
Impact of Psoas Muscle Area Index on Short- and Mid-Term Mortality in Patients Undergoing Valve Surgery for Infective Endocarditis: A Retrospective Analysis

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Considerations
2.3. Endocarditis Diagnosis
2.4. Indications for Valve Surgery
2.5. Surgical Procedure for Valve Replacement
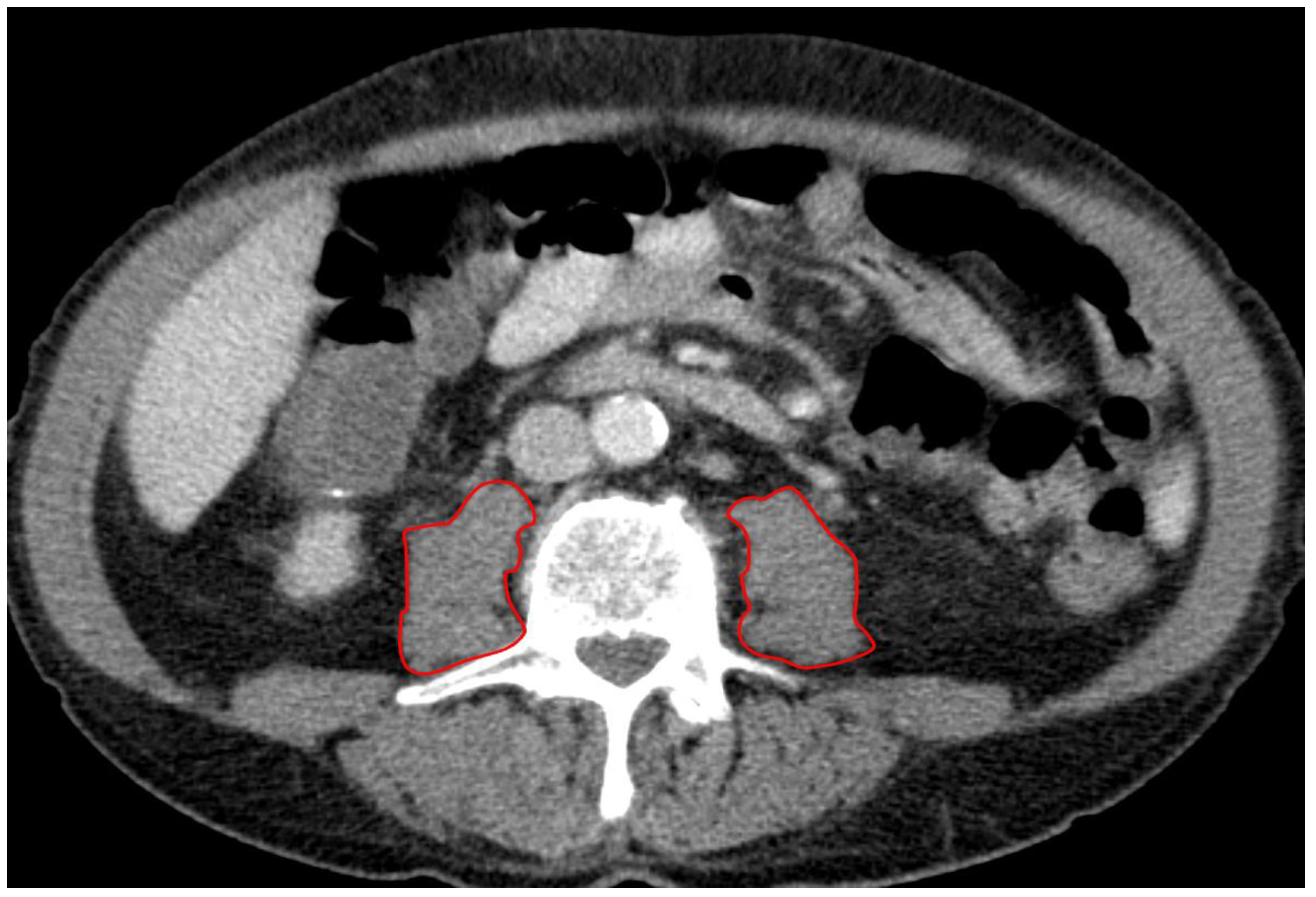
2.6. CT Protocol and Measurement of PMA
2.7. Statistical Analysis
3. Results
3.1. Sarcopenia Based on PMAi Quartiles
3.2. Baseline Characteristics of Overall Study Cohort and Sarcopenic vs. Non-Sarcopenic Patients
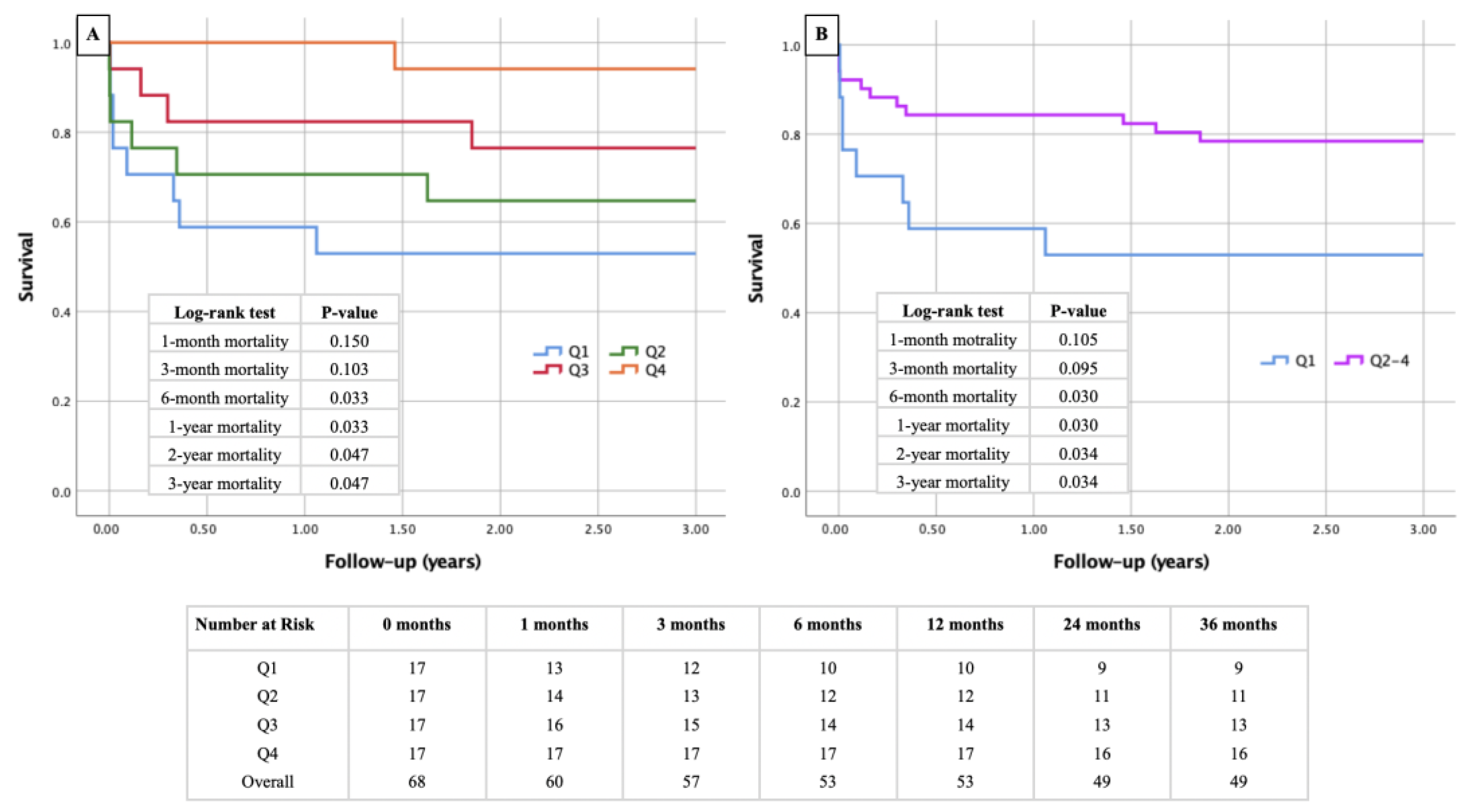
3.3. Kaplan–Meier Survival Curves Stratified by PMAi Quartiles and Sarcopenia Status
3.4. Predictive Value of PMAi for Short- and Mid-Term Mortality in Endocarditis Patients
3.5. Cox Regression Analysis in Patients Undergoing Valve Surgery for Endocarditis
3.6. Binary Logistic Regression Analysis for Predictors of Sarcopenia
4. Discussion
4.1. Sarcopenia as a Relevant Comorbidity in Endocarditis Patients and the Role of Radiology in Its Identification
4.2. Sarcopenia and Sex: A “Female Problem“?
4.3. CKI and Mortality
4.4. Protective Effect of ACEI/ARB/ARNI Therapy
4.5. Clinical Implications and Future Directions
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rajani, R.; Klein, J.L. Infective endocarditis: A contemporary update. Clin. Med. 2020, 20, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Cahill, T.J.; Baddour, L.M.; Habib, G.; Hoen, B.; Salaun, E.; Pettersson, G.B.; Schäfers, H.J.; Prendergast, B.D. Challenges in Infective Endocarditis. J. Am. Coll. Cardiol. 2017, 69, 325–344. [Google Scholar] [CrossRef]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G., Jr.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals from the American Heart Association. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef] [PubMed]
- Cimmino, G.; Bottino, R.; Formisano, T.; Orlandi, M.; Molinari, D.; Sperlongano, S.; Castaldo, P.; D’Elia, S.; Carbone, A.; Palladino, A.; et al. Current Views on Infective Endocarditis: Changing Epidemiology, Improving Diagnostic Tools and Centering the Patient for Up-to-Date Management. Life 2023, 13, 377. [Google Scholar] [CrossRef] [PubMed]
- Bea, C.; Vela, S.; García-Blas, S.; Perez-Rivera, J.A.; Díez-Villanueva, P.; de Gracia, A.I.; Fuertes, E.; Oltra, M.R.; Ferrer, A.; Belmonte, A.; et al. Infective Endocarditis in the Elderly: Challenges and Strategies. J. Cardiovasc. Dev. Dis. 2022, 9, 192. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, A.; Barbone, A.; Basciu, A.; Cuko, E.; Droandi, G.; Galbiati, D.; Romano, G.; Citterio, E.; Fumero, A.; Scarfò, I.; et al. Surgical Challenges in Infective Endocarditis: State of the Art. J. Clin. Med. 2023, 12, 5891. [Google Scholar] [CrossRef]
- Benedetto, U.; Spadaccio, C.; Gentile, F.; Moon, M.R.; Nappi, F. A narrative review of early surgery versus conventional treatment for infective endocarditis: Do we have an answer? Ann. Transl. Med. 2020, 8, 1626. [Google Scholar] [CrossRef]
- Dhillon, R.J.; Hasni, S. Pathogenesis and Management of Sarcopenia. Clin. Geriatr. Med. 2017, 33, 17–26. [Google Scholar] [CrossRef]
- Giovannini, S.; Brau, F.; Forino, R.; Berti, A.; D’Ignazio, F.; Loreti, C.; Bellieni, A.; D’Angelo, E.; Di Caro, F.; Biscotti, L.; et al. Sarcopenia: Diagnosis and Management, State of the Art and Contribution of Ultrasound. J. Clin. Med. 2021, 10, 5552. [Google Scholar] [CrossRef]
- Damluji, A.A.; Alfaraidhy, M.; AlHajri, N.; Rohant, N.N.; Kumar, M.; Al Malouf, C.; Bahrainy, S.; Ji Kwak, M.; Batchelor, W.B.; Forman, D.E.; et al. Sarcopenia and Cardiovascular Diseases. Circulation 2023, 147, 1534–1553. [Google Scholar] [CrossRef]
- Ansaripour, A.; Rad, A.A.; Koulouroudias, M.; Angouras, D.; Athanasiou, T.; Kourliouros, A. Sarcopenia Adversely Affects Outcomes following Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 5573. [Google Scholar] [CrossRef] [PubMed]
- Imamura, Y.; Suzuki, A.; Kamishima, K.; Suzuki, K.; Yamaguchi, J. Prognostic factors in patients with heart failure and sarcopenia: An observational retrospective study. Egypt. Heart J. 2024, 76, 52. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.; Wu, J.; Ren, Y.; Hu, J.; Yang, K.; Cao, J. Sarcopenia predicts adverse outcomes in an elderly population with coronary artery disease: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 493. [Google Scholar] [CrossRef] [PubMed]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Guo, Z.; Jiang, B.; Zhang, K.; Zhu, W.; Lian, X.; Xu, Y.; Zhao, Z.; Liu, L. Factors affecting sarcopenia in older patients with chronic diseases. Ann. Palliat. Med. 2022, 11, 972–983. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.B.; Mehaffey, J.H.; Charles, E.J.; Kern, J.A.; Lim, D.S.; Teman, N.R.; Ailawadi, G. Psoas Muscle Size Predicts Risk-Adjusted Outcomes after Surgical Aortic Valve Replacement. Ann. Thorac. Surg. 2018, 106, 39–45. [Google Scholar] [CrossRef]
- Bate, A.P.; Franke, K.B.; Jones, D.R.; Chokka, R.G.; Gibb, C.; Lau, J.K.; Montarello, J.; Psaltis, P.J.; Roberts-Thomson, R.L. Psoas Muscle Area as a Predictor of Transcatheter Aortic Valve Implantation Outcomes. Heart Lung Circ. 2024, 33, 310–315. [Google Scholar] [CrossRef]
- Delgado, V.; Marsan, N.A.; de Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the management of endocarditis. Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [CrossRef]
- Zuo, X.; Li, X.; Tang, K.; Zhao, R.; Wu, M.; Wang, Y.; Li, T. Sarcopenia and cardiovascular diseases: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2023, 14, 1183–1198. [Google Scholar] [CrossRef]
- Narici, M.V.; Maffulli, N. Sarcopenia: Characteristics, mechanisms and functional significance. Br. Med. Bull. 2010, 95, 139–159. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Ruiz, M.E.; Guarner-Lans, V.; Pérez-Torres, I.; Soto, M.E. Mechanisms Underlying Metabolic Syndrome-Related Sarcopenia and Possible Therapeutic Measures. Int. J. Mol. Sci. 2019, 20, 647. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Suzuki, T.; Enomoto, M.; Takashima, N.; Kinoshita, T. Psoas muscle size, possible sarcopenia and frailty, and long-term survival in elderly patients after isolated surgical aortic valve replacement for aortic stenosis. Indian J. Thorac. Cardiovasc. Surg. 2022, 38, 134–141. [Google Scholar] [CrossRef]
- Rodge, G.A.; Goenka, U.; Jajodia, S.; Agarwal, R.; Afzalpurkar, S.; Roy, A.; Goenka, M.K. Psoas Muscle Index: A Simple and Reliable Method of Sarcopenia Assessment on Computed Tomography Scan in Chronic Liver Disease and its Impact on Mortality. J. Clin. Exp. Hepatol. 2023, 13, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.-Y.; Li, C.; Zhang, H.; Liu, Y.; Wei, J.-M. Total Psoas Area Index is Valuable to Assess Sarcopenia, Sarcopenic Overweight/Obesity and Predict Outcomes in Patients Undergoing Open Pancreatoduodenectomy. Risk Manag. Healthc. Policy 2020, 13, 761–770. [Google Scholar] [CrossRef]
- Buckinx, F.; Aubertin-Leheudre, M. Sarcopenia in Menopausal Women: Current Perspectives. Int. J. Women’s Health 2022, 14, 805–819. [Google Scholar] [CrossRef]
- Papadopoulou, S.K. Sarcopenia: A Contemporary Health Problem among Older Adult Populations. Nutrients 2020, 12, 1293. [Google Scholar] [CrossRef]
- Sutil, D.V.; Parentoni, A.N.; Teixeira, L.A.D.C.; Moreira, B.d.S.; Leopoldino, A.A.O.; Mendonça, V.A.; Lacerda, A.C.R.; Danielewicz, A.L.; de Avelar, N.C.P. Prevalence of sarcopenia in older women and level of agreement between the diagnostic instruments proposed by the European Working Group on Sarcopenia in Older People 2 (EWGSOP2). BMC Musculoskelet. Disord. 2023, 24, 182. [Google Scholar] [CrossRef]
- Casas, A.; Mallén, A.; Blasco-Lucas, A.; Sbraga, F.; Guiteras, J.; Bolaños, N.; Castaño, E.; Torras, J.; Cruzado, J.M.; Navarro, E.; et al. Chronic Kidney Disease-Associated Inflammation Increases the Risks of Acute Kidney Injury and Mortality after Cardiac Surgery. Int. J. Mol. Sci. 2020, 21, 9689. [Google Scholar] [CrossRef]
- Moorthi, R.N.; Avin, K.G. Clinical relevance of sarcopenia in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2017, 26, 219–228. [Google Scholar] [CrossRef]
- Yu, M.-D.; Zhang, H.-Z.; Zhang, Y.; Yang, S.-P.; Lin, M.; Zhang, Y.-M.; Wu, J.-B.; Hong, F.-Y.; Chen, W.-X. Relationship between chronic kidney disease and sarcopenia. Sci. Rep. 2021, 11, 20523. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, A.; Cuppari, L.; Stenvinkel, P.; Lindholm, B.; Avesani, C.M. Sarcopenia in chronic kidney disease: What have we learned so far? J. Nephrol. 2021, 34, 1347–1372. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Zaballos, S.; Martínez-Sellés, M. Angiotensin-Converting Enzyme and Heart Failure. Front. Biosci. 2023, 28, 150. [Google Scholar] [CrossRef] [PubMed]
- Cao, D.-Y.; Giani, J.F.; Veiras, L.C.; Bernstein, E.A.; Okwan-Duodu, D.; Ahmed, F.; Bresee, C.; Tourtellotte, W.G.; Karumanchi, S.A.; Bernstein, K.E.; et al. An ACE inhibitor reduces bactericidal activity of human neutrophils in vitro and impairs mouse neutrophil activity in vivo. Sci. Transl. Med. 2021, 13, eabj2138. [Google Scholar] [CrossRef]
- Bartel, T.; Müller, S.; Nesser, H.J.; Möhlenkamp, S.; Bruch, C.; Erbel, R. Usefulness of motion patterns indentified by tissue Doppler echocardiography for diagnosing various cardiac masses, particularly valvular vegetations. Am. J. Cardiol. 1999, 84, 1428–1433. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| PMAi (mm2/m2) | |
|---|---|
| Q1 | <620.96 |
| Q2 | 620.96–789.60 |
| Q3 | 789.60–940.91 |
| Q4 | >940.91 |
| Total | Sarcopenia+ | Sarcopenia− | p-Value | |
|---|---|---|---|---|
| No. (%) | ||||
| Total | 68 (100.0) | 17 (25.0) | 51 (75.0) | - |
| Sex | ||||
| Female | 20 (29.4) | 14 (82.4) | 6 (11.8) | <0.001 |
| Male | 48 (70.6) | 3 (17.6) | 45 (88.2) | <0.001 |
| Pre-existing conditions | ||||
| Arterial hypertension | 35 (51.5) | 11 (64.7) | 24 (47.1) | 0.207 |
| Diabetes mellitus | 14 (20.6) | 3 (17.6) | 11 (21.6) | 0.729 |
| COPD | 6 (8.8) | 3 (17.6) | 3 (5.9) | 0.139 |
| CKI | 8 (11.8) | 1 (5.9) | 7 (13.7) | 0.385 |
| Chronic heart failure | 12 (17.6) | 2 (11.8) | 10 (19.6) | 0.463 |
| CVD | 24 (35.3) | 11 (64.7) | 13 (25.5) | 0.003 |
| AF | 20 (29.4) | 7 (41.2) | 13 (25.5) | 0.219 |
| Premedication | ||||
| Diuretics | 39 (44.1) | 9 (52.9) | 21 (41.2) | 0.398 |
| Beta-blocker | 33 (48.5) | 11 (64.7) | 22 (43.1) | 0.123 |
| ACEI/ARB/ARNI | 20 (29.4) | 5 (29.4) | 15 (29.4) | 1.000 |
| Echocardiography | ||||
| AR III | 15 (22.1) | 4 (23.5) | 11 (21.6) | 0.866 |
| MR III | 19 (27.9) | 4 (23.5) | 15 (29.4) | 0.640 |
| TR III | 5 (7.4) | 3 (17.6) | 2 (3.9) | 0.060 |
| Preoperative conditions | ||||
| Elective surgery | 2 (2.9) | 2 (11.8) | 0 (0.0) | 0.013 |
| Urgent surgery | 53 (77.9) | 13 (76.3) | 40 (78.4) | 0.866 |
| Emergency surgery | 13 (19.1) | 2 (11.8) | 11 (21.6) | 0.373 |
| Intraoperative conditions | ||||
| Endocarditis of one heart valve | 54 (79.4) | 14 (82.4) | 40 (78.4) | 0.729 |
| Endocarditis of two heart valves | 14 (20.6) | 3 (17.6) | 11 (21.6) | 0.729 |
| Endocarditis of three heart valves | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Postoperative conditions | ||||
| ECMO | 4 (5.9) | 1 (5.9) | 3 (5.9) | 1.000 |
| Bleeding/tamponade | 7 (10.3) | 0 (0.0) | 7 (13.7) | 0.107 |
| Stroke | 3 (4.4) | 2 (11.8) | 1 (2.0) | 0.088 |
| Valvular complications | 1 (1.5) | 0 (0.0) | 1 (2.0) | 0.561 |
| Third-degree atrioventricular block | 6 (8.8) | 2 (11.8) | 4 (7.8) | 0.622 |
| Sepsis | 1 (1.5) | 0 (0.0) | 1 (2.0) | 0.561 |
| In-hospital death | 12 (17.6) | 5 (29.4) | 7 (13.7) | 0.142 |
| Mean ± SD | ||||
| Age (years) | 62.4 ± 11.9 | 68.1 ± 10.7 | 60.5 ± 11.7 | 0.021 |
| Height (cm) | 172.9 ± 8.6 | 164.8 ± 8.5 | 175.6 ± 6.8 | <0.001 |
| Weight (kg) | 81.4 ± 16.2 | 72.1 ± 11.9 | 84.4 ± 16.3 | 0.006 |
| BMI (kg/m2) | 27.2 ± 4.7 | 26.6 ± 4.5 | 27.3 ± 4.9 | 0.599 |
| BSA (m2) | 1.9 ± 0.2 | 1.8 ± 0.2 | 2.0 ± 0.2 | <0.001 |
| PMA (mm2) | 1590.6 ± 543.9 | 937.1 ± 130.9 | 1808.4 ± 444.2 | <0.001 |
| PMAi (mm2/m2) | 809.8 ± 245.9 | 526.7 ± 74.3 | 904.2 ± 207.1 | <0.001 |
| Surgery time (min) | 284.9 ± 115.7 | 287.8 ± 95.1 | 283.9 ± 122.6 | 0.904 |
| Clamping time (min) | 109.3 ± 56.9 | 110.0 ± 44.7 | 109.0 ±60.8 | 0.952 |
| Perfusion time (min) | 167.7 ± 92.6 | 175.1 ± 76.2 | 165.2 ± 98.0 | 0.705 |
| Median ± IQR | ||||
| LVEF (%) | 55.0 ± 4.0 | 55.0 ± 7.5 | 55.0 ± 4.0 | 0.927 |
| Cox Regression Analysis | Univariate | Multivariable | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| 1-year mortality | ||||
| Gender (female) | 3.239 (1.173–8.948) | 0.023 | 2.104 (0.469–9.438) | 0.331 |
| Age | 0.779 (0.424–1.432) | 0.421 | ||
| BMI | 1.256 (0.797–1.978) | 0.326 | ||
| BSA | 0.831 (0.511–1.352) | 0.456 | ||
| Arterial hypertension | 0.584 (0.208–1.641) | 0.307 | ||
| Diabetes mellitus | 0.910 (0.257–3.224) | 0.884 | ||
| COPD | 1.905 (0.430–8.445) | 0.396 | ||
| CKI | 5.503 (1.867–16.222) | 0.002 | 4.762 (1.452–15.621) | 0.010 |
| Chronic heart failure | 0.662 (0.149–2.934) | 0.587 | ||
| CVD | 0.913 (0.312–2.671) | 0.867 | ||
| AF | 0.859 (0.273–2.697) | 0.794 | ||
| LVEF | 1.236 (0.739–2.068) | 0.418 | ||
| AR III° | 0.515 (0.116–2.282) | 0.382 | ||
| MR III° | 0.879 (0.280–2.760) | 0.825 | ||
| TR III° | 2.151 (0.485–9.550) | 0.314 | ||
| Diuretics | 2.775 (0.948–8.127) | 0.063 | 2.578 (0.831–7.991) | 0.101 |
| Beta blocker | 1.226 (0.445–3.381) | 0.694 | ||
| ACEI/ARB/ARNI | 0.149 (0.020–1.136) | 0.066 | 0.112 (0.014–0.870) | 0.036 |
| PMA | 0.529 (0.291–0.961) | 0.036 | 2.081 (0.232–18.670) | 0.513 |
| PMAi | 0.494 (0.265–0.920) | 0.026 | 0.378 (0.179–0.795) | 0.010 |
| 3-year mortality | ||||
| Gender (female) | 2.124 (0.853–5.289) | 0.106 | ||
| Age | 0.783 (0.453–1.351) | 0.379 | ||
| BMI | 1.338 (0.892–2.007) | 0.160 | ||
| BSA | 0.988 (0.644–1.516) | 0.956 | ||
| Arterial hypertension | 0.498 (0.196–1.265) | 0.143 | ||
| Diabetes mellitus | 0.979 (0.325–2.950) | 0.970 | ||
| COPD | 2.409 (0.701–8.277) | 0.163 | ||
| CKI | 4.224 (1.510–11.818) | 0.006 | 3.097 (1.019–9.409) | 0.046 |
| Chronic heart failure | 0.801 (0.233–2.748) | 0.724 | ||
| CVD | 1.074 (0.423–2.729) | 0.881 | ||
| AF | 1.086 (0.413–2.858) | 0.867 | ||
| LVEF | 1.122 (0.719–1.753) | 0.612 | ||
| AINS III° | 1.026 (0.434–3.349) | 0.720 | ||
| MINS III° | 0.873 (0.314–2.424) | 0.794 | ||
| TRINS III° | 1.693 (0.391–7.338) | 0.482 | ||
| Diuretics | 3.133 (1.189–8.253) | 0.021 | 2.846 (1.036–7.815) | 0.042 |
| Beta blocker | 1.881 (0.740–4.780) | 0.184 | ||
| ACEI/ARB/ARNI | 0.235 (0.054–1.019) | 0.053 | 0.162 (0.036–0.716) | 0.016 |
| PMA | 0.608 (0.366–1.009) | 0.054 | 2.523 (0.465–13.676) | 0.283 |
| PMAi | 0.541 (0.317–0.925) | 0.025 | 0.457 (0.249–0.841) | 0.012 |
| Binary Logistic Regression | Univariate | Multivariable | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Sarcopenia (lowest quartile of PMAi) | ||||
| Gender (female) | 35.000 (7.731–158.456) | <0.001 | 275.748 (17.491–4347.304) | <0.001 |
| Age | 2.677 (1.116–6.420) | 0.027 | 9.995 (2.150–46.465) | 0.003 |
| Weight | 0.376 (0.179–0.788) | 0.010 | 0.663 (0.226–1.947) | 0.455 |
| Height | 0.212 (0.093–0.480) | <0.001 | 1.188 (0.262–5.385) | 0.823 |
| BMI | 0.863 (0.503–1.480) | 0.593 | ||
| Arterial Hypertension | 2.062 (0.662–6.427) | 0.212 | ||
| Diabetes mellitus | 0.779 (0.189–3.205) | 0.730 | ||
| COPD | 3.429 (0.622–18.908) | 0.157 | ||
| CKI | 0.393 (0.045–3.448) | 0.399 | ||
| Chronic heart Failure | 0.547 (0.107–2.788) | 0.468 | ||
| CVD | 5.359 (1.651–17.393) | 0.005 | 2.016 (0.214–19.004) | 0.540 |
| AF | 2.046 (0.646–6.482) | 0.224 | ||
| LVEF | 1.191 (0.677–2.095) | 0.544 | ||
| AR III° | 1.119 (0.304–4.123) | 0.866 | ||
| MR III° | 0.738 (0.207–2.636) | 0.640 | ||
| TR III° | 5.250 (0.797–34.585) | 0.085 | 15.733 (0.312–792.195) | 0.168 |
| Diuretics | 1.607 (0.533–4.846) | 0.399 | ||
| Beta blocker | 2.417 (0.774–7.546) | 0.129 | ||
| ACEI/ARB/ARNI | 1.000 (0.300–3.336) | 1.000 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dinges, C.; Hammerer, M.; Schörghofer, N.; Knapitsch, C.; Hecke, G.; Klaus, S.; Steindl, J.; Rezar, R.; Seitelberger, R.; Hoppe, U.C.; et al. Impact of Psoas Muscle Area Index on Short- and Mid-Term Mortality in Patients Undergoing Valve Surgery for Infective Endocarditis: A Retrospective Analysis. Diagnostics 2024, 14, 2259. https://doi.org/10.3390/diagnostics14202259
Dinges C, Hammerer M, Schörghofer N, Knapitsch C, Hecke G, Klaus S, Steindl J, Rezar R, Seitelberger R, Hoppe UC, et al. Impact of Psoas Muscle Area Index on Short- and Mid-Term Mortality in Patients Undergoing Valve Surgery for Infective Endocarditis: A Retrospective Analysis. Diagnostics. 2024; 14(20):2259. https://doi.org/10.3390/diagnostics14202259
Chicago/Turabian StyleDinges, Christian, Matthias Hammerer, Nikolaos Schörghofer, Christoph Knapitsch, Gretha Hecke, Sophie Klaus, Johannes Steindl, Richard Rezar, Rainald Seitelberger, Uta C. Hoppe, and et al. 2024. "Impact of Psoas Muscle Area Index on Short- and Mid-Term Mortality in Patients Undergoing Valve Surgery for Infective Endocarditis: A Retrospective Analysis" Diagnostics 14, no. 20: 2259. https://doi.org/10.3390/diagnostics14202259
APA StyleDinges, C., Hammerer, M., Schörghofer, N., Knapitsch, C., Hecke, G., Klaus, S., Steindl, J., Rezar, R., Seitelberger, R., Hoppe, U. C., Hergan, K., Boxhammer, E., & Scharinger, B. (2024). Impact of Psoas Muscle Area Index on Short- and Mid-Term Mortality in Patients Undergoing Valve Surgery for Infective Endocarditis: A Retrospective Analysis. Diagnostics, 14(20), 2259. https://doi.org/10.3390/diagnostics14202259