
A Comparison of 68Ga-PSMA PET/CT-Based Split Renal Function with 99mTc-MAG3 Renography in Patients with Metastatic Castration-Resistant Prostate Carcinoma Treated with 177Lu-PSMA

Abstract
:1. Introduction
2. Materials and Methods
2.1. Imaging Procedure
2.1.1. 68Ga-PSMA PET/CT
2.1.2. 68Ga-PSMA PET/CT Image Analysis
2.1.3. 99mTc-MAG3 Renal Scintigraphy
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
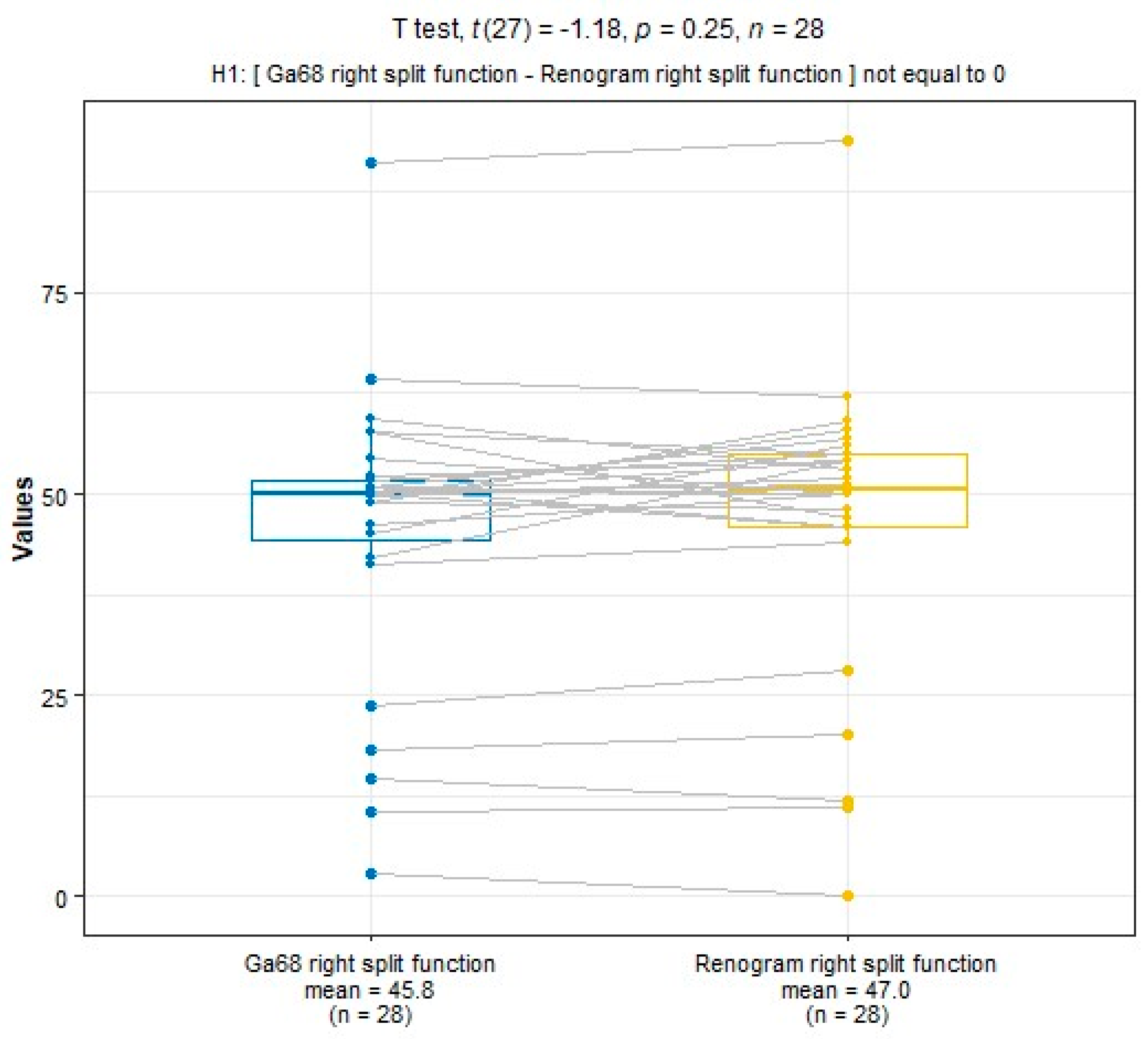
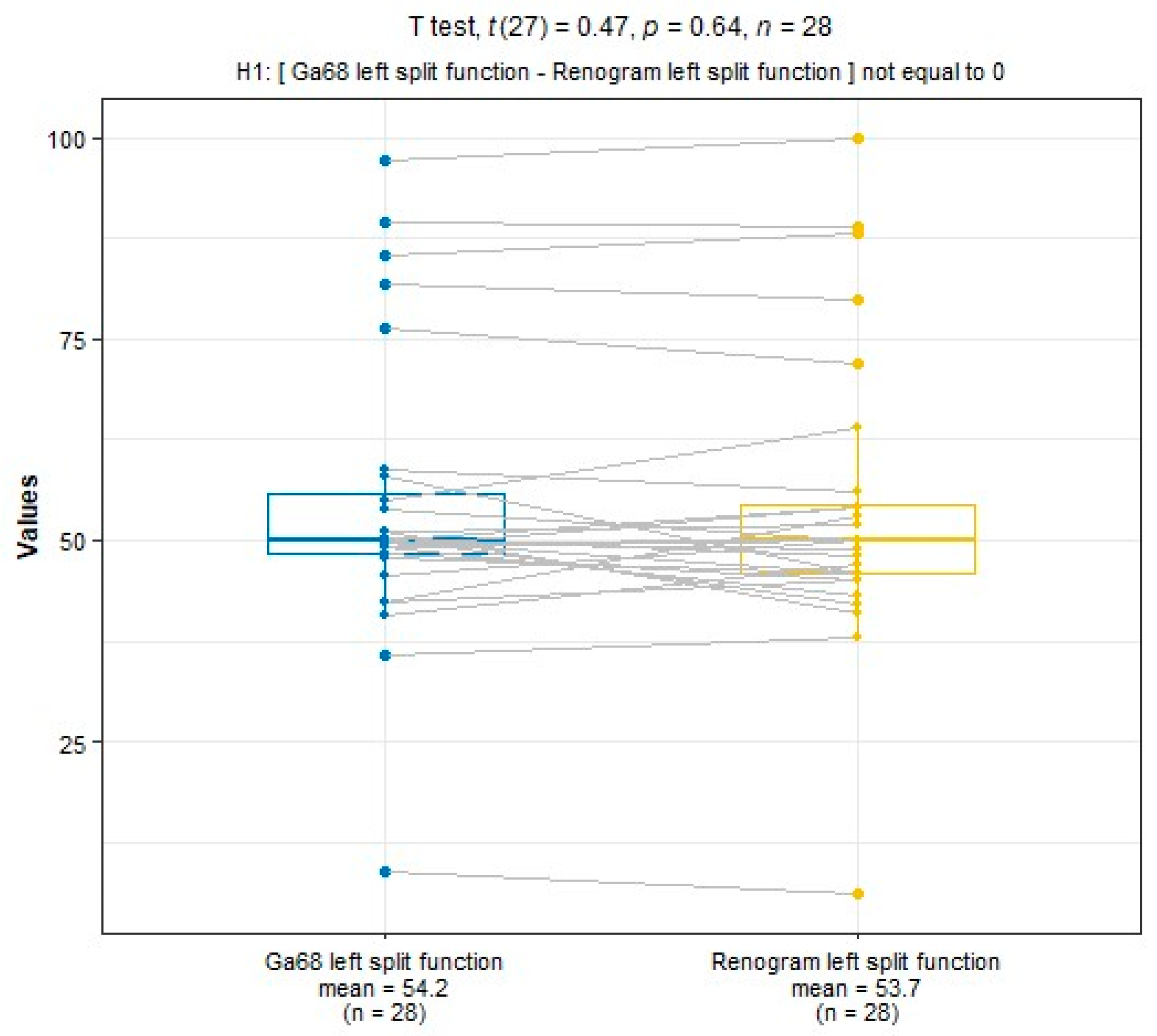
3.2. Comparison of SRF for 99mTc-MAG3 and PSMA
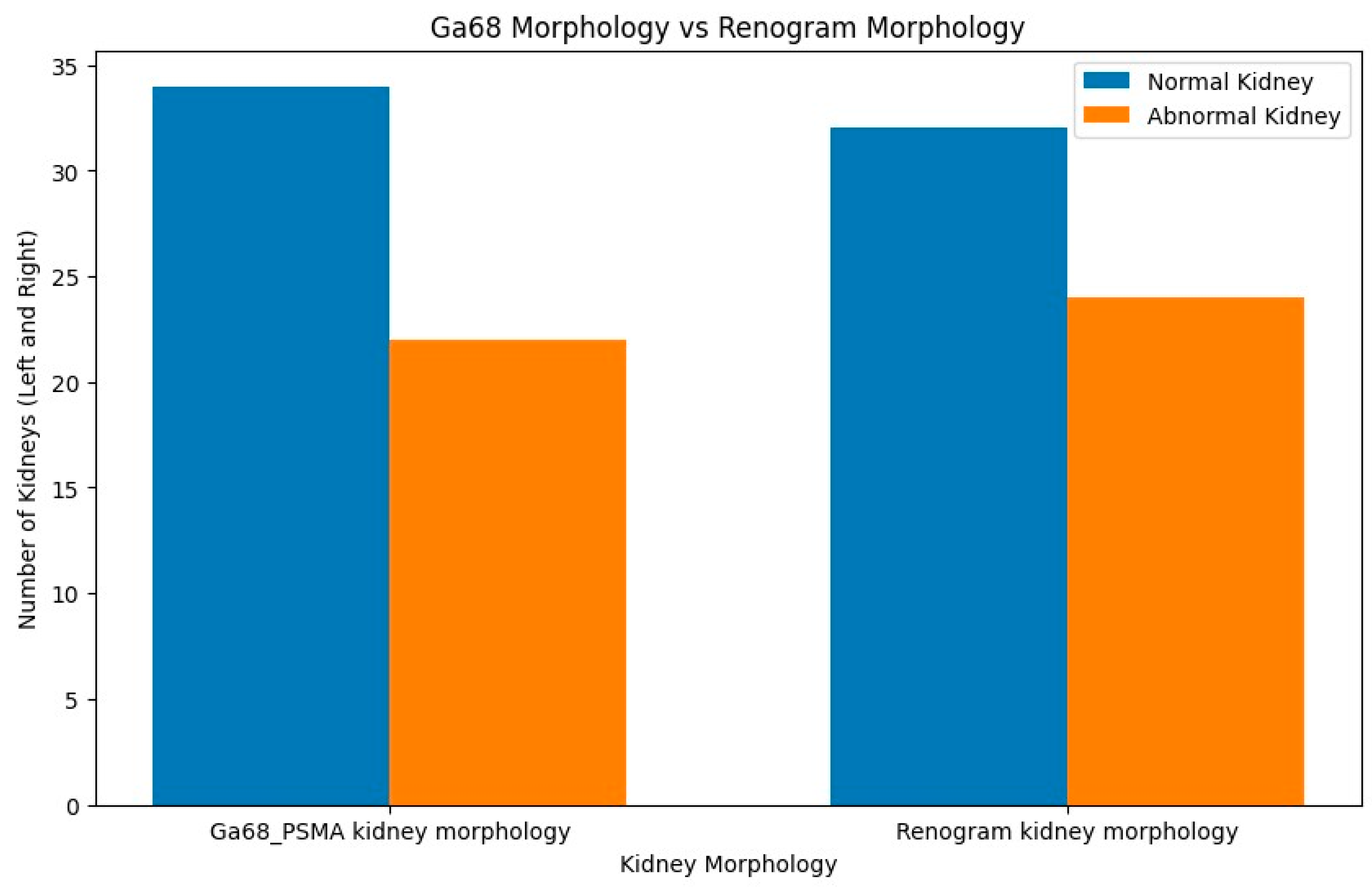
3.3. Comparison of Morphological Abnormalities
4. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | N | Method 1 | Method 2 | Correlation |
|---|---|---|---|---|---|
| Momin et al. [26] | 2018 | n = 50 | 99mTc-DMSA | 99mTc-MAG3 | 0.99 |
| Rassek et al. [28] | 2023 | n = 73 | 18F-PSMA | 99mTc-MAG3 | 0.872 |
| Rosar et al. [29] | 2020 | n = 97 | 68Ga-PSMA | 99mTc-MAG3 | 0.91 |
| Betz et al. [34] | 2021 | n = 50 | 68Ga-PSMA | 99mTc-DTPA | 0.53 |
| Present study | 2023 | n = 56 | 68Ga-PSMA | 99mTc-MAG3 | 0.957 |
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CKD | Chronic kidney disease |
| DMSA | Dimercapto succinic acid |
| DTPA | Diethylenetriamine pentaacetate |
| GFR | Glomerular filtration rate |
| MAG-3 | Mercaptoacetyltriglycine |
| mCRPC | Metastatic castration-resistant prostate cancer |
| PSA | Prostate-specific antigen |
| PSMA | Prostate-specific membrane antigen |
| RLT | Radioligand therapy |
| SRF | Split renal function |
References
- National Collaborating Centre for Cancer (UK). Prostate Cancer: Diagnosis and Treatment; National Collaborating Centre for Cancer: Cardiff, UK, 2008. Available online: https://www.ncbi.nlm.nih.gov/pubmed/21542543 (accessed on 1 March 2024).
- Sathekge, M.; Lengana, T.; Maes, A.; Vorster, M.; Zeevaart, J.; Lawal, I.; Ebenhan, T.; Van de Wiele, C. 68Ga-PSMA-11 PET/CT in primary staging of prostate carcinoma: Preliminary results on differences between black and white South-Africans. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 226–234. [Google Scholar] [CrossRef]
- Gong, J.; Kim, D.M.; Freeman, M.R.; Kim, H.; Ellis, L.; Smith, B.; Theodorescu, D.; Posadas, E.; Figlin, R.; Bhowmick, N.; et al. Genetic and biological drivers of prostate cancer disparities in Black men. Nat. Rev. Urol. 2023. [Google Scholar] [CrossRef]
- Gheybi, K.; Jiang, J.; Mutambirwa, S.B.; Soh, P.X.; Kote-Jarai, Z.; Jaratlerdsiri, W.; Eeles, R.A.; Bornman, M.R.; Hayes, V.M. Evaluating germline testing panels in southern African males with advanced prostate cancer. J. Natl. Compr. Canc. Netw. 2023, 21, 289–296. [Google Scholar] [CrossRef]
- Guo, Y.; Sigman, D.B.; Borkowski, A.; Kyprianou, N. Racial differences in prostate cancer growth: Apoptosis and cell proliferation in Caucasian and African-American patients. Prostate 2000, 42, 130–136. [Google Scholar] [CrossRef]
- Rahbar, K.; Bodei, L.; Morris, M.J. Is the vision of radioligand therapy for prostate cancer becoming a reality? An overview of the phase III VISION trial and its importance for the future of theranostics. J. Nucl. Med. 2019, 60, 1504–1506. [Google Scholar] [CrossRef]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schäfers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar]
- Emmett, L.; Willowson, K.; Violet, J.; Shin, J.; Blanksby, A.; Lee, J. Lutetium (177) PSMA radionuclide therapy for men with prostate cancer: A review of the current literature and discussion of practical aspects of therapy. J. Med. Radiat. Sci. 2017, 64, 52–60. [Google Scholar] [CrossRef]
- Kratochwil, C.; Fendler, W.P.; Eiber, M.; Hofman, M.S.; Emmett, L.; Calais, J.; Osborne, J.R.; Iravani, A.; Koo, P.; Lindenberg, L.; et al. Joint EANM/SNMMI procedure guideline for the use of 177Lu-labeled PSMA-targeted radioligand-therapy (177Lu-PSMARLT). Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 2830–2845. [Google Scholar]
- Fendler, W.P.; Rahbar, K.; Herrmann, K.; Kratochwil, C.; Eiber, M. 177Lu-PSMA radioligand therapy for prostate cancer. J. Nucl. Med. 2017, 58, 1196–1200. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kim, Y. Therapeutic responses and survival effects of 177Lu-PSMA-617 radioligand therapy in metastatic castrate-resistant prostate cancer: A meta-analysis. Clin. Nucl. Med. 2018, 43, 728–734. [Google Scholar] [CrossRef]
- Heck, M.M.; Tauber, R.; Schwaiger, S.; Retz, M.; D’Alessandria, C.; Maurer, T.; Gafita, A.; Wester, H.-J.; Gschwend, J.E.; Weber, W.A.; et al. Treatment Outcome, Toxicity, and Predictive Factors for Radioligand Therapy with (177)Lu-PSMA-I&T in Metastatic Castrationresistant Prostate Cancer. Eur. Urol. 2019, 75, 920–926. [Google Scholar]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [177Lu] Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Jackson, P.; Hofman, M.; McIntosh, L.; Buteau, J.P.; Kumar, A.R. Radiation dosimetry in 177Lu-PSMA-617 therapy. Semin. Nucl. Med. 2022, 52, 243–254. [Google Scholar] [CrossRef]
- Violet, J.; Jackson, P.; Ferdinandus, J.; Sandhu, S.; Akhurst, T.; Iravani, A.; Kong, G.; Kumar, A.R.; Thang, S.P.; Eu, P.; et al. Dosimetry of 177Lu-PSMA-617 in metastatic castration-resistant prostate cancer: Correlations between pretherapeutic imaging and whole-body tumor dosimetry with treatment outcomes. J. Nucl. Med. 2019, 60, 517–523. [Google Scholar] [CrossRef]
- Ngoc, C.N.; Happel, C.; Davis, K.; Groener, D.; Mader, N.; Mandel, P.; Tselis, N.; Gruenwald, F.; Sabet, A. Renal Function after Radioligand Treatment with 177Lu-PSMA-617. J. Nucl. Med. 2020, 61, 1279. [Google Scholar]
- Sadaghiani, M.S.; Sheikhbahaei, S.; Werner, R.A.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A.; Solnes, L.B.; Rowe, S.P. 177Lu-PSMA radioligand therapy effectiveness in metastatic castration-resistant prostate cancer: An updated systematic review and meta-analysis. Prostate 2022, 82, 826–835. [Google Scholar] [CrossRef]
- Levey, A.S. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Lythgoe, M.F.; Gordon, I.; Khader, Z.; Smith, T.; Anderson, P.J. Assessment of various parameters in the estimation of differential renal function using technetium-99m mercaptoacetyltriglycine. Eur. J. Nucl. Med. 1999, 26, 155–162. [Google Scholar] [CrossRef]
- Blaufox, M.D.; De Palma, D.; Taylor, A.; Szabo, Z.; Prigent, A.; Samal, M.; Li, Y.; Santos, A.; Testanera, G.; Tulchinsky, M. The SNMMI and EANM practice guideline for renal scintigraphy in adults. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2218–2228. [Google Scholar] [CrossRef]
- Taylor, A.T.; Brandon, D.C.; de Palma, D.; Blaufox, M.D.; Durand, E.; Erbas, B.; Grant, S.F.; Hilson, A.J.W.; Morsing, A. SNMMI Procedure Standard/EANM Practice Guideline for Diuretic Renal Scintigraphy in Adults with Suspected Upper Urinary Tract Obstruction 1.0. Semin. Nucl. Med. 2018, 48, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Sachpekidis, C.; Schepers, R.; Marti, M.; Kopp-Schneider, A.; Alberts, I.; Keramida, G.; Afshar-Oromieh, A.; Rominger, A. 99mTc-MAG3 Diuretic Renography: Intra- and InterObserver Repeatability in the Assessment of Renal Function. Diagnostics 2020, 10, 709. [Google Scholar] [CrossRef] [PubMed]
- Rosar, F.; Kochems, N.; Bartholomä, M.; Maus, S.; Stemler, T.; Linxweiler, J.; Khreish, F.; Ezziddin, S. Renal safety of [177Lu] Lu-PSMA-617 radioligand therapy in patients with compromised baseline kidney function. Cancers 2021, 13, 3095. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, Y.; Kuratsukuri, K.; Landas, S.; Imaida, K.; Rovito, P.M.; Wang, C.Y.; Haas, G.P. Expression of prostate-specific membrane antigen in normal and malignant human tissues. World J. Surg. 2006, 30, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Momin, M.A.; Abdullah, M.N.A.; Reza, M.S. Comparison of relative renal functions calculated with 99mTc-DTPA and 99mTc-DMSA for kidney patients of wide age ranges. Phys. Med. 2018, 45, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Schierz, J.H.; Sarikaya, I.; Albatineh, A.N.; Sarikaya, A. Assessing the correlation between (68)Ga-PSMA-11 renal PET parameters and renal function tests. J. Nucl. Med. Technol. 2021, 50, 43–48. [Google Scholar] [CrossRef]
- Rassek, P.; Schäfers, M.; Rahbar, K.; Backhaus, P. [18F]-PSMA-1007-PET for evaluation of kidney function. Nuklearmedizin-Nucl. Med. 2023, 62, 244–251. [Google Scholar] [CrossRef]
- Rosar, F.; Pauly, P.; Ries, M.; Schaefer-Schuler, A.; Maus, S.; Schreckenberger, M.; Khreish, F.; Ezziddin, S. Determination of split renal function by PSMA imaging: Comparison of 68Ga-PSMA-11 PET with 99mTc-MAG3 scintigraphy. Am. J. Nucl. Med. Mol. Imaging 2020, 10, 249. [Google Scholar]
- Esteves, F.P.; Halkar, R.K.; Issa, M.M.; Grant, S.; Taylor, A. Comparison of camera-based 99mTc-MAG3 and 24-hour creatinine clearances for evaluation of kidney function. Am. J. Roentgenol. 2006, 187, W316–W319. [Google Scholar] [CrossRef]
- Valind, K.; Minarik, D.; Garpered, S.; Persson, E.; Jögi, J.; Trägårdh, E. [18F] PSMA-1007 PET is comparable to [99mTc] Tc-DMSA SPECT for renal cortical imaging. Eur. J. Hybrid Imaging 2023, 7, 25. [Google Scholar] [CrossRef]
- Sarikaya, I.; Alqallaf, A.; Sarikaya, A. Renal cortical 68Ga-PSMA-11 PET and 99mTcDMSA images. J. Nucl. Med. Technol. 2021, 49, 30–33. [Google Scholar] [CrossRef]
- Valind, K.; Jögi, J.; Minarik, D.; Trägårdh, E. [18F] PSMA-1007 renal uptake parameters: Reproducibility and relationship to estimated glomerular filtration rate. Clin. Physiol. Funct. Imaging 2023, 43, 128–135. [Google Scholar] [CrossRef]
- Betz, A.; Buchholz, H.G.; Rosar, F.; Miederer, M.; Schreckenberger, M. Renal Function Evaluation by 68-Ga-PSMA-PET/CT. J. Nucl. Med. 2021, 62, 1303. [Google Scholar]
- Valind, K.; Jögi, J.; Minarik, D.; Brolin, G.; Trägårdh, E. Dose-reduced [18F] PSMA-1007 PET is feasible for functional imaging of the renal cortex. EJNMMI Phys. 2021, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Ruth, T.J. The shortage of technetium-99m and possible solutions. Annu. Rev. Nucl. Part Sci. 2020, 70, 77–94. [Google Scholar] [CrossRef]
- Gafita, A.; Wang, H.; Robertson, A.; Armstrong, W.R.; Zaum, R.; Weber, M.; Yagubbayli, F.; Kratochwil, C.; Grogan, T.R.; Nguyen, K.; et al. Tumor sink effect in 68Ga-PSMA11 PET: Myth or reality? J. Nucl. Med. 2022, 63, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Burgard, C.; Rosar, F.; Marlowe, R.J.; Bartholomä, M.; Dewes, S.; Schaefer-Schuler, A.; Linxweiler, J.; Khreish, F.; Ezziddin, S. Tumor Sink Effect with Prostate-Specific Membrane Antigen-Targeted Theranostics in Patients with Metastatic Castration-Resistant Prostate Cancer: Intra-Individual Evaluations. Cancers 2023, 15, 2592. [Google Scholar] [CrossRef]










| Number of patients | 28 |
| Age | (Years) |
| Min | 45 |
| Max | 86 |
| Mean | 64 |
| Median | 67.5 |
| Metastases | (n) |
| Bone | 28 |
| Lymph nodes | 19 |
| Lung | 2 |
| Others | 1 |
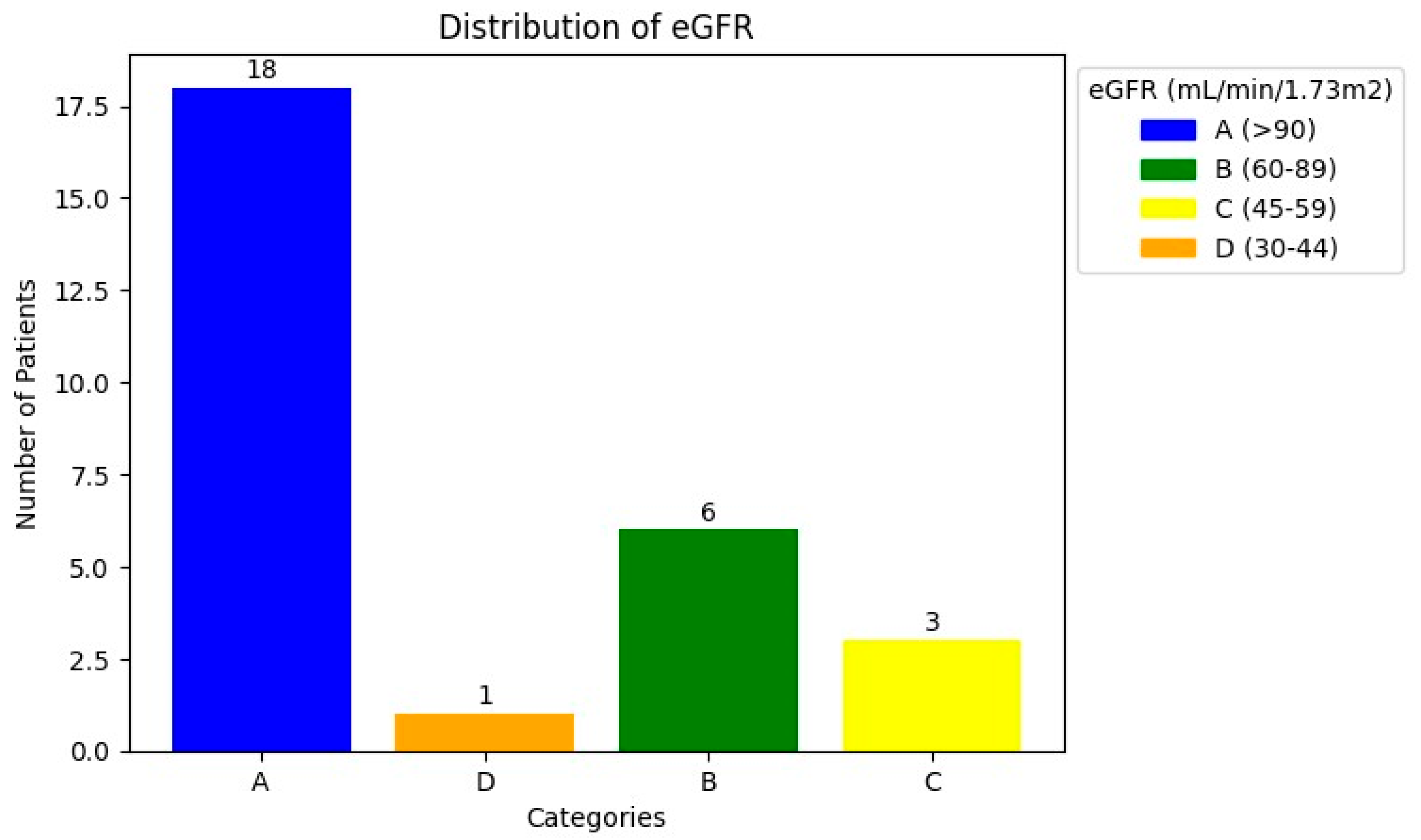
| eGFR | (mL/min) |
| <60 mL/min | n = 4 (CKD stage 3A n = 3; stage 3B n = 1) |
| ≥60 mL/min | n = 24 |
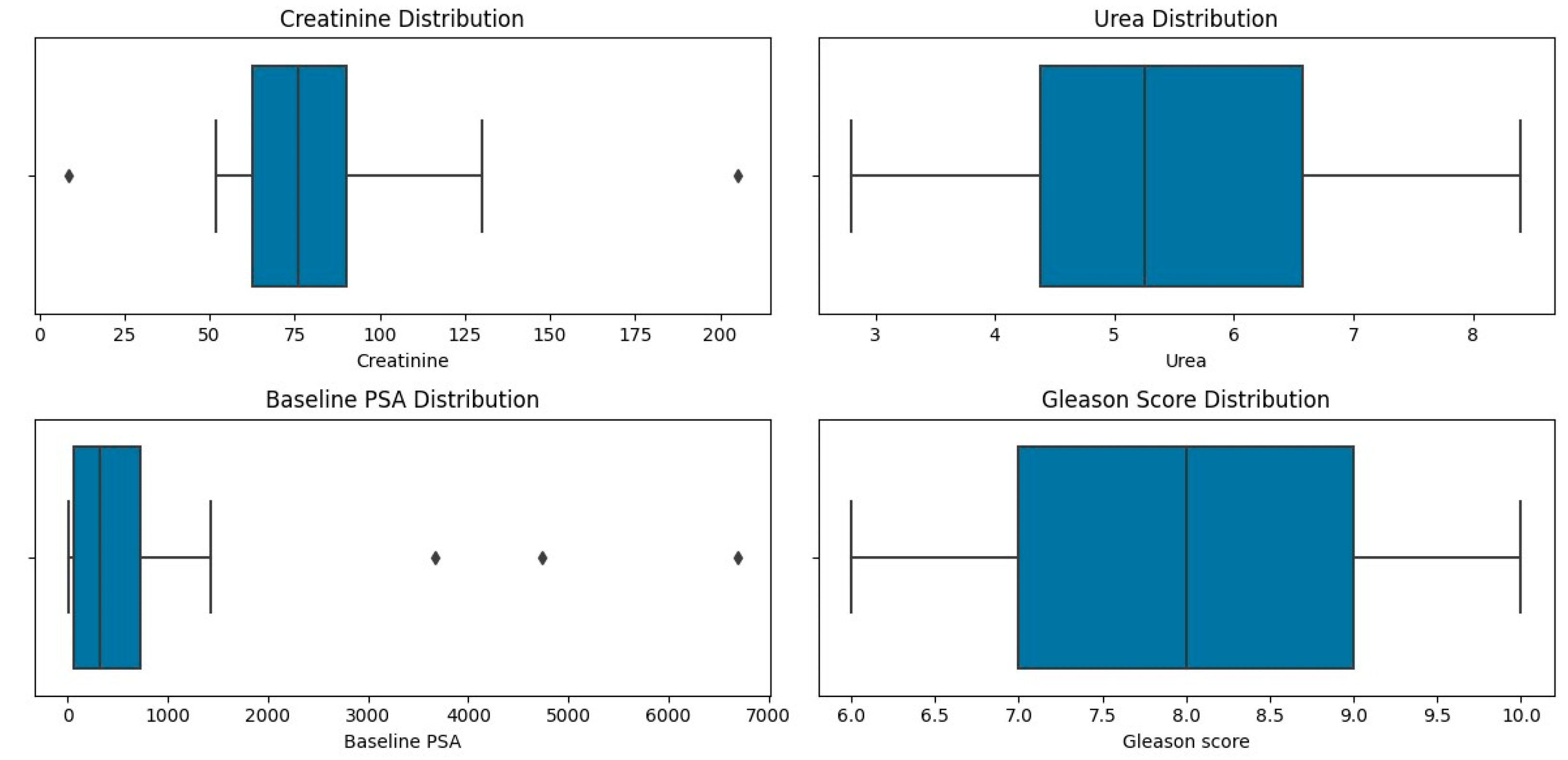
| Creatinine | µmol/L |
| Min | 52 |
| Max | 205 |
| Mean | 81 |
| Median | 76 |
| Urea | |
| Min | 2.8 |
| Max | 8.4 |
| Mean | 5.20 |
| Median | 5.25 |
| PSA | (ng/mL) |
| Min | 3.95 |
| Max | 6685 |
| Mean | 869.81 |
| Median | 359.07 |
| 68Ga-PSMA PET/CT (Right) | 99mTc- MAG3 (Right) | 68Ga-PSMA PET/CT (Left) | 99mTcMAG3 (Left) | |
|---|---|---|---|---|
| Mean | 45.8 | 47.0 | 54.2 | 53.7 |
| Median | 49.9 | 50.5 | 50 | 50 |
| Std | 17.8 | 18.4 | 17.8 | 18.4 |
| Min | 3 | 0.0 | 9 | 6 |
| 25% | 44.4 | 46 | 48.3 | 45.8 |
| 50% | 49.9 | 50.5 | 50.5 | 50 |
| 75% | 51.7 | 55 | 55.6 | 54.5 |
| Max | 91 | 94 | 97 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabela, L.; Mkhize, T.; Hadebe, B.; Harry, L.; Nxasana, T.; Ndlovu, N.; Pillay, V.; Masikane, S.; Patel, M.; Nyakale, N.E.; et al. A Comparison of 68Ga-PSMA PET/CT-Based Split Renal Function with 99mTc-MAG3 Renography in Patients with Metastatic Castration-Resistant Prostate Carcinoma Treated with 177Lu-PSMA. Diagnostics 2024, 14, 578. https://doi.org/10.3390/diagnostics14060578
Gabela L, Mkhize T, Hadebe B, Harry L, Nxasana T, Ndlovu N, Pillay V, Masikane S, Patel M, Nyakale NE, et al. A Comparison of 68Ga-PSMA PET/CT-Based Split Renal Function with 99mTc-MAG3 Renography in Patients with Metastatic Castration-Resistant Prostate Carcinoma Treated with 177Lu-PSMA. Diagnostics. 2024; 14(6):578. https://doi.org/10.3390/diagnostics14060578
Chicago/Turabian StyleGabela, Lerato, Thokozani Mkhize, Bawinile Hadebe, Lerwine Harry, Thembelihle Nxasana, Nontobeko Ndlovu, Venesen Pillay, Sphelele Masikane, Maryam Patel, Nozipho Elizabeth Nyakale, and et al. 2024. "A Comparison of 68Ga-PSMA PET/CT-Based Split Renal Function with 99mTc-MAG3 Renography in Patients with Metastatic Castration-Resistant Prostate Carcinoma Treated with 177Lu-PSMA" Diagnostics 14, no. 6: 578. https://doi.org/10.3390/diagnostics14060578
APA StyleGabela, L., Mkhize, T., Hadebe, B., Harry, L., Nxasana, T., Ndlovu, N., Pillay, V., Masikane, S., Patel, M., Nyakale, N. E., & Vorster, M. (2024). A Comparison of 68Ga-PSMA PET/CT-Based Split Renal Function with 99mTc-MAG3 Renography in Patients with Metastatic Castration-Resistant Prostate Carcinoma Treated with 177Lu-PSMA. Diagnostics, 14(6), 578. https://doi.org/10.3390/diagnostics14060578