
Clinicopathologic and Endosonographic Characteristics of Colon Subepithelial Tumors Discovered Incidentally


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Patients
2.2. Instruments
2.3. Procedures
2.4. Variables and Definition
2.5. Statistical Analysis
3. Results
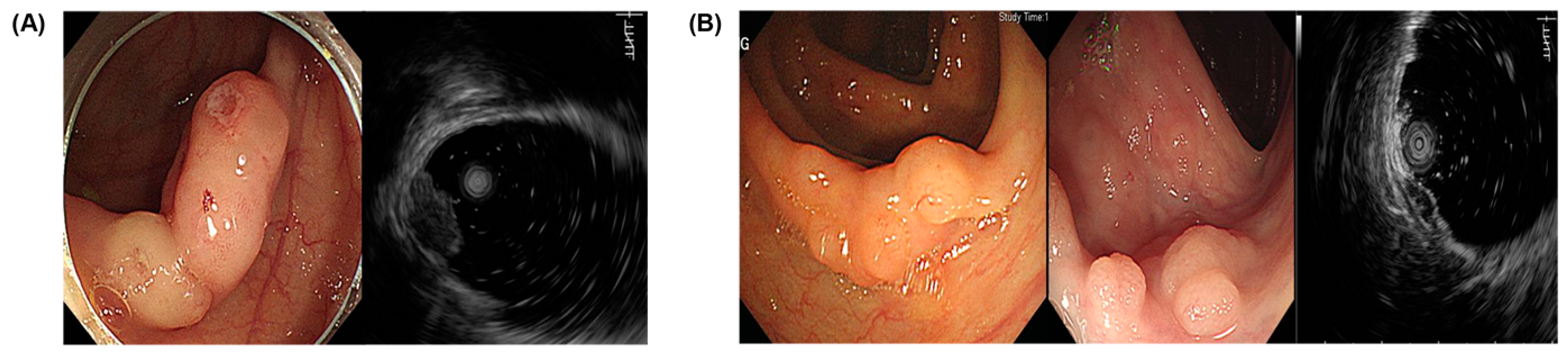
3.1. Endoscopic and EUS Characteristics
3.2. Histopathologic Findings
3.3. Endoscopic and Endosonographic Characteristics According to Histological Findings
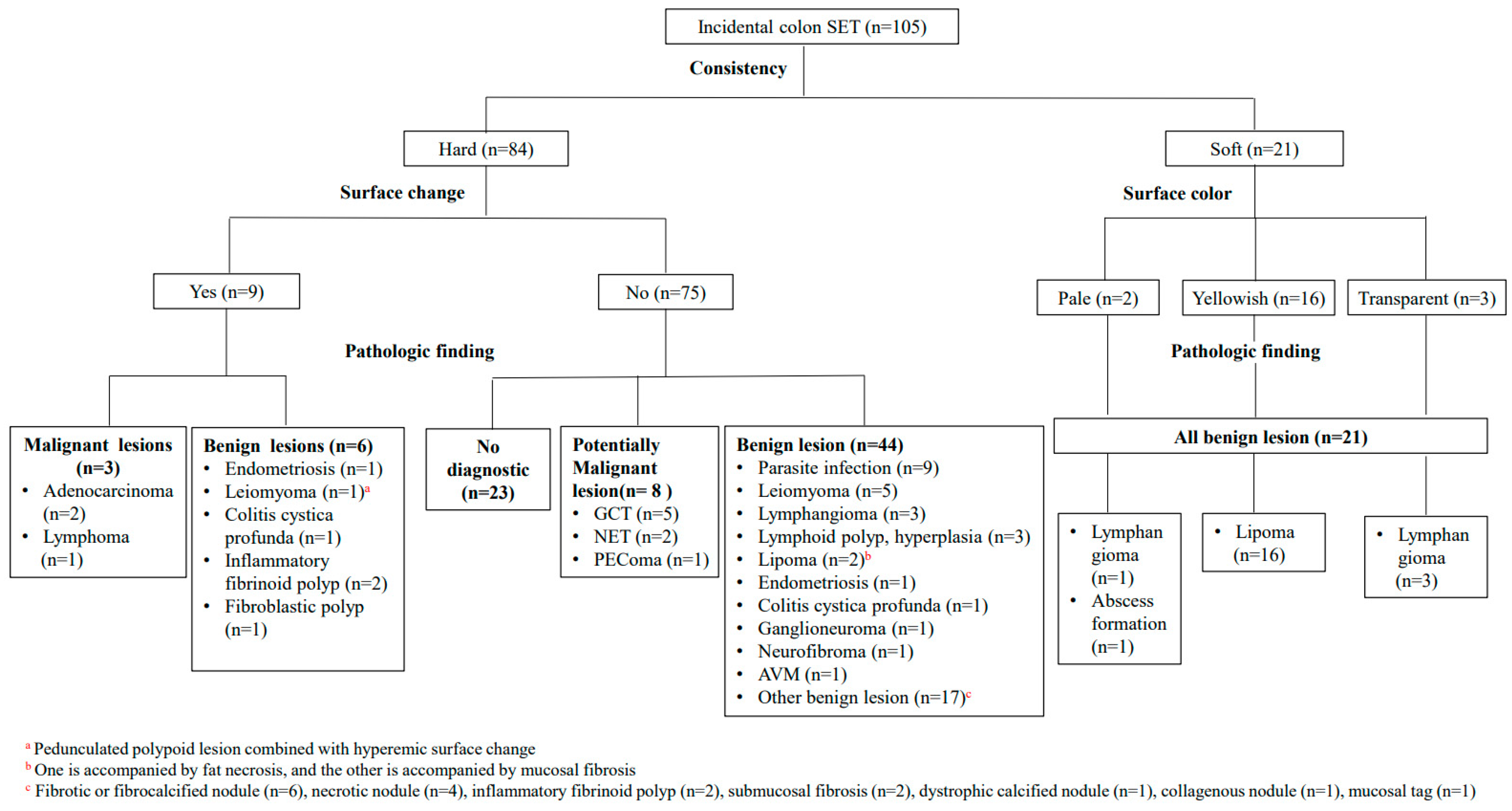
3.4. Diagnostic Approach for Incidental Colon SETs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chak, A. EUS in submucosal tumors. Gastrointest. Endosc. 2002, 56, S43–S48. [Google Scholar] [CrossRef]
- Zhou, P.H.; Yao, L.Q.; Zhong, Y.S.; He, G.J.; Xu, M.D.; Qin, X.Y. Role of endoscopic miniprobe ultrasonography in diagnosis of submucosal tumor of large intestine. World J. Gastroenterol. 2004, 10, 2444–2446. [Google Scholar] [CrossRef]
- Shimizu, S.; Tada, M.; Kawai, K. Use of endoscopic ultrasonography for the diagnosis of colorectal tumors. Endoscopy 1990, 22, 31–34. [Google Scholar] [CrossRef]
- Kawamoto, K.; Ueyama, T.; Iwashita, I.; Utsunomiya, T.; Honda, H.; Onitsuka, H.; Haraguchi, Y.; Kojima, N.; Takano, H.; Masuda, K. Colonic submucosal tumors: Comparison of endoscopic US and target air-enema CT with barium enema study and colonoscopy. Radiology 1994, 192, 697–702. [Google Scholar] [CrossRef]
- Cantor, M.J.; Davila, R.E.; Faigel, D.O. Yield of tissue sampling for subepithelial lesions evaluated by EUS: A comparison between forceps biopsies and endoscopic submucosal resection. Gastrointest. Endosc. 2006, 64, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.O. Colorectal Subepithelial Lesions. Clin. Endosc. 2015, 48, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Kameyama, H.; Niwa, Y.; Arisawa, T.; Goto, H.; Hayakawa, T. Endoscopic ultrasonography in the diagnosis of submucosal lesions of the large intestine. Gastrointest. Endosc. 1997, 46, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Polkowski, M.; Butruk, E. Submucosal lesions. Gastrointest. Endosc. Clin. N. Am. 2005, 15, 33–54. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Nakajima, M.; Yoshida, S.; Kiyota, K.; Kawai, K. The diagnosis of submucosal tumors of the stomach by endoscopic ultrasonography. Gastrointest. Endosc. 1989, 35, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Caletti, G.; Zani, L.; Bolondi, L.; Brocchi, E.; Rollo, V.; Barbara, L. Endoscopic ultrasonography in the diagnosis of gastric submucosal tumor. Gastrointest. Endosc. 1989, 35, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Rösch, T.; Lorenz, R.; Dancygier, H.; von Wickert, A.; Classen, M. Endosonographic diagnosis of submucosal upper gastrointestinal tract tumors. Scand. J. Gastroenterol. 1992, 27, 1–8. [Google Scholar] [CrossRef]
- Takada, N.; Higashino, M.; Osugi, H.; Tokuhara, T.; Kinoshita, H. Utility of endoscopic ultrasonography in assessing the indications for endoscopic surgery of submucosal esophageal tumors. Surg. Endosc. 1999, 13, 228–230. [Google Scholar] [CrossRef]
- Maione, F.; Chini, A.; Milone, M.; Gennarelli, N.; Manigrasso, M.; Maione, R.; Cassese, G.; Pagano, G.; Tropeano, F.P.; Luglio, G.; et al. Diagnosis and Management of Rectal Neuroendocrine Tumors (NETs). Diagnostics 2021, 11, 771. [Google Scholar] [CrossRef]
- Chablaney, S.; Zator, Z.A.; Kumta, N.A. Diagnosis and Management of Rectal Neuroendocrine Tumors. Clin. Endosc. 2017, 50, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Geboes, K.; De Wolf-Peeters, C.; Rutgeerts, P.; Vantrappen, G.; Desmet, V. Submucosal tumors of the colon: Experience with twenty-five cases. Dis. Colon Rectum 1978, 21, 420–425. [Google Scholar] [CrossRef]
- Aibe, T.; Fuji, T.; Okita, K.; Takemoto, T. A fundamental study of normal layer structure of the gastrointestinal wall visualized by endoscopic ultrasonography. Scand. J. Gastroenterol. Suppl. 1986, 123, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Kimmey, M.B.; Martin, R.W.; Haggitt, R.C.; Wang, K.Y.; Franklin, D.W.; Silverstein, F.E. Histologic correlates of gastrointestinal ultrasound images. Gastroenterology 1989, 96, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Fujimaki, E.; Kano, A.; Katayama, S.; Terasaki, K.; Kawata, T.; Tochinai, H. Endoscopic study of submucosal tumors of the lower GI tract. Gastroenterol. Endosc. 1987, 29, 1149–1156, (In Japanese with English Abstract). [Google Scholar]
- Gast, P.; Belaïche, J. Rectal endosonography in inflammatory bowel disease: Differential diagnosis and prediction of remission. Endoscopy 1999, 31, 158–166. [Google Scholar] [CrossRef]
- Mo, L.R.; Tseng, L.J.; Jao, Y.T.; Lin, R.C.; Wey, K.C.; Wang, C.H. Balloon sheath miniprobe compared to conventional EUS in the staging of colorectal cancer. Hepatogastroenterology 2002, 49, 980–983. [Google Scholar]
- Shimizu, S.; Myojo, S.; Nagashima, M.; Okuyama, Y.; Sugeta, N.; Sakamoto, S.; Kutsumi, H.; Otsuka, H.; Suyama, Y.; Fujimoto, S. A patient with rectal cancer associated with ulcerative colitis in whom endoscopic ultrasonography was useful for diagnosis. J. Gastroenterol. 1999, 34, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Rösch, T.; Kapfer, B.; Will, U.; Baronius, W.; Strobel, M.; Lorenz, R.; Ulm, K. Accuracy of endoscopic ultrasonography in upper gastrointestinal submucosal lesions: A prospective multicenter study. Scand. J. Gastroenterol. 2002, 37, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.A.; Gunasagaran, J.; Pailoor, J. Granular cell tumour: Malignant or benign? Singapore Med. J. 2015, 56, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Jetmore, A.B.; Ray, J.E.; Gathright, J.B., Jr.; McMullen, K.M.; Hicks, T.C.; Timmcke, A.E. Rectal carcinoids: The most frequent carcinoid tumor. Dis. Colon Rectum 1992, 35, 717–725. [Google Scholar] [CrossRef]
- Sohn, D.K.; Choi, H.S.; Chang, Y.S.; Huh, J.M.; Kim, D.H.; Kim, D.Y.; Kim, Y.H.; Chang, H.J.; Jung, K.H.; Jeong, S.Y. Granular cell tumor of colon: Report of a case and review of literature. World J. Gastroenterol. 2004, 10, 2452–2454. [Google Scholar] [CrossRef]
- Polkowski, M. Endoscopic ultrasound and endoscopic ultrasound-guided fine-needle biopsy for the diagnosis of malignant submucosal tumors. Endoscopy 2005, 37, 635–645. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. (%) |
|---|---|
| Location | |
| Cecum | 16 (15.2%) |
| Ascending colon | 17 (16.2%) |
| Hepatic flexure | 6 (5.7%) |
| Transverse colon | 32 (30.5%) |
| Splenic flexure | 2 (1.9%) |
| Descending colon | 3 (2.9%) |
| Sigmoid descending junction | 2 (1.9%) |
| Sigmoid colon | 20 (19.0%) |
| Rectosigmoid junction | 7 (6.7%) |
| Size (mm) | |
| <10 | 88 (83.8%) |
| ≥10 | 17 (16.2%) |
| Consistency | |
| Hard | 84 (80%) |
| Soft | 21 (20%) |
| Color | |
| Pale | 63 (60.0%) |
| Yellowish | 37 (35.2%) |
| Transparent | 5 (4.8%) |
| Surface change | |
| No | 96 (91.4%) |
| Yes | 9 (8.6%) |
| EUS layer of origin | |
| Muscularis mucosa (MM) | 16 (15.2%) |
| Submucosa (SM) | 54 (51.4%) |
| Proper muscle (PM) | 17 (16.2%) |
| MM + SM | 6 (5.7%) |
| SM + PM | 12 (11.4%) |
| Echogenecity | |
| Hypoechoic | 56 (53.3%) |
| Hyperechoic | 19 (18.1%) |
| Anechoic | 4 (3.8%) |
| Isoechoic | 2 (1.9%) |
| Mixed | 24 (22.9%) |
| Internal echo | |
| Homogeneous | 65 (61.9%) |
| Inhomogeneous | 40 (38.1%) |
| Pathology | No. (%) |
|---|---|
| Malignant lesion | |
| Adenocarcinoma, well differentiated | 2 (1.9%) |
| Lymphoma | 1 (1.0%) |
| Potentially malignant lesion | |
| Granular cell tumor | 5 (4.8%) |
| Neuroendocrine tumor | 2 (1.9%) |
| Perivascular epithelioid cell tumor | 1 (1.0%) |
| Benign lesion | |
| Lipoma | 18 (17.1%) |
| Parasitic infection | 9 (8.6%) |
| Lymphangioma | 7 (6.7%) |
| Leiomyoma | 6 (5.7%) |
| Fibrotic or fibrocalcified nodule | 5 (4.8%) |
| Inflammatory fibrinoid polyp | 4 (3.8%) |
| Necrotic nodule | 4 (3.8%) |
| Lymphoid polyp or hyperplasia | 3 (2.9%) |
| Endometriosis | 2 (1.9%) |
| Colitis cystica profunda | 2 (1.9%) |
| Submucosal fibrosis | 2 (1.9%) |
| Ganglioneuroma | 1 (1.0%) |
| Neurofibroma | 1 (1.0%) |
| Fibroblastic polyp | 1 (1.0%) |
| Fibrous tumor | 1 (1.0%) |
| Dystrophic calcified nodule | 1 (1.0%) |
| Collagenous nodule | 1 (1.0%) |
| Arteriovenous malformation (AVM) | 1 (1.0%) |
| Abscess formation | 1 (1.0%) |
| Mucosal tag | 1 (1.0%) |
| No diagnostic value | 23 (21.9%) |
| Total | 105 (100%) |
| Lesions | Endoscopic Finding | EUS Finding | ||||
|---|---|---|---|---|---|---|
| Consistency | Surface Change | Surface Color | Layer | Echogenecity | ||
| Malignant | Adenocarcinoma | Hard | Ulcer | Pale | Muscularis mucosa and submucosa | Hypoechoic (inhomogenous) |
| Lymphoma | Hard | Nodular changes | Pale | Muscularis mucosa | Hypoechoic | |
| Potentially malignant | Granular cell tumor | Hard | No | Yellowish | Muscularis mucosa or submucosa or multilayer | Hypoechoic |
| Neuroendocrine tumor | Hard | No | Yellowish | Muscularis mucosa or submucosa | Hypoechoic | |
| Perivascular epithelioid cell tumor | Hard | No | Pale | Proper muscle | Hypoechoic (inhomogenous) | |
| Benign | Lipoma | Mostly soft a | No | Yellowish | Submucosa | Hyperechoic |
| Parasitic infection | Hard | No | Mostly pale b | Muscularis mucosa or submucosa or multilayer | Mixed echogenicity | |
| Leiomyoma | Hard | No | Pale | Muscularis mucosa or submucosa or proper muscle | Hypoechoic c | |
| Endometriosis | Hard | No or nodular change-combined hyperemia | Pale | Multilayer | Mixed echogenicity | |
| Lymphangioma | Hard or soft | No | Pale or transparent | Submucosa | Anechoic or hypoehoic | |
| Colitis cystica profunda | Hard | No | Pale or transparent | Muscularis mucosa or submucosa | Anechoic or hypoehoic (inhomogenous) | |
| Ganglioneuroma | Hard | No | Pale | Submucosa | Hyperechoic | |
| Neurofibroma | Hard | No | Pale | Muscularis mucosa | Hypoehoic (inhomogenous) | |
| Arteriovenous malformation | Hard | No | Pale | Submucosa | Hypoehoic (inhomogenous) | |
| Lymphoid polyp or hyperplasia | Hard | No | Pale | Muscularis mucosa | Hypoehoic | |
| Fibrotic or fibrocalcified nodule | Hard | No | Pale or yellowish | Muscularis mucosa or submucosa or proper muscle | Mixed or hypoehoic (inhomogenous) | |
| Necrotic nodule | Hard | No | Pale or yellowish | Submucosa or proper muscle | Mixed echogenicity | |
| Inflammatory fibrinoid polyp | Hard | No or hyperemic change | Pale | Submucosa or proper muscle or multilayer | Mixed or hypoehoic (inhomogenous) | |
| Dystrophic calcified nodule | Hard | No | Yellowish | Submucosa | Hyperechoic | |
| Collagenous nodule | Hard | No | Pale | Submucosa and proper muscle | Mixed echogenicity | |
| Characteristics | Malignancy (n = 3) | Non-Malignancy (n = 102) | p-Value |
|---|---|---|---|
| Location | 0.55 | ||
| Right colon | 3 (100%) | 68 (66.7%) | |
| Left colon | 0 (0%) | 34 (33.3%) | |
| Size (mm) | 0.42 | ||
| <10 | 2 (66.7%) | 86 (84.3%) | |
| ≥10 | 1 (33.3%) | 16 (15.7%) | |
| Consistency | 1.00 | ||
| Hard | 3 (100%) | 81 (79.4%) | |
| Soft | 0 (0%) | 21 (20.6%) | |
| Color | 0.39 | ||
| Pale | 3 (100%) | 60 (58.8%) | |
| Yellowish | 0 (0%) | 37 (36.3%) | |
| Transparent | 0 (0%) | 5 (4.9%) | |
| Surface change | <0.001 | ||
| No | 0 (0%) | 96 (94.1%) | |
| Yes | 3 (100%) | 6 (5.9%) | |
| EUS layer of origin | 0.008 | ||
| Including muscularis mucosa (MM) a | 3 (100%) | 19 (18.6%) | |
| Others b | 0 (0%) | 83 (81.4%) | |
| Echogenecity | 0.65 | ||
| Hypoechoic | 3 (100%) | 53 (52.0%) | |
| Hyperechoic | 0 (0%) | 20 (19.6%) | |
| Anechoic | 0 (0%) | 4 (3.9%) | |
| Isoechoic | 0 (0%) | 2 (2.0%) | |
| Mixed | 0 (0%) | 23 (22.5%) | |
| Internal echo | 0.56 | ||
| Homogeneous | 1 (33.3%) | 64 (62.7%) | |
| Inhomogeneous | 2 (66.7%) | 38 (37.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, A.; Hong, S.N.; Chang, D.K.; Kim, Y.-H.; Kim, J.E.; Kim, E.R. Clinicopathologic and Endosonographic Characteristics of Colon Subepithelial Tumors Discovered Incidentally. Diagnostics 2024, 14, 551. https://doi.org/10.3390/diagnostics14050551
Kim A, Hong SN, Chang DK, Kim Y-H, Kim JE, Kim ER. Clinicopathologic and Endosonographic Characteristics of Colon Subepithelial Tumors Discovered Incidentally. Diagnostics. 2024; 14(5):551. https://doi.org/10.3390/diagnostics14050551
Chicago/Turabian StyleKim, Aryoung, Sung Noh Hong, Dong Kyung Chang, Young-Ho Kim, Ji Eun Kim, and Eun Ran Kim. 2024. "Clinicopathologic and Endosonographic Characteristics of Colon Subepithelial Tumors Discovered Incidentally" Diagnostics 14, no. 5: 551. https://doi.org/10.3390/diagnostics14050551
APA StyleKim, A., Hong, S. N., Chang, D. K., Kim, Y.-H., Kim, J. E., & Kim, E. R. (2024). Clinicopathologic and Endosonographic Characteristics of Colon Subepithelial Tumors Discovered Incidentally. Diagnostics, 14(5), 551. https://doi.org/10.3390/diagnostics14050551