
Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Liver Steatosis Assessment
- (1)
- FLI: (FLI = (e0.953*loge(triglycerides)+0.139*BMI+0.718*loge (GGT)+0.053*WC−15.745)/(1 + e0.953*loge(triglycerides)+0.139*BMI+0.718*loge (GGT)+0.053*WC−15.745) × 100) [14];
- (2)
- HIS: (HSI = 8 × ALT/AST + BMI(+2 if type 2 DM present, +2 if female)) [15];
- (3)
- TyG: Ln [Tg (mg/dL) × fasting glucose (mg/dL)/2] [19];
- (4)
- TyG-BMI: (TyG index × BMI) [25];
- (5)
- TyG-WC (TyG index) × (waist circumference (cm)) [25].
2.3. Statistical Analysis
3. Results
3.1. Study Population
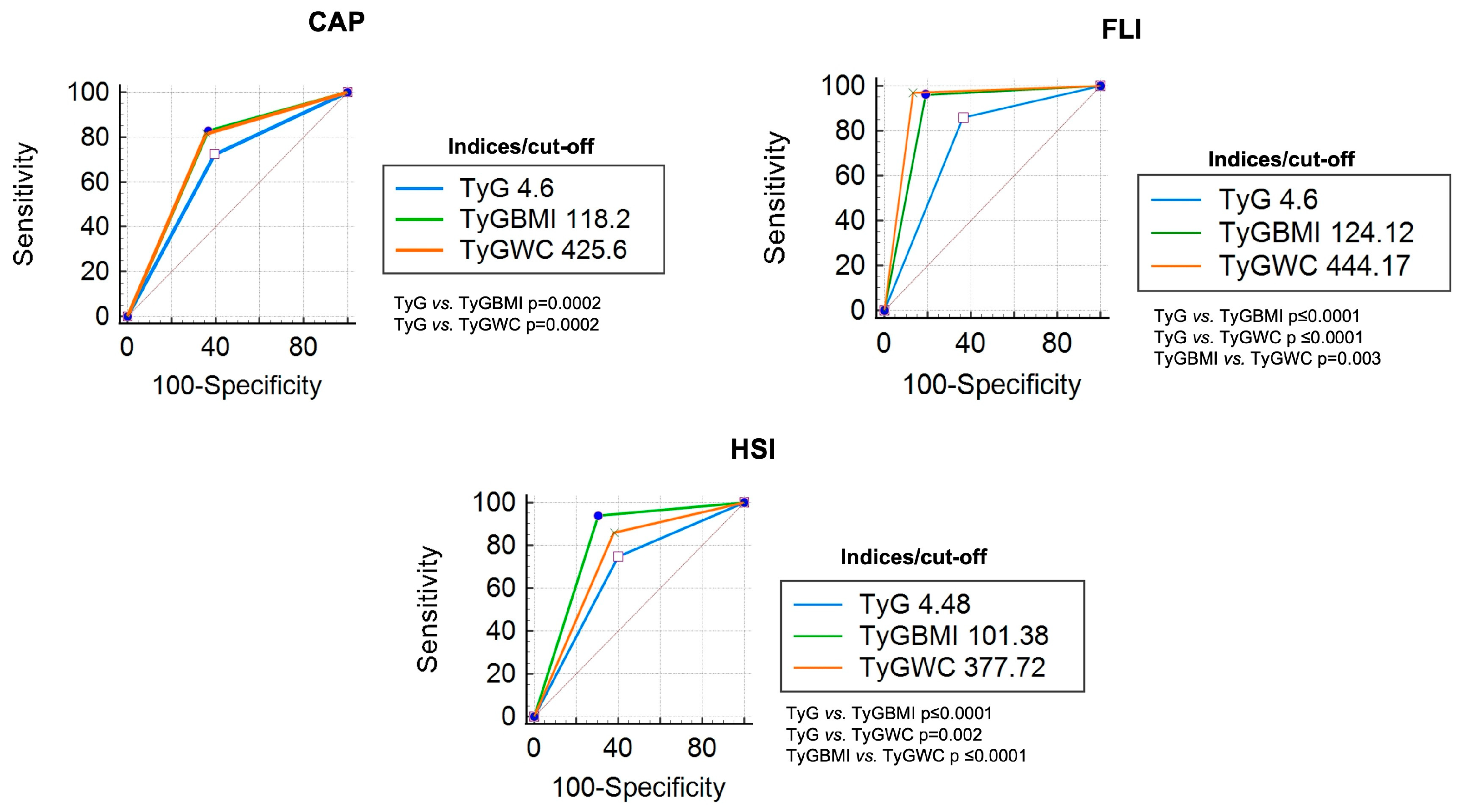
3.2. Diagnostic Accuracy of TyG Index, TyG-BMI Index, and TyG-WC Index
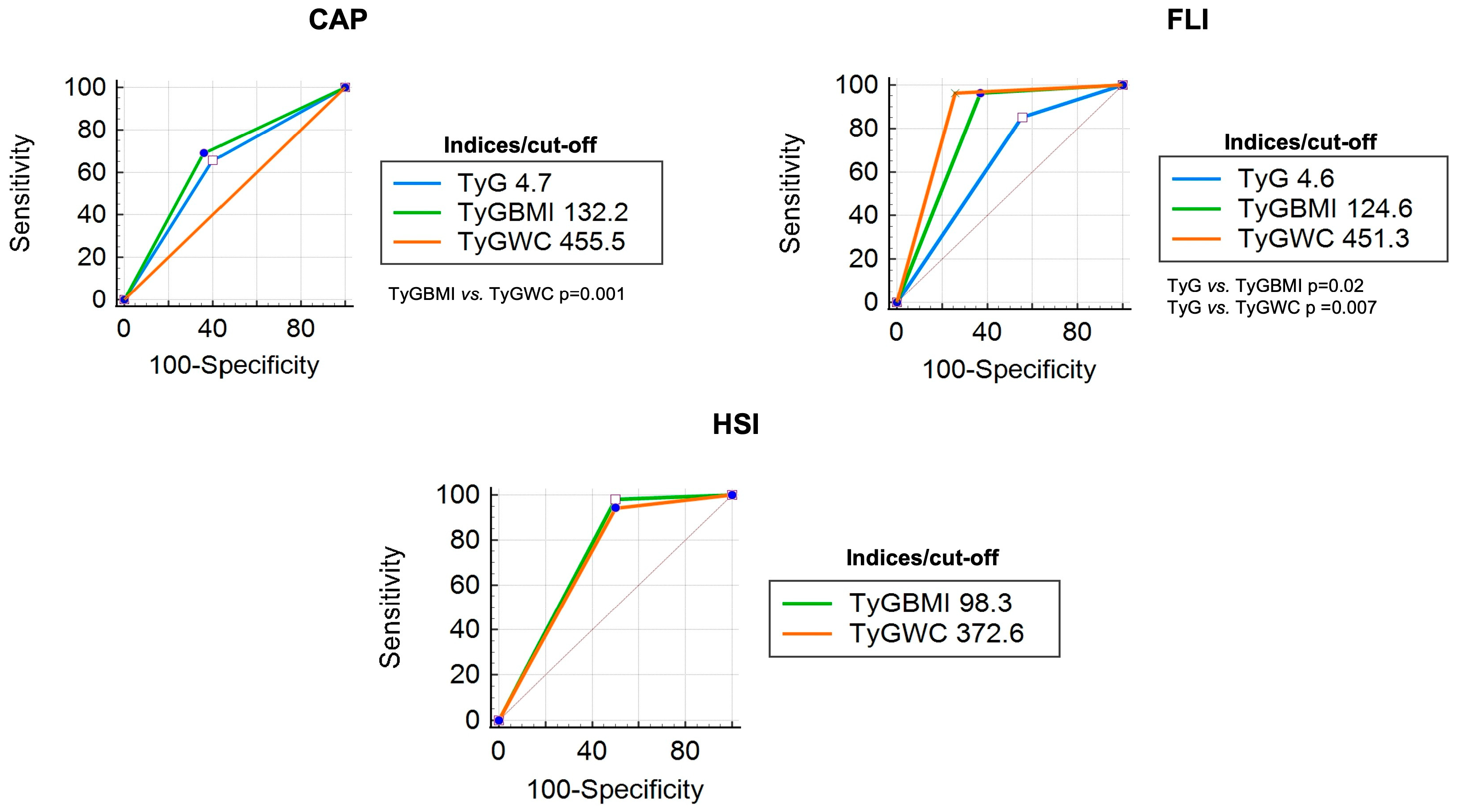
3.3. Diagnostic Accuracy of TyG Index, TyG-BMI Index, and TyG-WC Index in Patients with DM
3.4. Diagnostic Accuracy of TyG Index, TyG-BMI Index, and TyG-WC Index in Overweight/Obese Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A Multisociety Delphi Consensus Statement on New Fatty Liver Disease Nomenclature. J. Hepatol. 2023, 79, 1542–1556. [Google Scholar] [CrossRef]
- Khan, R.S.; Bril, F.; Cusi, K.; Newsome, P.N. Modulation of Insulin Resistance in Nonalcoholic Fatty Liver Disease. Hepatology 2019, 70, 711–724. [Google Scholar] [CrossRef] [PubMed]
- Tomizawa, M.; Kawanabe, Y.; Shinozaki, F.; Sato, S.; Motoyoshi, Y.; Sugiyama, T.; Yamamoto, S.; Sueishi, M. Triglyceride Is Strongly Associated with Nonalcoholic Fatty Liver Disease among Markers of Hyperlipidemia and Diabetes. Biomed. Rep. 2014, 2, 633–636. [Google Scholar] [CrossRef]
- Zhou, F.; Zhou, J.; Wang, W.; Zhang, X.J.; Ji, Y.X.; Zhang, P.; She, Z.G.; Zhu, L.; Cai, J.; Li, H. Unexpected Rapid Increase in the Burden of NAFLD in China From 2008 to 2018: A Systematic Review and Meta-Analysis. Hepatology 2019, 70, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Zhang, X.; Li, G.; Wong, G.L.H.; Wong, V.W.S. Epidemiology and Clinical Outcomes of Metabolic (Dysfunction)-Associated Fatty Liver Disease. J. Clin. Transl. Hepatol. 2021, 9, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The Diagnosis and Management of Non-Alcoholic Fatty Liver Disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease—Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Powell, E.E.; Wong, V.W.S.; Rinella, M. Non-Alcoholic Fatty Liver Disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Pal, S.C.; Méndez-Sánchez, N. Screening for MAFLD: Who, When and How? Ther. Adv. Endocrinol. Metab. 2023, 14, 20420188221145650. [Google Scholar] [CrossRef]
- Graffigna, M.; Catoira, N.; Soutelo, J.; Azpelicueta, A.; Berg, G.; Perel, C.; Migliano, M.E.; Aranguren, M.; Musso, C.; Farias, J. Diagnóstico de Esteatosis Hepática Por Métodos Clínicos, Bioquímicos y Por Imágenes. Rev. Argent. Endocrinol. Metab. 2017, 54, 37–46. [Google Scholar] [CrossRef]
- Pu, K.; Wang, Y.; Bai, S.; Wei, H.; Zhou, Y.; Fan, J.; Qiao, L. Diagnostic Accuracy of Controlled Attenuation Parameter (CAP) as a Non-Invasive Test for Steatosis in Suspected Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. BMC Gastroenterol. 2019, 19, 51. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Cuevas, J.; Santos, A.; Armendariz-Borunda, J. Pathophysiological Molecular Mechanisms of Obesity: A Link between MAFLD and NASH with Cardiovascular Diseases. Int. J. Mol. Sci. 2021, 22, 11629. [Google Scholar] [CrossRef] [PubMed]
- Pipitone, R.M.; Ciccioli, C.; Infantino, G.; La Mantia, C.; Parisi, S.; Tulone, A.; Pennisi, G.; Grimaudo, S.; Petta, S. MAFLD: A Multisystem Disease. Ther. Adv. Endocrinol. Metab. 2023, 14, 20420188221145549. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A Simple and Accurate Predictor of Hepatic Steatosis in the General Population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic Steatosis Index: A Simple Screening Tool Reflecting Nonalcoholic Fatty Liver Disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V. Performance and Limitations of Steatosis Biomarkers in Patients with Nonalcoholic Fatty Liver Disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Du, T.; Zhang, J.; Lu, H.; Lin, X.; Xie, J.; Yang, Y.; Yu, X. The Triglyceride and Glucose Index (TyG) Is an Effective Biomarker to Identify Nonalcoholic Fatty Liver Disease. Lipids Health Dis. 2017, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Simental-Mendía, L.E.; González-Ortiz, M.; Martínez-Abundis, E.; Ramos-Zavala, M.G.; Hernández-González, S.O.; Jacques-Camarena, O.; Rodríguez-Morán, M. The Product of Triglycerides and Glucose, a Simple Measure of Insulin Sensitivity. Comparison with the Euglycemic-Hyperinsulinemic Clamp. J. Clin. Endocrinol. Metab. 2010, 95, 3347–3351. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendía, L.E.; Rodríguez-Morán, M.; Guerrero-Romero, F. The Product of Fasting Glucose and Triglycerides as Surrogate for Identifying Insulin Resistance in Apparently Healthy Subjects. Metab. Syndr. Relat. Disord. 2008, 6, 299–304. [Google Scholar] [CrossRef]
- Wang, J.; Yan, S.; Cui, Y.; Chen, F.; Piao, M.; Cui, W. The Diagnostic and Prognostic Value of the Triglyceride-Glucose Index in Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD): A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4969. [Google Scholar] [CrossRef]
- Zheng, S.; Shi, S.; Ren, X.; Han, T.; Li, Y.; Chen, Y.; Liu, W.; Hou, P.C.; Hu, Y. Triglyceride Glucose-Waist Circumference, a Novel and Effective Predictor of Diabetes in First-Degree Relatives of Type 2 Diabetes Patients: Cross-Sectional and Prospective Cohort Study. J. Transl. Med. 2016, 14, 260. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Cho, Y.K.; Kim, E.H.; Lee, M.J.; Jung, C.H.; Park, J.Y.; Kim, H.K.; Lee, W.J. Triglyceride Glucose-Waist Circumference Is Superior to the Homeostasis Model Assessment of Insulin Resistance in Identifying Nonalcoholic Fatty Liver Disease in Healthy Subjects. J. Clin. Med. 2021, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Xu, J.; Li, M.; Gao, Y. Potential Screening Indicators for Early Diagnosis of NAFLD/MAFLD and Liver Fibrosis: Triglyceride Glucose Index-Related Parameters. Front. Endocrinol. 2022, 13, 951689. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.T.; Xiang, L.L.; Qi, F.; Zhang, Y.J.; Chen, Y.; Zhou, X.Q. Accuracy of Controlled Attenuation Parameter (CAP) and Liver Stiffness Measurement (LSM) for Assessing Steatosis and Fibrosis in Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. EClinicalMedicine 2022, 51, 101547. [Google Scholar] [CrossRef] [PubMed]
- Khamseh, M.E.; Malek, M.; Abbasi, R.; Taheri, H.; Lahouti, M.; Alaei-Shahmiri, F. Triglyceride Glucose Index and Related Parameters (Triglyceride Glucose-Body Mass Index and Triglyceride Glucose-Waist Circumference) Identify Nonalcoholic Fatty Liver and Liver Fibrosis in Individuals with Overweight/Obesity. Metab. Syndr. Relat. Disord. 2021, 19, 167–173. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Kitae, A.; Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. The Triglyceride and Glucose Index Is a Predictor of Incident Nonalcoholic Fatty Liver Disease: A Population-Based Cohort Study. Can. J. Gastroenterol. Hepatol. 2019, 2019, 5121574. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Shao, Z.; Shen, G. Association between Triglyceride Glucose-Related Markers and the Risk of Metabolic-Associated Fatty Liver Disease: A Cross-Sectional Study in Healthy Chinese Participants. BMJ Open 2023, 13, e070189. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Chang, M.; Shen, P.; Wei, W.; Li, H.; Shen, G. Application Value of Triglyceride-Glucose Index and Triglyceride-Glucose Body Mass Index in Evaluating the Degree of Hepatic Steatosis in Non-Alcoholic Fatty Liver Disease. Lipids Health Dis. 2023, 22, 186. [Google Scholar] [CrossRef]
- Li, N.; Tan, H.; Xie, A.; Li, C.; Fu, X.; Xang, W.; Kirim, A.; Huang, X. Value of the Triglyceride Glucose Index Combined with Body Mass Index in Identifying Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes. BMC Endocr. Disord. 2022, 22, 101. [Google Scholar] [CrossRef]
- Lim, J.; Kim, J.; Koo, S.H.; Kwon, G.C. Comparison of Triglyceride Glucose Index, and Related Parameters to Predict Insulin Resistance in Korean Adults: An Analysis of the 2007–2010 Korean National Health and Nutrition Examination Survey. PLoS ONE 2019, 14, e0212963. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Son, D.H.; Baik, S.J.; Cho, W.J.; Lee, Y.J. Triglyceride Glucose-Waist Circumference (TyG-WC) Is a Reliable Marker to Predict Non-Alcoholic Fatty Liver Disease. Biomedicines 2022, 10, 2251. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Feng, L.; Ding, J.; Zhou, W.; Yuan, T.; Mao, J. Triglyceride Glucose-Waist Circumference: The Optimum Index to Screen Nonalcoholic Fatty Liver Disease in Non-Obese Adults. BMC Gastroenterol. 2023, 23, 376. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Huang, X.; Qian, Y.; Sun, T. A Non-Linear Relationship between Triglyceride Glucose Waist Circumference and Nonalcoholic Fatty Liver Disease in a Japanese Population: A Secondary Analysis. Front. Endocrinol. 2023, 14, 1188214. [Google Scholar] [CrossRef] [PubMed]
- Castera, L.; Yuen Chan, H.L.; Arrese, M.; Afdhal, N.; Bedossa, P.; Friedrich-Rust, M.; Han, K.H.; Pinzani, M. EASL-ALEH Clinical Practice Guidelines: Non-Invasive Tests for Evaluation of Liver Disease Severity and Prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar]
- Lim, J.K.; Flamm, S.L.; Singh, S.; Falck-Ytter, Y.T.; Gerson, L.; Hirano, I.; Nguyen, G.C.; Rubenstein, J.H.; Smalley, W.E.; Stollman, N.; et al. American Gastroenterological Association Institute Guideline on the Role of Elastography in the Evaluation of Liver Fibrosis. Gastroenterology 2017, 152, 1536–1543. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | General (n = 855) | DM (n = 54) | Overweight/Obesity (n = 505) |
|---|---|---|---|
| %(n)/M [IQR] | %(n)/M [IQR] | %(n)/M [IQR] | |
| Male | 61.1 (522) | 63 (34) | 69.1 (349) |
| Age (years) | 48 (44–54) | 54 (49–61) | 49 (44–54) |
| BMI (kg/m2) | 25.7 [23.4–28.1] | 27.6 [25.3–30.9] | 27.5 [26.1–29.7] |
| DM | 6.3 (54) | - | 8.9 (45) |
| Hypertension | 35.1 (300) | 48.1 (26) | 44 (222) |
| Dyslipidemia | 38.7 (331) | 26.9 (16) | 39.2 (198) |
| Smoking | 20 (171) | 16.7 (1) | 21 (106) |
| WC (cm) | 92 (85–98) | 98 (91–106) | 97 (92–103) |
| Fasting glucose (mg/dL) | 90 (85–96) | 111.5 (91–136) | 91 (87–98) |
| Triglycerides (mg/dL) | 112 (80–159) | 116 [90.5–173.2] | 126 [94.5–181.5] |
| Cholesterol (mg/dL) | 208 (180–235) | 194.5 (157–225) | 208 (179–234) |
| HDL (mg/dL) | 53 (42–74) | 46.5 (41–81) | 49 (39–68) |
| LDL (mg/dL) | 131 (107–157) | 115 [88.7–144.7] | 131 (109–155) |
| HbA1c (%) | 5.3 [5.1–5.5] | 6.3 [5.5–7.3] | 5.4 [5.2–5.7] |
| AST (IU/L) | 26 (20–35) | 25 (21–38) | 28 (22–40) |
| ALT (IU/L) | 23 (20–28) | 24 (19–29) | 24 (21–30) |
| GGT (IU/L) | 21 (15–30) | 21 (14–32) | 24 (18–33) |
| dB | 243 (213–282) | 272 (243–309) | 264 (238–302) |
| kPa | 3.9 [3.3–4.6] | 4.2 [3.6–4.7] | 4.1 [3.4–4.6] |
| LS by CAP | 31.8 (272) | 53.7 (29) | 46.3 (234) |
| FLI | 37 (18–62) | 59.5 [28.7–79.5] | 55 (37–76) |
| LS by FLI | 27.4 (234) | 50 (27) | 45.1 (228) |
| HSI | 40 (43–47) | 42.4 [39.8–46.8] | 43 [40.5–46] |
| LS by HSI | 82.8 (708) | 96.3 (52) | 98.6 (498) |
| TyG | 4.6 [4.4–4.8] | 4.7 [4.5–5.03] | 4.6 [4.5–4.8] |
| TyG-BMI | 118.5 [106.1–133.5] | 133.8 [119.7–154.2] | 129.9 [12.5–142.5] |
| TyG-WC | 425.9 [384.6–467.8] | 470.3 [427.4–508.7] | 453.2 [424–495.3] |
| Index | Cut-Off | AUC | Sensitivity (CI 95%) | Specificity (CI 95%) | PPV | NPV | LR+ (CI 95%) | LR− (CI 95%) |
|---|---|---|---|---|---|---|---|---|
| CAP | ||||||||
| TyG | 4.61 | 0.72 | 0.72 (0.67–0.77) | 0.60 (0.54–0.66) | 0.46 | 0.82 | 1.83 (1.61–2.07) | 0.46 (0.37–0.56) |
| TyG-BMI | 118.2 | 0.82 | 0.82 (0.77–0.87) | 0.63 (0.57–0.69) | 0.51 | 0.88 | 2.26 (2.01–2.55) | 0.27 (0.21–0.36) |
| TyG-WC | 425.6 | 0.81 | 0.81 (0.76–0.86) | 0.64 (0.58–0.70) | 0.51 | 0.88 | 2.29 (2.02–2.59) | 0.29 (0.22–0.37) |
| FLI | ||||||||
| TyG | 4.6 | 0.84 | 0.85 (0.80–0.90) | 0.63 (0.57–0.69) | 0.46 | 0.92 | 2.35 (2.09–2.64) | 0.22 (0.16–0.31) |
| TyG-BMI | 124.12 | 0.96 | 0.96 (0.93–0.99) | 0.80 (0.75–0.85) | 0.65 | 0.98 | 5.02 (4.26–5.91) | 0.05 (0.03–0.09) |
| TyG-WC | 444.17 | 0.96 | 0.97 (0.95–0.99) | 0.86 (0.82–0.90) | 0.73 | 0.98 | 7.26 (5.93–8.88) | 0.03 (0.02–0.07) |
| HSI | ||||||||
| TyG | 4.4 | 0.74 | 0.74 (0.71–0.77) | 0.59 (0.55–0.63) | 0.89 | 0.33 | 1.87 (1.52–2.28) | 0.42 (0.35–0.50) |
| TyG-BMI | 101.38 | 0.93 | 0.93 (0.91–0.95) | 0.69 (0.66–0.72) | 0.93 | 0.70 | 3.07 (2.40–3.92) | 0.09 (0.06–0.12) |
| TyG-WC | 377.7 | 0.85 | 0.85 (0.82–0.88) | 0.61 (0.57–0.65) | 0.91 | 0.47 | 2.25 (1.83–2.78) | 0.23 (0.18–0.28) |
| Index | Cut-Off | AUC | Sensitivity (CI 95%) | Specificity (CI 95%) | PPV | NPV | LR+ (CI 95%) | LR− (CI 95%) |
|---|---|---|---|---|---|---|---|---|
| CAP | ||||||||
| TyG | 4.7 | 0.634 | 0.65 (0.48–0.82) | 0.60 (0.42–0.78) | 0.34 | 0.40 | 1.64 (0.95–2.83) | 0.57 (0.32–1.04) |
| TyG-BMI | 132.2 | 0.683 | 0.69 (0.52–0.86) | 0.36 (0.19–0.53) | 0.44 | 0.50 | 1.08 (0.75–1.58) | 0.86 (0.41–1.83) |
| TyG-WC | 455.5 | 0.708 | 0.72 (0.56–0.88) | 0.60 (0.42–0.78) | 0.32 | 0.34 | 1.81 (1.07–3.08) | 0.46 (0.24–0.90) |
| FLI | ||||||||
| TyG | 4.6 | 0.771 | 0.85 (0.72–0.98) | 0.44 (0.25–0.63) | 0.39 | 0.25 | 1.53 (1.06–2.22) | 0.33 (0.12–0.90) |
| TyG-BMI | 124.6 | 0.975 | 0.96 (0.89–1.03) | 0.63 (0.45–0.81) | 0.27 | 0.05 | 2.60 (1.58–4.28) | 0.06 (0.01–0.41) |
| TyG-WC | 451.3 | 0.966 | 0.96 (0.89–1.03) | 0.74 (0.57–0.91) | 0.21 | 0.04 | 3.71 (1.95–7.96) | 0.05 (0.01–0.35) |
| HSI | ||||||||
| TyG | - | - | - | - | - | - | - | - |
| TyG-BMI | 98.3 | 0.990 | 0.98 (0.94–1.02) | 0.50 (0.36–0.64) | 0.01 | 0.05 | 1.96 (0.49–7.85) | 0.04 (0.0–0.42) |
| TyG-WC | 372.6 | 0.952 | 0.94 (0.88–1.00) | 0.50 (0.36–0.64) | 0.02 | 0.75 | 1.88 (0.47–7.55) | 0.12 (0.02–0.68) |
| Index | Cut-Off | AUC | Sensitivity (CI 95%) | Specificity (CI 95%) | PPV | NPV | LR+ (CI 95%) | LR− (CI 95%) |
|---|---|---|---|---|---|---|---|---|
| CAP | ||||||||
| TyG | 4.6 | 0.674 | 0.74 (0.68–0.80) | 0.50 (0.44–0.56) | 0.43 | 0.30 | 1.49 (1.30–1.72) | 0.51 (0.40–0.65) |
| TyG-BMI | 128.1 | 0.756 | 0.76 (0.71–0.81) | 0.62 (0.56–0.68) | 0.36 | 0.24 | 2.02 (1.71–2.39) | 0.38 (0.30–0.49) |
| TyG-WC | 446.3 | 0.740 | 0.74 (0.68–0.80) | 0.60 (0.54–0.66) | 0.37 | 0.26 | 1.90 (1.61–2.25) | 0.42 (0.33–0.53) |
| FLI | ||||||||
| TyG | 4.6 | 0.827 | 0.85 (0.80–0.90) | 0.58 (0.52–0.64) | 0.36 | 0.16 | 2.08 (1.79–2.42) | 0.25 (0.18–0.34) |
| TyG-BMI | 127.8 | 0.929 | 0.93 (0.90–0.96) | 0.73 (0.67–0.79) | 0.25 | 0.06 | 3.54 (2.90–4.33) | 0.09 (0.05–0.15) |
| TyG-WC | 446.3 | 0.950 | 0.95 (0.92–0.98) | 0.77 (0.72–0.82) | 0.22 | 0.04 | 4.18 (3.36–5.21) | 0.06 (0.03–0.11) |
| HSI | ||||||||
| TyG | 4.5 | 0.695 | 0.76 (0.72–0.80) | 0.42 (0.38–0.46) | 0.01 | 0.97 | 1.34 (0.71–2.55) | 0.54 (0.23–1.30) |
| TyG-BMI | 115.6 | 0.884 | 0.88 (0.85–0.91) | 0.57 (0.53–0.61) | 0.006 | 0.93 | 2.07 (0.88–4.86) | 0.20 (0.10–0.40) |
| TyG-WC | - | - | - | - | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mijangos-Trejo, A.; Gómez-Mendoza, R.; Ramos-Ostos, M.H.; Castro-Narro, G.; Uribe, M.; Juárez-Hernández, E.; López-Méndez, I. Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection. Diagnostics 2024, 14, 762. https://doi.org/10.3390/diagnostics14070762
Mijangos-Trejo A, Gómez-Mendoza R, Ramos-Ostos MH, Castro-Narro G, Uribe M, Juárez-Hernández E, López-Méndez I. Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection. Diagnostics. 2024; 14(7):762. https://doi.org/10.3390/diagnostics14070762
Chicago/Turabian StyleMijangos-Trejo, Alejandra, Raúl Gómez-Mendoza, Martha Helena Ramos-Ostos, Graciela Castro-Narro, Misael Uribe, Eva Juárez-Hernández, and Iván López-Méndez. 2024. "Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection" Diagnostics 14, no. 7: 762. https://doi.org/10.3390/diagnostics14070762
APA StyleMijangos-Trejo, A., Gómez-Mendoza, R., Ramos-Ostos, M. H., Castro-Narro, G., Uribe, M., Juárez-Hernández, E., & López-Méndez, I. (2024). Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection. Diagnostics, 14(7), 762. https://doi.org/10.3390/diagnostics14070762