
Integrating Routine Hematological and Extended Inflammatory Parameters as a Novel Approach for Timely Diagnosis and Prognosis in Sepsis Management

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Collection and Analysis
2.3. Patient Follow-up for 30-Day Mortality
2.4. Statistical Analysis
3. Results
3.1. Subject Demographics and Extended Inflammatory Parameter Profiles
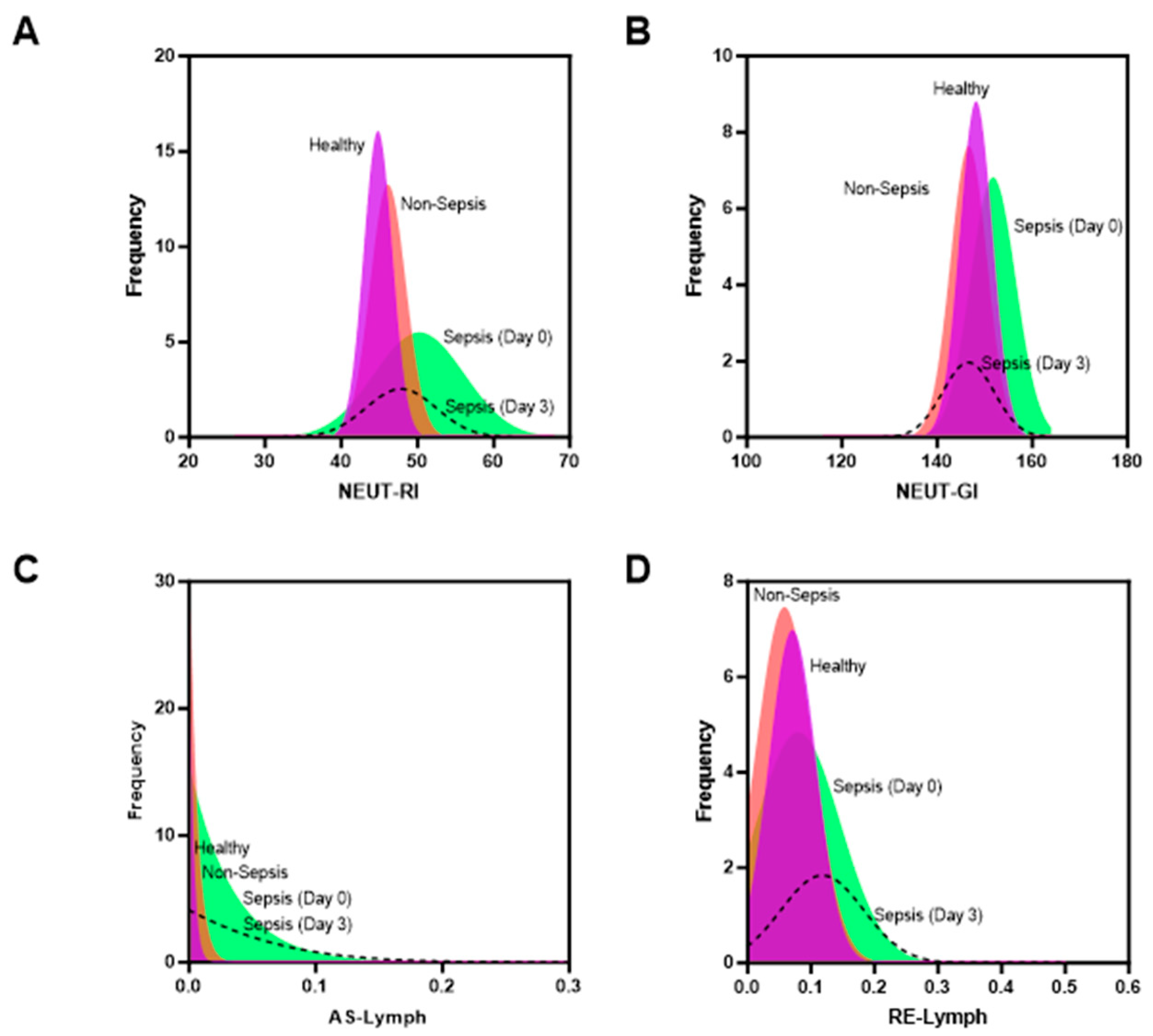
3.2. Discriminatory Power of Hematology Parameters to Identify Immune Responses between Groups
3.3. Prognostic Ability of Combined Hematological Parameters towarods 30-Day Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Septimus, E.J. Sepsis perspective 2020. J. Infect. Dis. 2020, 222, S71–S73. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Purba, A.K.R.; Mariana, N.; Aliska, G.; Wijaya, S.H.; Wulandari, R.R.; Hadi, U.; Hamzah; Nugroho, C.W.; van der Schans, J.; Postma, M.J. The burden and costs of sepsis and reimbursement of its treatment in a developing country: An observational study on focal infections in Indonesia. Int. J. Infect. Dis. 2020, 96, 211–218. [Google Scholar] [CrossRef]
- Li, Y.; Wang, C.; Chen, M.J.S.R. Metabolomics-based study of potential biomarkers of sepsis. Sci. Rep. 2023, 13, 585. [Google Scholar] [CrossRef]
- Ranjit, S.; Kissoon, N.J.T.P. Challenges and Solutions in translating sepsis guidelines into practice in resource-limited settings. Transl. Pediatr. 2021, 10, 2646–2665. [Google Scholar] [CrossRef]
- Kwizera, A.; Adhikari, N.K.; Angus, D.C.; Dondorp, A.M.; Dünser, M.W.; Festic, E.; Haniffa, R.; Kissoon, N.; Martin-Loeches, I.; Lundeg, G. Recognition of Sepsis in resource-limited settings. Sepsis Manag. Resour. Ltd. Settings 2019, 4, 69–84. [Google Scholar]
- Marik, P.E.; Taeb, A.M. SIRS, qSOFA and new sepsis definition. J. Thorac. Dis. 2017, 9, 943–945. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C. Sepsis-3: What is the meaning of a definition? Crit. Care Med. 2016, 44, 1459–1460. [Google Scholar] [CrossRef]
- Qiu, X.; Lei, Y.-P.; Zhou, R.-X. SIRS, SOFA, qSOFA, and NEWS in the diagnosis of sepsis and prediction of adverse outcomes: A systematic review and meta-analysis. Expert Rev. Anti-infective Ther. 2023, 21, 891–900. [Google Scholar] [CrossRef]
- Schertz, A.R.; Lenoir, K.M.; Bertoni, A.G.; Levine, B.J.; Mongraw-Chaffin, M.; Thomas, K.W. Sepsis Prediction Model for Determining Sepsis vs SIRS, qSOFA, and SOFA. JAMA 2023, 6, e2329729. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Rhodes, A.; Evans, L.; Alhazzani, W.; Beale, R.; Jaeschke, R.; Machado, F.R.; Masur, H.; Osborn, T.; Parker, M.M.; et al. Surviving sepsis campaign. Crit. Care Med. 2023, 51, 431–444. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Executive summary: Surviving sepsis campaign: International guidelines for the management of sepsis and septic shock 2021. Crit. Care Med. 2021, 49, 1974–1982. [Google Scholar] [CrossRef] [PubMed]
- Brusco, N.K.; Sykes, K.; Cheng, A.C.; Radia-George, C.; Travis, D.; Sullivan, N.; Dinh, T.; Foster, S.; Thursky, K. A state-wide implementation of a whole of hospital sepsis pathway with a mortality-based cost-effectiveness analysis from a healthcare sector perspective. PLoS Glob. Public Health 2023, 3, e0000687. [Google Scholar] [CrossRef] [PubMed]
- Gupta, E.; Saxena, J.; Kumar, S.; Sharma, U.; Rastogi, S.; Srivastava, V.K.; Kaushik, S.; Jyoti, A.J.D. Fast Track Diagnostic Tools for Clinical Management of Sepsis: Paradigm Shift from Conventional to Advanced Methods. Diagnostics 2023, 13, 277. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.; van Beuningen, F.; Ter Maaten, J.; Bouma, H.R. Hospital-related costs of sepsis around the world: A systematic review exploring the economic burden of sepsis. J. Crit. Care 2022, 71, 154096. [Google Scholar] [CrossRef] [PubMed]
- Oami, T.; Imaeda, T.; Nakada, T.; Abe, T.; Takahashi, N.; Yamao, Y.; Nakagawa, S.; Ogura, H.; Shime, N.; Umemura, Y.; et al. Temporal trends of medical cost and cost-effectiveness in sepsis patients: A Japanese nationwide medical claims database. J. Intensive Care 2022, 10, 33. [Google Scholar] [CrossRef] [PubMed]
- Rubio, I.; Osuchowski, M.F.; Shankar-Hari, M.; Skirecki, T.; Winkler, M.S.; Lachmann, G.; La Rosée, P.; Monneret, G.; Venet, F.; Bauer, M.; et al. Current gaps in sepsis immunology: New opportunities for translational research. Lancet 2019, 19, e422–e436. [Google Scholar] [CrossRef]
- Khodaiji, S. Newer CBC Parameters of Clinical Significance. In Hematopathology: Advances in Understanding; Springer Nature Singapore Pte Ltd.: Singapore, 2019; Volume 1. [Google Scholar]
- van der Geest, P.J.; Mohseni, M.; Linssen, J.; Duran, S.; de Jonge, R.; Groeneveld, A. The intensive care infection score–a novel marker for the prediction of infection and its severity. Crit. Care 2016, 20, 180. [Google Scholar] [CrossRef]
- Abeysuriya, V.; Choong, C.S.H.; Thilakawardana, B.U.; De Mel, P.; Shalindi, M.; De Mel, C.; Chandrasena, L.; Seneviratne, S.L.; Yip, C.; Yap, E.-S.; et al. The atypical lymphocyte count: A novel predictive factor for severe thrombocytopenia related to dengue. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 424–432. [Google Scholar] [CrossRef]
- Abeysuriya, V.; Seneviratne, S.L.; de Mel, P.; Clarice, C.S.H.; de Mel, C.; Chandrasena, L.; Yip, C.; Yap, E.-S.; de Mel, S. The immature platelet fraction, a predictive tool for early recovery from dengue-related thrombocytopenia: A prospective study. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 424–432. [Google Scholar] [CrossRef]
- Nierhaus, A.; Linssen, J.; Wichmann, D.; Braune, S.; Kluge, S.J.I.; Targets, A.-D. Use of a weighted, automated analysis of the differential blood count to differentiate sepsis from non-infectious systemic inflammation: The intensive care infection score (ICIS). Inflamm. Allergy Drug Targets 2012, 11, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Kaeslin, M.; Brunner, S.; Raths, J.; Huber, A. Improvement in detecting bacterial infection in lower respiratory tract infections using the Intensive Care Infection Score (ICIS). J. Lab. Med. 2016, 40, 175–182. [Google Scholar] [CrossRef]
- Merry, M.; Hartawan, I.G.A.G.U.; Aryabiantara, I.W.; Dewi, D.A.M.S. Profile of Sepsis Patients Treated in Intensive Care Unit of Sanglah Hospital Denpasar. Open Access Maced. J. Med. Sci. 2021, 9, 1701–1704. [Google Scholar] [CrossRef]
- Ho, S.F.; Tan, S.J.; Mazlan, M.Z.; Iberahim, S.; Lee, Y.X.; Hassan, R.J.D. Exploring extended white blood cell parameters for the evaluation of sepsis among patients admitted to intensive care units. Diagnostics 2023, 13, 2445. [Google Scholar] [CrossRef] [PubMed]
- Jha, B.; Goel, S.; Singh, M.K.; Sethi, M.; Deswal, V.; Kataria, S.; Mehta, Y.; Saxena, R. Value of new advanced hematological parameters in early prediction of severity of COVID-19. Int. J. Lab. Hematol. 2023, 45, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Ansari-Lari, M.A.; Kickler, T.S.; Borowitz, M.J. Immature granulocyte measurement using the Sysmex XE-2100: Relationship to infection and sepsis. Am J. Clin. Pathol. 2003, 120, 795–799. [Google Scholar] [CrossRef]
- Ranganathan, P.; Aggarwal, R. Common pitfalls in statistical analysis: Understanding the properties of diagnostic tests–Part 1. Perspect. Clin. Res. 2018, 9, 40–43. [Google Scholar] [CrossRef]
- Kowalska-Kępczyńska, A.; Domerecka, W.; Juszczyńska, M.; Donica, H. The application of new immune cell activation markers in the diagnosis of various disease states. Eur. J. Med. Technol. 2020, 4, 29. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Sepsis (n = 39) | Non-Sepsis (n = 39) | Healthy (n = 33) | p-Value |
|---|---|---|---|---|
| Age (year) | 60.77 ± 14.81 | 52.97 ± 16.33 | 33.67 ± 6.14 | |
| Gender | ||||
| Male | 20 (51.3%) | 24 (61.5%) | 23 (69.7%) | |
| Female | 19 (48.7%) | 15 (38.5%) | 10 (30.3%) | |
| Blood culture | ||||
| Positive | 5 (12.8%) | 0 | NA | |
| Negative | 34 (87.2%) | 39 (100%) | NA | |
| Laboratory result | ||||
| SOFA | 4 (2–12) | 0.9 (0–1) | NA | |
| TWBC (103/µL) | 16.84 (5.06–47.60) | 7.93 (4.47–20.80) | 7.83 (5.55–12.94) | <0.001 1 |
| Neut# (103/µL) | 13.40 (3.38–45.35) | 1.58 (0.28–3.17) | 4.50 (2.60–33.90) | <0.001 1 |
| Neut% | 79.10 (44.20–95.20) | 67.50 (44.20–93.40) | 56.90 (6.40–73.80) | <0.001 1 |
| Mono% | 5.89 ± 3.63 | 7.54 ± 2.76 | 7.02 ± 1.40 | 0.0012 2 |
| Lymph# (103/µL) | 0.94 (0.15–2.80) | 1.58 (0.28–3.17) | 2.50 (1.48–4.64) | <0.001 1 |
| Lymph% | 8.33 ± 7.06 | 20.41 ± 11.37 | 31.86 ± 7.07 | <0.001 2 |
| HGB (g/dL) | 9.84 ± 3.39 | 12.17 ± 2.15 | 14.39 ± 1.37 | <0.001 2 |
| PLT# ((103/µL) | 224 (13–598) | 281 (148–609) | 292 (168–424) | 0.399 1 |
| RET-He (pg) | 30.2 (20.5–37.8) | 31.2 (16.0–34.5) | 31.7 (23.7–34.6) | 0.203 1 |
| RBC-He (pg) | 28.7 (23.3–32.0) | 29.0 (14.7–33.6) | 29.3 (17.3–31.5) | 0.737 1 |
| Delta-He (pg) | 1.23 ± 3.83 | 2.35 ± 1.35 | 2.56 ± 0.90 | 0.265 2 |
| IG# (103/µL) | 0.20 (0.03–3.45) | 0.07 (0.01–0.58) | 0.08 (0.01–0.21) | <0.001 1 |
| IG% | 1.4 (0.3–14.5) | 0.8 (0.1–4.7) | 0.95 (0.1–1.8) | 0.001 1 |
| Neut-RI (FI) | 51.1 (40.3–67.8) | 46.2 (41.2–61.7) | 44.8 (26.9–48.6) | <0.001 1 |
| Neut-GI (SI) | 151.6 (138.2–164.4) | 147.0 (125.4–159.1) | 148.1 (141.0–161.2) | 0.001 1 |
| AS-Lymph (103/µL) | 0.01 (0.0–0.35) | 0.0 (0.0.–0.06) | 0.0 (0.0–0.07) | <0.001 1 |
| RE-Lymph (103/µL) | 0.10 (0.01–0.50) | 0.05 (0.0–0.17) | 0.06 (0.0–0.17) | 0.026 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herawati, S.; Somia, I.K.A.; Kosasih, S.; Wande, I.N.; Felim, J.; Payana, I.M.D. Integrating Routine Hematological and Extended Inflammatory Parameters as a Novel Approach for Timely Diagnosis and Prognosis in Sepsis Management. Diagnostics 2024, 14, 956. https://doi.org/10.3390/diagnostics14090956
Herawati S, Somia IKA, Kosasih S, Wande IN, Felim J, Payana IMD. Integrating Routine Hematological and Extended Inflammatory Parameters as a Novel Approach for Timely Diagnosis and Prognosis in Sepsis Management. Diagnostics. 2024; 14(9):956. https://doi.org/10.3390/diagnostics14090956
Chicago/Turabian StyleHerawati, Sianny, I Ketut Agus Somia, Sully Kosasih, I Nyoman Wande, Jethro Felim, and I Made Dwi Payana. 2024. "Integrating Routine Hematological and Extended Inflammatory Parameters as a Novel Approach for Timely Diagnosis and Prognosis in Sepsis Management" Diagnostics 14, no. 9: 956. https://doi.org/10.3390/diagnostics14090956
APA StyleHerawati, S., Somia, I. K. A., Kosasih, S., Wande, I. N., Felim, J., & Payana, I. M. D. (2024). Integrating Routine Hematological and Extended Inflammatory Parameters as a Novel Approach for Timely Diagnosis and Prognosis in Sepsis Management. Diagnostics, 14(9), 956. https://doi.org/10.3390/diagnostics14090956