
The Influence of Pericardial Fat on Left Ventricular Diastolic Function




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Protocol
2.3. Study Variables
2.4. Statistical Analysis of the Sample
2.5. Ethical Considerations
3. Results
3.1. Abdominal Circumference and Pericardial and Epicardial Fat
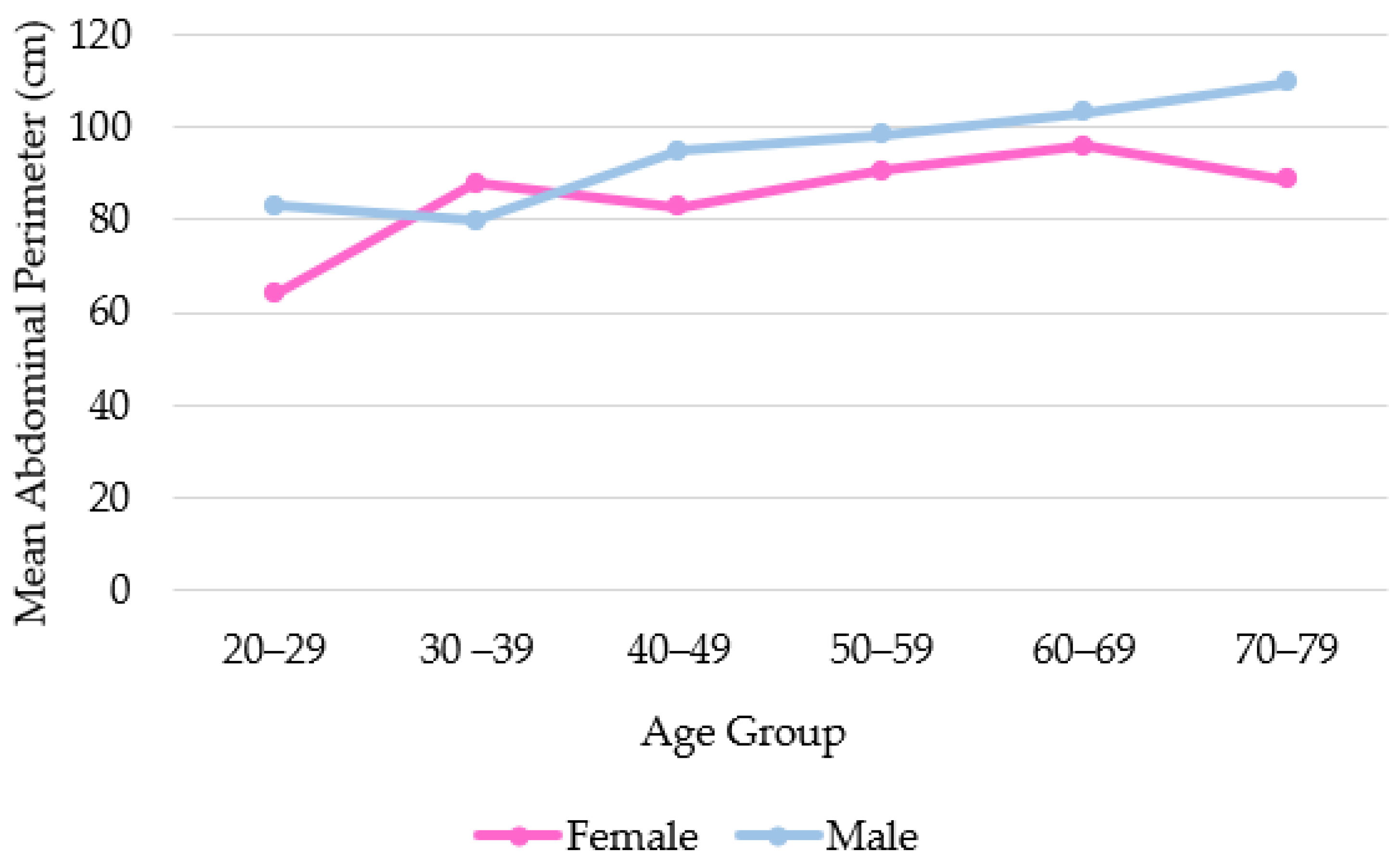
3.2. Association between Abdominal Circumference and Age Group
3.3. Assessment of Echocardiographic Variables and PF
3.4. Association between Abdominal Circumference and PF and EF Thickness
3.5. Association of Echocardiographic Variables with Pericardial Fat vs. Epicardial Fat
3.6. Association between Pericardial Fat and Echocardiographic Variables, Multivariable Adjustment of Co-Factors
3.7. Assessment between Pericardial Fat and the Diagnosis of Diastolic Function
4. Discussion
4.1. Sample Characterization
4.2. Association of Abdominal Circumference with Age in Male and Female
4.3. Relationship between Pericardial Fat and Abdominal Circumference
4.4. Assessment of Echocardiographic Variables and Pericardial Fat
4.5. Association of Echocardiographic Variables with Pericardial Fat vs. Epicardial Fat
4.6. Association between Pericardial Fat and Echocardiographic Variables, Multivariable Adjustment of Co-Factors
4.7. Assessment between PF and the Diagnosis of Diastolic Dysfunction
4.8. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Wit-Verheggen, V.H.W.; Altintas, S.; Spee, R.J.M.; Mihl, C.; Van Kuijk, S.M.J.; Wildberger, J.E.; Schrauwen-Hinderling, V.B.; Kietselaer, B.L.J.H.; van de Weijer, T. Pericardial fat and its influence on cardiac diastolic function. Cardiovasc. Diabetol. 2020, 19, 129. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Zhang, B.; Yang, Y.; Qi, L.; Zhou, J.; Li, M.; Jia, J.; Zhang, Y.; Yong, H. Association of epicardial fat thickness with left ventricular diastolic function parameters in a community population. BMC Cardiovasc. Disord. 2021, 21, 262. [Google Scholar] [CrossRef] [PubMed]
- Kitterer, D.; Latus, J.; Henes, J.; Birkmeier, S.; Backes, M.; Braun, N.; Sechtem, U.; Alscher, M.D.; Mahrholdt, H.; Greulich, S. Impact of long-term steroid therapy on epicardial and pericardial fat deposition: A cardiac MRI study. Cardiovasc. Diabetol. 2015, 14, 130. [Google Scholar] [CrossRef] [PubMed]
- Tekin, I.; Edem, E. Association of epicardial fat tissue with coronary artery disease and left ventricle diastolic function indicators. Med. Sci. Monit. 2018, 24, 6367–6374. [Google Scholar] [CrossRef]
- Kenchaiah, S.; Ding, J.; Carr, J.J.; Allison, M.A.; Budoff, M.J.; Tracy, R.P.; Burke, G.L.; McClelland, R.L.; Arai, A.E.; Bluemke, D.A. Pericardial Fat and the Risk of Heart Failure. J. Am. Coll. Cardiol. 2021, 77, 2638–2652. [Google Scholar] [CrossRef] [PubMed]
- Larsen, B.A.; Laughlin, G.A.; Saad, S.D.; Barrett-Connor, E.; Allison, M.A.; Wassel, C.L. Pericardial fat is associated with all-cause mortality but not incident CVD: The Rancho Bernardo Study. Atherosclerosis 2015, 239, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American society of echocardiography and the European association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Okura, K.; Maeno, K.; Okura, S.; Takemori, H.; Toya, D.; Tanaka, N.; Miyayama, S. Pericardial fat volume is an independent risk factor for the severity of coronary artery disease in patients with preserved ejection fraction. J. Cardiol. 2015, 65, 37–41. [Google Scholar] [CrossRef]
- Hirata, Y.; Yamada, H.; Sata, M. Epicardial fat and pericardial fat surrounding the heart have different characteristics. Circ. J. 2018, 82, 2475–2476. [Google Scholar] [CrossRef]
- Son, J.W.; Sung, J.K.; Lee, J.W.; Youn, Y.J.; Ahn, M.S.; Ahn, S.G.; Yoo, B.S.; Lee, S.H.; Yoon, J.; Koh, S.B.; et al. Abdominal obesity and structure and function of the heart in healthy male Koreans the ARIRANG study. Medicine 2016, 95, e4930. [Google Scholar] [CrossRef] [PubMed]
- Fontes-Carvalho, R.; Gonçalves, A.; Severo, M.; Lourenço, P.; Rocha Gonçalves, F.; Bettencourt, P.; Leite-Moreira, A.; Azevedo, A. Direct, inflammation-mediated and blood-pressure-mediated effects of total and abdominal adiposity on diastolic function: EPIPorto study. Int. J. Cardiol. 2015, 191, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Vural, M.; Talu, A.; Sahin, D.; Elalmis, O.U.; Durmaz, H.A.; UyanIk, S.; Dolek, B.A. Evaluation of the relationship between epicardial fat volume and left ventricular diastolic dysfunction. Jpn. J. Radiol. 2014, 32, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Konishi, M.; Sugiyama, S.; Sugamura, K.; Nozaki, T.; Matsubara, J.; Akiyama, E.; Utsunomiya, D.; Matsuzawa, Y.; Yamashita, Y.; Kimura, K.; et al. Accumulation of pericardial fat correlates with left ventricular diastolic dysfunction in patients with normal ejection fraction. J. Cardiol. 2012, 59, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Nerlekar, N.; Muthalaly, R.G.; Wong, N.; Thakur, U.; Wong, D.T.L.; Brown, A.J.; Marwick, T.H. Association of volumetric epicardial adipose tissue quantification and cardiac structure and function. J. Am. Heart Assoc. 2018, 7, e009975. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for Europe. WHO European Regional Obesity: Report; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Wharton, S.; Lau, D.C.W.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in adults: A clinical practice guideline. Can. Med. Assoc. J. 2020, 192, E875–E891. [Google Scholar] [CrossRef]
- Andrade, K.A.P.; Rojas, M.A.P. Abdominal Circumference Cut-Off Point: An Overview. AVFT Archivos Venezolanos de Farmacología y Terapéutica 2022, 41, 299–306. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Eroğlu, S. How do we measure epicardial adipose tissue thickness by transthoracic echocardiography? Anatol. J. Cardiol. 2015, 15, 416–419. [Google Scholar] [CrossRef]
- Perfil Regional de Saúde Região Centro [Internet]. 2018. Available online: https://www.arscentro.min-saude.pt/wp-content/uploads/sites/6/2021/04/PeRS_Centro_2018.pdf (accessed on 20 January 2024).
- Kuk, J.L.; Lee, S.; Heymsfield, S.B.; Ross, R. Waist circumference and abdominal adipose tissue distribution: Influence of age and sex. Am. J. Clin. Nutr. 2005, 81, 1330–1334. [Google Scholar] [CrossRef]
- Stevens, J.; Katz, E.G.; Huxley, R.R. Associations between gender, age and waist circumference. Eur. J. Clin. Nutr. 2010, 64, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Mahabadi, A.A.; Massaro, J.M.; Rosito, G.A.; Levy, D.; Murabito, J.M.; Wolf, P.A.; O’Donnell, C.J.; Fox, C.S.; Hoffmann, U. Association of pericardial fat, intrathoracic fat, and visceral abdominal fat with cardiovascular disease burden: The Framingham Heart Study. Eur. Heart J. 2009, 30, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Ni, X.; Jiao, L.; Zhang, Y.; Xu, J.; Zhang, Y.; Zhang, X.; Du, Y.; Sun, Z.; Wang, S. Correlation between the distribution of abdominal, pericardial and subcutaneous fat and muscle and age and gender in a middle-aged and elderly population. Diabetes Metab. Syndr. Obes. 2021, 14, 2201–2208. [Google Scholar] [CrossRef]
- Rabkin, S.W. The relationship between epicardial fat and indices of obesity and the metabolic syndrome: A systematic review and meta-analysis. Metab. Syndr. Relat. Disord. 2014, 12, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Gu, S.; Wang, Q.; Zhou, X.; Wang, S.; Fu, C.; Yang, W.; Wetzl, J.; Yan, F. Left ventricular myocardial deformation: A study on diastolic function in the Chinese male population and its relationship with fat distribution. Quant. Imaging Med. Surg. 2020, 10, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Vaibhav Patel, B.B.; Mori, J.; McLean, B.A.; Basu, R.; Das, S.K.; Ramprasath, T.; Parajuli, N.; Penninger, J.M.; Grant, M.B.; Lopaschuk, G.D. ACE2 deficiency worsens epicardial adipose tissue inflammation and cardiac dysfunction in response to diet-induced obesity. Diabetes 2015, 65, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Leonetti, F.; Singh, N.M.; Sharma, A. Relationship of epicardial adipose tissue with atrial dimensions and diastolic function in morbidly obese subjects. Int. J. Cardiol. 2007, 115, 272–273. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Kim, S.W.; Lee, J.S.; Lee, S.K.; Abbott, R.; Lee, K.Y.; Lim, H.E.; Sung, K.C.; Cho, G.Y.; Koh, K.K.; et al. Association of pericardial adipose tissue with left ventricular structure and function: A region-specific effect? Cardiovasc. Diabetol. 2021, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.S.; Gona, P.; Hoffmann, U.; Porter, S.A.; Salton, C.J.; Massaro, J.M.; Levy, D.; Larson, M.G.; D’Agostino, R.B.; O’Donnell, C.J.; et al. Pericardial fat, intrathoracic fat, and measures of left ventricular structure and function. Circulation 2009, 119, 1586–1591. [Google Scholar] [CrossRef]
- Mahajan, R.; Lau, D.H.; Brooks, A.G.; Shipp, N.J.; Manavis, J.; Wood, J.P.M.; Finnie, J.W.; Samuel, C.S.; Royce, S.G.; Twomey, D.J.; et al. Electrophysiological, Electroanatomical, and Structural Remodeling of the Atria as Consequences of Sustained Obesity. J. Am. Coll. Cardiol. 2015, 66, 1–11. [Google Scholar] [CrossRef]
- Hahn, R.T.; Badano, L.P.; Bartko, P.E.; Muraru, D.; Maisano, F.; Zamorano, J.L.; Donal, E. Tricuspid regurgitation: Recent advances in understanding pathophysiology, severity grading and outcome. Eur. Heart J.-Cardiovasc. Imaging 2022, 23, 913–929. [Google Scholar] [CrossRef] [PubMed]
- Cai, A.; Liu, L.; Zhou, D.; Zhou, Y.; Tang, S.; Feng, Y. The patterns of left ventricular alteration by adipose tissue distribution: Implication for heart failure prevention. ESC Heart Fail. 2021, 8, 3093–3105. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Kishino, T.; Sano, J.; Ariga, T.; Okuyama, S.; Mori, H.; Matsushima, S.; Ohtsuka, K.; Ohnishi, H.; Watanabe, T. Relationship between epicardial adipose tissue thickness and early impairment of left ventricular systolic function in patients with preserved ejection fraction. Heart Vessels 2016, 31, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- van Woerden, G.; Gorter, T.M.; Westenbrink, B.D.; Willems, T.P.; van Veldhuisen, D.J.; Rienstra, M. Epicardial fat in heart failure patients with mid-range and preserved ejection fraction. Eur. J. Heart Fail. 2018, 20, 1559–1566. [Google Scholar] [CrossRef] [PubMed]
- Obokata, M.; Reddy, Y.N.V.; Borlaug, B.A. Diastolic Dysfunction and Heart Failure with Preserved Ejection Fraction: Understanding Mechanisms by Using Noninvasive Methods. JACC Cardiovasc. Imaging 2020, 13, 245–257. [Google Scholar] [CrossRef]
- Cherian, S.; Lopaschuk, G.D.; Carvalho, E. Cellular cross-talk between epicardial adipose tissue and myocardium in relation to the pathogenesis of cardiovascular disease. Am. J. Physiol. Endocrinol. Metab. 2012, 303, E937–E949. [Google Scholar] [CrossRef]
- Van De Weijer, T.; Schrauwen-Hinderling, V.B.; Schrauwen, P. Lipotoxicity in type 2 diabetic cardiomyopathy. Cardiovasc. Res. 2011, 92, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.C.T.; Goo, S.Y.; Roche, N.; van der Geest, R.J.; Wang, W.Y.S. Epicardial Adipose Tissue Volume and Left Ventricular Myocardial Function Using 3-Dimensional Speckle Tracking Echocardiography. Can. J. Cardiol. 2016, 32, 1485–1492. [Google Scholar] [CrossRef]
- Arshi, B.; Aliahmad, H.A.; Ikram, M.A.; Bos, D.; Kavousi, M. Epicardial Fat Volume, Cardiac Function, and Incident Heart Failure: The Rotterdam Study. J. Am. Heart Assoc. 2023, 12, e026197. [Google Scholar] [CrossRef]
- Okura, H.; Takada, Y.; Yamabe, A.; Kubo, T.; Asawa, K.; Ozaki, T.; Yamagishi, H.; Toda, I.; Yoshiyama, M.; Yoshikawa, J.; et al. Age-and gender-specific changes in the left ventricular relaxation a doppler echocardiographic study in healthy individuals. Circ. Cardiovasc. Imaging 2009, 2, 41–46. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| Sex | |
| Female (n, %) | 39 (48%) |
| Male (n, %) | 43 (52%) |
| Age (years) | 58 ± 12.8 |
| Age Group (n) | |
| 20–29 y | 2 (2.4%) |
| 30–39 y | 6 (7.3%) |
| 40–49 y | 13 (15.9%) |
| 50–59 y | 17 (20.7%) |
| 60–69 y | 29 (35.4%) |
| 70–79 y | 15 (18.3%) |
| Weight (kg) | 79.56 ± 25.8 |
| Height (cm) | 164.85 ± 9.50 |
| BMI (kg/m2) | 29.17 ± 8.49 |
| BMI Classes (n) | |
| Underweight | 1 (1.2%) |
| Normal | 25 (30.5%) |
| Overweight | 30 (36.6%) |
| Obesity I | 16 (19.5%) |
| Obesity II | 5 (6.1%) |
| Obesity III | 5 (6.1%) |
| Abdominal Circumference (cm) | 94.8 ± 13.3 |
| PF Low | PF High | p-Value | |
|---|---|---|---|
| PF Thickness (mm) | 3.1 | 6.5 | <0.0001 |
| EF Thickness (mm) | 3.6 | 7.1 | <0.0001 |
| Abdominal Circumference (cm) | 89.62 | 101.7 | <0.0001 |
| Total (n) | 45 | 37 |
| Total Population (n = 82) | PF Low (n = 45) | PF High (n = 37) | (p-Value) | |
|---|---|---|---|---|
| E (cm/s) * | 67.88 ± 16.57 | 69.41 ± 11.92 | 66.01 ± 20.92 | p = 0.359 |
| DT (ms) * | 0.20 ± 0.05 | 0.18 ± 0.04 | 0.21 ± 0.063 | p = 0.013 |
| E/A ** | 1.03 ± 0.43 | 1.10 ± 0.34 | 0.94 ± 0.50 | p = 0.003 |
| septal e’ (cm/s) * | 8.25 ± 2.45 | 9.58 ± 2.17 | 6.64 ± 1.70 | p < 0.0001 |
| lateral e’ (cm/s) * | 11.82 ± 3.20 | 13.23 ± 3.30 | 10.12 ± 2.06 | p < 0.0001 |
| E/e’ * | 7.34 ± 2.62 | 6.40 ± 2.01 | 8.48 ± 2.83 | p < 0.0001 |
| LAV (mL/m2) * | 36.65 ± 8.33 | 32.80 ± 4.97 | 41.33 ± 9.22 | p < 0.0001 |
| LVEF (%) * | 65.57 ± 5.62 | 66.52 ± 4.99 | 64.42 ± 6.18 | p = 0.093 |
| LV Mass (g) * | 164.95 ± 52.34 | 149.64 ± 34.08 | 183.57 ± 63.99 | p = 0.003 |
| TRJV (cm/s) ** | 2.47 ± 0.29 | 2.32 ± 0.22 | 2.65 ± 0.26 | p < 0.0001 |
| LV Diameter (mm) * | 53.34 ± 5.19 | 52.07 ± 4.03 | 54.89 ± 6.04 | p = 0.014 |
| Pericardial Fat | Epicardial Fat | |||||
|---|---|---|---|---|---|---|
| Correlation | Correlation Degree | (p-Value) | Correlation | Correlation Degree | (p-Value) | |
| E (cm/s) | −0.053 | Non-Significant | p = 0.633 | 0.032 | Non-Significant | p = 0.776 |
| DT (ms) | 0.222 | Low | p = 0.045 | 0.208 | Non-Significant | p = 0.061 |
| E/A | −0.363 | Moderate | p = 0.001 | −0.403 | Moderate | p < 0.0001 |
| septal e’ (cm/s) | −0.686 | High | p < 0.0001 | −0.731 | High | p < 0.0001 |
| lateral e’ (cm/s) | −0.630 | High | p < 0.0001 | −0.662 | High | p < 0.0001 |
| E/e’ | 0.494 | Moderate | p < 0.0001 | 0.592 | High | p < 0.0001 |
| LAV (mL/m2) | 0.683 | High | p < 0.0001 | 0.693 | High | p < 0.0001 |
| LVEF (%) | −0.141 | Non-Significant | p = 0.207 | −0.216 | Non-Significant | p = 0.052 |
| LV Mass (g) | 0.359 | Moderate | p = 0.001 | 0.397 | Moderate | p < 0.0001 |
| TRJV (cm/s) | 0.629 | High | p < 0.0001 | 0.610 | High | p < 0.0001 |
| LV Diam (mm) | 0.227 | Low | p = 0.041 | 0.282 | Low | p = 0.010 |
| Variables | Unadjusted Regression Coefficient (95% CI) | p-Value | Adjusted Regression Coefficient (95% CI) ª | p-Value |
|---|---|---|---|---|
| septal e’ | −0.639 | <0.0001 | −0.189 | 0.031 |
| LAV | 0.613 | <0.0001 | 0.457 | <0.0001 |
| TRJV | 0.595 | <0.0001 | 0.381 | 0.001 |
| LVEF | −0.298 | 0.007 | −0.330 | 0.024 |
| LV Diameter | 0.388 | <0.0001 | 0.297 | 0.016 |
| LV Mass | 0.473 | <0.0001 | 0.381 | 0.001 |
| PF Low | PF High | p-Value | |
|---|---|---|---|
| Normal | 38 | 8 | <0.0001 |
| Undetermined | 4 | 12 | <0.0001 |
| Diastolic Dysfunction | 3 | 17 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, P.; Duarte, H.; Alcafache, C.; Rodrigues, F. The Influence of Pericardial Fat on Left Ventricular Diastolic Function. Diagnostics 2024, 14, 702. https://doi.org/10.3390/diagnostics14070702
Coelho P, Duarte H, Alcafache C, Rodrigues F. The Influence of Pericardial Fat on Left Ventricular Diastolic Function. Diagnostics. 2024; 14(7):702. https://doi.org/10.3390/diagnostics14070702
Chicago/Turabian StyleCoelho, Patrícia, Hugo Duarte, Carlos Alcafache, and Francisco Rodrigues. 2024. "The Influence of Pericardial Fat on Left Ventricular Diastolic Function" Diagnostics 14, no. 7: 702. https://doi.org/10.3390/diagnostics14070702
APA StyleCoelho, P., Duarte, H., Alcafache, C., & Rodrigues, F. (2024). The Influence of Pericardial Fat on Left Ventricular Diastolic Function. Diagnostics, 14(7), 702. https://doi.org/10.3390/diagnostics14070702