
| Cannulation time, (min) mean ± SD | 11.7 ± 9.9 | 10.5 ± 10.1 | 12.2 ± 9.9 | 0.60 |
| Method of cannulation WGC † with contrast-assisted/pancreatic guidewire/precut | 39/7/4 | 12/6/2 | 27/1/2 | 0.39 |
| Addition of Endoscopic Sphincterotomy, (yes/no) | 29/21 | 12/8 | 17/13 | 0.81 |
| The time of stents placement, (min) mean ± SD | 34.6 ± 15.3 | 35.4 ± 10.8 | 34.2 ± 17.7 | 0.61 |
| Length of CSEMS *, (n) 6/7/8/9 cm | 18/4/27/1 | 5/0/15/0 | 13/4/12/1 | 0.37 |
| Total (n = 50) | DSS (n = 20) | Conventional (n = 30) | p Value | |
|---|---|---|---|---|
| Clinical success, (yes, %) | 50 (100%) | 20 (100%) | 30 (100%) | 1 |
| Adverse events, (n, %) | 8 (17.3%) | 2 (10.0%) | 6 (20.0%) | 0.34 |
| Pancreatitis | 3 | 1 | 2 | |
| Cholecystitis | 3 | 0 | 3 | |
| Liver abscess | 1 | 1 | 0 | |
| Pancreatic leakage | 1 | 0 | 1 | |
| Success for re-intervention | 18/19 (94.7%) | 6/6 (100%) | 12/13 (92.3%) | 0.48 |
| DSS (n = 20) | Conventional (n = 30) | p Value | |
|---|---|---|---|
| The incidence of RBO * (n, %) | 6 (30%) | 13 (43%) | 0.34 |
| non-RBO rate, 3/6/12 month (%) | 100%/86%/64% | 74%/57%/28% | |
| reasons for RBO, (n) | |||
| occlusion | |||
| debris | 2 | 8 | 0.14 |
| food impaction | 0 | 0 | |
| overgrowth | 0 | 0 | |
| migration | 3 | 3 | 0.59 |
| non-obstructive cholangitis | 2 | 2 | 0.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, R.; Shiomi, H.; Okamoto, M.; Kawase, Y.; Yoshihara, K.; Yoshioka, R.; Kawata, S.; Yuri, Y.; Takashima, T.; Aizawa, N.; et al. Feasibility of Double-Deployment Small-Diameter Covered Metallic Stent for Malignant Distal Biliary Obstruction (with Video). Diagnostics 2024, 14, 2233. https://doi.org/10.3390/diagnostics14192233
Nakano R, Shiomi H, Okamoto M, Kawase Y, Yoshihara K, Yoshioka R, Kawata S, Yuri Y, Takashima T, Aizawa N, et al. Feasibility of Double-Deployment Small-Diameter Covered Metallic Stent for Malignant Distal Biliary Obstruction (with Video). Diagnostics. 2024; 14(19):2233. https://doi.org/10.3390/diagnostics14192233
Chicago/Turabian StyleNakano, Ryota, Hideyuki Shiomi, Mamiko Okamoto, Yuta Kawase, Kohei Yoshihara, Ryota Yoshioka, Shoki Kawata, Yukihisa Yuri, Tomoyuki Takashima, Nobuhiro Aizawa, and et al. 2024. "Feasibility of Double-Deployment Small-Diameter Covered Metallic Stent for Malignant Distal Biliary Obstruction (with Video)" Diagnostics 14, no. 19: 2233. https://doi.org/10.3390/diagnostics14192233