
The Impact of Magnetic Resonance Imaging Findings in Predicting Neurological Status Pre- and Post-Treatment of Spinal Dural Arteriovenous Fistulas: A 22-Year Experience in a Neurovascular and Spine Center

Abstract
:1. Introduction
2. Materials and Methods
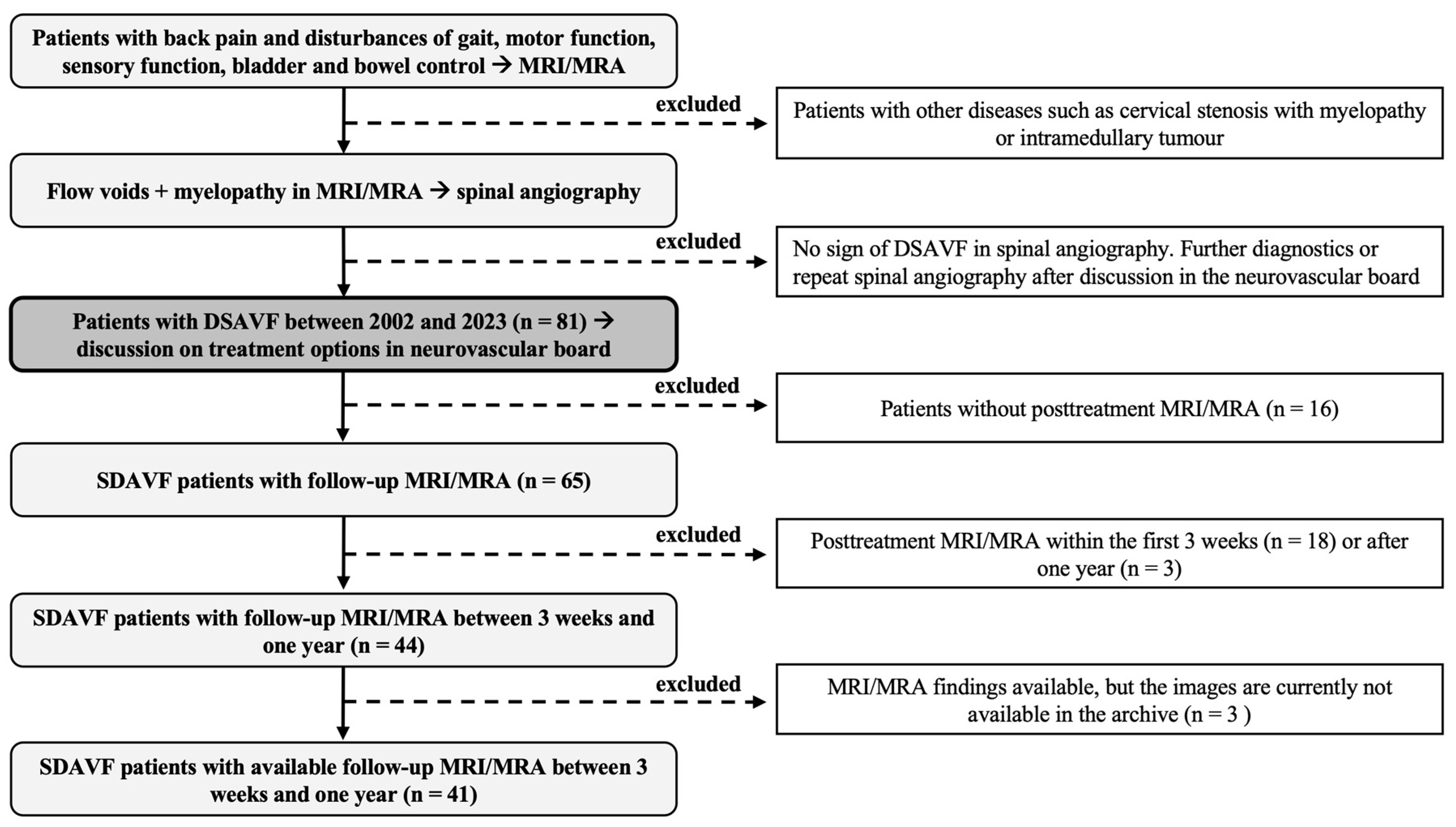
2.1. Study Design and Patient Data
2.1.1. Study Design
2.1.2. Patient Data and Institutional Review Board
2.2. Clinical Management
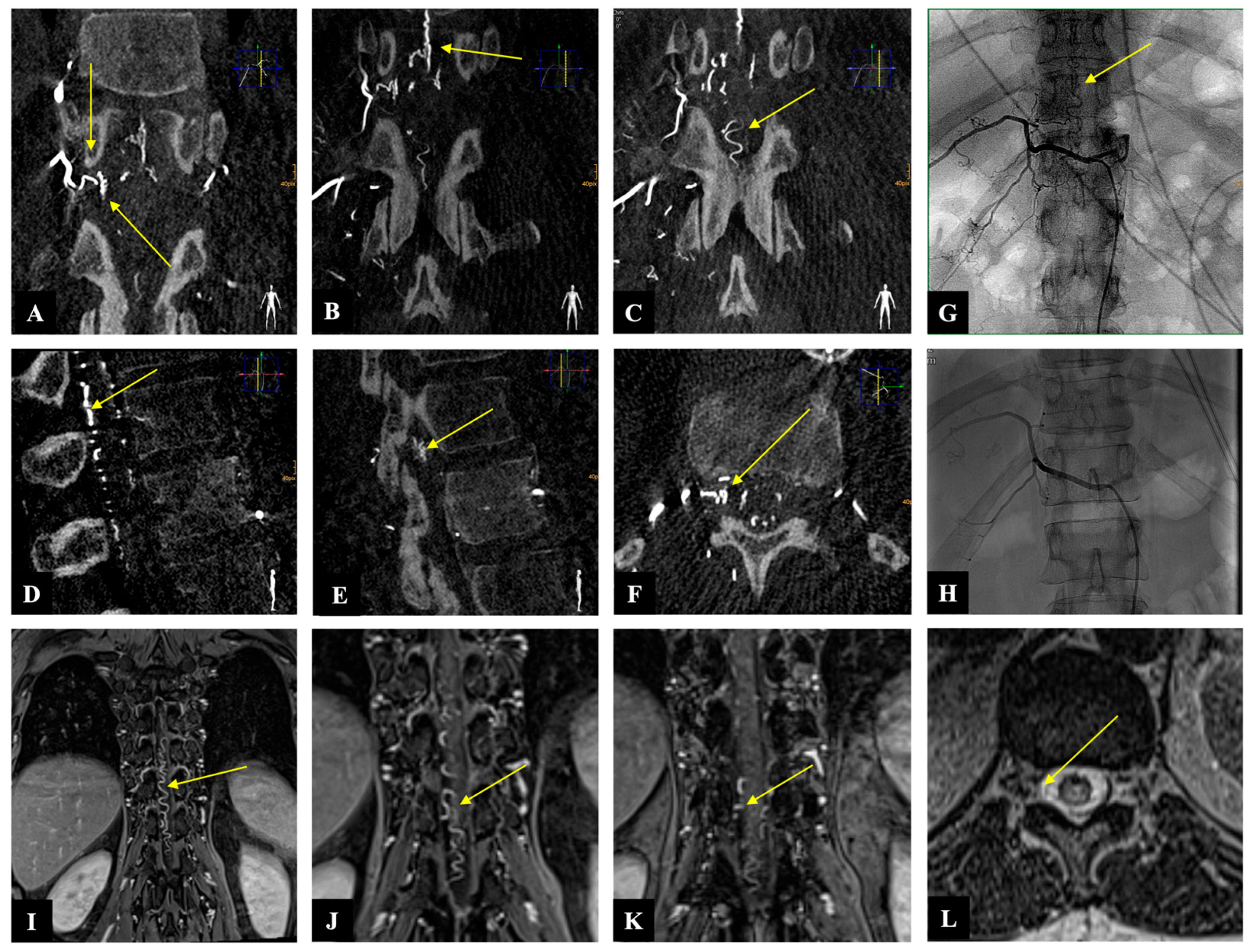
2.3. Illustrative Case
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Myelopathy and Flow Voids
3.3. Improvement in mALS and ASIA-MS
4. Discussion
Limitations and Strengths of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aminoff, M.J.; Logue, V. Clinical features of spinal vascular malformations. Brain 1974, 97, 197–210. [Google Scholar] [CrossRef]
- Aminoff, M.J.; Barnard, R.O.; Logue, V. The pathophysiology of spinal vascular malformations. J. Neurol. Sci. 1974, 23, 255–263. [Google Scholar] [CrossRef]
- Hurst, R.W.; Kenyon, L.C.; Lavi, E.; Raps, E.C.; Marcotte, P. Spinal dural arteriovenous fistula: The pathology of venous hypertensive myelopathy. Neurology 1995, 45, 1309–1313. [Google Scholar] [CrossRef]
- Narvid, J.; Hetts, S.W.; Larsen, D.; Neuhaus, J.; Singh, T.P.; McSwain, H.; Lawton, M.T.; Dowd, C.F.; Higashida, R.T.; Halbach, V.V. Spinal dural arteriovenous fistulae: Clinical features and long-term results. Neurosurgery 2008, 62, 159–166; discussion 166–167. [Google Scholar] [CrossRef]
- Muralidharan, R.; Saladino, A.; Lanzino, G.; Atkinson, J.L.; Rabinstein, A.A. The clinical and radiological presentation of spinal dural arteriovenous fistula. Spine 2011, 36, E1641–E1647. [Google Scholar] [CrossRef]
- Muralidharan, R.; Mandrekar, J.; Lanzino, G.; Atkinson, J.L.; Rabinstein, A.A. Prognostic value of clinical and radiological signs in the postoperative outcome of spinal dural arteriovenous fistula. Spine 2013, 38, 1188–1193. [Google Scholar] [CrossRef]
- Klopper, H.B.; Surdell, D.L.; Thorell, W.E. Type I spinal dural arteriovenous fistulas: Historical review and illustrative case. Neurosurg. Focus 2009, 26, E3. [Google Scholar] [CrossRef] [PubMed]
- Jellema, K.; Tijssen, C.C.; van Gijn, J. Spinal dural arteriovenous fistulas: A congestive myelopathy that initially mimics a peripheral nerve disorder. Brain 2006, 129, 3150–3164. [Google Scholar] [CrossRef]
- Shin, D.A.; Park, K.Y.; Ji, G.Y.; Yi, S.; Ha, Y.; Park, S.W.; Yoon, D.H.; Kim, K.N. The use of magnetic resonance imaging in predicting the clinical outcome of spinal arteriovenous fistula. Yonsei Med. J. 2015, 56, 397–402. [Google Scholar] [CrossRef]
- Marcus, J.; Schwarz, J.; Singh, I.P.; Sigounas, D.; Knopman, J.; Gobin, Y.P.; Patsalides, A. Spinal dural arteriovenous fistulas: A review. Curr. Atheroscler. Rep. 2013, 15, 335. [Google Scholar] [CrossRef]
- Bretonnier, M.; Henaux, P.L.; Gaberel, T.; Roualdes, V.; Kerdiles, G.; Le Reste, P.J.; Morandi, X. Spinal Dural Arteriovenous Fistulas: Clinical Outcome After Surgery Versus Embolization: A Retrospective Study. World Neurosurg. 2019, 127, e943–e949. [Google Scholar] [CrossRef]
- Cesak, T.; Adamkov, J.; Poczos, P.; Kanta, M.; Krajina, A.; Krajickova, D.; Herzig, R.; Valis, M. Multidisciplinary approach in the treatment of spinal dural arteriovenous fistula-results of endovascular and surgical treatment. Acta Neurochir. 2018, 160, 2439–2448. [Google Scholar] [CrossRef]
- Bakker, N.A.; Uyttenboogaart, M.; Luijckx, G.J.; Eshghi, O.S.; Mazuri, A.; Metzemaekers, J.D.; Groen, R.J.; Van Dijk, J.M. Recurrence Rates After Surgical or Endovascular Treatment of Spinal Dural Arteriovenous Fistulas: A Meta-analysis. Neurosurgery 2015, 77, 137–144; discussion 144. [Google Scholar] [CrossRef]
- Willinsky, R.; TerBrugge, K.; Lasjaunias, P.; Montanera, W. The variable presentations of craniocervical and cervical dural arteriovenous malformations. Surg. Neurol. 1990, 34, 118–123. [Google Scholar] [CrossRef]
- Brinjikji, W.; Colombo, E.; Cloft, H.J.; Lanzino, G. Clinical and Imaging Characteristics of Spinal Dural Arteriovenous Fistulas and Spinal Epidural Arteriovenous Fistulas. Neurosurgery 2021, 88, 666–673. [Google Scholar] [CrossRef]
- Oh, Y.; Heo, Y.; Jeon, S.R.; Roh, S.W.; Park, J.H. Microsurgery Versus Endovascular Treatment—Which Is Adequate for Initial Treatment of Spinal Dural Arteriovenous Fistula: A Case Series. Neurospine 2021, 18, 344–354. [Google Scholar] [CrossRef]
- Acerbi, F.; Ferroli, P. Surgery versus embolization in spinal dural arteriovenous fistulas: The ideal competition to improve the care of patients. World Neurosurg. 2013, 80, e191–e193. [Google Scholar] [CrossRef]
- Kirsch, M.; Berg-Dammer, E.; Musahl, C.; Bazner, H.; Kuhne, D.; Henkes, H. Endovascular management of spinal dural arteriovenous fistulas in 78 patients. Neuroradiology 2013, 55, 337–343. [Google Scholar] [CrossRef]
- Krings, T.; Geibprasert, S. Spinal dural arteriovenous fistulas. AJNR Am. J. Neuroradiol. 2009, 30, 639–648. [Google Scholar] [CrossRef]
- Tacconi, L.; Lopez Izquierdo, B.C.; Symon, L. Outcome and prognostic factors in the surgical treatment of spinal dural arteriovenous fistulas. A long-term study. Br. J. Neurosurg. 1997, 11, 298–305. [Google Scholar] [CrossRef]
- Ushikoshi, S.; Hida, K.; Kikuchi, Y.; Miyasaka, K.; Iwasaki, T.; Abe, H. Functional prognosis after treatment of spinal dural arteriovenous fistulas. Neurol. Med. Chir. 1999, 39, 206–212; discussion 212–213. [Google Scholar] [CrossRef]
- Shinoyama, M.; Endo, T.; Takahash, T.; Shimizu, H.; Takahashi, A.; Suzuki, M.; Tominaga, T. Long-term outcome of cervical and thoracolumbar dural arteriovenous fistulas with emphasis on sensory disturbance and neuropathic pain. World Neurosurg. 2010, 73, 401–408. [Google Scholar] [CrossRef]
- Safaee, M.M.; Clark, A.J.; Burkhardt, J.K.; Winkler, E.A.; Lawton, M.T. Timing, severity of deficits, and clinical improvement after surgery for spinal dural arteriovenous fistulas. J. Neurosurg. Spine 2018, 29, 85–91. [Google Scholar] [CrossRef]
- Ronald, A.A.; Yao, B.; Winkelman, R.D.; Piraino, D.; Masaryk, T.J.; Krishnaney, A.A. Spinal Dural Arteriovenous Fistula: Diagnosis, Outcomes, and Prognostic Factors. World Neurosurg. 2020, 144, e306–e315. [Google Scholar] [CrossRef]
- Niimi, Y.; Berenstein, A.; Setton, A.; Neophytides, A. Embolization of spinal dural arteriovenous fistulae: Results and follow-up. Neurosurgery 1997, 40, 675–682; discussion 682–683. [Google Scholar] [CrossRef]
- Luo, M.; Li, J.; Wu, C.; He, M. Prognostic value of magnetic resonance imaging in spinal dural arteriovenous fistulas. Acta Neurochir. 2022, 164, 49–54. [Google Scholar] [CrossRef]
- Hetts, S.W.; Moftakhar, P.; English, J.D.; Dowd, C.F.; Higashida, R.T.; Lawton, M.T.; Douglas, V.C.; Halbach, V.V. Spinal dural arteriovenous fistulas and intrathecal venous drainage: Correlation between digital subtraction angiography, magnetic resonance imaging, and clinical findings. J. Neurosurg. Spine 2012, 16, 433–440. [Google Scholar] [CrossRef]
- Lee, J.; Lim, Y.M.; Suh, D.C.; Rhim, S.C.; Kim, S.J.; Kim, K.K. Clinical presentation, imaging findings, and prognosis of spinal dural arteriovenous fistula. J. Clin. Neurosci. 2016, 26, 105–109. [Google Scholar] [CrossRef]
- Fugate, J.E.; Lanzino, G.; Rabinstein, A.A. Clinical presentation and prognostic factors of spinal dural arteriovenous fistulas: An overview. Neurosurg. Focus 2012, 32, E17. [Google Scholar] [CrossRef]
- Kaufmann, T.J.; Morris, J.M.; Saladino, A.; Mandrekar, J.N.; Lanzino, G. Magnetic resonance imaging findings in treated spinal dural arteriovenous fistulas: Lack of correlation with clinical outcomes. J. Neurosurg. Spine 2011, 14, 548–554. [Google Scholar] [CrossRef]
- Van Dijk, J.M.; TerBrugge, K.G.; Willinsky, R.A.; Farb, R.I.; Wallace, M.C. Multidisciplinary management of spinal dural arteriovenous fistulas: Clinical presentation and long-term follow-up in 49 patients. Stroke 2002, 33, 1578–1583. [Google Scholar] [CrossRef] [PubMed]
- Patsalides, A.; Knopman, J.; Santillan, A.; Tsiouris, A.J.; Riina, H.; Gobin, Y.P. Endovascular treatment of spinal arteriovenous lesions: Beyond the dural fistula. AJNR Am. J. Neuroradiol. 2011, 32, 798–808. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Age, median [IQR] | 65.9 [54.5–73.5] y |
| Female gender, n (%) | 11 (26.8%) |
| Time from symptom to MRI diagnosis, median [IQR] | 7 [2.5–24] m |
| Time from MRI diagnosis to treatment, median [IQR] | 15 [9–34.5] d |
| Myelopathy extension at admission on MRI, median [IQR] | 7 [6–8] v |
| Absence of myelopathy on FU MRI, n (%) | 29 (70.7%) |
| Flow void extension at admission on MRI, median [IQR] | 7 [4.5–10] v |
| Absence of flow voids on FU MRI, n (%) | 41 (100%) |
| mALS at admission, median [IQR] | 4 [2–7] |
| mALS at third FU, median [IQR] | 2 [0–4.5] |
| ASIA-MS at admission, median [IQR] | 97 [88–100] |
| ASIA-MS at third FU, median [IQR] | 100 [95–100] |
| Interval between treatment and FU MRI, median [IQR] | 4.6 [2.9–6.5] m |
| Fistulous point: | |
| Cervical, n (%) | 3 (7.3%) |
| Upper thoracic, n (%) | 7 (17.1%) |
| Lower thoracic, n (%) | 17 (41.5%) |
| Lumbar, n (%) | 12 (29.2%) |
| Sacral, n (%) | 2 (4.9%) |
| Side of fistula, n | R: 22, L: 18, B: 1 |
| Incomplete or failed occlusion, n (%) | 2 (4.9%) |
| Treatment- or hospital-related complications, n (%) | 6 (14.6%) |
| Improvement in mALS between admission and last FU, n (%) | 27 (65.9%) |
| Improvement in ASIA-MS between admission and last FU, n (%) | 32 (78%) |
| Diagnostic sensitivity of MRA to locate the fistula, n (%) | 28 (68.3%) |
| Surgery vs. embolization, n (%) | 36 (87.8%) vs. 5 (12.2%) |
| BMI | 27.5 [24.9–30.3] kg/m2 |
| Associated Variable | Simple Linear Regression | |||||
|---|---|---|---|---|---|---|
| B | (95% CI) | SE | β | R2 | p | |
| Extent of pre. myelopathy Pre. ASIA-MS | −0.109 | −0.185, −0.033 | 0.037 | −0.423 | 0.179 | 0.006 |
| Third FU ASIA-MS | −0.058 | −0.187, 0.071 | 0.062 | −0.212 | 0.045 | 0.357 |
| Improved ASIA-MS | 0.410 | −2.072, 2.892 | 1.227 | 0.053 | 0.003 | 0.740 |
| Pre. mALS | 0.319 | −0.002, 0.641 | 0.159 | 0.306 | 0.094 | 0.052 |
| Third FU mALS | 0.331 | −0.172, 0.834 | 0.240 | 0.302 | 0.091 | 0.184 |
| Improved mALS | −0.503 | −2.666, 1.661 | 1.070 | −0.075 | 0.006 | 0.641 |
| Extent of pre. Flow voids Pre. ASIA-MS | −0.075 | −0.168, 0.018 | 0.046 | −0.251 | 0.063 | 0.113 |
| Third FU ASIA-MS | −0.003 | −0.140, 0.134 | 0.065 | −0.012 | 0.000 | 0.960 |
| Improved ASIA-MS | −0.375 | −3.229, 2.479 | 1.411 | −0.430 | 0.002 | 0.792 |
| Pre. mALS | 0.195 | −0.189, 0.578 | 0.189 | 0.162 | 0.026 | 0.311 |
| Third FU mALS | 0.117 | −0.429, 0.662 | 0.261 | 0.102 | 0.010 | 0.660 |
| Improved mALS | −0.011 | −2.504, 2.483 | 1.233 | −0.001 | 0.000 | 0.993 |
| Associated Variable | Binary Logistic Regression | |
|---|---|---|
| OR (95% CI) | p Value | |
| Absence of myelopathy on FU MRI | ||
| Improved mALS in the last FU | 0.630 (0.157–2.533) | 0.515 |
| Improved ASIA-MS in the last FU | 4.190 (0.463–37.938) | 0.202 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filis, A.; Engellandt, K.; Romualdo, S.M.F.; El-Battrawy, I.; Podlesek, D.; Juratli, T.A.; Eyüpoglu, I.Y.; Hijazi, M.M. The Impact of Magnetic Resonance Imaging Findings in Predicting Neurological Status Pre- and Post-Treatment of Spinal Dural Arteriovenous Fistulas: A 22-Year Experience in a Neurovascular and Spine Center. Diagnostics 2024, 14, 581. https://doi.org/10.3390/diagnostics14060581
Filis A, Engellandt K, Romualdo SMF, El-Battrawy I, Podlesek D, Juratli TA, Eyüpoglu IY, Hijazi MM. The Impact of Magnetic Resonance Imaging Findings in Predicting Neurological Status Pre- and Post-Treatment of Spinal Dural Arteriovenous Fistulas: A 22-Year Experience in a Neurovascular and Spine Center. Diagnostics. 2024; 14(6):581. https://doi.org/10.3390/diagnostics14060581
Chicago/Turabian StyleFilis, Andreas, Kay Engellandt, Sergio M. F. Romualdo, Ibrahim El-Battrawy, Dino Podlesek, Tareq A. Juratli, Ilker Y. Eyüpoglu, and Mido Max Hijazi. 2024. "The Impact of Magnetic Resonance Imaging Findings in Predicting Neurological Status Pre- and Post-Treatment of Spinal Dural Arteriovenous Fistulas: A 22-Year Experience in a Neurovascular and Spine Center" Diagnostics 14, no. 6: 581. https://doi.org/10.3390/diagnostics14060581