
Deep Learning in Breast Cancer Imaging: State of the Art and Recent Advancements in Early 2024

Abstract
:1. Introduction
2. Contribution, Novelty, and Motivation Statement
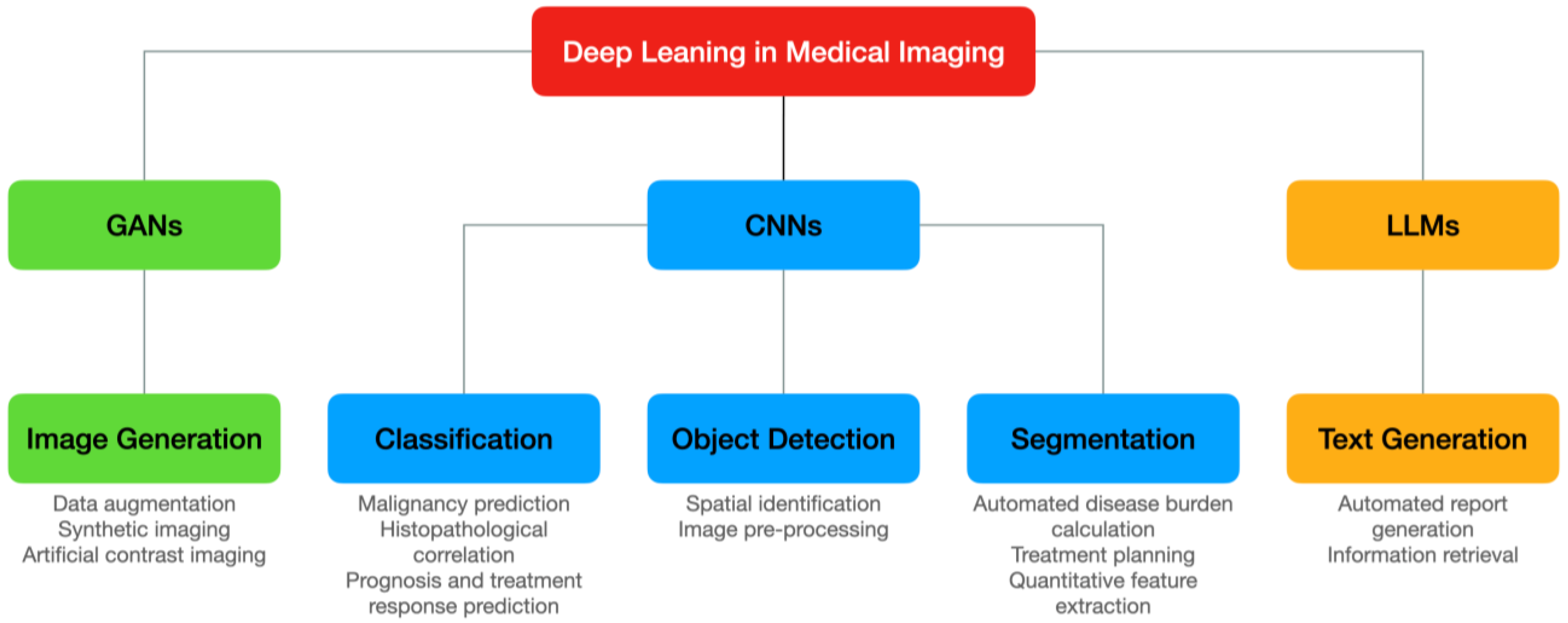
3. Deep Learning in Medical Imaging: Approaches and Techniques
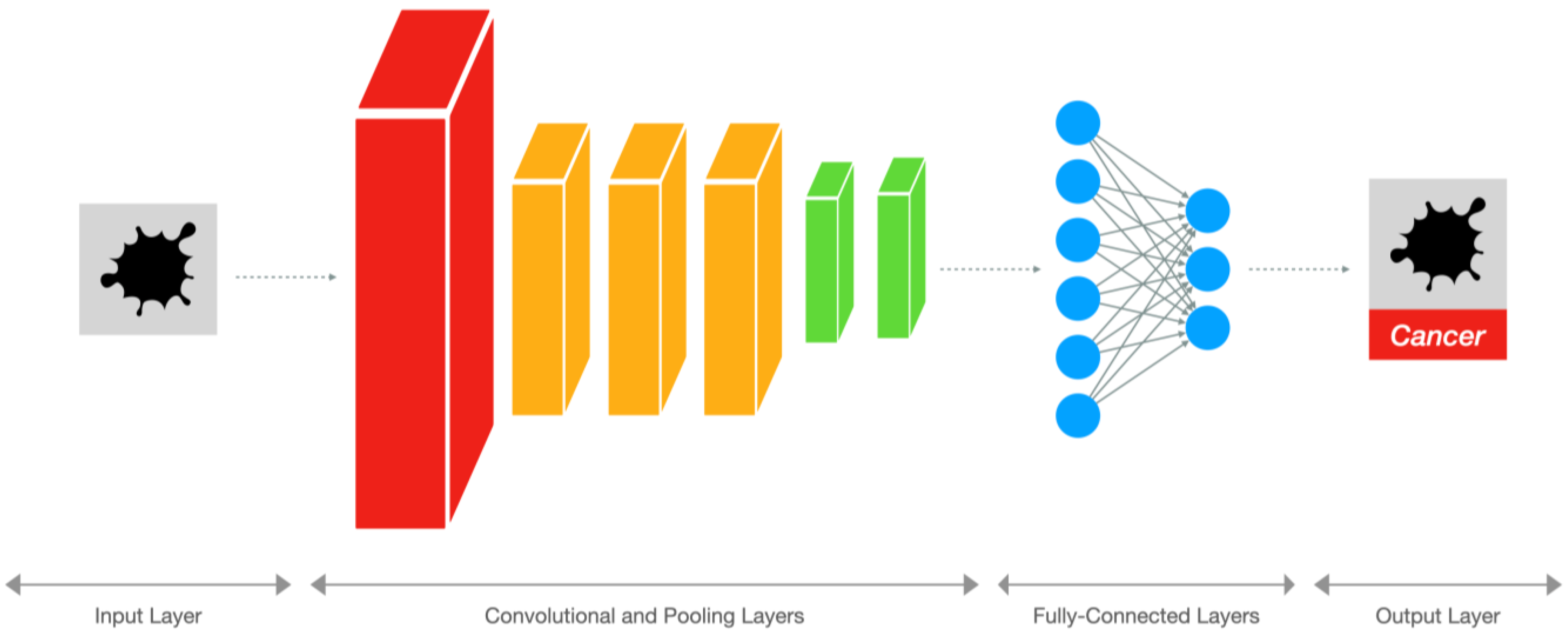
3.1. Convolutional Neural Networks
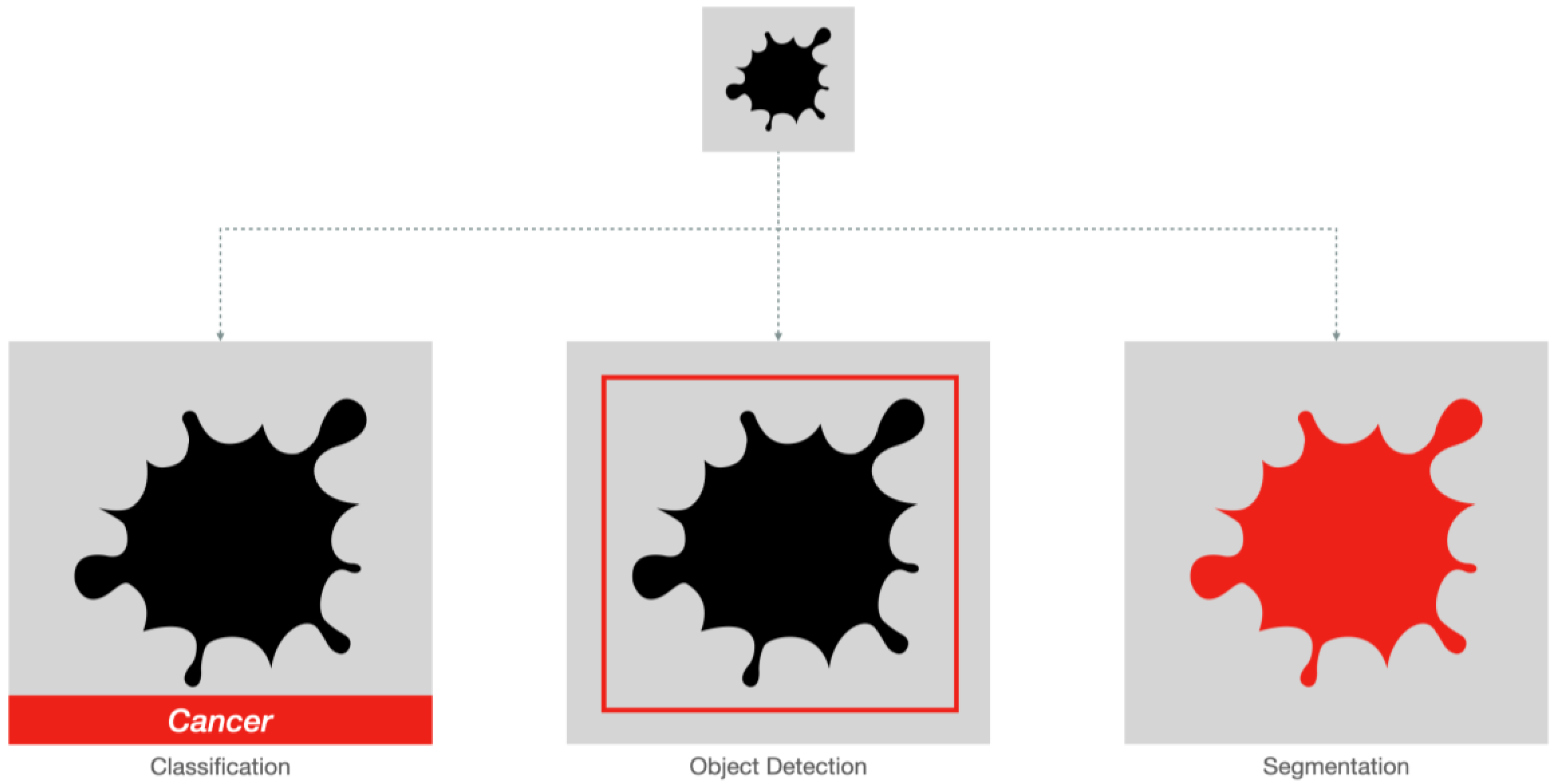
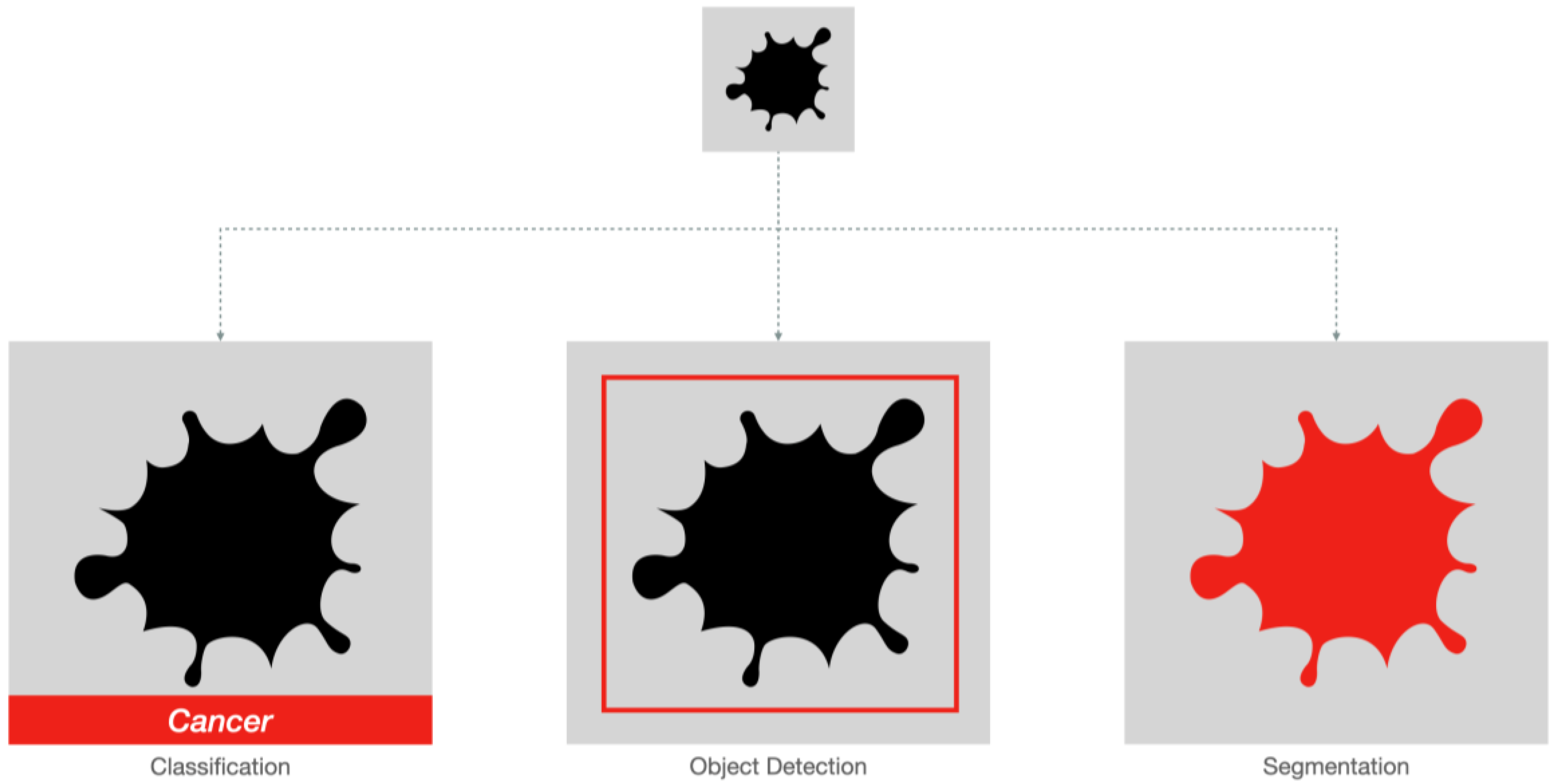
3.1.1. Classification and Object Detection
3.1.2. Segmentation
3.2. Generative Adversarial Networks
3.3. Large Language Models
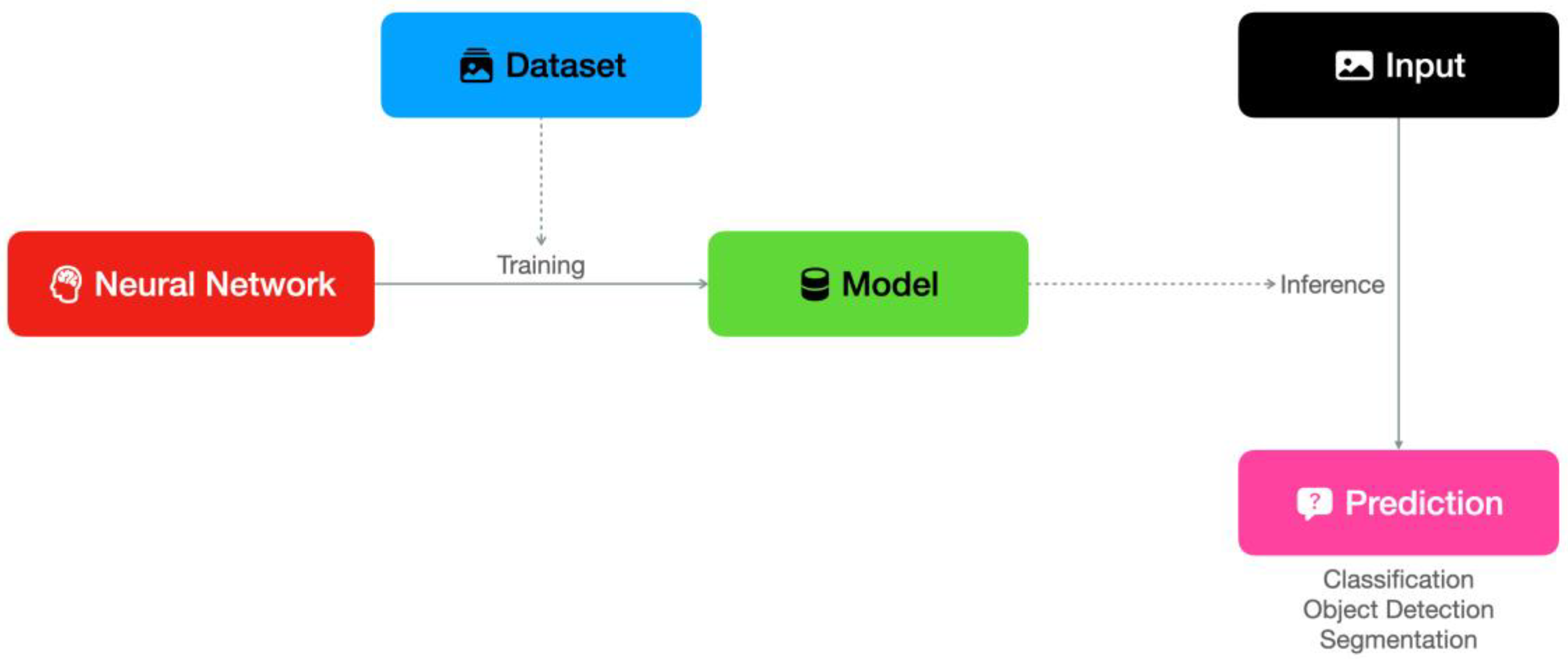
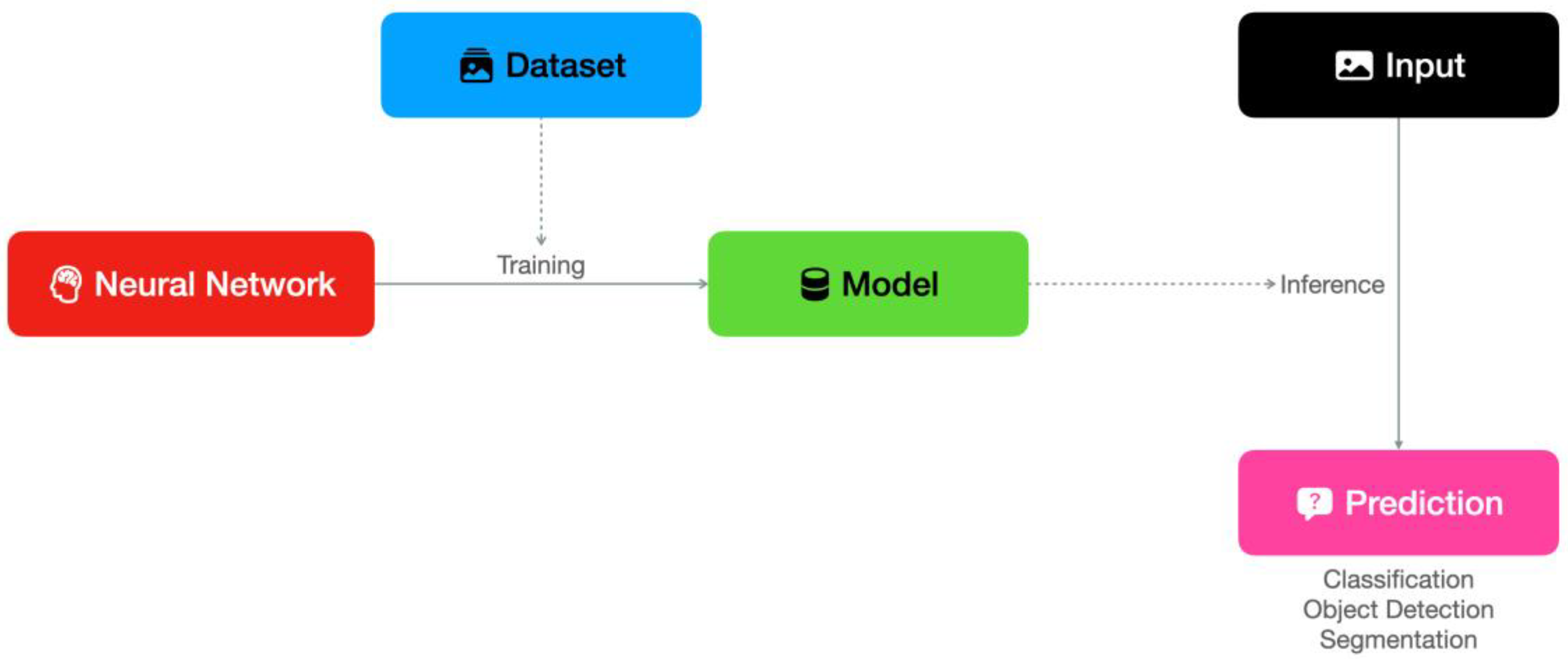
3.4. Technical Considerations: Training, Inference and Deployment
3.5. Performance Metrics for Medical Imaging Deep Learning Models
4. Deep Learning in Breast Cancer Imaging: Datasets
5. Deep Learning in Breast Cancer Imaging: Applications to Conventional Techniques
5.1. Conventional Mammography
5.2. Digital Breast Tomosynthesis
5.3. Contrast-Enhanced Mammography
5.4. Ultrasound
5.5. Magnetic Resonance Imaging
6. Deep Learning in Breast Cancer Imaging: Novel Techniques
6.1. Thermography
6.2. Microwave Breast Imaging
6.3. Other Techniques
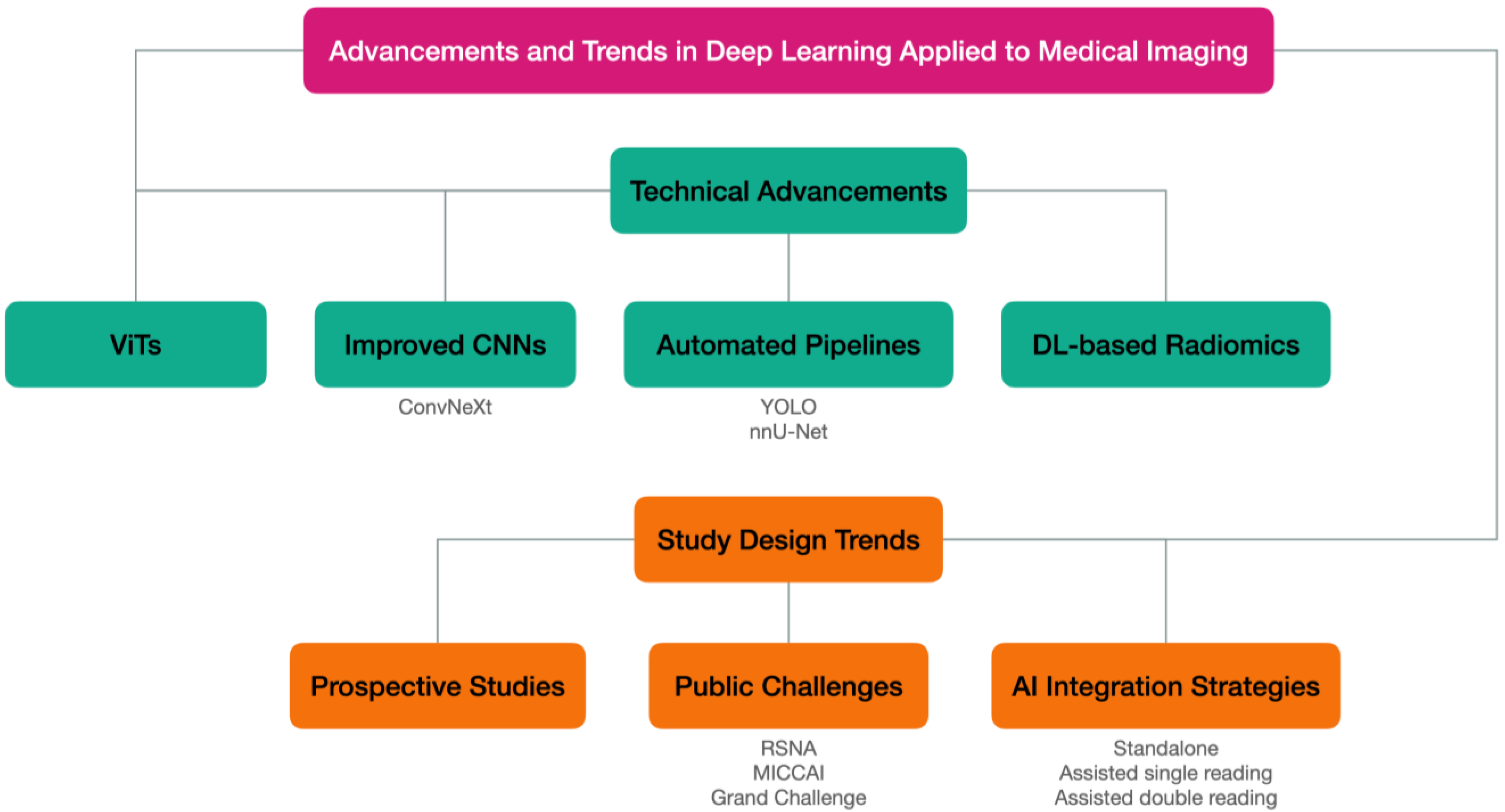
7. Deep Learning in Breast Cancer Imaging: Recent Advancements and Trends
7.1. Technical Advancements
7.1.1. Vision Transformers
7.1.2. Improved Convolutional Neural Networks: ConvNeXt
7.1.3. New Object Detectors: The YOLO Series
7.1.4. Automated Segmentation Pipelines: nnU-Net
7.1.5. Deep Learning-Based Radiomics Classifiers
7.2. Study Design Trends
7.2.1. Prospective versus Retrospective Approach
7.2.2. AI Integration Strategies
7.2.3. Public Challenges
8. Discussion
8.1. State of the Art
8.2. Limitations, Challenges and Future Directions
8.2.1. Generalizability
8.2.2. Multimodal Interpretation
8.2.3. Costs
8.2.4. Privacy
8.2.5. Human–AI Interaction
8.2.6. Explainability, Ethics, and Liability
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Independent UK Panel on Breast Cancer Screening. The Benefits and Harms of Breast Cancer Screening: An Independent Review. Lancet 2012, 380, 1778–1786. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.M.; Cho, N.; Moy, L. Breast MRI: State of the Art. Radiology 2019, 292, 520–536. [Google Scholar] [CrossRef] [PubMed]
- Benchoufi, M.; Matzner-Lober, E.; Molinari, N.; Jannot, A.-S.; Soyer, P. Interobserver Agreement Issues in Radiology. Diagn. Interv. Imaging 2020, 101, 639–641. [Google Scholar] [CrossRef] [PubMed]
- Minaee, S.; Boykov, Y.Y.; Porikli, F.; Plaza, A.J.; Kehtarnavaz, N.; Terzopoulos, D. Image Segmentation Using Deep Learning: A Survey. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 44, 3523–3542. [Google Scholar] [CrossRef]
- Liu, H.; Hu, D.; Li, H.; Oguz, I. Medical Image Segmentation Using Deep Learning. In Machine Learning for Brain Disorders; Colliot, O., Ed.; Neuromethods; Springer: New York, NY, USA, 2023; Volume 197, pp. 391–434. ISBN 978-1-07-163194-2. [Google Scholar]
- Van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in Medical Imaging—“How-to” Guide and Critical Reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- Allen, B.; Agarwal, S.; Coombs, L.; Wald, C.; Dreyer, K. 2020 ACR Data Science Institute Artificial Intelligence Survey. J. Am. Coll. Radiol. 2021, 18, 1153–1159. [Google Scholar] [CrossRef]
- Taylor, C.R.; Monga, N.; Johnson, C.; Hawley, J.R.; Patel, M. Artificial Intelligence Applications in Breast Imaging: Current Status and Future Directions. Diagnostics 2023, 13, 2041. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Wang, X.; Lin, Y.; Ma, X.; Tan, A.; Chan, R.; Vardhanabhuti, V.; Chu, W.C.; Cheng, K.-T.; Chen, H. Deep Learning in Breast Cancer Imaging: A Decade of Progress and Future Directions. arXiv 2023. [Google Scholar] [CrossRef]
- Hinton, G.E.; Osindero, S.; Teh, Y.-W. A Fast Learning Algorithm for Deep Belief Nets. Neural Comput. 2006, 18, 1527–1554. [Google Scholar] [CrossRef]
- Taye, M.M. Understanding of Machine Learning with Deep Learning: Architectures, Workflow, Applications and Future Directions. Computers 2023, 12, 91. [Google Scholar] [CrossRef]
- O’Shea, K.; Nash, R. An Introduction to Convolutional Neural Networks. arXiv 2015. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. arXiv 2015. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; van der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. arXiv 2016. [Google Scholar] [CrossRef]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. MobileNets: Efficient Convolutional Neural Networks for Mobile Vision Applications. arXiv 2017. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q.V. EfficientNet: Rethinking Model Scaling for Convolutional Neural Networks. arXiv 2019. [Google Scholar] [CrossRef]
- Liu, Z.; Mao, H.; Wu, C.-Y.; Feichtenhofer, C.; Darrell, T.; Xie, S. A ConvNet for the 2020s. arXiv 2022. [Google Scholar] [CrossRef]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You Only Look Once: Unified, Real-Time Object Detection. arXiv 2015. [Google Scholar] [CrossRef]
- Girshick, R.; Donahue, J.; Darrell, T.; Malik, J. Rich Feature Hierarchies for Accurate Object Detection and Semantic Segmentation. arXiv 2013. [Google Scholar] [CrossRef]
- Liu, W.; Anguelov, D.; Erhan, D.; Szegedy, C.; Reed, S.; Fu, C.-Y.; Berg, A.C. SSD: Single Shot MultiBox Detector. arXiv 2015. [Google Scholar] [CrossRef]
- Kalmet, P.H.S.; Sanduleanu, S.; Primakov, S.; Wu, G.; Jochems, A.; Refaee, T.; Ibrahim, A.; Hulst, L.V.; Lambin, P.; Poeze, M. Deep Learning in Fracture Detection: A Narrative Review. Acta Orthop. 2020, 91, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, Z.; Dai, C.; Dong, Q.; Badrigilan, S. Accuracy of Deep Learning for Automated Detection of Pneumonia Using Chest X-Ray Images: A Systematic Review and Meta-Analysis. Comput. Biol. Med. 2020, 123, 103898. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Yang, R.; Shen, L.; Feng, A.; Li, L.; He, N.; Li, S.; Huang, L.; Lyu, J. Deep Transfer Learning to Quantify Pleural Effusion Severity in Chest X-Rays. BMC Med. Imaging 2022, 22, 100. [Google Scholar] [CrossRef] [PubMed]
- Gooßen, A.; Deshpande, H.; Harder, T.; Schwab, E.; Baltruschat, I.; Mabotuwana, T.; Cross, N.; Saalbach, A. Deep Learning for Pneumothorax Detection and Localization in Chest Radiographs. arXiv 2019. [Google Scholar] [CrossRef]
- Lee, J.H.; Sun, H.Y.; Park, S.; Kim, H.; Hwang, E.J.; Goo, J.M.; Park, C.M. Performance of a Deep Learning Algorithm Compared with Radiologic Interpretation for Lung Cancer Detection on Chest Radiographs in a Health Screening Population. Radiology 2020, 297, 687–696. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, Y.; Zhang, G.; Qiu, X.; Tan, W.; Yin, X.; Liao, L. Deep Learning With Radiomics for Disease Diagnosis and Treatment: Challenges and Potential. Front. Oncol. 2022, 12, 773840. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Deng, Z.; Yang, Y. Recent Progress in Semantic Image Segmentation. Artif. Intell. Rev. 2019, 52, 1089–1106. [Google Scholar] [CrossRef]
- Krithika Alias AnbuDevi, M.; Suganthi, K. Review of Semantic Segmentation of Medical Images Using Modified Architectures of UNET. Diagnostics 2022, 12, 3064. [Google Scholar] [CrossRef] [PubMed]
- Hafiz, A.M.; Bhat, G.M. A Survey on Instance Segmentation: State of the Art. arXiv 2020. [Google Scholar] [CrossRef]
- Jader, G.; Fontineli, J.; Ruiz, M.; Abdalla, K.; Pithon, M.; Oliveira, L. Deep Instance Segmentation of Teeth in Panoramic X-ray Images. In Proceedings of the 2018 31st SIBGRAPI Conference on Graphics, Patterns and Images (SIBGRAPI), Parana, Brazil, 29 October–1 November 2018; pp. 400–407. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. arXiv 2015. [Google Scholar] [CrossRef]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. nnU-Net: A Self-Configuring Method for Deep Learning-Based Biomedical Image Segmentation. Nat. Methods 2021, 18, 203–211. [Google Scholar] [CrossRef]
- Wasserthal, J.; Breit, H.-C.; Meyer, M.T.; Pradella, M.; Hinck, D.; Sauter, A.W.; Heye, T.; Boll, D.; Cyriac, J.; Yang, S.; et al. TotalSegmentator: Robust Segmentation of 104 Anatomical Structures in CT Images. arXiv 2022. [Google Scholar] [CrossRef]
- Isensee, F.; Jaeger, P.F.; Full, P.M.; Vollmuth, P.; Maier-Hein, K.H. nnU-Net for Brain Tumor Segmentation. arXiv 2020. [Google Scholar] [CrossRef]
- Heller, N.; Isensee, F.; Maier-Hein, K.H.; Hou, X.; Xie, C.; Li, F.; Nan, Y.; Mu, G.; Lin, Z.; Han, M.; et al. The State of the Art in Kidney and Kidney Tumor Segmentation in Contrast-Enhanced CT Imaging: Results of the KiTS19 Challenge. arXiv 2019. [Google Scholar] [CrossRef]
- Goodfellow, I.J.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative Adversarial Networks. arXiv 2014. [Google Scholar] [CrossRef]
- Kebaili, A.; Lapuyade-Lahorgue, J.; Ruan, S. Deep Learning Approaches for Data Augmentation in Medical Imaging: A Review. arXiv 2023. [Google Scholar] [CrossRef] [PubMed]
- Yi, X.; Walia, E.; Babyn, P. Generative Adversarial Network in Medical Imaging: A Review. arXiv 2018. [Google Scholar] [CrossRef]
- Liu, M.; Maiti, P.; Thomopoulos, S.; Zhu, A.; Chai, Y.; Kim, H.; Jahanshad, N. Style Transfer Using Generative Adversarial Networks for Multi-Site MRI Harmonization. In Medical Image Computing and Computer Assisted Intervention—MICCAI 2021; De Bruijne, M., Cattin, P.C., Cotin, S., Padoy, N., Speidel, S., Zheng, Y., Essert, C., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2021; Volume 12903, pp. 313–322. ISBN 978-3-030-87198-7. [Google Scholar]
- Naveed, H.; Khan, A.U.; Qiu, S.; Saqib, M.; Anwar, S.; Usman, M.; Akhtar, N.; Barnes, N.; Mian, A. A Comprehensive Overview of Large Language Models. arXiv 2023. [Google Scholar] [CrossRef]
- Liu, C.; Tian, Y.; Song, Y. A Systematic Review of Deep Learning-Based Research on Radiology Report Generation. arXiv 2023. [Google Scholar] [CrossRef]
- Bhayana, R. Chatbots and Large Language Models in Radiology: A Practical Primer for Clinical and Research Applications. Radiology 2024, 310, e232756. [Google Scholar] [CrossRef]
- Singhal, K.; Azizi, S.; Tu, T.; Mahdavi, S.S.; Wei, J.; Chung, H.W.; Scales, N.; Tanwani, A.; Cole-Lewis, H.; Pfohl, S.; et al. Large Language Models Encode Clinical Knowledge. Nature 2023, 620, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Open, A.I.; Achiam, J.; Adler, S.; Agarwal, S.; Ahmad, L.; Akkaya, I.; Aleman, F.L.; Almeida, D.; Altenschmidt, J.; Altman, S.; et al. GPT-4 Technical Report. arXiv 2023. [Google Scholar] [CrossRef]
- Touvron, H.; Lavril, T.; Izacard, G.; Martinet, X.; Lachaux, M.-A.; Lacroix, T.; Rozière, B.; Goyal, N.; Hambro, E.; Azhar, F.; et al. LLaMA: Open and Efficient Foundation Language Models. arXiv 2023. [Google Scholar] [CrossRef]
- Han, T.; Adams, L.C.; Papaioannou, J.-M.; Grundmann, P.; Oberhauser, T.; Löser, A.; Truhn, D.; Bressem, K.K. MedAlpaca—An Open-Source Collection of Medical Conversational AI Models and Training Data. arXiv 2023. [Google Scholar] [CrossRef]
- Li, C.; Wong, C.; Zhang, S.; Usuyama, N.; Liu, H.; Yang, J.; Naumann, T.; Poon, H.; Gao, J. LLaVA-Med: Training a Large Language-and-Vision Assistant for Biomedicine in One Day. arXiv 2023. [Google Scholar] [CrossRef]
- Yu, H.; Yang, L.T.; Zhang, Q.; Armstrong, D.; Deen, M.J. Convolutional Neural Networks for Medical Image Analysis: State-of-the-Art, Comparisons, Improvement and Perspectives. Neurocomputing 2021, 444, 92–110. [Google Scholar] [CrossRef]
- Li, J.; Zhu, G.; Hua, C.; Feng, M.; Bennamoun, B.; Li, P.; Lu, X.; Song, J.; Shen, P.; Xu, X.; et al. A Systematic Collection of Medical Image Datasets for Deep Learning. ACM Comput. Surv. 2024, 56, 1–51. [Google Scholar] [CrossRef]
- Condon, J.J.J.; Oakden-Rayner, L.; Hall, K.A.; Reintals, M.; Holmes, A.; Carneiro, G.; Palmer, L.J. Replication of an Open-Access Deep Learning System for Screening Mammography: Reduced Performance Mitigated by Retraining on Local Data; Radiology and Imaging: Lakeland, FL, USA, 2021. [Google Scholar]
- Yang, J.; Soltan, A.A.S.; Clifton, D.A. Machine Learning Generalizability across Healthcare Settings: Insights from Multi-Site COVID-19 Screening. Npj Digit. Med. 2022, 5, 69. [Google Scholar] [CrossRef]
- Parisi, G.I.; Kemker, R.; Part, J.L.; Kanan, C.; Wermter, S. Continual Lifelong Learning with Neural Networks: A Review. Neural Netw. 2019, 113, 54–71. [Google Scholar] [CrossRef]
- Dhilleswararao, P.; Boppu, S.; Manikandan, M.S.; Cenkeramaddi, L.R. Efficient Hardware Architectures for Accelerating Deep Neural Networks: Survey. IEEE Access 2022, 10, 131788–131828. [Google Scholar] [CrossRef]
- Khalid, N.; Qayyum, A.; Bilal, M.; Al-Fuqaha, A.; Qadir, J. Privacy-Preserving Artificial Intelligence in Healthcare: Techniques and Applications. Comput. Biol. Med. 2023, 158, 106848. [Google Scholar] [CrossRef] [PubMed]
- Dikici, E.; Bigelow, M.; Prevedello, L.M.; White, R.D.; Erdal, B.S. Integrating AI into Radiology Workflow: Levels of Research, Production, and Feedback Maturity. J. Med. Imaging 2020, 7, 1. [Google Scholar] [CrossRef]
- Salahuddin, Z.; Woodruff, H.C.; Chatterjee, A.; Lambin, P. Transparency of Deep Neural Networks for Medical Image Analysis: A Review of Interpretability Methods. Comput. Biol. Med. 2022, 140, 105111. [Google Scholar] [CrossRef]
- Llama.Cpp. Available online: https://github.com/ggerganov/llama.cpp (accessed on 12 February 2024).
- ComfyUI. Available online: https://github.com/comfyanonymous/ComfyUI (accessed on 12 February 2024).
- Johnson, J.M.; Khoshgoftaar, T.M. Survey on Deep Learning with Class Imbalance. J. Big Data 2019, 6, 27. [Google Scholar] [CrossRef]
- Erickson, B.J.; Kitamura, F. Magician’s Corner: 9. Performance Metrics for Machine Learning Models. Radiol. Artif. Intell. 2021, 3, e200126. [Google Scholar] [CrossRef] [PubMed]
- Logan, J.; Kennedy, P.J.; Catchpoole, D. A Review of the Machine Learning Datasets in Mammography, Their Adherence to the FAIR Principles and the Outlook for the Future. Sci. Data 2023, 10, 595. [Google Scholar] [CrossRef] [PubMed]
- Heath, M.; Bowyer, K.; Kopans, D.; Kegelmeyer, P.; Moore, R.; Chang, K.; Munishkumaran, S. Current Status of the Digital Database for Screening Mammography. In Digital Mammography; Karssemeijer, N., Thijssen, M., Hendriks, J., Van Erning, L., Eds.; Computational Imaging and Vision; Springer: Dordrecht, The Netherlands, 1998; Volume 13, pp. 457–460. ISBN 978-94-010-6234-3. [Google Scholar]
- Moreira, I.C.; Amaral, I.; Domingues, I.; Cardoso, A.; Cardoso, M.J.; Cardoso, J.S. INbreast. Acad. Radiol. 2012, 19, 236–248. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.S.; Gimenez, F.; Hoogi, A.; Miyake, K.K.; Gorovoy, M.; Rubin, D.L. A Curated Mammography Data Set for Use in Computer-Aided Detection and Diagnosis Research. Sci. Data 2017, 4, 170177. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.T.; Nguyen, H.Q.; Pham, H.H.; Lam, K.; Le, L.T.; Dao, M.; Vu, V. VinDr-Mammo: A Large-Scale Benchmark Dataset for Computer-Aided Diagnosis in Full-Field Digital Mammography. Sci. Data 2023, 10, 277. [Google Scholar] [CrossRef]
- Frazer, H.M.L.; Tang, J.S.N.; Elliott, M.S.; Kunicki, K.M.; Hill, B.; Karthik, R.; Kwok, C.F.; Peña-Solorzano, C.A.; Chen, Y.; Wang, C.; et al. ADMANI: Annotated Digital Mammograms and Associated Non-Image Datasets. Radiol. Artif. Intell. 2023, 5, e220072. [Google Scholar] [CrossRef]
- RSNA Screening Mammography Breast Cancer Detection AI Challenge. Available online: https://www.rsna.org/rsnai/ai-image-challenge/screening-mammography-breast-cancer-detection-ai-challenge (accessed on 18 February 2024).
- Pawłowska, A.; Ćwierz-Pieńkowska, A.; Domalik, A.; Jaguś, D.; Kasprzak, P.; Matkowski, R.; Fura, Ł.; Nowicki, A.; Żołek, N. Curated Benchmark Dataset for Ultrasound Based Breast Lesion Analysis. Sci. Data 2024, 11, 148. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Flores, W.; Gregorio-Calas, M.J.; Coelho De Albuquerque Pereira, W. BUS-BRA: A Breast Ultrasound Dataset for Assessing Computer-aided Diagnosis Systems. Med. Phys. 2023, 51, 3110–3123. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.; Harowicz, M.R.; Grimm, L.J.; Kim, C.E.; Ghate, S.V.; Walsh, R.; Mazurowski, M.A. A Machine Learning Approach to Radiogenomics of Breast Cancer: A Study of 922 Subjects and 529 DCE-MRI Features. Br. J. Cancer 2018, 119, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Liao, Y.; Xie, J.; He, X.; Zhang, S.; Wang, G.; Fang, J.; Lu, H.; Yu, J. BreastDM: A DCE-MRI Dataset for Breast Tumor Image Segmentation and Classification. Comput. Biol. Med. 2023, 164, 107255. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Phang, J.; Geras, K.J. The NYU Breast Cancer Screening Dataset v1.0; New York University: New York, NY, USA, 2019. [Google Scholar]
- Shamout, F.; Shen, Y.; Geras, K.J. The NYU Breast Ultrasound Dataset v1.0; New York University: New York, NY, USA, 2021. [Google Scholar]
- Witowski, J.; Gong, S.; Geras, K.J. The NYU Breast MRI Dataset v1.0; New York University: New York, NY, USA, 2022. [Google Scholar]
- Becker, A.S.; Marcon, M.; Ghafoor, S.; Wurnig, M.C.; Frauenfelder, T.; Boss, A. Deep Learning in Mammography: Diagnostic Accuracy of a Multipurpose Image Analysis Software in the Detection of Breast Cancer. Investig. Radiol. 2017, 52, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.T.; Lim, V.; Vu, H.X.; Chim, R.; Weise, E.; Liu, J.; Bradley, W.G.; Comstock, C.E. Improved Cancer Detection Using Artificial Intelligence: A Retrospective Evaluation of Missed Cancers on Mammography. J. Digit. Imaging 2019, 32, 625–637. [Google Scholar] [CrossRef]
- Akselrod-Ballin, A.; Chorev, M.; Shoshan, Y.; Spiro, A.; Hazan, A.; Melamed, R.; Barkan, E.; Herzel, E.; Naor, S.; Karavani, E.; et al. Predicting Breast Cancer by Applying Deep Learning to Linked Health Records and Mammograms. Radiology 2019, 292, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Schaffter, T.; Buist, D.S.M.; Lee, C.I.; Nikulin, Y.; Ribli, D.; Guan, Y.; Lotter, W.; Jie, Z.; Du, H.; Wang, S.; et al. Evaluation of Combined Artificial Intelligence and Radiologist Assessment to Interpret Screening Mammograms. JAMA Netw. Open 2020, 3, e200265. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-E.; Kim, H.H.; Han, B.-K.; Kim, K.H.; Han, K.; Nam, H.; Lee, E.H.; Kim, E.-K. Changes in Cancer Detection and False-Positive Recall in Mammography Using Artificial Intelligence: A Retrospective, Multireader Study. Lancet Digit. Health 2020, 2, e138–e148. [Google Scholar] [CrossRef]
- Dembrower, K.; Wåhlin, E.; Liu, Y.; Salim, M.; Smith, K.; Lindholm, P.; Eklund, M.; Strand, F. Effect of Artificial Intelligence-Based Triaging of Breast Cancer Screening Mammograms on Cancer Detection and Radiologist Workload: A Retrospective Simulation Study. Lancet Digit. Health 2020, 2, e468–e474. [Google Scholar] [CrossRef]
- Dembrower, K.; Crippa, A.; Colón, E.; Eklund, M.; Strand, F. Artificial Intelligence for Breast Cancer Detection in Screening Mammography in Sweden: A Prospective, Population-Based, Paired-Reader, Non-Inferiority Study. Lancet Digit. Health 2023, 5, e703–e711. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.Y.; Oberije, C.J.G.; Ambrózay, É.; Szabó, E.; Serfőző, O.; Karpati, E.; Fox, G.; Glocker, B.; Morris, E.A.; Forrai, G.; et al. Prospective Implementation of AI-Assisted Screen Reading to Improve Early Detection of Breast Cancer. Nat. Med. 2023, 29, 3044–3049. [Google Scholar] [CrossRef] [PubMed]
- Romero-Martín, S.; Elías-Cabot, E.; Raya-Povedano, J.L.; Gubern-Mérida, A.; Rodríguez-Ruiz, A.; Álvarez-Benito, M. Stand-Alone Use of Artificial Intelligence for Digital Mammography and Digital Breast Tomosynthesis Screening: A Retrospective Evaluation. Radiology 2022, 302, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Zheng, T.; Lin, F.; Li, X.; Chu, T.; Gao, J.; Zhang, S.; Li, Z.; Gu, Y.; Wang, S.; Zhao, F.; et al. Deep Learning-Enabled Fully Automated Pipeline System for Segmentation and Classification of Single-Mass Breast Lesions Using Contrast-Enhanced Mammography: A Prospective, Multicentre Study. eClinicalMedicine 2023, 58, 101913. [Google Scholar] [CrossRef] [PubMed]
- Beuque, M.P.L.; Lobbes, M.B.I.; Van Wijk, Y.; Widaatalla, Y.; Primakov, S.; Majer, M.; Balleyguier, C.; Woodruff, H.C.; Lambin, P. Combining Deep Learning and Handcrafted Radiomics for Classification of Suspicious Lesions on Contrast-Enhanced Mammograms. Radiology 2023, 307, e221843. [Google Scholar] [CrossRef] [PubMed]
- Qian, N.; Jiang, W.; Guo, Y.; Zhu, J.; Qiu, J.; Yu, H.; Huang, X. Breast Cancer Diagnosis from Contrast-Enhanced Mammography Using Multi-Feature Fusion Neural Network. Eur. Radiol. 2023, 34, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Xu, W.; Lin, B.; An, X.; Tian, J.; Ran, H.; Ren, W.; Chang, C.; Yuan, J.; Kang, C.; et al. Deep Learning Based on Ultrasound Images Assists Breast Lesion Diagnosis in China: A Multicenter Diagnostic Study. Insights Imaging 2022, 13, 124. [Google Scholar] [CrossRef]
- Janse, M.H.A.; Janssen, L.M.; Van Der Velden, B.H.M.; Moman, M.R.; Wolters-van Der Ben, E.J.M.; Kock, M.C.J.M.; Viergever, M.A.; Van Diest, P.J.; Gilhuijs, K.G.A. Deep Learning-Based Segmentation of Locally Advanced Breast Cancer on MRI in Relation to Residual Cancer Burden: A Multi-Institutional Cohort Study. J. Magn. Reson. Imaging 2023, 58, 1739–1749. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Fan, Y.; Xu, D.; Li, Y.; Zhong, Z.; Pan, H.; Huang, B.; Xie, X.; Yang, Y.; Liu, B. Deep Learning Radiomic Analysis of DCE-MRI Combined with Clinical Characteristics Predicts Pathological Complete Response to Neoadjuvant Chemotherapy in Breast Cancer. Front. Oncol. 2023, 12, 1041142. [Google Scholar] [CrossRef]
- RSNA Announces Screening Mammography AI Challenge Results. Available online: https://www.rsna.org/news/2023/may/mammography-ai-challenge-winners (accessed on 18 February 2024).
- RSNA Screening Mammography Breast Cancer Detection—1st Place Solution. Available online: https://www.kaggle.com/competitions/rsna-breast-cancer-detection/discussion/392449 (accessed on 18 February 2024).
- Ge, Z.; Liu, S.; Wang, F.; Li, Z.; Sun, J. YOLOX: Exceeding YOLO Series in 2021. arXiv 2021. [Google Scholar] [CrossRef]
- Magni, V.; Cozzi, A.; Schiaffino, S.; Colarieti, A.; Sardanelli, F. Artificial Intelligence for Digital Breast Tomosynthesis: Impact on Diagnostic Performance, Reading Times, and Workload in the Era of Personalized Screening. Eur. J. Radiol. 2023, 158, 110631. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Mann, R.M. Contrast-Enhanced Mammography: Better with AI? Eur. Radiol. 2023, 34, 914–916. [Google Scholar] [CrossRef] [PubMed]
- Kinkar, K.K.; Fields, B.K.K.; Yamashita, M.W.; Varghese, B.A. Empowering Breast Cancer Diagnosis and Radiology Practice: Advances in Artificial Intelligence for Contrast-Enhanced Mammography. Front. Radiol. 2024, 3, 1326831. [Google Scholar] [CrossRef] [PubMed]
- Dan, Q.; Xu, Z.; Burrows, H.; Bissram, J.; Stringer, J.S.A.; Li, Y. Diagnostic Performance of Deep Learning in Ultrasound Diagnosis of Breast Cancer: A Systematic Review. Npj Precis. Oncol. 2024, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Yao, Z.; Huang, Y.; Yu, Y.; Wang, Y.; Liu, Y.; Mao, R.; Li, F.; Xiao, Y.; Wang, Y.; et al. Deep Learning Radiomics Can Predict Axillary Lymph Node Status in Early-Stage Breast Cancer. Nat. Commun. 2020, 11, 1236. [Google Scholar] [CrossRef]
- Sun, S.; Mutasa, S.; Liu, M.Z.; Nemer, J.; Sun, M.; Siddique, M.; Desperito, E.; Jambawalikar, S.; Ha, R.S. Deep Learning Prediction of Axillary Lymph Node Status Using Ultrasound Images. Comput. Biol. Med. 2022, 143, 105250. [Google Scholar] [CrossRef] [PubMed]
- Lyu, Y.; Xu, Y.; Jiang, X.; Liu, J.; Zhao, X.; Zhu, X. AMS-PAN: Breast Ultrasound Image Segmentation Model Combining Attention Mechanism and Multi-Scale Features. Biomed. Signal Process. Control 2023, 81, 104425. [Google Scholar] [CrossRef]
- Adam, R.; Dell’Aquila, K.; Hodges, L.; Maldjian, T.; Duong, T.Q. Deep Learning Applications to Breast Cancer Detection by Magnetic Resonance Imaging: A Literature Review. Breast Cancer Res. 2023, 25, 87. [Google Scholar] [CrossRef] [PubMed]
- LABC_Segmentation. Available online: https://github.com/Lab-Translational-Cancer-Imaging/LABC_Segmentation (accessed on 19 February 2024).
- Chung, M.; Calabrese, E.; Mongan, J.; Ray, K.M.; Hayward, J.H.; Kelil, T.; Sieberg, R.; Hylton, N.; Joe, B.N.; Lee, A.Y. Deep Learning to Simulate Contrast-Enhanced Breast MRI of Invasive Breast Cancer. Radiology 2023, 306, e213199. [Google Scholar] [CrossRef]
- Osuala, R.; Joshi, S.; Tsirikoglou, A.; Garrucho, L.; Pinaya, W.H.L.; Diaz, O.; Lekadir, K. Pre- to Post-Contrast Breast MRI Synthesis for Enhanced Tumour Segmentation. arXiv 2023. [Google Scholar] [CrossRef]
- Pre_Post_Synthesis. Available online: https://github.com/RichardObi/pre_post_synthesis (accessed on 19 February 2024).
- Mashekova, A.; Zhao, Y.; Ng, E.Y.K.; Zarikas, V.; Fok, S.C.; Mukhmetov, O. Early Detection of the Breast Cancer Using Infrared Technology—A Comprehensive Review. Therm. Sci. Eng. Prog. 2022, 27, 101142. [Google Scholar] [CrossRef]
- Gogoi, U.R.; Majumdar, G.; Bhowmik, M.K.; Ghosh, A.K. Evaluating the Efficiency of Infrared Breast Thermography for Early Breast Cancer Risk Prediction in Asymptomatic Population. Infrared Phys. Technol. 2019, 99, 201–211. [Google Scholar] [CrossRef]
- Mambou, S.; Maresova, P.; Krejcar, O.; Selamat, A.; Kuca, K. Breast Cancer Detection Using Infrared Thermal Imaging and a Deep Learning Model. Sensors 2018, 18, 2799. [Google Scholar] [CrossRef] [PubMed]
- Al Husaini, M.A.S.; Habaebi, M.H.; Gunawan, T.S.; Islam, M.R.; Elsheikh, E.A.A.; Suliman, F.M. Thermal-Based Early Breast Cancer Detection Using Inception V3, Inception V4 and Modified Inception MV4. Neural Comput. Appl. 2022, 34, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Alshehri, A.; AlSaeed, D. Breast Cancer Detection in Thermography Using Convolutional Neural Networks (CNNs) with Deep Attention Mechanisms. Appl. Sci. 2022, 12, 12922. [Google Scholar] [CrossRef]
- Alshehri, A.; AlSaeed, D. Breast Cancer Diagnosis in Thermography Using Pre-Trained VGG16 with Deep Attention Mechanisms. Symmetry 2023, 15, 582. [Google Scholar] [CrossRef]
- Mohamed, E.A.; Rashed, E.A.; Gaber, T.; Karam, O. Deep Learning Model for Fully Automated Breast Cancer Detection System from Thermograms. PLoS ONE 2022, 17, e0262349. [Google Scholar] [CrossRef] [PubMed]
- Civilibal, S.; Cevik, K.K.; Bozkurt, A. A Deep Learning Approach for Automatic Detection, Segmentation and Classification of Breast Lesions from Thermal Images. Expert Syst. Appl. 2023, 212, 118774. [Google Scholar] [CrossRef]
- Khomsi, Z.; Elfezazi, M.; Bellarbi, L. Deep Learning-Based Approach in Surface Thermography for Inverse Estimation of Breast Tumor Size. Sci. Afr. 2024, 23, e01987. [Google Scholar] [CrossRef]
- Singh, A.; Bhat, V.; Sudhakar, S.; Namachivayam, A.; Gangadharan, C.; Pulchan, C.; Sigamani, A. Multicentric Study to Evaluate the Effectiveness of Thermalytix as Compared with Standard Screening Modalities in Subjects Who Show Possible Symptoms of Suspected Breast Cancer. BMJ Open 2021, 11, e052098. [Google Scholar] [CrossRef]
- Bansal, R.; Collison, S.; Krishnan, L.; Aggarwal, B.; Vidyasagar, M.; Kakileti, S.T.; Manjunath, G. A Prospective Evaluation of Breast Thermography Enhanced by a Novel Machine Learning Technique for Screening Breast Abnormalities in a General Population of Women Presenting to a Secondary Care Hospital. Front. Artif. Intell. 2023, 5, 1050803. [Google Scholar] [CrossRef] [PubMed]
- AlSawaftah, N.; El-Abed, S.; Dhou, S.; Zakaria, A. Microwave Imaging for Early Breast Cancer Detection: Current State, Challenges, and Future Directions. J. Imaging 2022, 8, 123. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Bayuela, D.Á.; Ghavami, N.; Tiberi, G.; Sani, L.; Vispa, A.; Bigotti, A.; Raspa, G.; Badia, M.; Papini, L.; Ghavami, M.; et al. A Multicentric, Single Arm, Prospective, Stratified Clinical Investigation to Evaluate MammoWave’s Ability in Breast Lesions Detection. PLoS ONE 2023, 18, e0288312. [Google Scholar] [CrossRef] [PubMed]
- Moloney, B.M.; McAnena, P.F.; Abd Elwahab, S.M.; Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Glynn, C.; O’Connell, A.; Ennis, R.; Lowery, A.J.; et al. Microwave Imaging in Breast Cancer—Results from the First-In-Human Clinical Investigation of the Wavelia System. Acad. Radiol. 2022, 29, S211–S222. [Google Scholar] [CrossRef] [PubMed]
- Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Moloney, B.M.; Abd Elwahab, S.M.; Kerin, M.J. Automated Breast Lesion Detection and Characterization with the Wavelia Microwave Breast Imaging System: Methodological Proof-of-Concept on First-in-Human Patient Data. Appl. Sci. 2021, 11, 9998. [Google Scholar] [CrossRef]
- Sani, L.; Vispa, A.; Loretoni, R.; Duranti, M.; Ghavami, N.; Alvarez Sánchez-Bayuela, D.; Caschera, S.; Paoli, M.; Bigotti, A.; Badia, M.; et al. Breast Lesion Detection through MammoWave Device: Empirical Detection Capability Assessment of Microwave Images’ Parameters. PLoS ONE 2021, 16, e0250005. [Google Scholar] [CrossRef] [PubMed]
- Moloney, B.M.; McAnena, P.F.; Elwahab, S.M.; Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Glynn, C.; O’Connell, A.; Ennis, R.; Lowery, A.J.; et al. The Wavelia Microwave Breast Imaging System–Tumour Discriminating Features and Their Clinical Usefulness. Br. J. Radiol. 2021, 94, 20210907. [Google Scholar] [CrossRef] [PubMed]
- The MammoScreen Project. Available online: https://mammoscreenproject.eu/ (accessed on 18 March 2024).
- Papini, L.; Badia, M.; Sani, L.; Rana, S.P.; Álvarez Sánchez-Bayuela, D.; Vispa, A.; Bigotti, A.; Raspa, G.; Ghavami, N.; Castellano, C.R.; et al. Breast Cancer Detection Using Machine Learning Approaches on Microwave-Based Data. In Proceedings of the 2023 17th European Conference on Antennas and Propagation (EuCAP), Florence, Italy, 26–31 March 2023; pp. 1–5. [Google Scholar]
- Barr, R.G. Future of Breast Elastography. Ultrasonography 2019, 38, 93–105. [Google Scholar] [CrossRef]
- Zhang, Q.; Xiao, Y.; Dai, W.; Suo, J.; Wang, C.; Shi, J.; Zheng, H. Deep Learning Based Classification of Breast Tumors with Shear-Wave Elastography. Ultrasonics 2016, 72, 150–157. [Google Scholar] [CrossRef]
- Fukuda, T.; Tsunoda, H.; Yagishita, K.; Naganawa, S.; Hayashi, K.; Kurihara, Y. Deep Learning for Differentiation of Breast Masses Detected by Screening Ultrasound Elastography. Ultrasound Med. Biol. 2023, 49, 989–995. [Google Scholar] [CrossRef]
- Tadwalkar, R.V.; Rapelyea, J.A.; Torrente, J.; Rechtman, L.R.; Teal, C.B.; Mcswain, A.P.; Donnelly, C.; Kidwell, A.B.; Coffey, C.M.; Brem, R.F. Breast-Specific Gamma Imaging as an Adjunct Modality for the Diagnosis of Invasive Breast Cancer with Correlation to Tumour Size and Grade. Br. J. Radiol. 2012, 85, e212–e216. [Google Scholar] [CrossRef] [PubMed]
- Brem, R.F.; Ruda, R.C.; Yang, J.L.; Coffey, C.M.; Rapelyea, J.A. Breast-Specific γ-Imaging for the Detection of Mammographically Occult Breast Cancer in Women at Increased Risk. J. Nucl. Med. 2016, 57, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Dong, M.; Yang, D.; Wang, L.; Wang, H.; Ma, L. Deep Learning for Differentiating Benign from Malignant Tumors on Breast-Specific Gamma Image. Technol. Health Care 2023, 31, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, D.; Madsen, K.S.; Kalinyak, J.E.; Berg, W.A. Interpretation of Positron Emission Mammography: Feature Analysis and Rates of Malignancy. Am. J. Roentgenol. 2011, 196, 956–970. [Google Scholar] [CrossRef] [PubMed]
- Glass, S.B.; Shah, Z.A. Clinical Utility of Positron Emission Mammography. Bayl. Univ. Med. Cent. Proc. 2013, 26, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Herranz, M.; Ruibal, A. Optical Imaging in Breast Cancer Diagnosis: The Next Evolution. J. Oncol. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Godavarty, A.; Rodriguez, S.; Jung, Y.-J.; Gonzalez, S. Optical Imaging for Breast Cancer Prescreening. Breast Cancer Targets Ther. 2015, 7, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Xue, M.; Li, S.; Zou, Y.; Zhu, Q. Fusion Deep Learning Approach Combining Diffuse Optical Tomography and Ultrasound for Improving Breast Cancer Classification. Biomed. Opt. Express 2023, 14, 1636. [Google Scholar] [CrossRef] [PubMed]
- Dosovitskiy, A.; Beyer, L.; Kolesnikov, A.; Weissenborn, D.; Zhai, X.; Unterthiner, T.; Dehghani, M.; Minderer, M.; Heigold, G.; Gelly, S.; et al. An Image Is Worth 16x16 Words: Transformers for Image Recognition at Scale. arXiv 2021, arXiv:2010.11929. [Google Scholar]
- Han, K.; Wang, Y.; Chen, H.; Chen, X.; Guo, J.; Liu, Z.; Tang, Y.; Xiao, A.; Xu, C.; Xu, Y.; et al. A Survey on Vision Transformer. IEEE Trans. Pattern Anal. Mach. Intell. 2023, 45, 87–110. [Google Scholar] [CrossRef]
- Parvaiz, A.; Khalid, M.A.; Zafar, R.; Ameer, H.; Ali, M.; Fraz, M.M. Vision Transformers in Medical Computer Vision—A Contemplative Retrospection. Eng. Appl. Artif. Intell. 2023, 122, 106126. [Google Scholar] [CrossRef]
- Gao, X.; Khan, M.H.-M.; Hui, R.; Tian, Z.; Qian, Y.; Gao, A.; Baichoo, S. COVID-VIT: Classification of Covid-19 from 3D CT Chest Images Based on Vision Transformer Model. In Proceedings of the 2022 3rd International Conference on Next Generation Computing Applications (NextComp), Flic-en-Flac, Mauritius, 6–8 October 2022; pp. 1–4. [Google Scholar]
- Chen, X.; Zhang, K.; Abdoli, N.; Gilley, P.W.; Wang, X.; Liu, H.; Zheng, B.; Qiu, Y. Transformers Improve Breast Cancer Diagnosis from Unregistered Multi-View Mammograms. Diagnostics 2022, 12, 1549. [Google Scholar] [CrossRef] [PubMed]
- Hoang, G.M.; Kim, U.-H.; Kim, J.G. Vision Transformers for the Prediction of Mild Cognitive Impairment to Alzheimer’s Disease Progression Using Mid-Sagittal sMRI. Front. Aging Neurosci. 2023, 15, 1102869. [Google Scholar] [CrossRef] [PubMed]
- Ayana, G.; Dese, K.; Dereje, Y.; Kebede, Y.; Barki, H.; Amdissa, D.; Husen, N.; Mulugeta, F.; Habtamu, B.; Choe, S.-W. Vision-Transformer-Based Transfer Learning for Mammogram Classification. Diagnostics 2023, 13, 178. [Google Scholar] [CrossRef] [PubMed]
- Cantone, M.; Marrocco, C.; Tortorella, F.; Bria, A. Convolutional Networks and Transformers for Mammography Classification: An Experimental Study. Sensors 2023, 23, 1229. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.; Debnath, S.; Hu, R.; Chen, X.; Liu, Z.; Kweon, I.S.; Xie, S. ConvNeXt V2: Co-Designing and Scaling ConvNets with Masked Autoencoders. arXiv 2023, arXiv:2301.00808. [Google Scholar]
- Hassanien, M.A.; Singh, V.K.; Puig, D.; Abdel-Nasser, M. Predicting Breast Tumor Malignancy Using Deep ConvNeXt Radiomics and Quality-Based Score Pooling in Ultrasound Sequences. Diagnostics 2022, 12, 1053. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-Y.; Bochkovskiy, A.; Liao, H.-Y.M. YOLOv7: Trainable Bag-of-Freebies Sets New State-of-the-Art for Real-Time Object Detectors. arXiv 2022, arXiv:2207.02696. [Google Scholar]
- Wang, C.-Y.; Yeh, I.-H.; Liao, H.-Y.M. YOLOv9: Learning What You Want to Learn Using Programmable Gradient Information. arXiv 2024, arXiv:2402.13616. [Google Scholar]
- YOLOv8. Available online: https://github.com/ultralytics/ultralytics (accessed on 8 March 2024).
- Aly, G.H.; Marey, M.; El-Sayed, S.A.; Tolba, M.F. YOLO Based Breast Masses Detection and Classification in Full-Field Digital Mammograms. Comput. Methods Programs Biomed. 2021, 200, 105823. [Google Scholar] [CrossRef]
- Su, Y.; Liu, Q.; Xie, W.; Hu, P. YOLO-LOGO: A Transformer-Based YOLO Segmentation Model for Breast Mass Detection and Segmentation in Digital Mammograms. Comput. Methods Programs Biomed. 2022, 221, 106903. [Google Scholar] [CrossRef] [PubMed]
- Hassan, N.M.; Hamad, S.; Mahar, K. YOLO-Based CAD Framework with ViT Transformer for Breast Mass Detection and Classification in CESM and FFDM Images. Neural Comput. Appl. 2024, 36, 6467–6496. [Google Scholar] [CrossRef]
- Prinzi, F.; Insalaco, M.; Orlando, A.; Gaglio, S.; Vitabile, S. A Yolo-Based Model for Breast Cancer Detection in Mammograms. Cogn. Comput. 2024, 16, 107–120. [Google Scholar] [CrossRef]
- nnU-Net V2. Available online: https://github.com/MIC-DKFZ/nnUNet/releases/tag/v2.0 (accessed on 8 March 2024).
- Hassija, V.; Chamola, V.; Mahapatra, A.; Singal, A.; Goel, D.; Huang, K.; Scardapane, S.; Spinelli, I.; Mahmud, M.; Hussain, A. Interpreting Black-Box Models: A Review on Explainable Artificial Intelligence. Cogn. Comput. 2024, 16, 45–74. [Google Scholar] [CrossRef]
- Tabnak, P.; HajiEsmailPoor, Z.; Baradaran, B.; Pashazadeh, F.; Aghebati Maleki, L. MRI-Based Radiomics Methods for Predicting Ki-67 Expression in Breast Cancer: A Systematic Review and Meta-Analysis. Acad. Radiol. 2023, 31, 763–787. [Google Scholar] [CrossRef] [PubMed]
- Euser, A.M.; Zoccali, C.; Jager, K.J.; Dekker, F.W. Cohort Studies: Prospective versus Retrospective. Nephron Clin. Pract. 2009, 113, c214–c217. [Google Scholar] [CrossRef] [PubMed]
- Tripepi, G.; Jager, K.J.; Dekker, F.W.; Zoccali, C. Selection Bias and Information Bias in Clinical Research. Nephron Clin. Pract. 2010, 115, c94–c99. [Google Scholar] [CrossRef] [PubMed]
- Nunan, D.; Aronson, J.; Bankhead, C. Catalogue of Bias: Attrition Bias. BMJ Evid.-Based Med. 2018, 23, 21–22. [Google Scholar] [CrossRef]
- Herington, J.; McCradden, M.D.; Creel, K.; Boellaard, R.; Jones, E.C.; Jha, A.K.; Rahmim, A.; Scott, P.J.H.; Sunderland, J.J.; Wahl, R.L.; et al. Ethical Considerations for Artificial Intelligence in Medical Imaging: Deployment and Governance. J. Nucl. Med. 2023, 64, 1509–1515. [Google Scholar] [CrossRef]
- Dratsch, T.; Chen, X.; Rezazade Mehrizi, M.; Kloeckner, R.; Mähringer-Kunz, A.; Püsken, M.; Baeßler, B.; Sauer, S.; Maintz, D.; Pinto Dos Santos, D. Automation Bias in Mammography: The Impact of Artificial Intelligence BI-RADS Suggestions on Reader Performance. Radiology 2023, 307, e222176. [Google Scholar] [CrossRef]
- Hartman, D.J.; Van Der Laak, J.A.W.M.; Gurcan, M.N.; Pantanowitz, L. Value of Public Challenges for the Development of Pathology Deep Learning Algorithms. J. Pathol. Inform. 2020, 11, 7. [Google Scholar] [CrossRef]
- RSNA AI Challenges. Available online: https://www.rsna.org/rsnai/ai-image-challenge (accessed on 8 March 2024).
- MICCAI Registered Challenges. Available online: http://www.miccai.org/special-interest-groups/challenges/miccai-registered-challenges/ (accessed on 8 March 2024).
- Grand Challenge—Challenges. Available online: https://grand-challenge.org/challenges/ (accessed on 8 March 2024).
- Maleki, F.; Ovens, K.; Gupta, R.; Reinhold, C.; Spatz, A.; Forghani, R. Generalizability of Machine Learning Models: Quantitative Evaluation of Three Methodological Pitfalls. Radiol. Artif. Intell. 2023, 5, e220028. [Google Scholar] [CrossRef]
- Pei, X.; Zuo, K.; Li, Y.; Pang, Z. A Review of the Application of Multi-Modal Deep Learning in Medicine: Bibliometrics and Future Directions. Int. J. Comput. Intell. Syst. 2023, 16, 44. [Google Scholar] [CrossRef]
- Thompson, N.C.; Greenewald, K.; Lee, K.; Manso, G.F. The Computational Limits of Deep Learning. arXiv 2020. [Google Scholar] [CrossRef]
- Lobig, F.; Subramanian, D.; Blankenburg, M.; Sharma, A.; Variyar, A.; Butler, O. To Pay or Not to Pay for Artificial Intelligence Applications in Radiology. Npj Digit. Med. 2023, 6, 117. [Google Scholar] [CrossRef]
- Saranya, A.; Subhashini, R. A Systematic Review of Explainable Artificial Intelligence Models and Applications: Recent Developments and Future Trends. Decis. Anal. J. 2023, 7, 100230. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Origin | Release Year | Number of Patients | Modality |
|---|---|---|---|---|
| DDSM | United States | 1999 | 2620 | SFM |
| INBreast | Portugal | 2011 | 115 | FFDM |
| CBIS-DDSM | United States | 2017 | 1566 | SFM (improved) |
| VinDr-Mammo | Vietnam | 2022 | 5000 | FFDM |
| ADMANI | Australia | 2022 | 630,000 (40,000 public test images) | FFDM |
| BrEaST | Poland | 2023 | 256 | US |
| BUS-BRA | Brazil | 2023 | 1064 | US |
| Duke-Breast-Cancer-MRI | United States | 2022 | 922 | DCE-MRI |
| BreastDM | China | 2023 | 232 | DCE-MRI |
| Authors | Year | Software/Model | Modality | Type | Task |
|---|---|---|---|---|---|
| Becker et al. [76] | 2017 | dANN (ViDi 2.0) | MG | Retrospective | Classification |
| Watanabe et al. [77] | 2019 | cmAssist® | MG | Retrospective | Classification |
| Akselrod-Ballin et al. [78] | 2019 | Custom ML + DL | MG | Retrospective | Classification |
| Schaftter et al. [79] | 2020 | Multiple (public challenge) | MG | Retrospective | Classification |
| Kim et al. [80] | 2020 | INSIGHT MMG | MG | Retrospective | Classification |
| Dembrower et al. [81] | 2020 | INSIGHT MMG | MG | Retrospective | Classification |
| Dembrower et al. [82] | 2023 | INSIGHT MMG 1.1.6 | MG | Prospective | Classification |
| Ng et al. [83] | 2023 | Mia® 2.0 (Kheiron Medical Technologies Ltd., London, UK) | MG | Prospective | Classification |
| Romero-Martín et al. [84] | 2021 | Transpara® | MG, DBT | Retrospective | Classification |
| Zheng et al. [85] | 2023 | RefineNet + Xception | CEM | Prospective | Segmentation, Classification |
| Beuque et al. [86] | 2023 | DL + handcrafted radiomics | CEM | Retrospective | Segmentation, Classification |
| Qian et al. [87] | 2023 | Multi-feature fusion network | CEM | Retrospective | Classification |
| Gu et al. [88] | 2022 | VGG19 | US | Prospective | Classification |
| Janse et al. [89] | 2023 | nnU-Net | DCE-MRI | Retrospective | Segmentation |
| Li et al. [90] | 2023 | Custom DLR | DCE-MRI | Retrospective | Treatment Response Prediction |
| Product | Vendor | Country | Modality |
|---|---|---|---|
| cmAssist® | CureMetrix Inc., La Jolla, CA, USA | United States | MG |
| Genius AI Detection | Hologic Inc., Marlborough, MA, USA | United States | MG and DBT |
| INSIGHT MMG | Lunit Inc., Seoul, Republic of Korea | South Korea | MG |
| MammoScreen® 2.0 | Therapixel SA, Nice, France | France | MG and DBT |
| ProFound AI® | iCAD Inc., Nashua, NH, USA | United States | MG and DBT |
| Saige-Dx | DeepHealth Inc., Somerville, MA, USA | United States | MG |
| Transpara® | ScreenPoint Medical B.V., Nijmegen, The Netherlands | Netherlands | MG and DBT |
| Authors | Study Design | Key Results | Highlighted Limitations |
|---|---|---|---|
| Becker et al. [76] | Standalone classifier for breast cancer detection versus experienced radiologists | AUC = 0.81 on first training dataset, 0.79 on external testing cohort, 0.82 on second, screening-like cohort (statistically equivalent to experienced radiologists) | Not true screening cohort and retrospective design leading to potential selection bias; worse specificity than experienced radiologists; no understanding of laterality and time evolution, and no inclusion of clinical and bioptic data in the algorithm |
| Watanabe et al. [77] | Radiologist-paired classifier for breast cancer detection to improve radiologists’ sensitivity | Overall reader CDR increased from mean of 51% to mean of 62% (mean of 27% relative increase) | Cancer-enriched dataset and retrospective design leading to potential selection bias; lack of comparison of prior mammograms for radiologists, funding by AI software company |
| Akselrod-Ballin et al. [78] | Standalone classifier for breast cancer detection (malignancy prediction) | AUC = 0.91 with specificity of 77.3% at a sensitivity of 87% | Selection bias; single mammography scanner vendor potentially limiting generalizability; many patients excluded after a single negative examination; distinction between screening and diagnostic studies not well defined; no lesion localization |
| Schaftter et al. [79] | Standalone and radiologist-paired classifier for breast cancer detection; public challenge | Standalone: AUC = 0.858 and 0.903 on the internal and external validation dataset, respectively; radiologist-paired: AUC = 0.942 | Interaction between radiologists and AI not well studied; larger training and validation datasets not available for challenge participants; no cancer spatial annotation; small number of positive cases |
| Kim et al. [80] | Standalone classifier for breast cancer detection versus unassisted and AI-assisted radiologists | AUC = 0.940 for standalone AI versus 0.810 for unassisted radiologists and 0.881 for assisted radiologists, with better performance in detection of mass, distortion, asymmetry, and T1 and node-negative cancers | Cancer-enriched dataset and retrospective design; clinical factors not considered by the algorithm; reading setting potentially different from clinical practice; funding by AI software company |
| Dembrower et al. [81] | Standalone classifier for screening mammograms triage | Missed cancers: 0, 0.3%, or 2.6% for 60%, 70%, or 80%-lowest AI score rule-out, respectively; additional interval cancer detection: 12% or 27% for 1% or 5%-high AI score rule-in, respectively; additional next-round cancer detection: 14% or 35%, respectively | Retrospective design; screening cohort not fully examined; previous mammogram within 30 months before diagnosis required for inclusion; no cancer spatial annotation; single demographic; biennial screening program; interaction between radiologists and AI not well studied; arbitrary triage cut-offs |
| Dembrower et al. (2023) [82] | Radiologist-paired classifier (assisted single reading) for breast cancer detection versus standalone classifier, unassisted double reading, and assisted double reading (triple reading); prospective, non-inferiority study | Non-inferiority of both assisted single reading and standalone classifier compared to double reading | Availability of both AI and radiologists results in the consensus discussion, potentially underestimating AI ability; abnormality threshold based on retrospective data; no quality assurance mechanisms implemented; single-arm paired design preventing comparison of differences in interval cancer rates; no biopsy for negative screening examinations; single scanning machine vendor and AI software used potentially limiting generalizability, funding by AI software company |
| Ng et al. [83] | Radiologist-paired classifier (assisted double reading) for breast cancer detection versus unassisted double reading; prospective study | Additional 0.7–1.6 cancer detection per 1000 cases, with 0.16–0.30% additional recalls, 0–0.23% unnecessary recalls, and 0.1–1.9% increase in positive predictive value; majority of extra detected cancers featuring invasiveness and small size | Data collected from a single breast cancer institution; only one commercial AI software evaluated; short follow-up (2 to 9 months) preventing evaluation of interval cancer rates; unclear impact of inter-reader variation when introducing AI in the process, funding by AI software company |
| Potential | Challenges |
|---|---|
| Non-ionizing radiation | Limited availability of scan devices |
| No breast compression | Lack of standardized protocols |
| Lower costs | Limited availability of curated datasets |
| Lower performance loss in dense breasts | Lack of studies in clinical and screening settings |
| Authors | Year | Software/Model | Modality | Type | Task |
|---|---|---|---|---|---|
| Mambou et al. [108] | 2017 | Custom ML + DL | TG | Retrospective | Classification |
| Mohammed et al. [109] | 2021 | InceptionV4 | TG | Retrospective | Classification |
| Alshehri et al. [110] | 2022 | Custom CNN + AM | TG | Retrospective | Classification |
| Mohamed et al. [112] | 2022 | U-Net + bespoke classifier and VGG16 | TG | Retrospective | Segmentation, Classification |
| Civiliban et al. [113] | 2023 | Mask R-CNN | TG | Retrospective | Segmentation |
| Khomsi et al. [114] | 2024 | Custom FNN | TG | Retrospective | Tumor size estimation |
| Singh et al. [115] | 2021 | Thermalytix® | TG | Prospective | Classification |
| Bansal et al. [116] | 2023 | Thermalytix® | TG | Prospective | Classification |
| Zhang et al. [126] | 2015 | DNN feature extractor + ML classifier | USE | Retrospective | Classification |
| Fukuda et al. [127] | 2023 | GoogLeNet | USE | Retrospective | Classification |
| Yu et al. [130] | 2023 | ResNet18 | BSGI | Retrospective | Classification |
| Zhang et al. [135] | 2023 | Custom fusion model (VGG11 + AE) | DOT + US | Retrospective | Classification |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carriero, A.; Groenhoff, L.; Vologina, E.; Basile, P.; Albera, M. Deep Learning in Breast Cancer Imaging: State of the Art and Recent Advancements in Early 2024. Diagnostics 2024, 14, 848. https://doi.org/10.3390/diagnostics14080848
Carriero A, Groenhoff L, Vologina E, Basile P, Albera M. Deep Learning in Breast Cancer Imaging: State of the Art and Recent Advancements in Early 2024. Diagnostics. 2024; 14(8):848. https://doi.org/10.3390/diagnostics14080848
Chicago/Turabian StyleCarriero, Alessandro, Léon Groenhoff, Elizaveta Vologina, Paola Basile, and Marco Albera. 2024. "Deep Learning in Breast Cancer Imaging: State of the Art and Recent Advancements in Early 2024" Diagnostics 14, no. 8: 848. https://doi.org/10.3390/diagnostics14080848
APA StyleCarriero, A., Groenhoff, L., Vologina, E., Basile, P., & Albera, M. (2024). Deep Learning in Breast Cancer Imaging: State of the Art and Recent Advancements in Early 2024. Diagnostics, 14(8), 848. https://doi.org/10.3390/diagnostics14080848