
Can Plasma Volume Determination in Cirrhosis Be Replaced by an Algorithm Using Body Weight and Hematocrit?

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
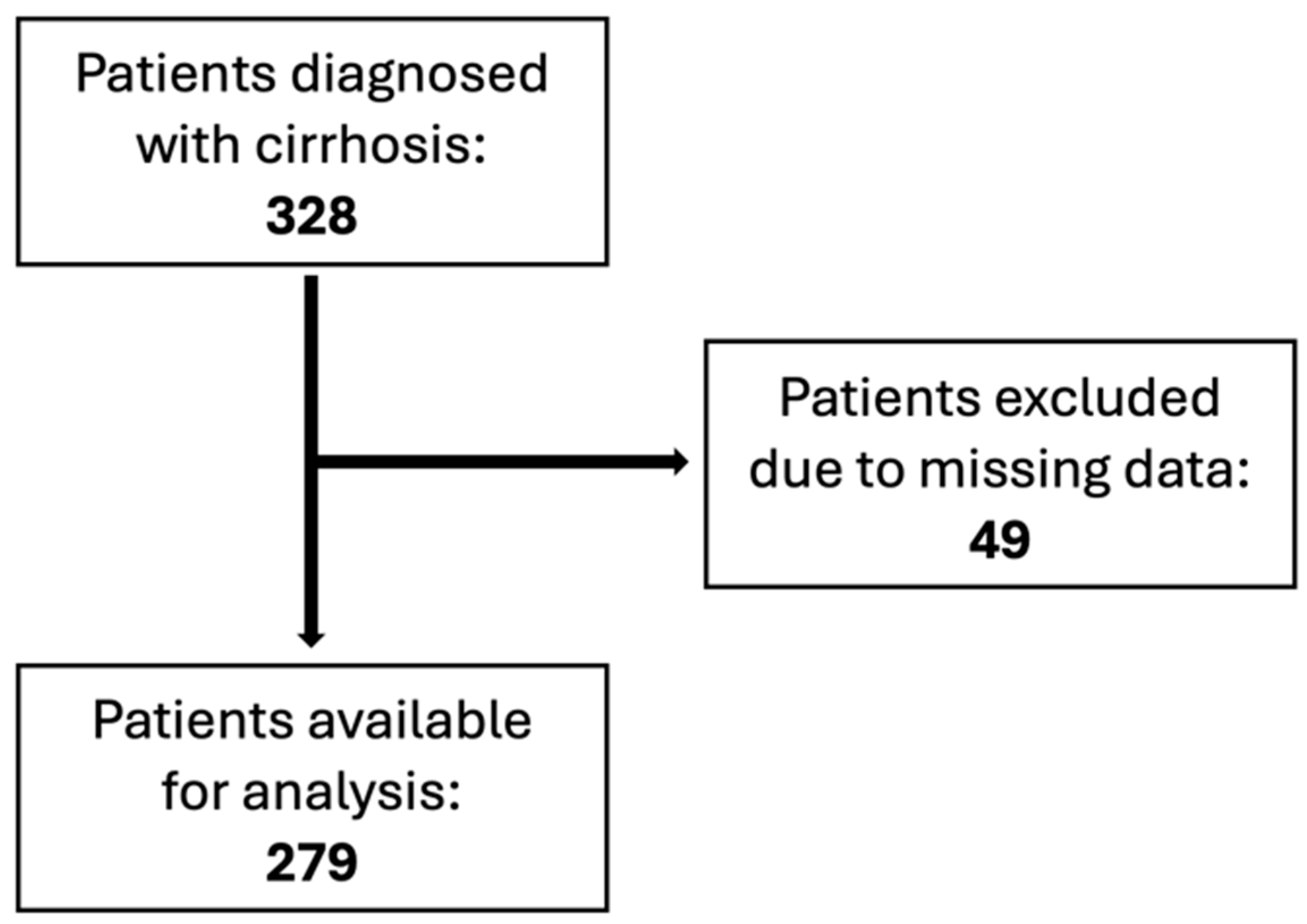
2.1. Study Population
2.2. Liver Vein Catheterization
2.3. Plasma Volume Measurement
2.4. Plasma Volume Equations
2.5. Statistics
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karlsen, T.H.; Sheron, N.; Zelber-Sagi, S.; Carrieri, P.; Dusheiko, G.; Bugianesi, E.; Pryke, R.; Hutchinson, S.J.; Sangro, B.; Martin, N.K.; et al. The EASL–Lancet Liver Commission: Protecting the next Generation of Europeans against Liver Disease Complications and Premature Mortality. Lancet 2022, 399, 61–116. [Google Scholar] [CrossRef] [PubMed]
- Ginès, P.; Krag, A.; Abraldes, J.G.; Solà, E.; Fabrellas, N.; Kamath, P.S. Liver Cirrhosis. Lancet 2021, 398, 1359–1376. [Google Scholar] [CrossRef]
- Loomba, R.; Wong, R.; Fraysse, J.; Shreay, S.; Li, S.; Harrison, S.; Gordon, S.C. Nonalcoholic Fatty Liver Disease Progression Rates to Cirrhosis and Progression of Cirrhosis to Decompensation and Mortality: A Real World Analysis of Medicare Data. Aliment. Pharmacol. Ther. 2020, 51, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Cheemerla, S.; Balakrishnan, M. Global Epidemiology of Chronic Liver Disease. Clin. Liver Dis. 2021, 17, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Teng, M.L.; Ng, C.H.; Huang, D.Q.; Chan, K.E.; Tan, D.J.; Lim, W.H.; Yang, J.D.; Tan, E.; Muthiah, M.D. Global Incidence and Prevalence of Nonalcoholic Fatty Liver Disease. Clin. Mol. Hepatol. 2023, 29, S32–S42. [Google Scholar] [CrossRef]
- Lonardo, A.; Mantovani, A.; Lugari, S.; Targher, G. Epidemiology and Pathophysiology of the Association between NAFLD and Metabolically Healthy or Metabolically Unhealthy Obesity. Ann. Hepatol. 2020, 19, 359–366. [Google Scholar] [CrossRef] [PubMed]
- O’Beirne, J.; Skoien, R.; Leggett, B.A.; Hartel, G.F.; Gordon, L.G.; Powell, E.E.; Valery, P.C. Diabetes Mellitus and the Progression of Non-alcoholic Fatty Liver Disease to Decompensated Cirrhosis: A Retrospective Cohort Study. Med. J. Aust. 2023, 219, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Laursen, T.L.; Hagemann, C.A.; Wei, C.; Kazankov, K.; Thomsen, K.L.; Knop, F.K.; Grønbæk, H. Bariatric Surgery in Patients with Non-Alcoholic Fatty Liver Disease—From Pathophysiology to Clinical Effects. World J. Hepatol. 2019, 11, 138–149. [Google Scholar] [CrossRef]
- Tacke, F.; Weiskirchen, R. Non-Alcoholic Fatty Liver Disease (NAFLD)/Non-Alcoholic Steatohepatitis (NASH)-Related Liver Fibrosis: Mechanisms, Treatment and Prevention. Ann. Transl. Med. 2021, 9, 729. [Google Scholar] [CrossRef]
- Ginès, P.; Fernández, J.; Durand, F.; Saliba, F. Management of Critically-Ill Cirrhotic Patients. J. Hepatol. 2012, 56, S13–S24. [Google Scholar] [CrossRef]
- Pugh, R.N.H.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the Oesophagus for Bleeding Oesophageal Varices. Br. J. Surg. 2005, 60, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Child, C.G.; Turcotte, J.G. Surgery and Portal Hypertension. Major Probl. Clin. Surg. 1964, 1, 1–85. [Google Scholar] [PubMed]
- Engelmann, C.; Clària, J.; Szabo, G.; Bosch, J.; Bernardi, M. Pathophysiology of Decompensated Cirrhosis: Portal Hypertension, Circulatory Dysfunction, Inflammation, Metabolism and Mitochondrial Dysfunction. J. Hepatol. 2021, 75, S49–S66. [Google Scholar] [CrossRef] [PubMed]
- Jindal, A.; Bhardwaj, A.; Kumar, G.; Sarin, S.K. Clinical Decompensation and Outcomes in Patients with Compensated Cirrhosis and a Hepatic Venous Pressure Gradient ≥20 Mm Hg. Am. J. Gastroenterol. 2020, 115, 1624–1633. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Bernardi, M.; Angeli, P. Towards a New Definition of Decompensated Cirrhosis. J. Hepatol. 2022, 76, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Angeli, P.; Moreau, R.; Jalan, R.; Clària, J.; Trebicka, J.; Fernández, J.; Gustot, T.; Caraceni, P.; Bernardi, M.; et al. The Systemic Inflammation Hypothesis: Towards a New Paradigm of Acute Decompensation and Multiorgan Failure in Cirrhosis. J. Hepatol. 2021, 74, 670–685. [Google Scholar] [CrossRef] [PubMed]
- Simbrunner, B.; Caparrós, E.; Neuwirth, T.; Schwabl, P.; Königshofer, P.; Bauer, D.; Marculescu, R.; Trauner, M.; Scheiner, B.; Stary, G.; et al. Bacterial Translocation Occurs Early in Cirrhosis and Triggers a Selective Inflammatory Response. Hepatol. Int. 2023, 17, 1045–1056. [Google Scholar] [CrossRef]
- Simbrunner, B.; Villesen, I.F.; Königshofer, P.; Scheiner, B.; Bauer, D.; Paternostro, R.; Schwabl, P.; Timelthaler, G.; Ramazanova, D.; Wöran, K.; et al. Systemic Inflammation Is Linked to Liver Fibrogenesis in Patients with Advanced Chronic Liver Disease. Liver Int. Off. J. Int. Assoc. Study Liver 2022, 42, 2501–2512. [Google Scholar] [CrossRef] [PubMed]
- Jalan, R.; D’Amico, G.; Trebicka, J.; Moreau, R.; Angeli, P.; Arroyo, V. New Clinical and Pathophysiological Perspectives Defining the Trajectory of Cirrhosis. J. Hepatol. 2021, 75 (Suppl. S1), S14–S26. [Google Scholar] [CrossRef]
- Kim, M.Y.; Baik, S.K.; Lee, S.S. Hemodynamic Alterations in Cirrhosis and Portal Hypertension. Korean J. Hepatol. 2010, 16, 347–352. [Google Scholar] [CrossRef]
- Ripoll, C.; Ibáñez-Samaniego, L.; Neumann, B.; Vaquero, J.; Greinert, R.; Bañares, R.; Zipprich, A. Evaluation of the Definition of Hyperdynamic Circulation in Patients with Cirrhosis and Ascites. Hepatol. Commun. 2022, 6, 3528–3538. [Google Scholar] [CrossRef] [PubMed]
- Bolognesi, M.; Di Pascoli, M.; Verardo, A.; Gatta, A. Splanchnic Vasodilation and Hyperdynamic Circulatory Syndrome in Cirrhosis. World J. Gastroenterol. 2014, 20, 2555–2563. [Google Scholar] [CrossRef]
- Jepsen, P.; Lash, T.L.; Vilstrup, H. The Clinical Course of Alcoholic Cirrhosis: Development of Comorbid Diseases. A Danish Nationwide Cohort Study. Liver Int. 2016, 36, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Merkel, C.; Bolognesi, M.; Finucci, G.F.; Angeli, P.; Caregaro, L.; Rondana, M.; Gatta, A. Indocyanine Green Intrinsic Hepatic Clearance as a Prognostic Index of Survival in Patients with Cirrhosis. J. Hepatol. 1989, 9, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Schrier, R.W.; Berl, T.; Anderson, R.J. Osmotic and Nonosmotic Control of Vasopressin Release. Am. J. Physiol. 1979, 236, F321–F332. [Google Scholar] [CrossRef] [PubMed]
- Sansoè, G.; Aragno, M.; Wong, F. Pathways of Hepatic and Renal Damage through Non-Classical Activation of the Renin-Angiotensin System in Chronic Liver Disease. Liver Int. 2020, 40, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Recommended Methods for Measurement of Red-Cell and Plasma Volume: International Committee for Standardization in Haematology. J. Nucl. Med. 1980, 21, 793–800.
- Ling, H.Z.; Flint, J.; Damgaard, M.; Bonfils, P.K.; Cheng, A.S.; Aggarwal, S.; Velmurugan, S.; Mendonca, M.; Rashid, M.; Kang, S.; et al. Calculated Plasma Volume Status and Prognosis in Chronic Heart Failure. Eur. J. Heart Fail. 2015, 17, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Daugirdas, J.T.; Blake, P.G.; Ing, T.S. (Eds.) Handbook of Dialysis, 3rd ed.; A Lippincott Williams & Wilkins Handbook; Lippincott, Williams & Wilkins: Philadelphia, PA, USA, 2001; ISBN 978-0-316-17381-0. [Google Scholar]
- Longo, D.L. (Ed.) Harrison’s Principles of Internal Medicine, 18th ed.; McGraw-Hill: New York, NY, USA, 2012; ISBN 978-0-07-174889-6. [Google Scholar]
- Yoshihisa, A.; Abe, S.; Sato, Y.; Watanabe, S.; Yokokawa, T.; Miura, S.; Misaka, T.; Sato, T.; Suzuki, S.; Oikawa, M.; et al. Plasma Volume Status Predicts Prognosis in Patients with Acute Heart Failure Syndromes. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 330–338. [Google Scholar] [CrossRef]
- Fudim, M.; Miller, W.L. Calculated Estimates of Plasma Volume in Patients with Chronic Heart Failure—Comparison with Measured Volumes. J. Card. Fail. 2018, 24, 553–560. [Google Scholar] [CrossRef]
- Lu, Q.; Leong, S.; Lee, K.A.; Patel, A.; Chua, J.M.E.; Venkatanarasimha, N.; Lo, R.H.; Irani, F.G.; Zhuang, K.D.; Gogna, A.; et al. Hepatic Venous-Portal Gradient (HVPG) Measurement: Pearls and Pitfalls. Br. J. Radiol. 2021, 94, 20210061. [Google Scholar] [CrossRef] [PubMed]
- Christensen, T.N.; Mortensen, C.; Henriksen, J.H.; Møller, S. Different Injection Techniques in the Assessment of Central Haemodynamics in Patients with Cirrhosis. Scand. J. Clin. Lab. Investig. 2013, 73, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Møller, S.; Bendtsen, F.; Henriksen, J.H. Splanchnic and Systemic Hemodynamic Derangement in Decompensated Cirrhosis. Can. J. Gastroenterol. J. Can. Gastroenterol. 2001, 15, 94–106. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Møller, S.; Henriksen, J.H.; Bendtsen, F. Central and Noncentral Blood Volumes in Cirrhosis: Relationship to Anthropometrics and Gender. Am. J. Physiol.-Gastrointest. Liver Physiol. 2003, 284, G970–G979. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, U.L.; Henriksen, J.H.; Bendtsen, F.; Møller, S. 99mTc-Labelled Human Serum Albumin Cannot Replace 125I-Labelled Human Serum Albumin to Determine Plasma Volume in Patients with Liver Disease. Clin. Physiol. Funct. Imaging 2013, 33, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Bonfils, P.K.; Damgaard, M.; Stokholm, K.H.; Nielsen, S.L. 99mTc-Albumin Can Replace 125I-Albumin to Determine Plasma Volume Repeatedly. Scand. J. Clin. Lab. Investig. 2012, 72, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.; Hopper, J.; Hodges, J.L.; Bradley, B.; Wennesland, R.; Yamauchi, H. Red Cell, Plasma, and Blood Volume in the Healthy Women Measured by Radiochromium Cell-Labeling and Hematocrit. J. Clin. Investig. 1962, 41, 2182–2190. [Google Scholar] [CrossRef] [PubMed]
- Wennesland, R.; Brown, E.; Hopper, J.; Hodges, J.L.; Guttentag, O.E.; Scott, K.G.; Tucker, I.N.; Bradley, B. Red Cell, Plasma and Blood Volume in Healthy Men Measured by Radiochromium (Cr51) Cell Tagging and Hematocrit: Influence of Age, Somatotype and Habits of Physical Activity on the Variance after Regression of Volumes to Height and Weight Combined. J. Clin. Investig. 1959, 38, 1065–1077. [Google Scholar] [CrossRef] [PubMed]
- Niedermeyer, S.E.; Stephens, R.S.; Kim, B.S.; Metkus, T.S. Calculated Plasma Volume Status Is Associated with Mortality in Acute Respiratory Distress Syndrome. Crit. Care Explor. 2021, 3, e0534. [Google Scholar] [CrossRef]
- Maznyczka, A.M.; Barakat, M.F.; Ussen, B.; Kaura, A.; Abu-Own, H.; Jouhra, F.; Jaumdally, H.; Amin-Youssef, G.; Nicou, N.; Baghai, M.; et al. Calculated Plasma Volume Status and Outcomes in Patients Undergoing Coronary Bypass Graft Surgery. Heart 2019, 105, 1020–1026. [Google Scholar] [CrossRef]
- Duarte, K.; Monnez, J.-M.; Albuisson, E.; Pitt, B.; Zannad, F.; Rossignol, P. Prognostic Value of Estimated Plasma Volume in Heart Failure. JACC Heart Fail. 2015, 3, 886–893. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics | |
|---|---|
| Age (years) | 58 (9.4) |
| Height (cm) | 173 (8.5) |
| Body weight (kg) | 77 (16.5) |
| Gender (M/F) | 206/73 |
| Body mass index (Kg/m2) | 25.2 (4.8) |
| Ascites (+/−) | 141/137 [1] |
| Esophageal varice (+/−) | 75/173 [31] |
| Coma (+/−) | 3/275 [1] |
| Biochemistry | |
| Blood hemoglobin (mmol/L) | 7.5 (1.2) |
| Serum creatinine (μmol/L) | 77.5 (27.9) |
| Serum sodium (mmol/L) | 136.6 (4.6) |
| Serum Albumin (g/L) | 32 (6.1) [3] |
| Serum Bilirubin (μmol/L9) | 23.8 (23.2) [2] |
| Plasma coagulation factors 2, 7, 10 (U) | 0.62 (0.21) [2] |
| Platelets | 169 (96) [3] |
| ALAT | 38.7 (33.5) [3] |
| INR | 1.3 (0.27) [1] |
| Hemodynamics | |
| Hepatic venous pressure gradient (mmHg) | 14.4 (5.9) [3] |
| Mean arterial pressure (mmHg) | 91.5 (14.5) |
| Heart rate (bpm) | 74.6 (14.2) |
| The curse of liver cirrhosis stated as the number and (%) | |
| Alcohol | 209 (74.9) |
| Alcohol + Hepatitis | 3 (1.1) |
| Alpha 1-antitrypsin deficiency | 3 (1.1) |
| Autoimmune hepatitis | 4 (1.4) |
| Hepatitis B | 7 (2.5) |
| Hepatitis C | 16 (5.7) |
| Hepatitis B, C, and HIV | 1 (0.4) |
| Granulomatous hepatitis | 1 (0.4) |
| Hemochromatosis | 1 (0.4) |
| Cryptogenic liver disease | 12 (4.3) |
| NASH | 6 (2.2) |
| Primary biliary cholangitis | 2 (0.7) |
| Portal hypertension | 3 (1.1) |
| Prehepatic portal hypertension | 1 (0.4) |
| Missing data | 10 (3.6) |
| 4 | Mean (SD) | p-Value |
|---|---|---|
| PVa | 3.09 (0.54) | <0.001 |
| PVi | 3.01 (0.65) | <0.001 |
| PVI-125 | 3.99 (1.01) |
| Variable | Mean (SD) | p-Value |
|---|---|---|
| PVa Child–Pugh class A | 3.0 (0.56) | <0.001 |
| PVI-125 Child–Pugh class A | 3.66 (0.95) | |
| PVa Child–Pugh class B | 3.0 (0.54) | <0.001 |
| PVI-125 Child–Pugh class B | 3.94 (0.88) | |
| PVa Child–Pugh class C | 3.26 (0.47) | <0.001 |
| PVI-125 Child–Pugh class C | 4.41 (1.04) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nørskov, M.P.; Mønsted, T.; Kimer, N.; Damgaard, M.; Møller, S. Can Plasma Volume Determination in Cirrhosis Be Replaced by an Algorithm Using Body Weight and Hematocrit? Diagnostics 2024, 14, 835. https://doi.org/10.3390/diagnostics14080835
Nørskov MP, Mønsted T, Kimer N, Damgaard M, Møller S. Can Plasma Volume Determination in Cirrhosis Be Replaced by an Algorithm Using Body Weight and Hematocrit? Diagnostics. 2024; 14(8):835. https://doi.org/10.3390/diagnostics14080835
Chicago/Turabian StyleNørskov, Martine Prütz, Thormod Mønsted, Nina Kimer, Morten Damgaard, and Søren Møller. 2024. "Can Plasma Volume Determination in Cirrhosis Be Replaced by an Algorithm Using Body Weight and Hematocrit?" Diagnostics 14, no. 8: 835. https://doi.org/10.3390/diagnostics14080835
APA StyleNørskov, M. P., Mønsted, T., Kimer, N., Damgaard, M., & Møller, S. (2024). Can Plasma Volume Determination in Cirrhosis Be Replaced by an Algorithm Using Body Weight and Hematocrit? Diagnostics, 14(8), 835. https://doi.org/10.3390/diagnostics14080835