
Relationship of Maxillary Sinus Volume and Nasal Septum Deviation: A Cone Beam Computed Tomography Study

 ,
,  ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Population
2.2. CBCT Image Analysis
2.3. Image Analysis
- V = 4/3 r3. It was called the mMSV “sphere”.
- V = 1/3 A × h. It was called the mMSV “pyramid”.

2.4. Statistical Analysis
3. Results
3.1. Maxillary Sinus Volume Analysis
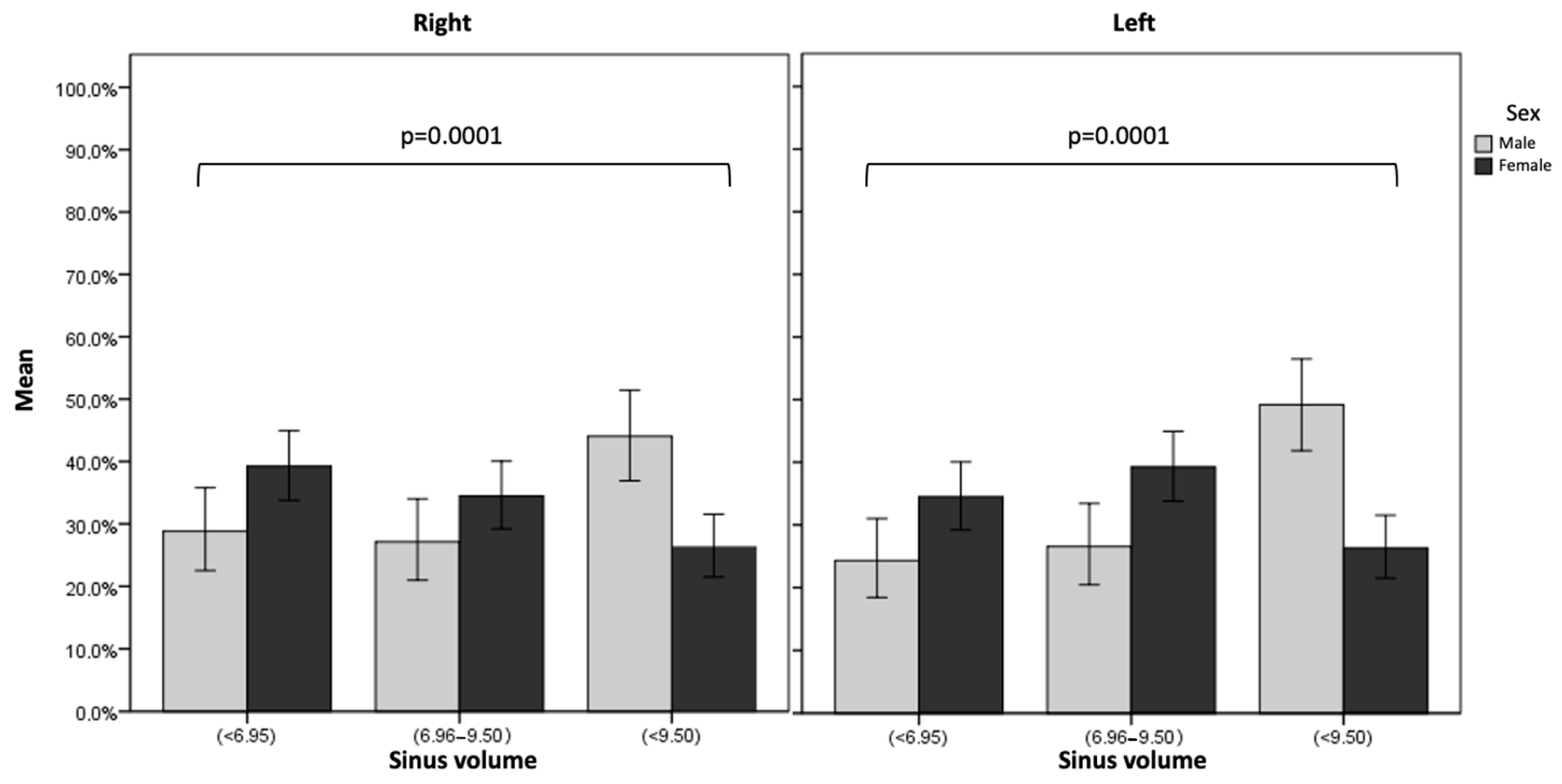
3.2. Relationship between Sex and Left and Right Maxillary Sinus Volume
3.3. Nasal Septum Deviation Analysis
3.4. Maxillary Sinus Volume and Degrees of Septal Deviation Analysis
3.5. Additional Tomographic Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kapusuz Gencer, Z.; Özkırış, M.; Okur, A.; Karaçavuş, S.; Saydam, L. The effect of nasal septal deviation on maxillary sinus volumes and development of maxillary sinusitis. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 3069–3073. [Google Scholar] [CrossRef]
- Kawarai, Y.; Fukushima, K.; Ogawa, T.; Nishizaki, K.; Gunduz, M.; Fujimoto, M.; Masuda, Y. Volume quantification of healthy paranasal cavity by three-dimensional CT imaging. Acta Oto-Laryngol. 1999, 119, 45–49. [Google Scholar]
- Kucybała, I.; Janik, K.A.; Ciuk, S.; Storman, D.; Urbanik, A. Nasal septal deviation and concha bullosa–do they have an impact on maxillary sinus volumes and prevalence of maxillary sinusitis? Pol. J. Radiol. 2017, 82, 126–133. [Google Scholar] [CrossRef]
- Lawson, W.; Patel, Z.M.; Lin, F.Y. The development and pathologic processes that influence maxillary sinus pneumatization. Anat. Rec. Adv. Integr. Anat. Evol. Biol. Adv. Integr. Anat. Evol. Biol. 2008, 291, 1554–1563. [Google Scholar] [CrossRef]
- Przystańska, A.; Kulczyk, T.; Rewekant, A.; Sroka, A.; Jończyk-Potoczna, K.; Lorkiewicz-Muszyńska, D.; Gawriołek, K.; Czajka-Jakubowska, A. Introducing a simple method of maxillary sinus volume assessment based on linear dimensions. Ann. Anat. Anat. Anz. 2018, 215, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Sapmaz, E.; Kavaklı, A.; Sapmaz, H.I.; Ögetürk, M. Impact of hard palate angulation caused by septal deviation on maxillary sinus volume. Turk. Arch. Otorhinolaryngol. 2018, 56, 75. [Google Scholar] [CrossRef] [PubMed]
- Wolf, G.; Anderhuber, W.; Kuhn, F. Development of the paranasal sinuses in children: Implications for paranasal sinus surgery. Ann. Otol. Rhinol. Laryngol. 1993, 102, 705–711. [Google Scholar] [CrossRef]
- Oz, A.Z.; Oz, A.A.; El, H.; Palomo, J.M. Maxillary sinus volume in patients with impacted canines. Angle Orthod. 2017, 87, 25–32. [Google Scholar] [CrossRef]
- Tassoker, M.; Magat, G.; Lale, B.; Gulec, M.; Ozcan, S.; Orhan, K. Is the maxillary sinus volume affected by concha bullosa, nasal septal deviation, and impacted teeth? A CBCT study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 227–233. [Google Scholar] [CrossRef]
- Bingham, B.; Wang, R.G.; Hawke, M.; Kwok, P. The embryonic development of the lateral nasal wall from 8 to 24 weeks. Laryngoscope 1991, 101, 992–997. [Google Scholar] [CrossRef]
- Collet, S.; Bertrand, B.; Cornu, S.; Eloy, P.; Rombaux, P. Is septal deviation a risk factor for chronic sinusitis? Review of literature. Acta Oto-Rhino-Laryngol. Belg. 2001, 55, 299–304. [Google Scholar]
- Orlandi, R.R. A systematic analysis of septal deviation associated with rhinosinusitis. Laryngoscope 2010, 120, 1687–1695. [Google Scholar] [CrossRef] [PubMed]
- Al-Rawi, N.H.; Uthman, A.T.; Abdulhameed, E.; Al Nuaimi, A.S.; Seraj, Z. Concha bullosa, nasal septal deviation, and their impacts on maxillary sinus volume among Emirati people: A cone-beam computed tomography study. Imaging Sci. Dent. 2019, 49, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Akay, G.; Yaman, D.; Karadağ, Ö.; Güngör, K. Evaluation of the Relationship of Dimensions of Maxillary Sinus Drainage System with Anatomical Variations and Sinusopathy: Cone-Beam Computed Tomography Findings. Med. Princ. Pr. 2020, 29, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Aktuna Belgin, C.; Colak, M.; Adiguzel, O.; Akkus, Z.; Orhan, K. Three-dimensional evaluation of maxillary sinus volume in different age and sex groups using CBCT. Eur. Arch. Otorhinolaryngol. 2019, 276, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Kalabalık, F.; Tarım Ertaş, E. Investigation of maxillary sinus volume relationships with nasal septal deviation, concha bullosa, and impacted or missing teeth using cone-beam computed tomography. Oral Radiol. 2019, 35, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Mladina, R.; Cujić, E.; Subarić, M.; Vuković, K. Nasal septal deformities in ear, nose, and throat patients: An international study. Am. J. Otolaryngol. 2008, 29, 75–82. [Google Scholar] [CrossRef]
- Orhan, I.; Ormeci, T.; Aydin, S.; Altin, G.; Urger, E.; Soylu, E.; Yilmaz, F. Morphometric analysis of the maxillary sinus in patients with nasal septum deviation. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 727–732. [Google Scholar] [CrossRef]
- Biafora, M.; Bertazzoni, G.; Trimarchi, M. Maxillary sinusitis caused by dental implants extending into the maxillary sinus and the nasal cavities. J. Prosthodont. 2014, 23, 227–231. [Google Scholar] [CrossRef]
- Kim, S.J.; Park, J.S.; Kim, H.T.; Lee, C.H.; Park, Y.H.; Bae, J.H. Clinical features and treatment outcomes of dental implant-related paranasal sinusitis: A 2-year prospective observational study. Clin. Oral Implant. Res. 2016, 27, e100–e104. [Google Scholar] [CrossRef]
- Testori, T.; Weinstein, T.; Taschieri, S.; Wallace, S.S. Risk factors in lateral window sinus elevation surgery. Periodontology 2000 2019, 81, 91–123. [Google Scholar] [CrossRef]
- Van den Bergh, J.P.; ten Bruggenkate, C.M.; Disch, F.J.; Tuinzing, D.B. Anatomical aspects of sinus floor elevations. Clin. Oral Implant. Res. 2000, 11, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Gies, M.; Kalender, W.A.; Wolf, H.; Suess, C.; Madsen, M.T. Dose reduction in CT by anatomically adapted tube current modulation. I. Simulation studies. Med. Phys. 1999, 26, 2235–2247. [Google Scholar] [CrossRef] [PubMed]
- Möhlhenrich, S.C.; Heussen, N.; Peters, F.; Steiner, T.; Hölzle, F.; Modabber, A. Is the maxillary sinus really suitable in sex determination? A three-dimensional analysis of maxillary sinus volume and surface depending on sex and dentition. J. Craniofacial Surg. 2015, 26, e723–e726. [Google Scholar] [CrossRef] [PubMed]
- Ulm, C.; Solar, P.; Gselimann, B.; Matejka, M.; Watzek, G. The edentulous maxillary alveolar process in the region of the maxillary sinus—A study of physical dimension. Int. J. Oral Maxillofac. Surg. 1995, 24, 279–282. [Google Scholar] [CrossRef]
- Mygind, N.; Dahl, R. Anatomy, physiology and function of the nasal cavities in health and disease. Adv. Drug Deliv. Rev. 1998, 29, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, A.-M.; Chrysikos, D.; Samolis, A.; Tsakotos, G.; Troupis, T. Anatomical variations of the nasal cavities and paranasal sinuses: A systematic review. Cureus 2021, 13, e12727. [Google Scholar] [CrossRef] [PubMed]
- Neeley, W.W., II; Edgin, W.A.; Gonzales, D.A. A review of the effects of expansion of the nasal base on nasal airflow and resistance. J. Oral Maxillofac. Surg. 2007, 65, 1174–1179. [Google Scholar] [CrossRef]
- Alhazmi, A. Association between maxillary sinus dimensions and midface width: 2-D and 3-D volumetric cone-beam computed tomography cross-sectional study. J. Contemp. Dent. Pr. 2020, 21, 317–321. [Google Scholar] [CrossRef]
- Song, S.Y.; Hong, J.W.; Roh, T.S.; Kim, Y.O.; Kim, D.W.; Park, B.Y. Volume and distances of the maxillary sinus in craniofacial deformities with midfacial hypoplasia. Otolaryngol. -Head. Neck Surg. 2009, 141, 614–620. [Google Scholar] [CrossRef]
- Shetty, S.R.; Al Bayatti, S.W.; Al-Rawi, N.H.; Marei, H.; Reddy, S.; Abdelmagyd, H.A.; Narasimhan, S.; Al Kawas, S.; Mathew, A. Analysis of inferior nasal turbinate width and concha bullosa in subjects with nasal septum deviation: A cone beam tomography study. BMC Oral Health 2021, 21, 206. [Google Scholar] [CrossRef] [PubMed]
- Park, W.B.; Kim, Y.J.; Kang, K.L.; Lim, H.C.; Han, J.Y. Long-term outcomes of the implants accidentally protruding into nasal cavity extended to posterior maxilla due to inferior meatus pneumatization. Clin. Implant. Dent. Relat. Res. 2020, 22, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Ilie, A.C.; Jianu, A.M.; Rusu, M.C.; Mureșan, A.N. Anatomical Changes in a Case with Asymmetrical Bilateral Maxillary Sinus Hypoplasia. Medicina 2022, 58, 564. [Google Scholar] [CrossRef] [PubMed]
- Sirikci, A.; Bayazit, Y.; G÷m÷sburun, E.; Bayram, M.; Kanlikana, M. A new approach to the classification of maxillary sinus hypoplasia with relevant clinical implications. Surg. Radiol. Anat. 2001, 22, 243–247. [Google Scholar] [CrossRef]
- Güngör, G.; Okur, N.; Okur, E. Uncinate Process Variations and Their Relationship with Ostiomeatal Complex: A Pictorial Essay of Multidedector Computed Tomography (MDCT) Findings. Pol. J. Radiol. 2016, 81, 173–180. [Google Scholar] [CrossRef][Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Right MSV | p Value | Left MSV | p Value | ||||
|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | ||||
| Sex | |||||||
| Male | 9 | (6.8–11.7) | 0.000 | 9.4 | (7.2–11.4) | 0.000 | |
| Female | 7.7 | (5.8–9.6) | 7.9 | (6.1–9.7) | |||
| Deviation | |||||||
| No | 7.2 | (5–9.2) | 0.213 | 8.3 | (5.5–10.4) | 0.669 | |
| Yes | 8.2 | (6.2–10.5) | 8.3 | (6.5–10.4) | |||
| Septum laterality | |||||||
| Left | 8.4 | (6.2–10.6) | 0.757 | 8.3 | (6.6–10.3) | 0.826 | |
| Right | 8 | (6.2–10.3) | 8.3 | (6–10.6) | |||
| Number of right maxillary septum | |||||||
| 0 | 7.5 b | (5.6–9.5) | 0.000 | 7.7 b | (5.8–10.1) | 0.000 | |
| 1 | 9 a | (7–10.9) | 9.1 a | (7.4–10.6) | |||
| 2 | 10 | (7.9–11.4) | 10.3 | (8.3–12) | |||
| 3 | 9.2 | (7–12.2) | 8.6 | (7.1–9.5) | |||
| Number of right maxillary septum | |||||||
| 0 | 7.7 b | (5.6–9.8) | 0.005 | 7.8 b | (5.9–10) | 0.000 | |
| 1 | 8.6 a | (7.1–10.6) | 9.1 ac | (7.2–10.8) | |||
| 2 | 9.4 | (6.6–11.1) | 9.6 b | (7.8–11.6) | |||
| 3 | 8.5 | (6.5–10.6) | 5.9 | (4–7.8) | |||
| 4 | 7.4 | (3.5–11.2) | 7.8 | (4–11.6) | |||
| Right Capsular | |||||||
| 0 | 9.1 | (7.2–11.1) | 0.789 | 9.3 | (7.5–10.8) | 0.647 | |
| 1 | 10.5 | (8.6–11.2) | 8.8 | (7.9–10.7) | |||
| 2 | 9.3 | (9.3–9.3) | 11 | (11–11) | |||
| Left Capsular | |||||||
| 0 | 8.8 | (7–10.9) | 0.118 | 9.2 | (7.4–11.1) | 0.285 | |
| 1 | 7.4 | (6.8–8.2) | 8.5 | (7.1–10.2) | |||
| 2 | 6.1 | (5.7–6.4) | 6.2 | (4.5–7.8) | |||
| 3 | 10.6 | (10.6–10.6) | 7.8 | (7.8–7.8) | |||
| Right turbinate | |||||||
| Absence | 8.2 | (6.3–10.5) | 0.202 | 8.4 | (6.5–10.5) | 0.037 | |
| Presence | 7.3 | (4.8–9.5) | 7.3 | (4.2–9.3) | |||
| Left turbinate | |||||||
| Absence | 8.2 | (6.3–10.3) | 0.350 | 8.3 | (6.5–10.4) | 0.545 | |
| Presence | 7.1 | (5–10.6) | 7.8 | (5.5–10.7) | |||
| Right Ostium | |||||||
| Absence | 8.2 | (6.2–10.3) | 0.891 | 8.3 | (6.5–10.4) | 0.918 | |
| Presence | 7.7 | (6.7–9.5) | 9.1 | (7.3–9.7) | |||
| Left Ostium | |||||||
| Absence | 8.2 | (6.2–10.5) | 0.576 | 8.3 | (6.5–10.4) | 0.389 | |
| Presence | 8.2 | (5.5–9.3) | 8.2 | (6.6–9) | |||
| Right Hypoplasia | |||||||
| Absence | 8.2 | (6.2–10.4) | 0.016 | 8.3 | (6.5–10.4) | 0.017 | |
| Presence | 1.5 | (1–2.1) | 2 | (1.7–2.2) | |||
| Left Hypoplasia | |||||||
| Absence | 8.2 | (6.2–10.3) | 0.502 | 8.3 | (6.5–10.4) | 0.003 | |
| Presence | 7.2 | (2.1–10.7) | 1.4 | (0.5–2.2) | |||
| Location of Edentulism | |||||||
| Right | 8.2 | (6.3–10.7) | 0.056 | 8.8 | (6–10.7) | 0.417 | |
| Left | 7.4 | (5.8–8.9) | 8.1 | (6.1–9.5) | |||
| Bilateral | 7.7 | (5.8–10.6) | 8.2 | (6.4–10.5) | |||
| Random multiple | 8.7 | (6.8–11.2) | 8.5 | (6.3–11.1) | |||
| Right Sinus Volume | p Value | Left Sinus Volume | p Value | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low (<6.95) | Medium (6.96–9.50) | High (<9.50) | Low (<6.95) | Medium (6.96–9.50) | High (<9.50) | ||||||||||
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | ||||
| Sex | |||||||||||||||
| Male | 51 | (28.81) | 48 | (27.12) | 78 | (44.07) | 0.000 | 43 | (24.29) | 47 | (26.55) | 87 | (49.15) | 0.000 | |
| Female | 115 | (39.25) | 101 | (34.47) | 77 | (26.28) | 101 | (34.47) | 115 | (39.25) | 77 | (26.28) | |||
| Deviation | |||||||||||||||
| No | 6 | (40.0) | 6 | (40.0) | 3 | (20.0) | 0.542 | 4 | (26.67) | 5 | (33.33) | 6 | (40.00) | 0.904 | |
| Yes | 160 | (35.16) | 143 | (31.43) | 152 | (33.41) | 140 | (30.77) | 157 | (34.51) | 158 | (34.73) | |||
| Septum laterality | |||||||||||||||
| Left | 95 | (34.55) | 88 | (32.00) | 92 | (33.45) | 0.928 | 82 | (29.82) | 99 | (36.00) | 94 | (34.18) | 0.700 | |
| Right | 65 | (36.11) | 55 | (30.56) | 60 | (33.33) | 58 | (32.22) | 58 | (32.22) | 64 | (35.56) | |||
| Number of right maxillary septum | |||||||||||||||
| 0 | 123 | (44.40) | 86 | (31.05) | 68 | (24.55) | 0.000 | 111 | (40.07) | 89 | (32.13) | 77 | (27.80) | 0.000 | |
| 1 | 37 | 24.34) | 50 | (32.89) | 65 | (42.76) | 30 | (19.74) | 58 | (38.16) | 64 | (42.11) | |||
| 2 | 4 | 11.76) | 11 | (32.35) | 19 | (55.88) | 2 | (5.88) | 11 | (32.35) | 21 | (61.76) | |||
| 3 | 2 | 28.57) | 2 | (28.57) | 3 | (42.86) | 1 | (14.29) | 4 | (57.14) | 2 | (28.57) | |||
| Number of left maxillary septum | |||||||||||||||
| 0 | 116 | (42.65) | 79 | (29.04) | 77 | (28.31) | 0.008 | 101 | (37.13) | 94 | (34.56) | 77 | (28.31) | 0.006 | |
| 1 | 37 | (24.34) | 59 | (38.82) | 56 | (36.84) | 34 | (22.37) | 54 | (35.53) | 64 | (42.11) | |||
| 2 | 11 | (26.19) | 11 | (26.19) | 20 | (47.62) | 7 | (16.67) | 13 | (30.95) | 22 | (52.38) | |||
| 3 | 1 | (50.00) | 0 | (0.00) | 1 | (50.00) | 1 | (50.00) | 1 | (50.00) | 0 | (0.00) | |||
| 4 | 1 | (50.00) | 0 | (0.00) | 1 | (50.00) | 1 | (50.00) | 0 | (0.00) | 1 | (50.00) | |||
| Left Capsular | |||||||||||||||
| 0 | 45 | (24.46) | 63 | (34.24) | 76 | (41.30) | 0.046 | 40 | (21.74) | 61 | (33.15) | 83 | (45.11) | 0.622 | |
| 1 | 3 | (27.27) | 7 | (63.64) | 1 | (9.09) | 2 | (18.18) | 5 | (45.45) | 4 | (36.36) | |||
| 2 | 2 | (100.00) | 0 | (0.00) | 0 | (0.00) | 1 | (50.00) | 1 | (50.00) | 0 | (0.00) | |||
| 3 | 0 | (0.00) | 0 | (0.00) | 1 | (100.00) | 0 | (0.00) | 1 | (100.00) | 0 | (0.00) | |||
| Left Ostium | |||||||||||||||
| Absence | 163 | (35.28) | 146 | (31.60) | 153 | (33.12) | 0.881 | 141 | (30.52) | 157 | (33.98) | 164 | (35.50) | 0.090 | |
| Presence | 3 | (37.50) | 3 | (37.50) | 2 | (25.00) | 3 | (37.50) | 5 | (62.50) | 0 | (0.00) | |||
| Right Hypoplasia | |||||||||||||||
| Absence | 164 | (35.04) | 149 | (31.84) | 155 | (33.12) | 0.159 | 142 | (30.34) | 162 | (34.62) | 164 | (35.04) | 0.103 | |
| Presence | 2 | (100.00) | 0 | (0.00) | 0 | (0.00) | 2 | (100.00) | 0 | (0.00) | 0 | (0.00) | |||
| Left Hypoplasia | |||||||||||||||
| Absence | 165 | (35.33) | 148 | (31.69) | 154 | (32.98) | 0.997 | 141 | (30.19) | 162 | (34.69) | 164 | (35.12) | 0.033 | |
| Presence | 1 | (33.33) | 1 | (33.33) | 1 | (33.33) | 3 | (100.00) | 0 | (0.00) | 0 | (0.00) | |||
| Edentulism location | |||||||||||||||
| Right | 21 | (33.33) | 17 | (26.98) | 25 | (39.68) | 0.068 | 21 | (33.33) | 18 | (28.57) | 24 | (38.10) | 0.412 | |
| Left | 29 | (42.65) | 26 | (38.24) | 13 | (19.12) | 23 | (33.82) | 28 | (41.18) | 17 | (25.00) | |||
| Bilateral | 21 | (42.00) | 12 | (24.00) | 17 | (34.00) | 18 | (36.00) | 13 | (26.00) | 19 | (38.00) | |||
| Random Multiple | 17 | (26.15) | 21 | (32.31) | 27 | (41.54) | 17 | (26.15) | 23 | (35.38) | 25 | (38.46) | |||
| Decreased Right Maxillary Sinus | Decreased Left Maxillary Sinus | ||||||
|---|---|---|---|---|---|---|---|
| OR | IC 95% | p Value | OR | IC 95% | p Value | ||
| Gender | |||||||
| Male | 1 | 1 | |||||
| Female | 1.89 | (1.23–2.91) | 0.004 | 1.87 | (1.20–2.93) | 0.006 | |
| Numbers of right septa | |||||||
| 0 | 1 | 1 | |||||
| 1 | 0.46 | (0.28–0.73) | 0.001 | 0.39 | (0.23–0.64) | 0.000 | |
| 2 | 0.19 | (0.06–0.60) | 0.005 | 0.11 | (0.02–0.49) | 0.004 | |
| 3 | 0.64 | (0.11–3.60) | 0.614 | 0.31 | (0.03–2.82) | 0.304 | |
| Numbers of left septa | |||||||
| 0 | 1 | 1 | |||||
| 1 | 0.50 | (0.31–0.81) | 0.005 | 0.60 | (0.36–0.98) | 0.044 | |
| 2 | 0.79 | (0.35–1.79) | 0.578 | 0.60 | (0.24–1.53) | 0.295 | |
| 3 | 1.69 | (0.08 -32.0) | 0.726 | 2.16 | (0.10–43.6) | 0.613 | |
| 4 | 1.23 | (0.71- 21.1) | 0.885 | 1.58 | (0.08–27.8) | 0.753 | |
| Left obstruction | |||||||
| Absence | 1 | 1 | |||||
| Presence | 0.25 | (0.05–1.17) | 0.080 | 0.30 | (0.06–1.45) | 0.137 | |
| Right turbinate | |||||||
| Absence | 1 | 1 | |||||
| Presence | 0.25 | (0.05–1.17) | 0.080 | 0.91 | (0.43–1.94) | 0.825 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez Betancourt, A.B.; Martinez Somoza, L.J.; Romero Mesa, C.; Tozum, T.F.; Mourão, C.F.; Shibli, J.A.; Suárez, L.J. Relationship of Maxillary Sinus Volume and Nasal Septum Deviation: A Cone Beam Computed Tomography Study. Diagnostics 2024, 14, 647. https://doi.org/10.3390/diagnostics14060647
Rodriguez Betancourt AB, Martinez Somoza LJ, Romero Mesa C, Tozum TF, Mourão CF, Shibli JA, Suárez LJ. Relationship of Maxillary Sinus Volume and Nasal Septum Deviation: A Cone Beam Computed Tomography Study. Diagnostics. 2024; 14(6):647. https://doi.org/10.3390/diagnostics14060647
Chicago/Turabian StyleRodriguez Betancourt, Amanda B., Leidy J. Martinez Somoza, Carlos Romero Mesa, Tolga Fikret Tozum, Carlos Fernando Mourão, Jamil Awad Shibli, and Lina J. Suárez. 2024. "Relationship of Maxillary Sinus Volume and Nasal Septum Deviation: A Cone Beam Computed Tomography Study" Diagnostics 14, no. 6: 647. https://doi.org/10.3390/diagnostics14060647
APA StyleRodriguez Betancourt, A. B., Martinez Somoza, L. J., Romero Mesa, C., Tozum, T. F., Mourão, C. F., Shibli, J. A., & Suárez, L. J. (2024). Relationship of Maxillary Sinus Volume and Nasal Septum Deviation: A Cone Beam Computed Tomography Study. Diagnostics, 14(6), 647. https://doi.org/10.3390/diagnostics14060647