
Histopathological Evaluation of Somatostatin Receptor 2 Expression in Myocarditis—Rationale for the Diagnostic Use of Somatostatin Receptor Imaging

 , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Diagnostic Criteria
2.2. Histological, Immunohistochemical, and Immunofluorescene Analysis
2.3. Western Blot Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient and Control Characteristics
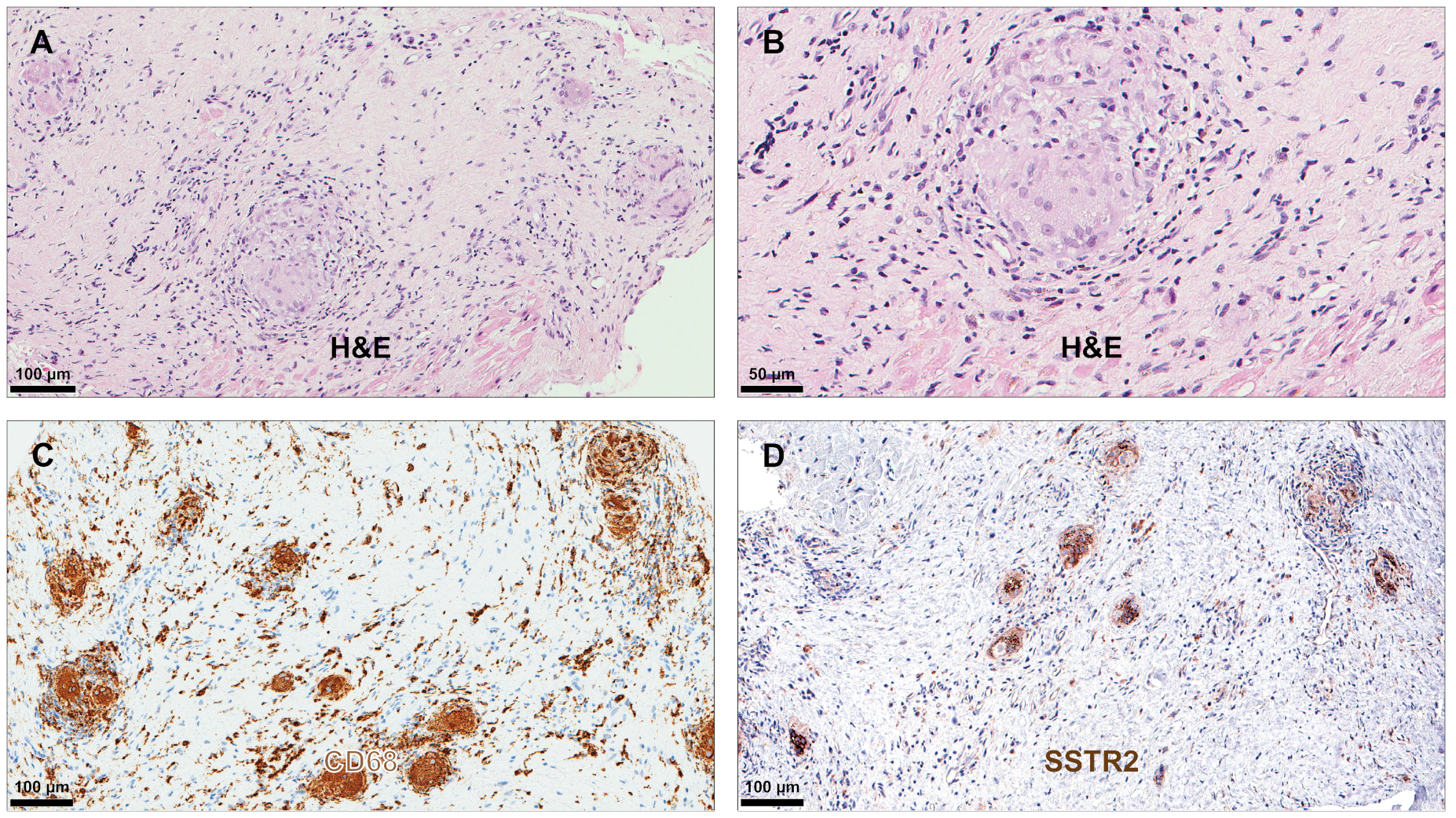
3.2. Histological, Immunohistochemical, and Immunofluorescence Characteristics
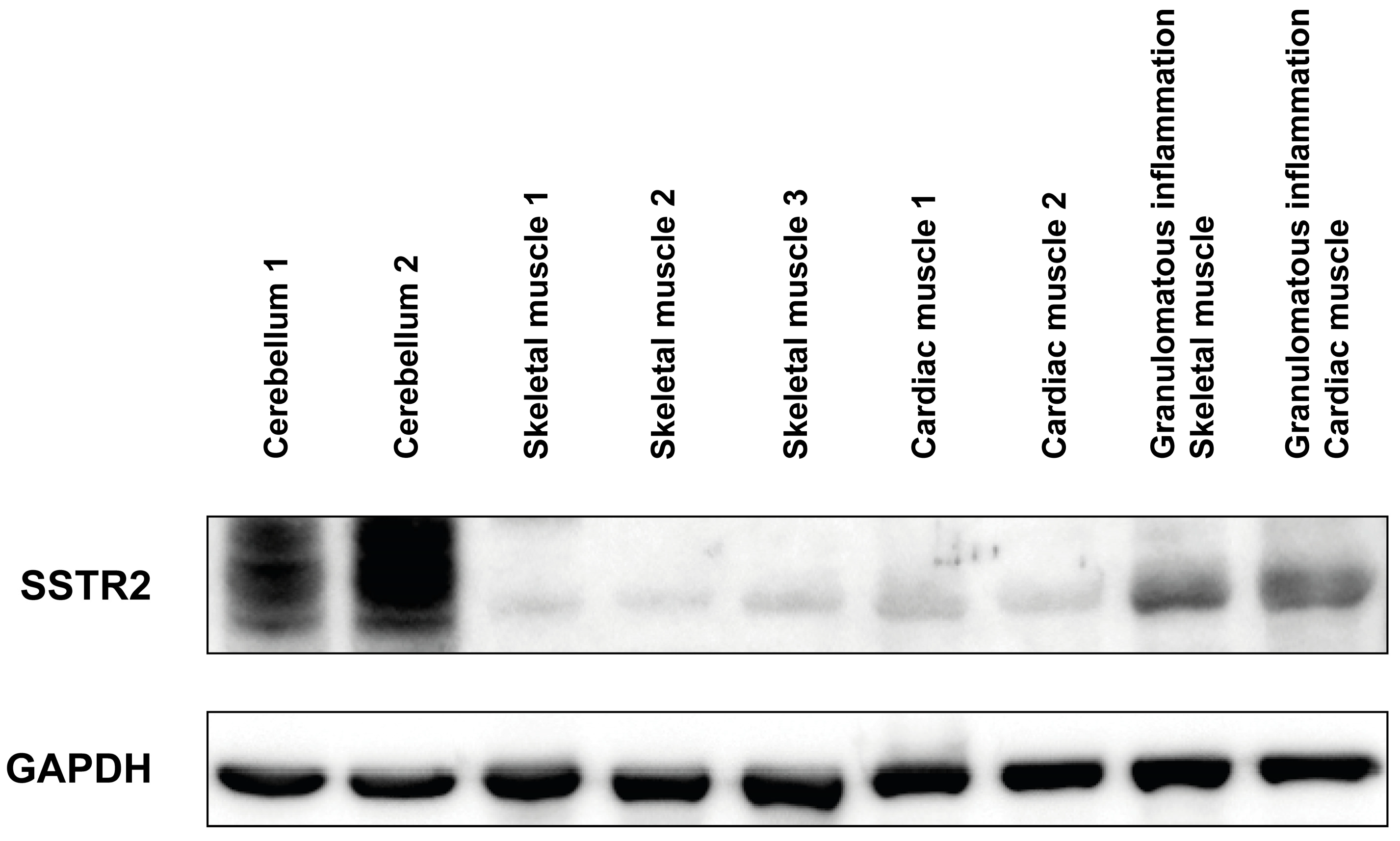
3.3. Western Blot Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Helio, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef] [PubMed]
- Kindermann, I.; Barth, C.; Mahfoud, F.; Ukena, C.; Lenski, M.; Yilmaz, A.; Klingel, K.; Kandolf, R.; Sechtem, U.; Cooper, L.T.; et al. Update on myocarditis. J. Am. Coll. Cardiol. 2012, 59, 779–792. [Google Scholar] [CrossRef] [PubMed]
- Bang, V.; Ganatra, S.; Shah, S.P.; Dani, S.S.; Neilan, T.G.; Thavendiranathan, P.; Resnic, F.S.; Piemonte, T.C.; Barac, A.; Patel, R.; et al. Management of Patients with Giant Cell Myocarditis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2021, 77, 1122–1134. [Google Scholar] [CrossRef]
- Cooper, L.T., Jr.; Berry, G.J.; Shabetai, R. Idiopathic giant-cell myocarditis--natural history and treatment. Multicenter Giant Cell Myocarditis Study Group Investigators. N. Engl. J. Med. 1997, 336, 1860–1866. [Google Scholar] [CrossRef]
- Trivieri, M.G.; Spagnolo, P.; Birnie, D.; Liu, P.; Drake, W.; Kovacic, J.C.; Baughman, R.; Fayad, Z.A.; Judson, M.A. Challenges in Cardiac and Pulmonary Sarcoidosis: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 1878–1901. [Google Scholar] [CrossRef]
- Birnie, D.H.; Nery, P.B.; Ha, A.C.; Beanlands, R.S. Cardiac Sarcoidosis. J. Am. Coll. Cardiol. 2016, 68, 411–421. [Google Scholar] [CrossRef]
- Trachtenberg, B.H.; Hare, J.M. Inflammatory Cardiomyopathic Syndromes. Circ. Res. 2017, 121, 803–818. [Google Scholar] [CrossRef] [PubMed]
- Kadkhodayan, A.; Chareonthaitawee, P.; Raman, S.V.; Cooper, L.T. Imaging of Inflammation in Unexplained Cardiomyopathy. JACC Cardiovasc. Imaging 2016, 9, 603–617. [Google Scholar] [CrossRef]
- Chareonthaitawee, P.; Gutberlet, M. Clinical Utilization of Multimodality Imaging for Myocarditis and Cardiac Sarcoidosis. Circ. Cardiovasc. Imaging 2023, 16, e014091. [Google Scholar] [CrossRef]
- Lichtenauer-Kaligis, E.G.; van Hagen, P.M.; Lamberts, S.W.; Hofland, L.J. Somatostatin receptor subtypes in human immune cells. Eur. J. Endocrinol. 2000, 143 (Suppl. 1), S21–S25. [Google Scholar] [CrossRef]
- Lapa, C.; Reiter, T.; Li, X.; Werner, R.A.; Samnick, S.; Jahns, R.; Buck, A.K.; Ertl, G.; Bauer, W.R. Imaging of myocardial inflammation with somatostatin receptor based PET/CT—A comparison to cardiac MRI. Int. J. Cardiol. 2015, 194, 44–49. [Google Scholar] [CrossRef]
- Gormsen, L.C.; Haraldsen, A.; Kramer, S.; Dias, A.H.; Kim, W.Y.; Borghammer, P. A dual tracer (68)Ga-DOTANOC PET/CT and (18)F-FDG PET/CT pilot study for detection of cardiac sarcoidosis. EJNMMI Res. 2016, 6, 52. [Google Scholar] [CrossRef]
- Lapa, C.; Reiter, T.; Kircher, M.; Schirbel, A.; Werner, R.A.; Pelzer, T.; Pizarro, C.; Skowasch, D.; Thomas, L.; Schlesinger-Irsch, U.; et al. Somatostatin receptor based PET/CT in patients with the suspicion of cardiac sarcoidosis: An initial comparison to cardiac MRI. Oncotarget 2016, 7, 77807–77814. [Google Scholar] [CrossRef] [PubMed]
- Pizarro, C.; Kluenker, F.; Dabir, D.; Thomas, D.; Gaertner, F.C.; Essler, M.; Grohe, C.; Nickenig, G.; Skowasch, D. Cardiovascular magnetic resonance imaging and clinical performance of somatostatin receptor positron emission tomography in cardiac sarcoidosis. ESC Heart Fail. 2018, 5, 249–261. [Google Scholar] [CrossRef]
- Bravo, P.E.; Bajaj, N.; Padera, R.F.; Morgan, V.; Hainer, J.; Bibbo, C.F.; Harrington, M.; Park, M.A.; Hyun, H.; Robertson, M.; et al. Feasibility of somatostatin receptor-targeted imaging for detection of myocardial inflammation: A pilot study. J. Nucl. Cardiol. 2021, 28, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Boughdad, S.; Latifyan, S.; Fenwick, C.; Bouchaab, H.; Suffiotti, M.; Moslehi, J.J.; Salem, J.E.; Schaefer, N.; Nicod-Lalonde, M.; Costes, J.; et al. (68)Ga-DOTATOC PET/CT to detect immune checkpoint inhibitor-related myocarditis. J. Immunother. Cancer 2021, 9, e003594. [Google Scholar] [CrossRef]
- Polte, C.L.; Bollano, E.; Oldfors, A.; Dudas, A.; Lagerstrand, K.M.; Himmelman, J.; Bobbio, E.; Karason, K.; van Essen, M.; Bergh, N. Somatostatin Receptor Positron Emission Tomography/Computed Tomography in Giant Cell Myocarditis: A Promising Approach to Molecular Myocardial Inflammation Imaging. Circ. Cardiovasc. Imaging 2021, 15, e013551. [Google Scholar] [CrossRef]
- Polte, C.L.; Bergh, N.; Oldfors, A.; Hanna, B.; Bollano, E. Cardiac involvement in immune-mediated necrotizing myopathy: Insights from CMR and somatostatin receptor PET/CT. Eur. Heart J. Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef]
- Bollano, E.; Bergh, N.; Dudas, A.; Bobbio, E.; Polte, C.L. Somatostatin receptor positron emission tomography/computed tomography in myocarditis following mRNA COVID-19 vaccination. Eur. Heart J. Case Rep. 2022, 6, ytac117. [Google Scholar] [CrossRef]
- Boursier, C.; Chevalier, E.; Filippetti, L.; Imbert, L.; Roch, V.; Huttin, O.; Claudin, M.; Marie, P.Y. (68)Ga-DOTATOC digital-PET imaging of inflammatory cell infiltrates in myocarditis following COVID-19 vaccination. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1433–1434. [Google Scholar] [CrossRef]
- Lee, H.; Schubert, E.K.; Vidula, M.K.; Pryma, D.A.; Marchlinski, F.E.; Goldberg, L.R.; Clancy, C.B.; Rossman, M.D.; DiCarli, M.F.; Bravo, P.E. Potential clinical utility of (68)Ga-DOTATATE PET/CT for detection and response assessment in cardiac sarcoidosis. J. Nucl. Cardiol. 2023, 30, 1075–1087. [Google Scholar] [CrossRef] [PubMed]
- Boursier, C.; Weizman, O.; Chevalier, E.; Imbert, L.; Mandry, D.; Varlot, J.; Hueber, A.; Marie, P.Y. Acute Left Atrial Myocarditis due to Close Contact with Inflammatory Nodes and Identified by Combined Cardiac Magnetic Resonance and (68)Ga-Dotatoc Positron Emission Tomography Image Analysis. Circ. Cardiovasc. Imaging 2023, 16, e014770. [Google Scholar] [CrossRef] [PubMed]
- Boursier, C.; Chevalier, E.; Varlot, J.; Filippetti, L.; Huttin, O.; Roch, V.; Imbert, L.; Albuisson, E.; Claudin, M.; Mandry, D.; et al. Detection of acute myocarditis by ECG-triggered PET imaging of somatostatin receptors compared to cardiac magnetic resonance: Preliminary results. J. Nucl. Cardiol. 2023, 30, 1043–1049. [Google Scholar] [CrossRef]
- Okura, Y.; Dec, G.W.; Hare, J.M.; Kodama, M.; Berry, G.J.; Tazelaar, H.D.; Bailey, K.R.; Cooper, L.T. A clinical and histopathologic comparison of cardiac sarcoidosis and idiopathic giant cell myocarditis. J. Am. Coll. Cardiol. 2003, 41, 322–329. [Google Scholar] [CrossRef]
- Kato, S.; Sakai, Y.; Okabe, A.; Kawashima, Y.; Kuwahara, K.; Shiogama, K.; Abe, M.; Ito, H.; Morimoto, S. Histology of Cardiac Sarcoidosis with Novel Considerations Arranged upon a Pathologic Basis. J. Clin. Med. 2022, 11, 251. [Google Scholar] [CrossRef]
- Dubowitz, V.; Sewry, C.A.; Oldfors, A. Muscle Biopsy: A Practical Approach, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Lamberts, S.W.; van der Lely, A.J.; de Herder, W.W.; Hofland, L.J. Octreotide. N. Engl. J. Med. 1996, 334, 246–254. [Google Scholar] [CrossRef]
- Lichtenauer-Kaligis, E.G.; Dalm, V.A.; Oomen, S.P.; Mooij, D.M.; van Hagen, P.M.; Lamberts, S.W.; Hofland, L.J. Differential expression of somatostatin receptor subtypes in human peripheral blood mononuclear cell subsets. Eur. J. Endocrinol. 2004, 150, 565–577. [Google Scholar] [CrossRef]
- ten Bokum, A.M.; Hofland, L.J.; de Jong, G.; Bouma, J.; Melief, M.J.; Kwekkeboom, D.J.; Schonbrunn, A.; Mooy, C.M.; Laman, J.D.; Lamberts, S.W.; et al. Immunohistochemical localization of somatostatin receptor sst2A in sarcoid granulomas. Eur. J. Clin. Invest. 1999, 29, 630–636. [Google Scholar] [CrossRef]
- Kircher, M.; Lapa, C. Novel Noninvasive Nuclear Medicine Imaging Techniques for Cardiac Inflammation. Curr. Cardiovasc. Imaging Rep. 2017, 10, 6. [Google Scholar] [CrossRef]
- Castillero, E.; Camillo, C.; Erwin, W.C.; Singh, S.; Mohamoud, N.; George, I.; Eapen, E.; Dockery, K.; Ferrari, G.; Gupta, H. Somatostatin receptors in fibrotic myocardium. PLoS ONE 2024, 19, e0304813. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LM (n = 5) | GCM (n = 11) | CS (n = 17) | Overall p-Value | |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age (years) | 29 (25–67) | 54 (51–67) | 58 (52–62) | 0.096 |
| Sex (male) | 2 (40) | 5 (45) | 10 (59) | 0.673 |
| BMI (kg/m2) | 29 (24–30) | 23 (21–26) | 26 (20–31) | 0.351 |
| Comorbidities | ||||
| Hypertension | 1 (20) | 2 (18) | 4 (24) | 0.942 |
| Diabetes mellitus | 0 | 1 (9) | 0 | 0.357 |
| Coronary artery disease | 0 | 0 | 4 (24) | 0.117 |
| Clinical presentation * | ||||
| Heart failure | 2 (40) | 4 (36) | 12 (71) | 0.161 |
| Chest pain | 3 (60) | 4 (36) | 2 (12) | 0.074 |
| Tachyarrhythmia | 0 | 3 (27) | 4 (24) | 0.440 |
| Bradyarrhythmia/Heart block | 2 (40) | 1 (9) | 3 (18) | 0.330 |
| Sudden cardiac death | 0 | 1 (9) | 0 | 0.357 |
| Other | 0 | 0 | 1 (6) | 0.616 |
| Clinical course | ||||
| Fulminant | 3 (60) | 4 (36) | 6 (35) | 0.591 |
| Control No. | Gender | Age (Years) | Cause of Death | Clinical Background |
|---|---|---|---|---|
| 1 | M | 62 | Subarachnoid haemorrhage | Atrial fibrillation, previous Maze surgery |
| 2 | M | 63 | Cardiac arrest | Previous mitral valve replacement |
| 3 | F | 50 | Intracerebral haemorrhage | Previous ventricular tachycardia, suspected previous AMI, suspected Takotsubo cardiomyopathy in the acute setting |
| 4 | F | 63 | Ischemic cerebral oedema, due to cardiac arrest | Ischemic heart disease, obesity, hypertension, diabetes mellitus type 2, hypothyroidism, renal insufficiency, emphysema |
| 5 | F | 19 | Ischemic cerebral oedema due to cardiac arrest | Anorexia |
| 6 | F | 42 | Intracerebral haemorrhage | Takotsubo cardiomyopathy in the acute setting |
| 7 | F | 43 | Ischemic cerebral oedema due to cardiac arrest caused by major bleeding | None |
| 8 | M | 24 | Cardiac arrest | Hypertrophic cardiomyopathy, athlete |
| Patient No. | Gender | Age (Years) | Diagnosis | Endomyocardial Biopsy */Explant | SSTR2 Positive Staining | |
|---|---|---|---|---|---|---|
| Mononuclear Inflammatory Cells | Multinuclear Giant Cells | |||||
| 1 | F | 29 | LM | 2/3 | +++ | |
| 2 | F | 71 | LM | 2/4 | + | |
| 3 | F | 21 | LM | 3/3 | + | |
| 4 | M | 29 | LM | 4/4 | + | |
| 5 | M | 63 | LM | 3/4 | + | |
| 6 | F | 71 | GCM | 4/4 | + | +++ |
| 7 | F | 53 | GCM | 8/8 | ++ | ++ |
| 8 | M | 54 | GCM | 3/3 | ++ | +++ |
| 9 | M | 78 | GCM | 3/3 | - | ++ |
| 10 | M | 54 | GCM | 4/5 | ++ | +++ |
| 11 | M | 60 | GCM | 1/2 | ++ | ++ |
| 12 | M | 19 | GCM | 1/1 | + | ++ |
| 13 | F | 56 | GCM | 2/2 | +++ | +++ |
| 14 | F | 48 | GCM | 7/7 | ++ | +++ |
| 15 | F | 51 | GCM | Explant | + | ++ |
| 16 | F | 74 | GCM | 2/2 | ++ | ++ |
| 17 | F | 54 | CS | 2/4 | ++ | +++ |
| 18 | M | 59 | CS | 2/2 | ++ | +++ |
| 19 | M | 63 | CS | 2/5 | ++ | +++ |
| 20 | M | 58 | CS | 2/6 | ++ | +++ |
| 21 | M | 52 | CS | 2/3 | + | +++ |
| 22 | M | 58 | CS | 1/2 | + | +++ |
| 23 | F | 52 | CS | 1/4 | + | +++ |
| 24 | M | 48 | CS | 3/5 | + | +++ |
| 25 | F | 51 | CS | Explant | + | +++ |
| 26 | F | 66 | CS | Explant | + | +++ |
| 27 | M | 61 | CS | 1/4 | ++ | +++ |
| 28 | M | 64 | CS | 4/7 | ++ | +++ |
| 29 | M | 63 | CS | Explant | ++ | +++ |
| 30 | F | 57 | CS | Explant | + | +++ |
| 31 | F | 44 | CS | Explant | + | +++ |
| 32 | F | 59 | CS | 3/4 | ++ | +++ |
| 33 | M | 55 | CS | 1/4 | + | +++ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polte, C.L.; Visuttijai, K.; Vukusic, K.; Sandstedt, J.; Sandstedt, M.; Bobbio, E.; Björkenstam, M.; Karason, K.; Bergh, N.; Bollano, E.; et al. Histopathological Evaluation of Somatostatin Receptor 2 Expression in Myocarditis—Rationale for the Diagnostic Use of Somatostatin Receptor Imaging. Diagnostics 2024, 14, 2374. https://doi.org/10.3390/diagnostics14212374
Polte CL, Visuttijai K, Vukusic K, Sandstedt J, Sandstedt M, Bobbio E, Björkenstam M, Karason K, Bergh N, Bollano E, et al. Histopathological Evaluation of Somatostatin Receptor 2 Expression in Myocarditis—Rationale for the Diagnostic Use of Somatostatin Receptor Imaging. Diagnostics. 2024; 14(21):2374. https://doi.org/10.3390/diagnostics14212374
Chicago/Turabian StylePolte, Christian L., Kittichate Visuttijai, Kristina Vukusic, Joakim Sandstedt, Mikael Sandstedt, Emanuele Bobbio, Marie Björkenstam, Kristjan Karason, Niklas Bergh, Entela Bollano, and et al. 2024. "Histopathological Evaluation of Somatostatin Receptor 2 Expression in Myocarditis—Rationale for the Diagnostic Use of Somatostatin Receptor Imaging" Diagnostics 14, no. 21: 2374. https://doi.org/10.3390/diagnostics14212374
APA StylePolte, C. L., Visuttijai, K., Vukusic, K., Sandstedt, J., Sandstedt, M., Bobbio, E., Björkenstam, M., Karason, K., Bergh, N., Bollano, E., & Oldfors, A. (2024). Histopathological Evaluation of Somatostatin Receptor 2 Expression in Myocarditis—Rationale for the Diagnostic Use of Somatostatin Receptor Imaging. Diagnostics, 14(21), 2374. https://doi.org/10.3390/diagnostics14212374