
Location, Location, Location: A Pilot Study to Compare Electrical with Echocardiographic-Guided Targeting of Left Ventricular Lead Placement in Cardiac Resynchronisation Therapy
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population and Study Protocol
2.2. Baseline Assessment
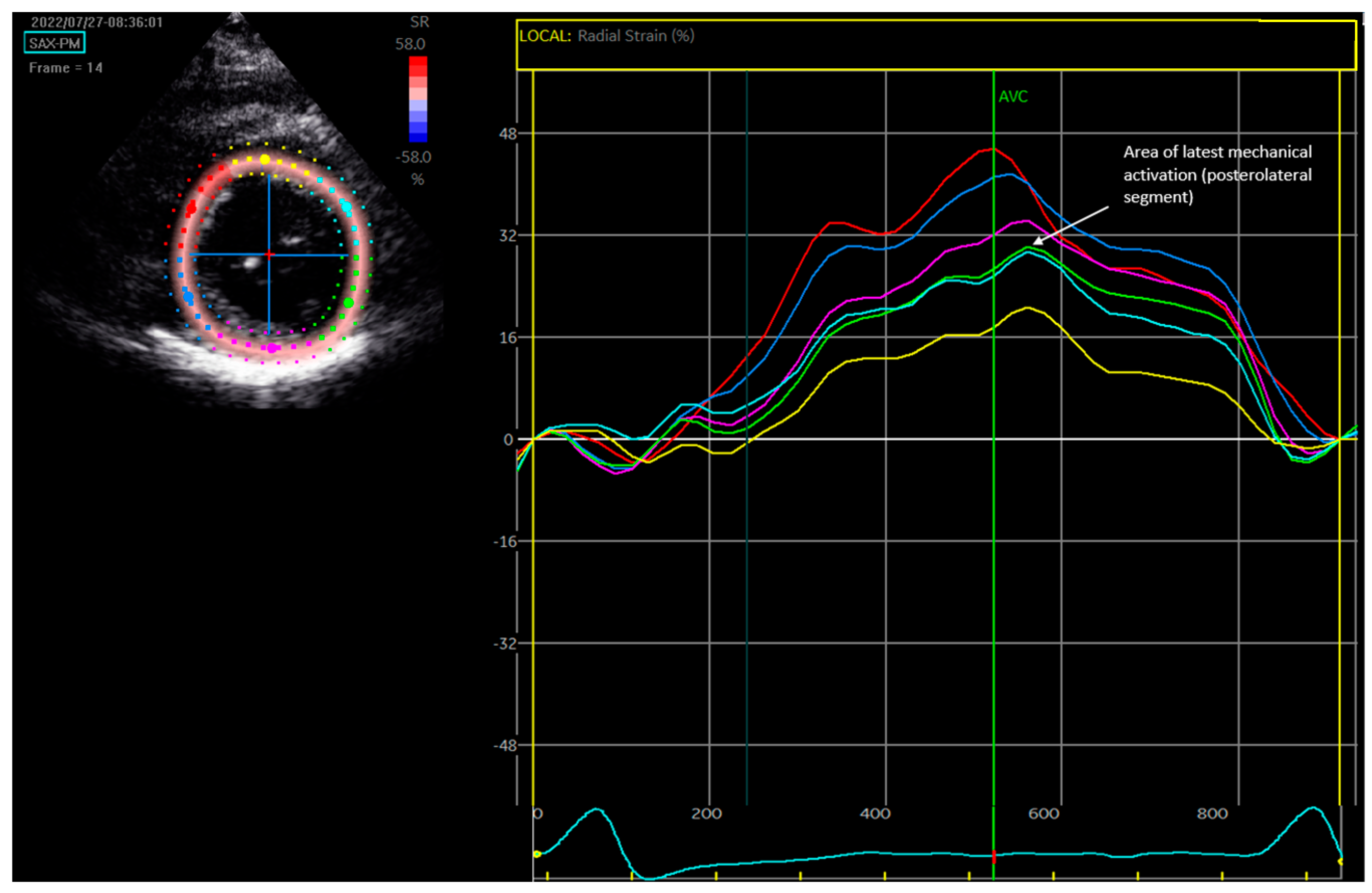
2.3. Speckle-Tracking Radial Strain Echocardiography
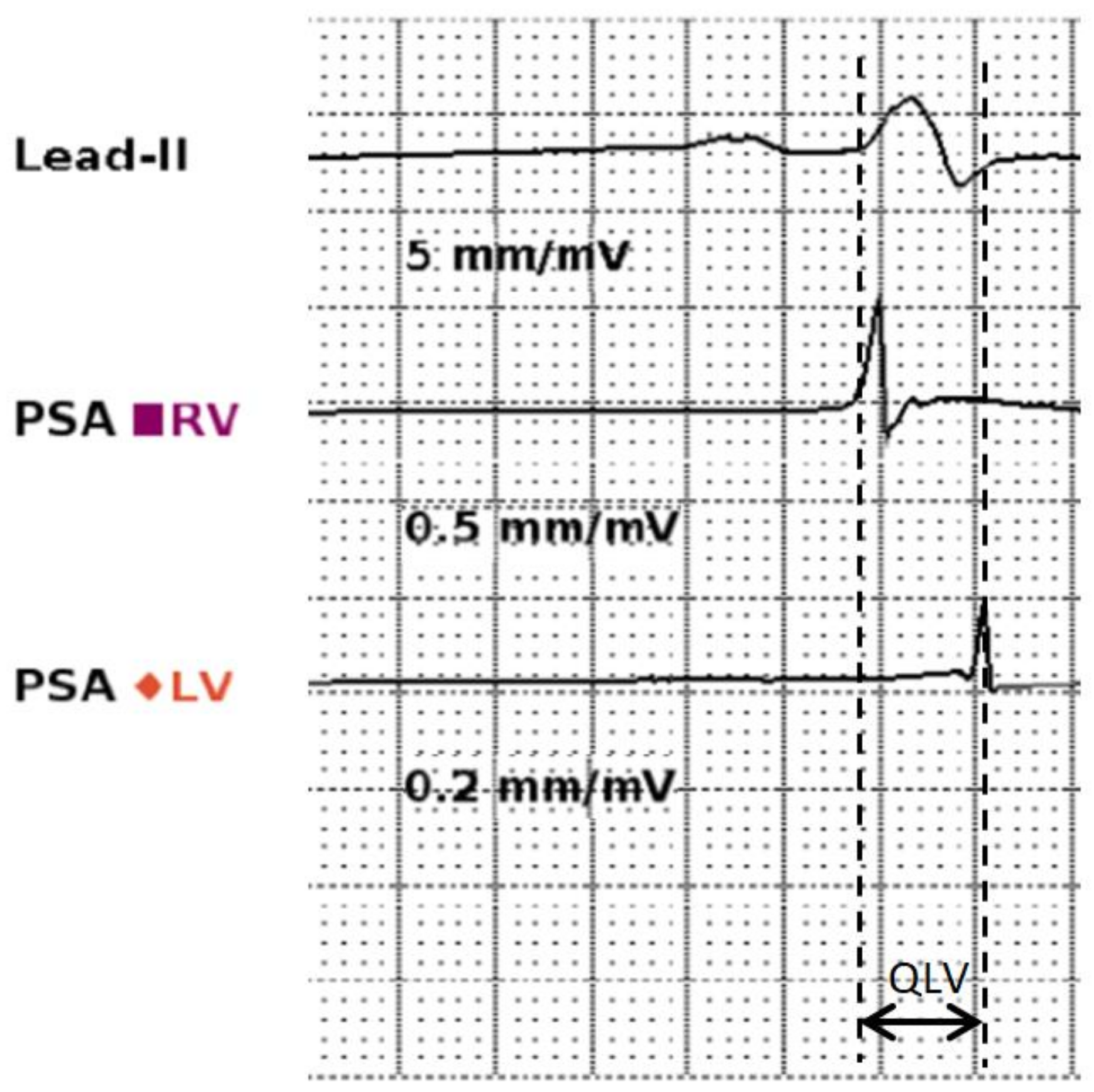
2.4. QLV Measurement
2.5. R-Wave Amplitude Measurement
2.6. CRT Implantation
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Implant Characteristics
3.3. Comparison of Procedural Elements to Published Standards
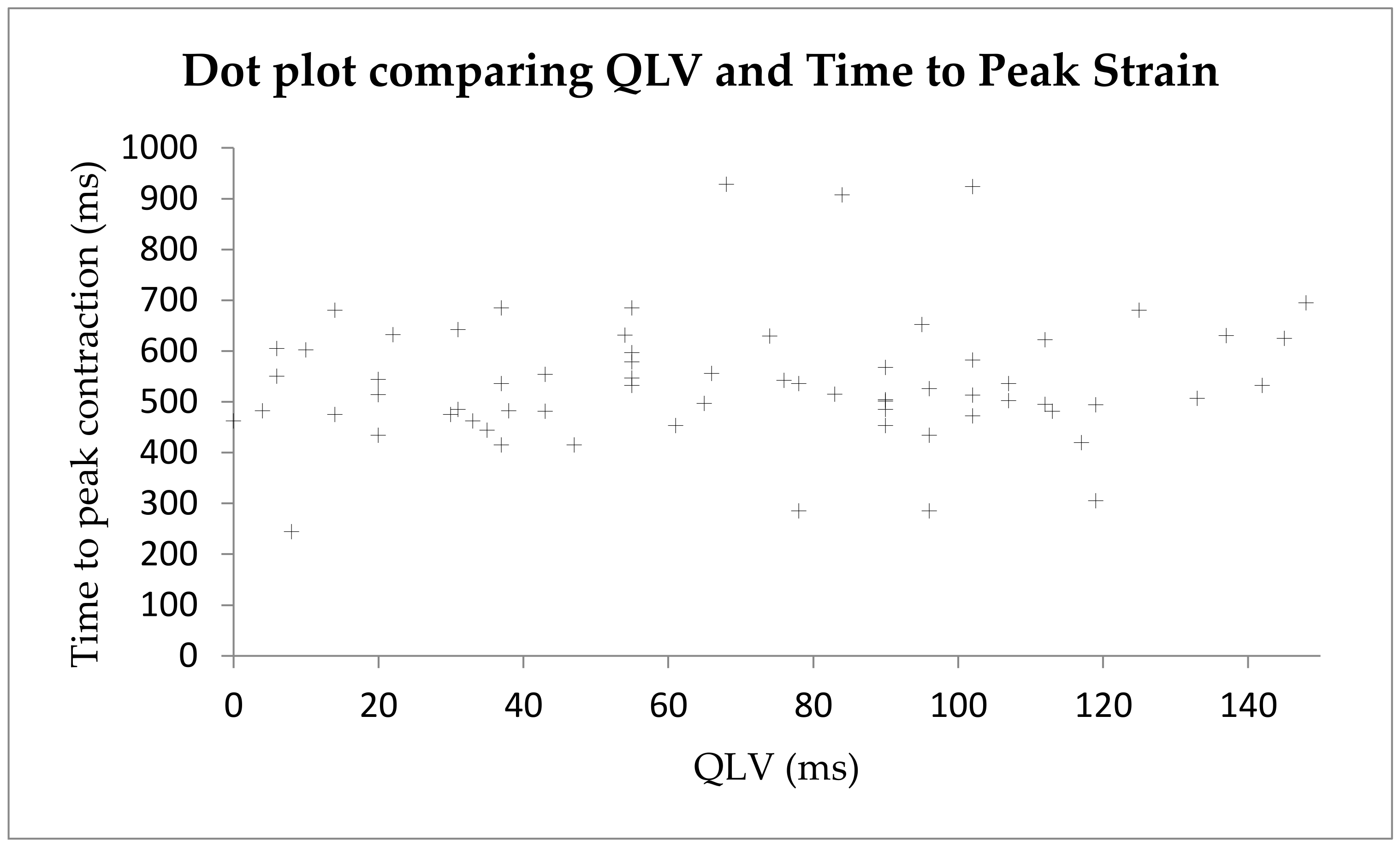
3.4. Comparing QLV and Radial Strain for Identification of the Area of Latest Activation
3.5. Comparing Sensed R-Wave Amplitude and Strain Amplitude Defined LV Scar
4. Discussion
4.1. Summary of Results
4.2. The Evidence for Targeting the Area of Latest Electrical Activation
4.3. Why Is Imaging-Based Targeting Insufficient?
4.4. Coronary Sinus Anatomy
4.5. Future Directions
4.6. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Epstein, A.E.; DiMarco, J.P.; Ellenbogen, K.A.; Estes, N.A., 3rd; Freedman, R.A.; Gettes, L.S.; Gillinov, A.M.; Gregoratos, G.; Hammill, S.C.; Hayes, D.L.; et al. 2012 ACCF/AHA/HRS Focused Update of the 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. J. Am. Coll. Cardiol. 2013, 61, e6–e75. [Google Scholar]
- 2021 ESC Guidelines on Cardiac Pacing and Cardiac Resynchronization Therapy. Available online: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Cardiac-Pacing-and-Cardiac-Resynchronization-Therapy (accessed on 8 May 2022).
- Sieniewicz, B.J.; Gould, J.; Porter, B.; Sidhu, B.S.; Teall, T.; Webb, J.; Carr-White, G.; Rinaldi, C.A. Understanding non-response to cardiac resynchronisation therapy: Common problems and potential solutions. Heart Fail. Rev. 2019, 24, 41–54. [Google Scholar] [CrossRef]
- Daubert, C.; Behar, N.; Martins, R.P.; Mabo, P.; Leclercq, C. Avoiding non-responders to cardiac resynchronization therapy: A practical guide. Eur. Heart J. 2017, 38, 1463–1472. [Google Scholar] [CrossRef]
- Chousou, P.A.; Pugh, P.J. How to deliver optimal cardiac resynchronisation therapy. Heart Br. Card. Soc. 2017, 2017, 311210. [Google Scholar] [CrossRef]
- Khan, F.Z.; Virdee, M.S.; Palmer, C.R.; Pugh, P.J.; O’Halloran, D.; Elsik, M.; Read, P.A.; Begley, D.; Fynn, S.P.; Dutka, D.P. Targeted Left Ventricular Lead Placement to Guide Cardiac Resynchronization Therapy: The TARGET Study: A Randomized, Controlled Trial. J. Am. Coll. Cardiol. 2012, 59, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- Saba, S.; Marek, J.; Schwartzman, D.; Jain, S.; Adelstein, E.; White, P.; Gorcsan, J.; Saba, S. Echocardiography-guided left ventricular lead placement for cardiac resynchronization therapy: Results of the Speckle Tracking Assisted Resynchronization Therapy for Electrode Region trial. Circ. Heart Fail. 2013, 6, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Bleeker, G.B.; Kaandorp, T.A.M.; Lamb, H.J.; Boersma, E.; Steendijk, P.; de Roos, A.; van der Wall, E.E.; Schalij, M.J.; Bax, J.J. Effect of Posterolateral Scar Tissue on Clinical and Echocardiographic Improvement After Cardiac Resynchronization Therapy. Circulation 2006, 113, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.J.; Umar, F.; Panting, J.R.; Stegemann, B.; Leyva, F. Left ventricular lead position, mechanical activation, and myocardial scar in relation to left ventricular reverse remodeling and clinical outcomes after cardiac resynchronization therapy: A feature-tracking and contrast-enhanced cardiovascular magnetic resonance study. Heart Rhythm 2016, 13, 481–489. [Google Scholar] [PubMed]
- Pazhenkottil, A.P.; Buechel, R.R.; Nkoulou, R.; Ghadri, J.-R.; Herzog, B.A.; Husmann, L.; Wolfrum, M.; Küest, S.M.; Fiechter, M.; Gaemperli, O.; et al. Left ventricular dyssynchrony assessment by phase analysis from gated PET-FDG scans. J. Nucl. Cardiol. 2011, 18, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Borgquist, R.; Carlsson, M.; Markstad, H.; Werther-Evaldsson, A.; Ostenfeld, E.; Roijer, A.; Bakos, Z. Cardiac Resynchronization Therapy Guided by Echocardiography, MRI, and CT Imaging: A Randomized Controlled Study. JACC Clin. Electrophysiol. 2020, 6, 1300–1309. [Google Scholar] [CrossRef]
- Sommer, A.; Kronborg, M.B.; Nørgaard, B.L.; Poulsen, S.H.; Bouchelouche, K.; Böttcher, M.; Jensen, H.K.; Jensen, J.M.; Kristensen, J.; Gerdes, C.; et al. Multimodality imaging-guided left ventricular lead placement in cardiac resynchronization therapy: A randomized controlled trial. Eur. J. Heart Fail. 2016, 18, 1365–1374. [Google Scholar] [CrossRef] [PubMed]
- Kydd, A.C.; Khan, F.; Gopalan, D.; Ring, L.; Rana, B.S.; Virdee, M.S.; Dutka, D.P. Utility of speckle tracking echocardiography to characterize dysfunctional myocardium in patients with ischemic cardiomyopathy referred for cardiac resynchronization therapy. Echocardiography 2014, 31, 736–743. [Google Scholar] [CrossRef]
- Gold, M.R.; Birgersdotter-Green, U.; Singh, J.P.; Ellenbogen, K.A.; Yu, Y.; Meyer, T.E.; Seth, M.; Tchou, P.J. The relationship between ventricular electrical delay and left ventricular remodelling with cardiac resynchronization therapy. Eur. Heart J. 2011, 32, 2516–2524. [Google Scholar] [CrossRef] [PubMed]
- Nayar, V.; Khan, F.Z.; Pugh, P.J. Optimizing atrioventricular and interventricular intervals following cardiac resynchronization therapy. Expert. Rev. Cardiovasc. Ther. 2011, 9, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. Practical Statistics for Medical Research: 12, 1st ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 1990; 624p. [Google Scholar]
- Khan, F.Z.; Virdee, M.S.; Gopalan, D.; Rudd, J.; Watson, T.; Fynn, S.P.; Dutka, D.P. Characterization of the suitability of coronary venous anatomy for targeting left ventricular lead placement in patients undergoing cardiac resynchronization therapy. Europace 2009, 11, 1491–1495. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, N.A.; Gold, M.R.; Waggoner, A.D.; Picard, M.H.; Stein, K.M.; Yu, Y.; Meyer, T.E.; Wold, N.; Ellenbogen, K.A.; Singh, J.P. Longer Left Ventricular Electric Delay Reduces Mitral Regurgitation After Cardiac Resynchronization Therapy: Mechanistic Insights From the SMART-AV Study (SmartDelay Determined AV Optimization: A Comparison to Other AV Delay Methods Used in Cardiac Resynchronization Therapy). Circ. Arrhythm. Electrophysiol. 2016, 9, e004346. [Google Scholar] [PubMed]
- Roubicek, T.; Wichterle, D.; Kucera, P.; Nedbal, P.; Kupec, J.; Sedlakova, J.; Cerny, J.; Stros, J.; Kautzner, J.; Polasek, R. Left Ventricular Lead Electrical Delay Is a Predictor of Mortality in Patients with Cardiac Resynchronization Therapy. Circ. Arrhythm. Electrophysiol. 2015, 8, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.P.; Berger, R.D.; Doshi, R.N.; Lloyd, M.; Moore, D.; Stone, J.; Daoud, E.G.; ENHANCE CRT Study Group. Targeted Left Ventricular Lead Implantation Strategy for Non-Left Bundle Branch Block Patients: The ENHANCE CRT Study. JACC Clin. Electrophysiol. 2020, 6, 1171–1181. [Google Scholar] [CrossRef] [PubMed]
- Stephansen, C.; Sommer, A.; Kronborg, M.B.; Jensen, J.M.; Nørgaard, B.L.; Gerdes, C.; Kristensen, J.; Jensen, H.K.; Fyenbo, D.B.; Bouchelouche, K.; et al. Electrically vs. imaging-guided left ventricular lead placement in cardiac resynchronization therapy: A randomized controlled trial. Europace 2019, 21, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Field, M.E.; Yu, N.; Wold, N.; Gold, M.R. Comparison of measures of ventricular delay on cardiac resynchronization therapy response. Heart Rhythm. 2020, 17, 615–620. [Google Scholar] [CrossRef]
- Fyenbo, D.B.; Sommer, A.; Nørgaard, B.L.; Kronborg, M.B.; Kristensen, J.; Gerdes, C.; Jensen, H.K.; Jensen, J.M.; Nielsen, J.C. Long-term outcomes in a randomized controlled trial of multimodality imaging-guided left ventricular lead placement in cardiac resynchronization therapy. Europace 2022, 24, 828–834. [Google Scholar] [CrossRef]
- Vinther, M.; Risum, N.; Philbert, B.T. A large inherent delay between the ECG and EGM signals in the pacing system analyzer from Medtronic makes it unsuitable to estimate timing events during CRT implantation. J. Electrocardiol. 2020, 58, 33–36. [Google Scholar] [CrossRef]
- van Dam, P.M.; Melgaard, J.; Fruelund, P.Z.; Sommer, A.; Riahi, S.; Graff, C. Po-662-06 Estimating Qlv from the 12-Lead Ecg to Support Cardiac Resynchronization Therapy Selection And Implant Procedures. Heart Rhythm. 2022, 19 (Suppl. S5), S291. [Google Scholar] [CrossRef]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.A.; Cleland, J.; Deharo, J.C.; Delgado, V.; Elliott, P.M. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Europace 2013, 15, 1070–1118. [Google Scholar] [PubMed]
- Friedman, D.J.; Singh, J.P. Is Image Guidance for Left Ventricular Lead Targeting Overkill? JACC Clin. Electrophysiol. 2020, 6, 1310–1312. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 22 | |
|---|---|
| Patient Demographics | |
| Age (years) | 73.2 ± 9.00 |
| Male | 17 (77.2) |
| CRT-P | 14 (63.6) |
| CRT-D | 8 (36.4) |
| NYHA 1 | 0 (0) |
| NYHA 2 | 7 (31.8) |
| NYHA 3 | 13 (59.1) |
| NYHA 4 | 2 (9.1) |
| Pre-implant ECG | |
| QRS duration (msec) | 159.8 ± 17.5 |
| PR duration (msec) | 186.2 ± 36.0 |
| Heart failure phenotype | |
| Ischaemic | 8 (36.4) |
| Non-ischaemic | 14 (63.6) |
| Pharmoctherapy | |
| Beta-blocker | 21 (95.5) |
| MRA | 11 (50.0) |
| RAASi | 21 (95.5) |
| ACEi | 13 (59.1) |
| ARB | 4 (18.2) |
| ARNi | 4 (18.2) |
| Sufficient quality echo for strain analysis | 19 (86.4) |
| n = 22 | |
|---|---|
| Presence of coronary sinus branch | |
| Posterior vein | 8 (36.4) |
| Posterolateral vein | 11 (50.0) |
| Lateral vein | 22 (100) |
| Anterolateral vein | 14 (63.6) |
| Anterior vein | 18 (81.8) |
| Site of LV lead placement | |
| Posterior vein | 4 (18.2) |
| Posterolateral vein | 4 (18.2) |
| Lateral vein | 14 (63.6) |
| Anterolateral vein | 0 (0) |
| Anterior vein | 0 (0) |
| Number of accessible coronary sinus branches | |
| 1 | 1 (4.54) |
| 2 | 2 (9.09) |
| 3 | 9 (40.9) |
| 4 | 9 (40.9) |
| 5 | 1 (4.54) |
| Lead type | |
| Unipolar | 2 (9.09) |
| Bipolar | 4 (18.2) |
| Quadripolar | 16 (72.7) |
| Procedure time (minutes) | 124.3 (47.4) |
| Contrast volume (mL) | 54.3 (67.8) |
| Skin dose (mGy/m2) | 330.1 (396.6) |
| Fluoroscopy time (minutes) | 29.3 (20.2) |
| Number of procedures by senior trainee | 9 (40.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chousou, P.A.; Chattopadhyay, R.K.; Matthews, G.D.K.; Vassiliou, V.S.; Pugh, P.J. Location, Location, Location: A Pilot Study to Compare Electrical with Echocardiographic-Guided Targeting of Left Ventricular Lead Placement in Cardiac Resynchronisation Therapy. Diagnostics 2024, 14, 299. https://doi.org/10.3390/diagnostics14030299
Chousou PA, Chattopadhyay RK, Matthews GDK, Vassiliou VS, Pugh PJ. Location, Location, Location: A Pilot Study to Compare Electrical with Echocardiographic-Guided Targeting of Left Ventricular Lead Placement in Cardiac Resynchronisation Therapy. Diagnostics. 2024; 14(3):299. https://doi.org/10.3390/diagnostics14030299
Chicago/Turabian StyleChousou, Panagiota A., Rahul K. Chattopadhyay, Gareth D. K. Matthews, Vassilios S. Vassiliou, and Peter J. Pugh. 2024. "Location, Location, Location: A Pilot Study to Compare Electrical with Echocardiographic-Guided Targeting of Left Ventricular Lead Placement in Cardiac Resynchronisation Therapy" Diagnostics 14, no. 3: 299. https://doi.org/10.3390/diagnostics14030299